
FEDERAL COURT OF AUSTRALIA
Karpik v Carnival plc (The Ruby Princess) (Initial Trial) [2023] FCA 1280
ORDERS
Applicant | ||
AND: | CARNIVAL PLC (ARBN 107 998 443 / ABN 23107998443) First Respondent PRINCESS CRUISE LINES LTD (A COMPANY REGISTERED IN BERMUDA) Second Respondent | |
DATE OF ORDER: |
THE COURT ORDERS THAT:
1. The matter be listed for the making of final orders and further case management at 9.30am on 10 November 2023, or at such other time and date as the parties may arrange with the Associate to Stewart J.
2. The parties email agreed or competing orders to give effect to the reasons for judgment published today, including with regard to common questions or the process for the making of orders on common questions, to the Associate to Stewart J by noon on 9 November 2023.
Note: Entry of orders is dealt with in Rule 39.32 of the Federal Court Rules 2011.
STEWART J:
1 On 8 March 2020, shortly before midnight, the passenger liner Ruby Princess cast off from the Ocean Passenger Terminal at Circular Quay in Sydney. It made its way through the heads of Port Jackson and towards New Zealand. It had on board about 2,671 passengers and 1,146 crew members for a 13-day cruise to a number of ports in New Zealand and back to Sydney. At that time, Australia was bracing itself for the novel coronavirus pandemic which had already had a devastating impact in other parts of the world, disrupting daily life and bringing illness and death. What lay ahead for Australia was unknown, and feared.
2 Amongst the passengers were Susan and Henry Karpik from Figtree, a tranquil suburb of Wollongong in New South Wales. Mr Karpik fell ill during the voyage to the disease caused by the virus, although whether he contracted the disease on board or before boarding is in dispute. He later nearly died – he was intubated, ventilated and placed into an induced coma, and spent nearly two months in hospital. Mrs Karpik says that she also contracted the disease – that being in dispute, although her symptoms were mercifully relatively minor. Mrs Karpik endured witnessing the suffering of her husband, without being able to be by his bedside for a long period because she was in isolation herself after the voyage. She says that the impact on her mental health has been significant. Many other passengers fell ill and some later died. The cruise itinerary was abandoned on 15 March 2020 with the ship returning to Sydney three days early.
3 Arising out of those broadly sketched events, Mrs Karpik, as lead applicant, commenced a representative proceeding against the owner and operators of the vessel in which she seeks damages for personal injuries and distress and disappointment of more than $300,000. The group members on whose behalf the proceeding is brought include passenger group members, being passengers on the voyage who are not deceased, executor group members, being executors of passengers who died from having contracted coronavirus on the voyage, and close family group members, being close family members of passengers on the voyage who died or became severely ill from contracting coronavirus on the voyage. The matter proceeded to trial on only Mrs Karpik’s claim on the basis that a number of common issues of fact and law would, in that process, also be decided in respect of all group members.
4 Mrs Karpik’s causes of action, as ultimately advanced, noting that certain pleaded parts of the case were not pressed in closing submissions, are the following.
5 First, she relies on s 61 of the Australian Consumer Law (ACL, being Sch 2 of the Competition and Consumer Act 2010 (Cth) (CCA)) by which, she says, the respondents guaranteed that the services that they provided to Mrs Karpik and other passengers, being the services necessary for the cruise, would be reasonably fit for the intended purpose of a safe, relaxing and pleasurable holiday from which they would come back feeling refreshed and reinvigorated. She says that the respondents also guaranteed that the services would be of such a nature, and quality, state or condition, that they might reasonably be expected to achieve that result, namely a safe, relaxing and pleasurable holiday from which she and the other passengers would come back feeling refreshed and reinvigorated.
6 Mrs Karpik says that the services supplied by the respondents failed to comply with those guarantees in a number of respects and were nowhere near reasonably fit for the intended purpose, or as might reasonably be expected to achieve the desired result. She says that the purpose was not achieved. Mrs Karpik says that far from having a safe, relaxing and pleasurable holiday from which she would come back feeling refreshed and reinvigorated:
(1) Mr Karpik contracted COVID-19 early on in the voyage;
(2) Mrs Karpik spent a considerable period of time caring for her husband on the voyage, particularly during the latter part of the cruise when his condition significantly worsened;
(3) by 15 March 2020, there was an outbreak of respiratory illness on board “with everyone febrile”;
(4) ultimately, many hundreds of passengers and crew contracted COVID-19 and a significant number of passengers died;
(5) she was, in addition to her husband, one of the passengers who contracted COVID-19;
(6) Mr Karpik nearly died from COVID-19 so, as well as dealing with her own illness, Mrs Karpik had to endure witnessing the suffering of her husband, without being able to be by his bedside for a long period because she was in isolation herself after the voyage.
7 Mrs Karpik says that it is not necessary, in the absence of any suggestion that the failure to achieve the purpose was unconnected with the services, to analyse the deficiencies in the services. However, to the extent that that may be necessary or helpful, on behalf of Mrs Karpik and the other group members it is contended that the services were deficient in particular respects. For reasons that are not clear to me, those alleged deficiencies are not the same as the respects in which it is alleged the respondents were negligent, to which I will come. Be that as it may, the particular deficiencies that the applicant relies on in respect of failure to comply with the statutory purpose and result guarantees are these:
(1) Pre-embarkation screening of passengers and crew for the voyage was deficient in that:
(a) There were large numbers of passengers who had travelled from jurisdictions with large numbers of confirmed cases of COVID-19 who were not refused to board and were not subject to any further screening;
(b) Passengers who were symptomatic, but had not travelled from or through one of the countries identified on the respondents’ pre-embarkation health declaration, were permitted to board and were not subject to any additional screening;
(c) The additional screening of passengers who had travelled from or through the identified countries was ineffective because COVID-19 could be transmitted by persons who are asymptomatic or pre-symptomatic;
(d) The passports of passengers and crew were not checked to ensure that the information that they provided in their health declarations was correct; and
(e) There were no temperature checks of passengers and crew, which checks would have detected the most common symptom for COVID-19.
(2) Hand hygiene: The measures adopted by the respondents to improve hygiene by installing additional hand sanitising stations and reducing the use of common utensils were ineffective to reduce the transmission of COVID-19 because fomite transmission was a minor contributor to transmission.
(3) Cleaning: For the same reason, the measures adopted to increase the level of cleaning on-board by, for example, increasing the concentration of disinfectant, were ineffective to reduce transmission.
8 Mrs Karpik submits that it is highly doubtful whether there could have been a safe cruise departing on 8 March 2020 with the result that the cruise should have been cancelled and the passengers refunded their fares. In that regard, she says the following:
(1) there is an increased risk of an outbreak of a respiratory virus like COVID-19 on board cruise ships;
(2) the respondents were well aware of the principal characteristics of coronavirus well before 8 March 2020;
(3) the respondents had already experienced two coronavirus outbreaks on cruise ships operated by them, the Diamond Princess and the Grand Princess, the consequences of which were catastrophic;
(4) the possibility of a further outbreak, including on the Ruby Princess, was very real;
(5) the respondents offered all passengers departing on cruises leaving on 9 March 2020 and thereafter a full refund or credit because of the risks of coronavirus, yet they made no such offer in respect of the Ruby Princess cruise in question;
(6) the circumstances of the immediately preceding cruise of the Ruby Princess were such as to create a heightened risk;
(7) when the Ruby Princess departed on the voyage in question, the respondents knew that there were insufficient supplies of crucial medical equipment on board – particularly face masks – to deal with any coronavirus outbreak; and
(8) on 13 March 2020, the respondents announced a decision to cancel all their cruises worldwide but have offered no explanation of their decision not to cancel the cruise in question which departed on 8 March 2020.
9 Secondly, Mrs Karpik contends that the respondents contravened the prohibition on misleading or deceptive conduct in s 18 of the ACL (there had also been reliance on s 29(1)(b) but that was not pressed in closing submissions). She relies on the respondents’ promotional and marketing material which advertised the cruise under the trademark “come back new”, an email to passengers that reiterated a commitment to safety including by implementing increased monitoring, screening and sanitation protocols to protect the health of guests, and that passengers were invited to board the ship without any accompanying health warning from the respondents. She says that that conduct gave rise to “safe to board”, “protection”, “best practices” and “pleasurable cruise” representations which were misleading or deceptive, or likely to mislead or deceive, contrary to ACL s 18.
10 Thirdly, in reliance on s 60 of the ACL which guarantees that certain services are rendered with due skill and care, and the tort of negligence, Mrs Karpik says that the respondents owed her a duty of care to take reasonable precautions to protect her from illness and from suffering mental harm on account of her husband’s illness. She says that the reasonable precautions that a person in the respondents’ position would have taken are the following:
(1) cancel the cruise;
(2) alternatively:
(a) warn passengers that the risk of contracting COVID-19 on the cruise was heightened as compared to the community generally and to cruise ships generally;
(b) screen passengers and crew for relevant symptoms and not permit travellers with such symptoms to board regardless of what countries they had recently travelled from or through;
(c) reduce the number of passengers on board and take steps to ensure that appropriate physical distancing was observed;
(d) isolate guests and crew members with relevant symptoms for 14 days and isolate their roommates for 14 days in separate cabins;
(e) maintain sufficient medical supplies onboard, and in particular face masks so that medical staff, symptomatic passengers and their close contacts could be provided with face masks;
(f) keep up-to-date with and implement all relevant guidelines and protocols; and
(g) consistent with those guidelines, isolate and quarantine passengers and crew who were experiencing symptoms that were consistent with COVID-19; or
(3) further alternatively, warn passengers that the risk of contracting COVID-19 on the cruise was heightened as compared to the community generally and to cruise ships generally and that the reasonable precautions set out in (2)(b)-(g) could or would not be implemented.
11 Broadly stated, the respondents contend that Mr Karpik did not contract COVID-19 on board and that Mrs Karpik never contracted COVID-19 at all. On the s 61 claims, they say that the fundamental reason why Mrs Karpik’s case fails is that no purpose or desired result was ever communicated to the respondents, but that their services were in any event not relevantly deficient. On the s 18 case, they say that the communications relied upon by Mrs Karpik could not be reasonably interpreted as giving rise to the specific representations pleaded. On the negligence case, they deny that they owed passengers a duty of care that extends to protecting against the risk of contracting COVID-19 and say that, even if they did, they did not breach their duty of care essentially because they complied with all relevant guidelines of various peak health bodies.
12 This case generated a substantial volume of evidence. For ease of future reference, I have included document identity references to the evidence in square brackets in these reasons for judgment. The references do not form part of the reasons for judgment. They are not exhaustive of the evidence that I have considered in relation to, or that is supportive of, the findings to which they relate. I mention also that there are colour graphics in these reasons for judgment that will make limited sense in black and white, so they are best read in colour.
13 Mrs Karpik was 69 years of age and had been married to Mr Karpik for nearly 50 years at the time of the cruise. She had retired from nursing but continued to work part-time as an official visitor under the Mental Health Act 2007 (NSW).
14 Mr Karpik, a retired police officer, was 72 years of age. He was sight-impaired to such a degree that he is described as “legally blind.”
15 Mr and Mrs Karpik both gave evidence. Mrs Karpik also relies on the evidence of an additional seven lay witnesses who were all fellow passengers on RU2007, her treating psychiatrist, Dr McMahon, and six expert witnesses. I will identify the expert witnesses in section B.3 below. The lay witnesses gave evidence of their experiences on the cruise. Several of them were cross-examined.
16 At all material times, the first respondent, Carnival plc, was incorporated in the United Kingdom. It was also a registered foreign company in Australia and carried on business in Australia with a registered office in New South Wales. It was the time charterer of the Ruby Princess. [CRT.500.004.0001 [3]]
17 Carnival traded as “Princess Cruises” and “Carnival Australia.” It employed shore-based personnel in Sydney who were involved in, amongst other things, managing the arrival and departure of the Ruby Princess and issuing instructions about the conduct of the voyage. Princess Cruises, P&O Australia, Holland America Line and Seabourn are all brands of the Holland America Group (HA Group).
18 The second respondent, Princess Cruise Lines Ltd (PCL), was incorporated in Bermuda. It owned and operated the Ruby Princess, as well as other passenger liners which feature in what follows, including the Diamond Princess and the Grand Princess. [CRT.500.004.0001 [4]] The Ruby Princess was time chartered by PCL as owner to Carnival as charterer for the period from 23 October 2019 to 2 May 2020.
19 Although the respondents foreshadowed in opening that they would urge the Court to draw a distinction between Carnival and PCL as reflected in their pleaded defence, no such distinction was drawn in closing either in writing or orally. Indeed, it is part of the agreed facts that Mrs Karpik contracted with “the respondents.” [JNT.002.001.0001 [3]] Accordingly, save where it is necessary to distinguish between Carnival and PCL, they are referred to hereunder simply as the respondents.
20 The Ruby Princess is a large, modern, ocean-going cruise ship. It has a range of indoor and outdoor venues, including shops, restaurants, a gymnasium, a theatre, a casino, cafes and bars, an outdoor cinema, swimming pools, an outdoor sports court and a mini golf course. The vessel is 290m in length, has a gross tonnage of 113,561mt, was launched in 2008, has 17 decks and is flagged in Bermuda. [LAY_SKA.003.001.0047 p 51]
21 Immediately preceding the voyage at the heart of this case, the Ruby Princess undertook a similar voyage from Sydney to New Zealand and back to Sydney. The voyage is referred to as RU2006. It ended in Sydney early on 8 March 2020. On that day, the passengers from that voyage disembarked and the passengers for the next voyage, referred to as RU2007, embarked.
22 On 15 March 2020, the Australian Government announced that from 16 March 2020 it would deny entry to cruise ships that had left foreign ports, but that there would be an exception for international cruise ships that had already departed their last foreign port and were headed to Australia prior to that time. For that reason, RU2007 was cut short and the Ruby Princess headed directly for Sydney, arriving very early on 19 March 2020. [CAU.001.014.4906]
23 The respondents relied on the evidence of 16 lay witnesses who were all from amongst the hotel crew on the vessel on RU2007. The highest ranking amongst them was Charles Arnoldus Verwaal, the Hotel General Manager. Mr Verwaal explained that he was the second most senior crew member on board after the Captain and equal in rank to the Chief Engineer and the Staff Captain. His responsibilities were confined to the hotel. He was responsible for operations and maintenance of the hotel through the management of six hotel departments, each led by a head of department who reported directly to him. Those departments were Entertainment, Food and Beverage, Housekeeping/Accommodation, Customer Services, Medical and Sanitation. [LAY_RES.001.001.0342 [14-15]]
24 The heads of the Housekeeping/Accommodation and Customer Services departments, Artur Manuel Ferreira and Loren Kerri Budd respectively, also gave evidence. Like Mr Verwaal, they were in their roles on both RU2006 and RU2007. None of the other department heads gave evidence, and no one from the Medical or Sanitation departments gave evidence. The other witnesses were from lower levels within the Food and Beverage and Housekeeping/Accommodation departments, and one was the Crew Manager. No shore-side personnel of either respondent gave evidence.
25 The result is that there was no witness evidence on a number of important issues. Those include the circumstances around and reasons for the respondents’ decision, first, on or about 5 March 2020 to offer full refunds on all cruises worldwide departing from 9 March 2020 and not, say, 8 March, and, second, on or about 13 March 2020 to suspend all cruises worldwide for an initial period of 60 days. They also include the likely burden on the respondents had they taken various precautions which the applicant alleges that they should have taken, for example, cancelling the cruise, conducting temperature screening of all passengers and crew before boarding, imposing a requirement of physical distancing between people where possible on board the vessel and isolating passengers and crew who presented with acute respiratory infection (ARI) and/or influenza-like illness (ILI) (each of which is referred to as an acute respiratory disease (ARD)). The applicant asks the Court to draw certain inferences from these gaps in the respondents’ evidence. I will deal with those at the appropriate places in canvassing the various issues below.
26 The parties relied on the evidence of a number of expert witnesses. It is convenient to introduce them, and which party called them at the outset.
27 The expert witnesses relied on by the applicant, and their respective fields of expertise, are as follows:
(1) Dr Enrico Parmegiani – Dr Parmegiani is a consultant psychiatrist. He holds a Bachelor of Medicine and a Bachelor of Surgery (Honours) from the University of Sydney, as well as a Diploma of Forensic Psychiatry from the NSW Institute of Psychiatry. Dr Parmegiani became a Fellow of the Royal Australian and New Zealand College of Psychiatrists in 1999 and since that time has consistently practiced in the field of psychiatry. At the time of trial, Dr Parmegiani worked in private practice as a consultant psychiatrist and independent medical examiner and was a Psychiatrist Member of the NSW Mental Health Review Tribunal and a Personal Injury Commission Medical Assessor.
(2) Dr Joseph Herrera – Dr Herrera is a medical physician specialising in the field of physical medicine and rehabilitation. He holds a Bachelor of Science from Rutgers University and a medical degree from Rowan University School of Osteopathic Medicine. Dr Herrera is certified by the American Board of Physical Medicine and Rehabilitation and has been employed for over twenty years as a medical practitioner and academic in that field. At the time of trial, Dr Herrera was System Chair of Physical Medicine and Rehabilitation within the Department of Rehabilitation and Human Performance and the Lucy G Moses Professor at the Icahn School of Medicine at Mount Sinai, New York, and was a physician at the Mount Sinai Center for Post Covid Care.
(3) Professor Joacim Rocklöv – Professor Rocklöv is an academic epidemiologist specialising in infectious diseases and, in particular, epidemiological analysis and modelling. He holds a PhD in Occupational and Environmental Medicine, a Master of Science in Mathematical Studies and a Bachelor of Science in Mathematics from Umeå University, Sweden. Professor Rocklöv’s background is in statistics, but he has 15 years of exclusive experience in epidemiology. At the time of trial, Professor Rocklöv was a Professor of Epidemiology and Global Health at Heidelberg University, Germany, and a guest Professor at Umeå University.
(4) Professor Annelies Wilder-Smith – Professor Wilder-Smith is a medical academic with particular expertise in emerging viral diseases, travel and tropical medicine, international health and public health. She holds a PhD in Infectious Diseases and Tropical Medicine from the University of Amsterdam, a Master in International Health from Curtin University, a Doctor of Medicine from the University of Heidelberg, a Diploma in Tropical Medicine and Hygiene from the London School of Tropical Medicine and various specialist accreditations in the fields of public health, tropical medicine, travel medicine and infectious diseases. At the time of trial, Professor Wilder-Smith was a Professor of Emerging Infectious Diseases at the London School of Hygiene and Tropical Medicine and an Adjunct Professor at the Institute of Social and Preventive Medicine at the University of Bern, Switzerland.
(5) Professor Edward Holmes – Professor Holmes is an academic of over 30 years’ experience and a specialist in the fields of virology, microbiology, genomics, genomic/molecular epidemiology and evolutionary biology, in particular in phylogenetics. He holds a Doctorate in Zoology from the University of Cambridge and a Bachelor of Science in Anthropology from the University of London. Professor Holmes was the first person globally to share and make public the genome sequence of SARS-CoV-2. At the time of trial, Professor Holmes was a Professor of Biology and Medicine at the University of Sydney and an Australian Research Council Australian Laureate Fellow.
(6) Professor Alison Kesson – Professor Kesson is a virologist, microbiologist and infectious diseases physician. She holds a PhD from the Australian National University and a Bachelor of Medicine and Surgery from the University of Sydney. At the time of trial, Professor Kesson was Head of Pathology and a physician in the Department of Infectious Diseases and Microbiology at the Children’s Hospital at Westmead and a Conjoint Professor in Child and Adolescent Health in the Sydney Institute for Infectious Diseases at the University of Sydney.
28 The expert witnesses relied on by the respondents, and their respective fields of expertise, are as follows:
(1) Associate Professor Hassan Vally – Associate Professor Vally is an applied epidemiologist and academic specialising in communicable diseases epidemiology with particular expertise in the analysis and interpretation of health data and the computation and communication of risk. At the time of trial, Associate Professor Vally was an Associate Professor at the School of Health and Social Development at Deakin University. Associate Professor Vally co-authored a report with Professors McCaw and Bennett, and the three of them participated in some of the joint reports with the applicant’s experts. However, of the three of them, only Professor Bennett was cross-examined on the basis that the co-authored report was to be taken as authored by her and the respondents would advance no point that Associate Professor Vally and Professor McCaw had not been cross-examined. (T336:35.)
(2) Professor James McCaw – Professor McCaw is a mathematical biologist and epidemiologist with a particular focus on infectious disease dynamics. At the time of trial, he was a Professor of Mathematical Biology at the Melbourne School of Population and Global Health and the School of Mathematics and Statistics, and Unit Head (Modelling and Simulation) at the Centre for Epidemiology and Biostatistics at the University of Melbourne. As mentioned, Professor McCaw was not cross-examined on the same basis that Associate Professor Vally was not cross-examined.
(3) Dr Anthony Samuels – Dr Samuels is a consultant psychiatrist. He holds a Bachelor of Medicine and Surgery and a Master of Criminology and is a foundation member of the Royal Australian and New Zealand College of Psychiatrists Faculty of Forensic Psychiatry. Dr Samuels has more than 20 years’ professional experience in the field of psychiatry and, at the time of trial, was engaged in private practice and was an Adjunct Associate Professor at the School of Psychiatry at the University of New South Wales.
(4) Associate Professor Laith Yakob – Associate Professor Yakob is an infectious diseases epidemiologist. He holds a PhD in Mathematical Modelling from the University of Oxford, a Master of Science in Modern Epidemiology from the Imperial College, London and a Bachelor of Science in Parasitology from the University of Glasgow. Much of Associate Professor Yakob’s current research focuses on COVID-19, with an emphasis on modelling. At the time of trial, Associate Professor Yakob was an Associate Professor of Infectious Diseases in the Department of Disease Control at the London School of Hygiene and Tropical Medicine, an advisor to Pfizer and the European Centre for Disease Prevention and Control and a collaborator with the Centre for Mathematical Modelling of Infectious Diseases COVID-19 Working Group.
(5) Professor David Paterson – Professor Paterson is an infectious diseases physician and academic. Professor Paterson holds a PhD and a Bachelor of Medicine and Surgery from the University of Queensland and a Postgraduate Diploma in Clinical Epidemiology and Biostatistics, and is Australia’s most cited infectious diseases physician. Professor Paterson is a Fellow of the Royal Australian College of Physicians (Infectious Diseases) and a Fellow of the Royal College of Pathologists (Clinical Microbiology). At the time of trial, Professor Paterson was a Professor of Medicine and Director of the clinical research network Advancing Clinical Evidence in Infectious Diseases at the National University of Singapore.
(6) Professor Catherine Bennett – Professor Bennett is an academic epidemiologist specialising in infectious disease epidemiology, public health and community transmission. She holds a PhD in population genetics and applied biostatistics from La Trobe University, a Master in Applied Epidemiology specialising in communicable disease epidemiology from the Australian National University and a Bachelor of Science (Genetics and Microbiology) (Honours) from La Trobe University. At the time of trial, Professor Bennett was the Chair in Epidemiology at Deakin University.
(7) Dr Peter Chen – Dr Chen is a physician and academic specialising in pulmonary and critical care. Dr Chen holds a medical degree from Baylor College of Medicine and a Bachelor of Science (Honours) from the University of Texas at Austin. Dr Chen’s research focuses upon mechanisms of lung injury and, in recent years, translational, epidemiological and treatment studies of COVID-19 and the impact of COVID-19 infection on pulmonary dysfunction. At the time of trial, Dr Chen was the Director of the Division of Pulmonary and Critical Care Medicine and a Professor in the Department of Medicine (Pulmonary and Critical Care Division) at Cedars-Sinai Medical Center, Los Angeles, and a Professor-in-Residence at the University of California, Los Angeles.
29 The following table summarises the joint reports that were provided by the expert witnesses as the product of their discussions in conclave and relied on by the parties in evidence. Those discussions, and the production of the joint reports, were facilitated by an independent barrister appointed by the Court and paid for by the parties.
Report | Contributors | Report Topic |
Joint Expert Report 1 dated 16 September 2022 | Professors Paterson, Wilder-Smith, Bennett, McCaw and Associate Professor Vally | What were the characteristics of coronavirus as at March 8, 2020, including what was known at that time? |
Joint Expert Report 2 dated 16 September 2022 | Professors Wilder-Smith, Rocklöv, Bennett, McCaw and Associate Professor Vally | How contagious was COVID-19 as at 8 March 2020, including what was known at that time? |
Joint Expert Report 3 dated 16 September 2022 | Professors Wilder-Smith, Rocklöv, Bennett, McCaw and Associate Professor Vally | Was the risk of contracting COVID-19 on a cruise ship compared to the risk of contracting COVID-19 in the community generally heightened as at 8 March 2020, including what was known at that time? |
Joint Expert Report 5 dated 16 September 2022 | Professors Wilder-Smith, Rocklöv, Bennett and McCaw and Associate Professor Vally | Having regard to what was known or knowable as at 8 March 2020, was the risk of contracting COVID-19 on RU2007 heightened compared to the risk of contracting COVID-19 on another cruise ship at that time? |
Joint Expert Report 6 dated 16 September 2022 | Professors Wilder-Smith, Holmes, Rocklöv and Paterson and Associate Professor Yakob | The probability that Mr Karpik was infected prior to boarding RU2007 |
Joint Expert Report 7 dated 14 September 2022 | Professors Paterson and Kesson | What is the likelihood that Mrs Karpik contracted COVID-19 before 20 April 2020? |
Joint Expert Report 8 dated 15 September 2022 | Professors Wilder-Smith and Paterson and Associate Professor Yakob | If it is likely that Mrs Karpik was infected with COVID-19 before 20 April 2020, what is the likelihood that she was infected on RU2007 or from another passenger on RU2007, including Mr Karpik? |
Joint Expert Report 9 dated 16 September 2022 | Professors Paterson and Wilder-Smith | Whether social distancing was known to reduce the spread of COVID-19 by 8 March 2020? Whether social distancing would have made a difference to the risk of Mrs Karpik contracting COVID-19 during the voyage? |
Medico-Legal (Psychiatry) Experts Joint Conference Report dated 10 September 2022 | Dr Parmegiani and Dr Samuels | Eight topics related to Mrs Karpik’s psychiatric health. |
Medico-Legal (Long COVID) Experts Joint Conference Report dated 13 September 2022 | Dr Herrera and Dr Chen | Eight topics related to “Long COVID” and whether and the extent to which Mrs Karpik suffers from the condition. |
30 In late 2019, a novel coronavirus emerged at Wuhan in China which came to be named severe acute respiratory syndrome coronavirus 2, or SARS-CoV-2 (hereafter, also the virus or coronavirus), and the disease caused by it was named coronavirus disease 2019, or COVID-19 – recognising that, depending on the context, it may not be relevant to distinguish between the virus and the disease. The virus had not previously been seen in humans indicating negligible, if any, immunity in the population. The characteristics of the virus and COVID-19 have largely been agreed between the relevant experts. What follows is drawn from their joint reports and the parties’ statement of agreed facts.
31 SARS-CoV-2 is a beta-coronavirus and is related to (ie, shares about 86% genetic similarity with) the SARS coronavirus that caused a major SARS outbreak in 2003, SARS-CoV. Although, SARS-CoV-2 has undergone further viral evolution with further variants, as at 8 March 2020, only the ancestral strain (ie, the Wuhan strain) was circulating. The first published reports of human-to-human transmission of SARS-CoV-2 were made available in late January 2020. [JNT.001.001.0001 [1]-[3]]
B.4.2 Characteristics and transmission
32 Transmission of coronavirus can occur via respiratory droplets from an infected person, aerosol transmission and contact with objects that have been contaminated with respiratory droplets from an infected person. The latter is referred to as fomite transmission. [CRT.500.004.0001 [11]]
33 A respiratory droplet is a small aqueous droplet >10µm in diameter (although there is a continuous distribution between small particles <5µm to large particles >15µm) consisting of saliva and other matter derived from respiratory tract surfaces. Respiratory droplets are produced naturally as a result of breathing, speaking, sneezing, coughing or vomiting, so they are always present in a person’s breath, but certain functions such as speaking and coughing increase their number. Coughing, sneezing and singing also result in a more forceful expulsion of such droplets. [CRT.500.004.0001 [13]; JNT.001.001.0001 [22]] When a person is infected, these droplets carry virus and transmit infection. The largest droplets settle out of the air rapidly, within seconds to minutes. Infection via contact with respiratory droplets is referred to as respiratory droplet transmission.
34 The smallest of the aqueous droplets – particles that are <5µm in diameter – rapidly dry and become aerosol particles. [EXP_SKA.003.003.0226 [42]; EXP_SKA.001.001.0001 [23]] Aerosols can remain in the air for longer periods of time (up to hours, depending on ventilation) and travel further than respiratory droplets. Aerosol transmission is distinct from respiratory droplet transmission and refers to the presence of viruses within small droplet nuclei.
35 Transmission occurs in all three modes of transmission via inhalation of large respiratory droplets and smaller aerosol droplets or particles, settling of large respiratory droplets and/or smaller aerosol droplets or particles on exposed mucous membranes in the mouth, nose or eye by direct splashes and sprays, or touching mucous membranes with hands that have been soiled either directly via virus-containing respiratory fluids or indirectly by touching surfaces with virus on them. Point of entry is mainly through the nose. [CRT.500.004.0001 [14]]
36 Once infectious droplets and particles are exhaled by an infected person, they move outward from the person (the source). The highest concentration of droplets is in close proximity to the source. [CRT.500.004.0001 [16]]
37 Risk of transmission is greatest within 1.5 to 2 metres as this is where the concentration of these droplets and particles is greatest. The risk of infection decreases with increasing distance from the source of infection and increasing time after exhalation. Enclosed spaces with inadequate ventilation within which the concentration of exhaled respiratory fluids can build up in the air space increases the risk of infection. Another factor is prolonged exposure to these conditions, typically more than 10-15 minutes. [CRT.500.004.0001 [17]; JNT.001.001.0001 [22 (g)]]
38 The relevant experts agree that the characteristics of respiratory droplets and principles of transmission of respiratory droplets constitute standard knowledge in the field of epidemiology and outbreak investigations that preceded both the COVID-19 and the SARS outbreaks. [JNT.001.001.0001 [23]]
39 As at 8 March 2020, the median incubation period for the virus was considered to be 5-6 days, ranging from 0-14 days. A paper was published in January 2020 in respect of an outbreak in Germany that month which reported a median incubation time of 4 days, with a range of 2.3 to 4.4. [JNT.001.001.0001 [7]-[8]]
40 Coronavirus can be transmitted in the ways identified above by both symptomatic and asymptomatic infected persons. [CRT.500.004.0001 [20]] Asymptomatic infection occurs when a person is infected but develops no symptoms. [JNT.001.001.0001 [9]]
41 The relevant experts agree that the existence of asymptomatic transmission was known from three peer-reviewed reports published before 8 March 2020, but the extent of asymptomatic transmission was not known. As at 8 March 2020, asymptomatic transmission was not thought to be a major driver of transmission. After 8 March 2020, one of the reports was corrected to be a pre-symptomatic case. [JNT.001.001.0001 [24]] A pre-print study (ie, not yet peer reviewed) was published on 20 February 2020 that documented the proportion of asymptomatic infections to be 18%, although after 8 March 2020 it became known that a substantial proportion (20-45%) of people infected with the ancestral Wuhan strain do not develop symptoms. [JNT.001.001.0001 [11]-[12]]
42 A risk assessment internal to the respondents dated 25 February 2020 shows that the respondents were aware of asymptomatic transmission at that stage, although the “extent” of such transmission was not known. [PCL.001.006.7128] It was also put to Mrs Karpik in cross-examination as a positive proposition that as at 8 March 2020 she knew that the virus could be transmitted by someone who had no symptoms, and that it was said in the news that there was a theory that on the Diamond Princess transmission had occurred from asymptomatic people (T142:25-30). Although Mrs Karpik said that she was not sure that she had that knowledge at that time, the fact of knowledge of asymptomatic transmission having been put as a positive assertion grounds the inference that the respondents, who had reason to know far more about the virus and its transmission than an ordinary passenger such as Mrs Karpik, had that knowledge at that time. (See [122] below on the questions of assertions in cross-examination amounting to admissions against interest.)
43 The experts also agree that by February 2020, it was known that the serial interval of COVID-19 is shorter than its median incubation period. That indicates that a certain proportion of secondary transmission occurs prior to illness onset. Pre-symptomatic transmission plays an important role in transmission dynamics of COVID-19. [JNT.001.001.0001 [25]]
44 Coronavirus can cause the following symptoms: fatigue, cough, shortness of breath and fever. In cases of severe and critical illness, the virus can cause respiratory failure and an inability to properly breathe without a respirator, septic shock, multiple organ dysfunction/failure and death. [CRT.500.004.0001 [22]-[23]]
45 On 18 February 2020, China’s Centre for Disease Control published their data of the first 72,314 cases including 44,672 confirmed cases. About 80% of the confirmed cases were reported to be mild disease or less severe forms of pneumonia, 13.8% severe and 4.7% critically ill. The study also noted that nearly half (49%) of critically ill patients died. Initial estimate of the overall case fatality rate was around 2.2%. Severe disease is defined as those with dyspnoea, hypoxia, or >50% percent lung involvement on imaging. Critical disease is defined as respiratory failure, shock, or multi-organ dysfunction. [JNT.001.001.0001 [15]]
46 Acute respiratory distress syndrome (ARDS) is the major complication in patients with severe disease and can manifest shortly after the onset of dyspnoea. Other complications of severe illness include thromboembolic events, acute cardiac injury, kidney injury, and inflammatory complications and various others. [JNT.001.001.0001 [16]]
47 Some people who have been infected with the virus can experience a condition known as Long COVID which is where common COVID-19 symptoms such as fatigue, shortness of breath or cognitive dysfunction last either for at least four weeks after infection or at least three months after infection and are present for at least two months. Long COVID symptoms may improve or relapse over time. [CRT.500.004.0001 [28]-[29]]
48 There is currently no biomarker or diagnostic test for Long COVID. The diagnosis of Long COVID is based upon an evaluation of a person’s symptoms. Often, this evaluation occurs in conjunction with a physical examination and imaging or functional testing. Careful consideration of pre-existing condition is important in evaluating someone for Long COVID to ensure that the symptoms are not from previously known diseases. Clinicians need to also consider new diagnoses that are not considered Long COVID but are contributing to the patient’s symptoms. [CRT.500.004.0001 [30]]
B.4.4 The respondents’ knowledge
49 It is common ground that by 5 March 2020, the respondents knew or ought reasonably to have known the following:
(1) coronavirus can be transmitted via objects and bodily fluids contaminated with the virus;
(2) coronavirus is capable of human-to-human transmission;
(3) human-to-human transmission of coronavirus can occur via droplets and fomites from an infected person;
(4) an infected person may be asymptomatic;
(5) coronavirus can cause the following symptoms: lethargy, coughing, shortness of breath, fever, and inability to properly breathe without a respirator, and death;
(6) the symptoms of coronavirus may be similar to, or the same as, symptoms caused by an ARI and/or ILI;
(7) the mortality rate in people infected with coronavirus increases with age;
(8) people who are elderly or who have comorbid conditions are more susceptible to becoming severely ill or dying due to coronavirus than people who are not elderly or have no comorbidities;
(9) coronavirus is contagious;
(10) there was no vaccine for coronavirus at any time before completion of the voyage. [CRT.500.004.0001 [31]]
50 The respondents deny as a fact, and they deny that before the voyage they knew, that the risk of contracting coronavirus on a cruise ship was higher than the risk in the community generally. I deal with this dispute in section B.5.3 below.
B.4.5 Prevalence of coronavirus prior to 8 March 2020
51 On 30 January 2020, the World Health Organization (WHO) declared the outbreak of coronavirus a Public Health Emergency of International Concern. The respondents knew this. [CRT.500.004.0001 [32]]
52 By 8 March 2020, based on the “WHO Coronavirus Disease 2019 (COVID-19) Situation Report – 47”:
(1) there had been over 100,000 confirmed cases of coronavirus reported globally;
(2) over 90 countries had confirmed cases of coronavirus;
(3) countries that had over 100 confirmed cases included: the United Kingdom, the United States of America, France, Germany, Italy and The Netherlands; and
(4) there had been local transmission of coronavirus reported in more than 40 countries including each of the countries listed above as well as Canada and Spain. [CRT.500.004.0001 [33]]
53 By 8 March 2020, based on the Australian Government, Department of Health, “Communicable Diseases Intelligence, COVID-19, Australia: Epidemiological Report 6” (published on 11 March 2020), in Australia:
(1) there were over 70 confirmed cases of coronavirus, including two deaths;
(2) 16 cases had direct or indirect links to mainland China;
(3) 10 cases were among the Diamond Princess cruise ship passengers repatriated from Japan;
(4) 16 cases had direct or indirect links to the Islamic Republic of Iran;
(5) 14 cases had a recent travel history to other countries; and
(6) there were approximately 40 reported cases of coronavirus in NSW. [CRT.500.004.0001 [34]-[35]]
54 On 11 March 2020, several days into the voyage of the Ruby Princess, the WHO declared COVID-19 a pandemic. In a statement that day, the Director-General of the WHO stated that “we are deeply concerned both by the alarming levels of spread and severity, and by the alarming levels of inaction.” Back on 23 February 2020, Dr Grant Tarling, the respondents’ Senior Vice President and Chief Medical Officer, had stated that he expected that COVID-19 would soon become a pandemic. [SKA.005.001.0264; PCL.002.025.1105] The evidence shows that Dr Tarling was involved since January 2020 with the United States’ Centers for Disease Control and Prevention (CDC) and industry groups (including the Cruise Line International Association, or CLIA) in developing response protocols and communications concerning the developing coronavirus situation. [PCL.001.006.4630 p 2]
55 The evidence also shows that there were comprehensive situation reports about developments in relation to coronavirus that were sent to the respondents’ executives on an almost daily basis through, relevantly, January to March 2020. These reports provided updates with respect to various vessels in the respondents’ fleet, such as number of infections on board, port of call restrictions, itinerary changes and the risk of certain passengers joining; as well as more general updates about the global situation with respect to the spread of coronavirus, such as case and fatality numbers. [SBM.010.002.0001 fn 164]
B.5.1 Previous coronavirus outbreaks on cruise ships
56 Prior to the voyage in question, there had been cases of coronavirus on board the Diamond Princess and the Grand Princess, both of which are cruise ships owned by PCL. [CRT.500.004.0001 [36]] The outbreaks on those vessels are relevant because of the respondents’ knowledge of the material circumstances of those outbreaks. There had also been an outbreak of ARI and ILI on board the cruise of the Ruby Princess immediately preceding Mrs Karpik’s cruise, namely voyage RU2006. That is relevant because of what it might say about the risk of coronavirus being on the vessel and being carried over to voyage RU2007.
57 On 20 January 2020, the Diamond Princess departed Yokohama Port in Japan on a 16-day round trip itinerary, including travelling to Hong Kong on 25 January 2020. There were approximately 3,700 passengers and crew on board. [CRT.500.004.0001 [37]-[38]]
58 On or about 1 February 2020, one passenger from Hong Kong who travelled on the Diamond Princess cruise for five days from 20 January and disembarked in Hong Kong on 25 January 2020, tested positive for coronavirus. By about 4 February 2020, 10 people on board the Diamond Princess had tested positive for coronavirus, including two Australian guests, three Japanese guests, three guests from Hong Kong, and one guest from the United States, in addition to one Filipino crew member. The number of infected passengers and crew steadily increased and by 20 February 2020, over 600 people who had been on the Diamond Princess cruise had tested positive for coronavirus. [CRT.500.004.0001 [39]-[40], [43]-[45]]
59 On or about 1 March 2020, a passenger who had contracted coronavirus on the Diamond Princess cruise became the first Australian to die due to coronavirus. [CRT.500.004.0001 [46]]
60 By 5 March 2020, the respondents knew of the matters set out in the preceding paragraphs concerning the Diamond Princess. [CRT.500.004.0001 [49]]
61 By 7 March 2020, over 600 passengers who had been on the Diamond Princess cruise had tested positive for coronavirus, over 300 of those confirmed cases showed no symptoms of coronavirus at the time of specimen collection for testing, and more than five passengers had died due to coronavirus. [CRT.500.004.0001 [47]]
62 By 8 March 2020, when the Ruby Princess departed Sydney, seven passengers from the Diamond Princess cruise had died due to coronavirus, nearly 700 (over 18%) of the approximately 3,700 passengers who had been on the Diamond Princess cruise had tested positive for coronavirus, and over 40% of the people on the Diamond Princess cruise who tested positive for coronavirus were asymptomatic at the time of testing. [CRT.500.004.0001 [48]; PUB.005.001.0425]
63 The respondents knew of the matters set out in the preceding two paragraphs by the evening of 8 March before the Ruby Princess departed from Sydney. [CRT.500.004.0001 [50]]
64 From 11 to 21 February 2020, the Grand Princess sailed on a roundtrip passenger cruise from San Francisco, California, to Mexico and Hawaii (the first trip). On 21 February 2020, the Grand Princess departed San Francisco on a second roundtrip voyage to Hawaii, carrying approximately 2,422 guests and 1,122 crew. [CRT.500.004.0001 [51]-[52]; PCL.001.002.1985]
65 By 4 March 2020, at least one passenger from the first trip had tested positive for coronavirus and at least one had died from coronavirus. On or about 4 or 5 March 2020, after PCL was notified of the positive test, it commenced cancelling all social activities planned for the remainder of the second voyage. [CRT.500.004.0001 [53]-[54]] By 5 March 2020, CDC had reported another positive case from the first trip and that one of the individuals was being treated in an Intensive Care Unit (ICU). [PCL.001.006.9323]
66 By 6 March 2020, over 20 passengers on the second trip of the Grand Princess had tested positive for coronavirus. [CRT.500.004.0001 [55]] By 7 March 2020, there were 11 positive cases from the first trip. [PCL.001.002.1985]
67 On 7 March 2020 at 5.00pm CT, ie, 9.00am on 8 March in Sydney, PCL reported to the press that of 45 guests and crew who were tested for the virus on the second trip, 21 people had tested positive, being two guests and 19 crew. The 45 people selected for testing was on the basis that they had presented with ILI on the voyage as they were regarded as the highest risk cohort and were required by the CDC to be tested. It was also reported that it was believed that the index case on the vessel, ie, the person who took the virus onto the vessel, was a guest on the first trip, and that the virus had spread from that person to other guests and crew. The problem for the second trip was that the crew remained on board. [PCL.001.003.6200]
68 The respondents knew of the matters recorded above about the Grand Princess cruises before the embarkation of passengers for voyage RU2007 in Sydney. [CRT.500.004.0001 [56]]
(3) Seven Nile River cruise ships
69 On 14 March 2020, the CDC reported that it was not only large cruise ships that had experienced coronavirus outbreaks. An outbreak on board a Nile River cruise with 171 passengers and crew resulted in 45 confirmed COVID-19 cases. Many of the passengers returned home before any notifications about COVID-19 were provided, potentially spreading the disease to their home communities. Evidence of COVID-19 transmission on board six similar Nile River cruise ships, each carrying approximately 100 passengers, was said to illustrate that even ships with moderate numbers of passengers and crew on board carried a substantial risk of disease transmission and outbreak. [PUB.010.003.0001]
(4) The Ruby Princess voyage RU2006
70 On 24 February 2020, the Ruby Princess departed Sydney on a cruise to New Zealand, returning to Sydney on 8 March 2020. There were approximately 3,000 passengers and 1,163 crew on board. The ship’s medical centre maintained an acute respiratory diseases log (ARD log) from which much of the data that follows is drawn. [CRT.500.004.0001 [57]-[58]]
71 During the cruise, 162 persons presented to the ship’s medical centre with ARI. Guests accounted for 150 of those people, and crew members, 12. [CRT.500.004.0001 [59]-[60]]
72 Of the crew members, 10 were recorded as having ARI and two as having ILI. Four crew members were tested for influenza A and B, but all of them tested negative. The remaining eight were not tested. [CRT.500.004.0001 [61]]
73 Of the guests, 134 were recorded as having ARI and 16 as having ILI. Only 26 guests were tested for influenza A and B, of whom seven tested positive and 19 tested negative. [CRT.500.004.0001 [62]]
74 When the Ruby Princess docked in Sydney on 8 March 2020 at the conclusion of the cruise, 360 passengers (8.8%) presented in response to an announcement calling for anyone with a travel history of concern or respiratory symptoms to present themselves for screening by NSW Health. Of those passengers, only nine were tested by NSW Health for the virus – three crew and six guests. All the tests were negative. [SBM.010.002.0001 [57]; CRT.500.004.0001 [64]]
75 It is unclear what role the ARI/ILI outbreak on voyage RU2006 had with regard to the outbreak of COVID-19 on RU2007. A number of observations can nevertheless be made.
76 First, the symptoms of ARI and ILI are also symptoms of COVID-19, so passengers and crew reporting with such symptoms may have had COVID-19, particularly considering that only nine people were tested for the virus and someone with COVID-19 may have no symptoms or mild symptoms such that they would not have been selected for testing. That was known by the respondents because of their Diamond Princess experience (see [62]-[63] above).
77 Secondly, over 1,100 of the approximately 1,200 crew on RU2006 stayed on board for RU2007. There was thus a considerable risk that if anyone amongst the crew on RU2006 was carrying the virus, they would take it onto RU2007. The respondents must be taken to have known of that risk because of their Grand Princess experience (see [67]-[68] above).
78 Thirdly, albeit that fomite transmission is not a principal means of transmission of the virus, if it was present on RU2006, there is a risk that it would cause an outbreak on RU2007. The respondents knew of that risk (see [49(1)] above).
79 Fourthly, while health screening was taking place on the vessel on 8 March at the end of RU2006, the respondents prepared a draft media statement in case any of the passengers or crew tested positive for the virus. From the draft statement and the email exchanges between officers of the respondents, it is apparent that the respondents planned to cancel RU2007 in the event that there was a positive case on RU2006. Moreover, a 100% refund and 100% future cruise credit would be offered to passengers in the event of a cancellation, as well as hotel accommodation in Sydney and “some incidentals” – possibly onward flights and accommodation. This was said to be “in line with what we are offering for Guests also impacted by Grand and Royal cancellations.” [PCL.001.004.4279] The reference to Royal is a reference to the Royal Princess which had its cruise departing a US port on 7 March 2020 cancelled because one crew member had transferred to it from the Grand Princess and the CDC required the crew member to be tested for coronavirus and that could not be done quickly enough.
80 The telling observation is that the respondents planned to immediately cancel RU2007 on one positive test being returned from RU2006, yet apparently did not consider cancelling RU2007, or even offering the passengers the possibility to cancel with a refund, even though there was a substantial ARI/ILI outbreak on RU2006. The respondents knew that a person could be infectious with very mild symptoms or even no symptoms at all and hence not be caught by the screening on RU2006, and only nine people from RU2006 were being tested for coronavirus. In other words, the respondents knew or ought to have known that there was a substantial risk of COVID-19 on RU2006 and that the testing of only nine people from the voyage was not likely to identify all positive cases, with the result that there was a heightened risk of the virus being on RU2007 compared with cruise ships generally.
B.5.2 Guidelines, protocols and procedures
81 Since the start of the coronavirus pandemic, governments and government-related institutions around the world have introduced protocols and guidelines aimed at reducing the spread of the virus. Some of those protocols and guidelines are directed at passenger liners, and others are relevant to the management of passenger liners.
(1) The Centers for Disease Control and Prevention
82 The CDC is a United States federal government agency. The CDC’s guidance is relevant not only because it is a leading public health agency internationally, but also because the respondents are headquartered in the USA and, as would be expected, monitored statements and advice issued by the CDC that was relevant to a cruise ship operator.
83 On 18 February 2020, the CDC revised its “Coronavirus Disease 2019 Guidance for Ships” (CDC COVID Ship Guidance). The respondents were aware of that information before the Ruby Princess departed from Sydney on 8 March 2020. The revised guidance included statements to the following effect: [CAU.001.107.0003]
(1) Early detection, prevention, and control of COVID-19 on ships is important to protect the health of travellers on ships and to avoid transmission of the virus by disembarking passengers and crew members who are suspected of having COVID-19.
(2) Commercial shipping, including cruise ships and other passenger vessels, involves the movement of large numbers of people in closed and semi-closed settings. This may facilitate the transmission of respiratory viruses from person-to-person through exposure to respiratory droplets or contact with contaminated surfaces.
(3) To reduce the spread of respiratory infections including COVID-19, it is recommended that ships encourage crew members and passengers to self-isolate and inform the on-board medical centre if they develop symptoms.
(4) Identifying and isolating passengers and crew with possible symptoms of COVID-19 as soon as possible is needed to minimise transmission of this virus.
(5) Because the signs and symptoms of COVID-19 are non-specific, people on board who have fever or ARI should be tested for influenza.
(6) Deny boarding of a passenger or crew member who is suspected to have COVID-19 infection based on signs and symptoms plus travel history in China or other known exposure at the time of embarkation.
(7) In addition to routine cleaning and disinfection strategies, ships may consider more frequent cleaning of commonly touched surfaces such as handrails, countertops, and doorknobs. The primary mode of COVID-19 virus transmission is believed to be through respiratory droplets that are spread from an infected person through coughing or sneezing to a susceptible close contact within about 6 feet. Therefore, widespread disinfection is unlikely to be effective.
84 On 14 March 2020, the CDC issued a “No Sail Order” for all commercial non-cargo passenger-carrying ships within its jurisdiction with the capacity to carry 250 or more passengers and crew with an itinerary anticipating an overnight stay on board or a twenty-four hour stay on board for either passengers or crew. The “No Sail Order” records that the CDC had previously recommended that travellers, particularly those with underlying health conditions, avoid all cruise ship travel worldwide, and that the US Department of State had issued guidance that US citizens should not travel by cruise ship. [PUB.010.003.0001]
(2) The World Health Organization’s Interim Guidance
85 On 24 February 2020, the WHO issued an interim guidance entitled “Operational considerations for managing COVID-19 cases and outbreaks on board ships” (WHO Interim Ship Guidance).
(3) NSW’s Enhanced COVID-19 Procedures for the Cruise Line Industry
86 On 23 February 2020, the “Enhanced COVID-19 Procedures for the Cruise Line Industry” (Enhanced NSW Cruise Procedures) introduced by the Chief Health Officer for New South Wales was provided to the respondents who were asked to confirm that each cruise ship docking in New South Wales was able to meet those procedures. The enhanced procedures document included statements to the following effect: [CAU.001.040.5818; CAU.001.040.6314]
(1) The recent outbreak of COVID-19 on the Diamond Princess cruise ship in Japan demonstrates the serious impact this disease can have in cruise ship environments.
(2) Each cruise ship vessel should ensure that they have sufficient supplies of materials to manage a respiratory outbreak on board, including: face masks, alcohol hand rub for ill passengers and crew, and personal protective equipment (PPE) for clinic staff.
(3) A respiratory outbreak is defined as >1% of people on board affected. Smaller numbers of cases with mild respiratory illness are expected and do not necessarily represent an outbreak.
(4) Passengers who may be infectious should be appropriately isolated.
87 By 7 March 2020, the respondents had received a revised version of the procedures put in place by the New South Wales Chief Health Officer for cruise ships dated 3 March 2020. The revised procedures included statements to the following effect: [PCL.001.005.6517; PCL.001.005.6518]
(1) Each cruise ship should ensure that they have sufficient supplies of materials to manage a respiratory outbreak on board, including face masks and alcohol hand rub for passengers and crew with ARI.
(2) Each ship should collect and retain for 14 days after each cruise in case required a log of where passengers and crew have travelled in the 14 days prior to embarkation – in order to facilitate this, it is strongly recommended that pre-embarkation screening of crew and passengers include a history of travel in the previous 14 days.
(3) Cruise ship staff should ensure that they actively identify passengers and crew with ARI – including cough, sore throat, fever or difficulty breathing – by making regular announcements throughout the cruise, inviting them to attend the clinic for assessment.
(4) Passengers with ARI/ILI who may be infectious should be appropriately isolated, and provided with alcohol hand rub and face masks. If sharing a cabin, roommates should be provided with alcohol hand rub and face masks, and educated on how to protect themselves.
(4) Federal Government regulation and guidance
88 On 1 February 2020, the Australian Government announced that it would not permit foreign nationals who had been in mainland China on or after 1 February 2020 to enter Australia for 14 days from the time of leaving or transiting through mainland China, and that Australian citizens and permanent residents who had been in mainland China were required to self-isolate for 14 days from the time they had left. The announcement also stated the following: [PUB.001.012.0001]
In particular, the changing epidemiology of the coronavirus in China and the uncertainty that remains around its transmission and virulence, mean the utmost precaution is warranted.
There is no basis for alarm. It is important to remember the risk to Australians is currently very low. We need to keep it that way.
89 On or about 6 February 2020, the Australian Health Protection Principal Committee (AHPPC) published a statement advising that transmission of the virus occurred “through close contact with an infected individual, mostly face-to-face or household contact” and that the virus could not “jump across a room or be carried for long distances in the air.” It was said that “the current evidence suggests that sick people early in their illness are the main driver of spread.” [PUB.005.001.0010]
90 On 29 February 2020, the Australian Government announced travel restrictions banning non-citizens (other than permanent residents) who had been in Iran on or after 1 March 2020 from entering Australia for 14 days from the time they had left or transited through Iran, and requiring Australian citizens and permanent residents to self-isolate at home for 14 days from the day they had left Iran. [PUB.001.013.0001]
91 By the end of February 2020, international arrivals from other countries identified as “high risk”, namely Cambodia, Hong Kong, Indonesia, Iran, Italy, Japan, Singapore, South Korea and Thailand, were not required to isolate, but were asked to monitor their health for a period of 14 days after their arrival to Australia. [EXP_RES.002.001.1458 [23]]
92 On 6 March 2020, the Australian Government Department of Health also issued the “National Protocol for Managing Novel Coronavirus Disease (COVID-19) Risk from Cruise Ships” (National Cruise Ship Protocol). The document included statements to the following effect: [PCL.001.003.0313]
(1) Given the population density, duration of cruises and the mixing patterns of people on board, there may be the spread of diseases from international travellers who pose human biosecurity risks to other travellers. It is therefore necessary to have enhanced surveillance and control measures among travellers.
(2) Respiratory illnesses (common cold and influenza) are some of the most common infections affecting people on cruise ships, and cases of COVID-19 aboard passenger ships have occurred. Because cases of seasonal influenza often occur on ships and sustained community transmission of COVID-19 has been observed, it is possible that passenger ships carrying thousands of people would have travellers with COVID-19.
93 By the time the Ruby Princess departed Sydney on 8 March 2020, no Australian government had utilised their extensive powers to restrict public gatherings, force the closure of businesses or impose conditions on entry into premises, such as limits on numbers, physical distancing, mask wearing, and so on.
(5) The respondents’ protocols, instructions and decisions
94 On 24 January 2020, the respondents issued version 1 of “Instructional Notice HEA/01/2020: Prevention and Control of 2019-Novel Coronavirus” which required all their vessels by 27 January 2020 to screen passengers and crew (by requiring passengers to complete Traveller’s Health Declarations) for recent travel history through Wuhan and to deny boarding to any of those persons with a fever or respiratory symptoms.
95 Instructional Notice HEA/01/2020 was updated several times, and various operational directives were issued by the HA Group detailing the operational procedures to be implemented by ships within the HA Group fleet (which include the Ruby Princess as a PCL vessel) to give effect to the requirements of Instructional Notice HEA/01/2020 as amended from time to time.
96 Revision 3 of Instructional Notice HEA/01/2020 was effective on 11 February 2020 when the Grand Princess embarked on its ill-fated voyage. That notice required pre-embarkation screening based on travel history and symptoms, preventing travellers from boarding if they had been in Mainland China, Macau or Hong Kong in the previous 14 days or had contact with a suspected or confirmed case of coronavirus and they reported relevant symptoms. [PCL.002.035.4484] Mrs Karpik observes that that form of screening based on travel history and reported symptoms did not work to keep the Grand Princess free of disease.
97 On 8 February 2020, Brian Badura, the Director of Global Public Relations & Strategic Initiatives of the respondent’s Seabourn brand emailed the other brands recording that Seabourn had had two instances where guests had not properly disclosed travel through China prior to boarding a vessel. In both cases, the guests checked “no” when asked if they had come via any prohibited areas. As a response, Mr Badura proposed including wording in the health declaration that shipboard staff would be scanning guest passports to verify that the information given was correct and threatening to disembark passengers who failed to disclose travel through prohibited areas. [PCL.002.035.0952]
98 Dr Tarling, the HA Group’s Chief Medical Officer, responded by supporting the new language in the health declarations but observed that, operationally, it was doubtful that check-in staff have the time or the knowledge to recognise Chinese entry and exit stamps and that “[t]here will not be many people admitting to China travel with the restrictions currently in place.” Mr Badura agreed and commented that the additional language was intended to be a deterrent and would hopefully encourage proper disclosures. [PCL.002.035.0952]
99 The respondents issued a protocol for “Identification, Assessment and Management of Patients for Coronavirus Disease 2019 (COVID-19)” in February 2020. It outlined procedures for the identification, assessment and management of patients presenting with an ARD for COVID-19. It covered both pre-embarkation screening and on-board management. [PCL.002.022.3537]
100 On or around 27 February 2020, the respondents distributed a document entitled “Enhanced Cleaning Protocols”, which required, inter alia, thermal screening at entrances to cruise terminals and increased frequency of sanitising of hand touch surfaces (every 15 minutes). [CRT.500.004.0001 [85]-[86]; CAU.001.107.0001]
101 As dealt with further below in dealing with communications sent to passengers before boarding for RU2007, on 5 March 2020 the respondents announced a change to their cancellation policies which would allow passengers booked on any cruises scheduled to depart from 9 March and thereafter (ie, the day after RU2007) to be given a full credit for a future booking.
102 Also on 5 March 2020, Revision 5 of Instructional Notice HEA/01/2020 was issued with effect from 7 March 2020. On 6 March 2020, an amended version of “Operational Directive PHS/04/20 – Coronavirus Boarding Instructions” was issued setting out revised boarding procedures and instructions for all ships within the HA Group fleet to give effect to Revision 5. [CAU.001.040.7332; CAU.001.018.0045; CAU.001.010.8754]
103 Pursuant to Revision 5, all passengers and crew were to be required to complete a standard form “Traveller’s Health Declaration”, which asked them to declare answers to specific questions. Based on the answers to the questions posed in the Traveller’s Health Declarations:
(1) travellers (and their close contacts) from or who had transited through mainland China, Hong Kong, Macau, South Korea or Iran (or a location subject to quarantine measures, such as certain municipalities in Italy) were to be denied boarding;
(2) travellers (and their close contacts) who had been in contact with a suspected or confirmed case of COVID-19 or a person monitoring for COVID-19 were to be denied boarding; and
(3) travellers from or who had transited through Italy, Japan, Singapore, Taiwan or Thailand were to undergo secondary health screening by medical staff in the terminal before being permitted to board, and were to be denied boarding (together with their close contacts) if they had fever, cough or difficulty breathing.
104 Revision 5 also provided that check-in staff should identify individuals travelling on Chinese, Hong Kong, Macau, South Korean and Iranian passports and reconfirm that they had not recently travelled from or through countries with active quarantine locations. There was no requirement that passports from other countries be checked, or that the passengers’ health declarations otherwise be checked for accuracy or truthfulness. [CAU.001.040.7332 p 3]
105 On 7 March 2020, the vessel’s Hotel General Manager was emailed an “Enhanced Public Health Protocols” document by Amanda Kent, Guest Experience & Product Development, which he distributed to his direct reports. That document is a marked up and amended version of the Enhanced Cleaning Protocols that was issued by the respondents on 27 February 2020. On 8 March 2020 at 7:51am, Mr Verwaal was emailed a clean version of the Enhanced Public Health Protocols document (ie, with the mark-up removed and changes accepted) by Livio Rebagliati, Public Health Support for HA Group. It had instructions under different headings which included the following: [CAU.001.001.0012; CAU.001.001.0013]
(1) Pre-cruise and during transfer to ship: basic hygiene guidance for passengers such as frequent hand washing and coughing into elbows, providing hand sanitisers before boarding buses and sanitising buses.
(2) Check-in/terminal: respiratory symptoms screening and detailed passport review at check-in by embarkation staff.
(3) On-board: detailed instructions for daily communication with all crew reinforcing basic hygiene practices including frequent hand washing, avoiding hand contact, refraining from serving drinks in reusable tumblers and encouraging crew to report any guests who show relevant signs of illness; detailed enhanced hygiene measures including staff monitoring hand washing at food venues, the provision of hand sanitiser and directing guests to wash their hands, increasing frequency of sanitising for high traffic hand touch surfaces in public areas, providing hand sanitiser in each guest stateroom, and propping doors open to reduce door handle touching.
(4) Crew on-boarding process in the terminal: All crew joining are screened for travel and for fever; confirm health questionnaire has been completed; detailed passport review; provide a small hand sanitiser for each crewmember.
106 Importantly, it deleted the requirement of either thermal or touchless temperature screening prior to embarkation. Thus, as at 8 March 2020, there was no longer any policy of, or instructions from, the respondents that there should be generalised temperature screening prior to allowing passengers or crew to board a vessel, despite a raised temperature being a defining symptom of COVID-19. As dealt with in more detail below (at [633]), in an email on 11 March 2020 about sourcing thermal cameras, Sture Myrell, the President of Carnival Australia, said to Jeremy Goodman, Carnival’s Supply Chain Director, that another cruise line, Royal Caribbean, had already implemented temperature screening and that “we are way behind.” He said that Carnival had been talking about it for four weeks and that it should now be a number one priority. [CAU.001.039.8328]
107 On 11 March 2020, the respondents issued an update of a document entitled “Health Advisory and Travel Safety Procedures.” It provided, inter alia, as follows: [PCL.001.007.2331]
Beginning in select embarkation terminals on March 7th and as soon as possible in all embarkation terminals, we will be temperature checking all guests embarking on our ships using temporal scanning thermometers. All guests presenting with a fever or flu-like symptoms will be denied boarding, irrespective of their recent travel history. All guests who are denied boarding due to sickness will be issued a full cruise credit or refund.
It is not clear on the face of the document what was updated in the document and when it was first issued. However, given that there are numerous references to 7 March 2020 in the document, it had to have been initially issued on or prior to that date.
108 On 13 March 2020, the respondents announced a decision to suspend all Princess cruising globally for an initial period of 60 days and to move each ship to a “soft layup” position. The respondents’ explanation for the decision was given by them as follows: [CAU.001.011.6854]
Princess has experienced several COVID-19 related incidents. In recognizing this we are committed to the safely (sic), health and wellbeing of our teammates, guests and the communities we visit globally. In an abundance of caution, in the spirit of Respect, Protect, Connect, we believe this important decision is the right thing to do. We also recognize the teams are currently stretched to the point where an additional quarantine incident would be extremely difficult to manage. The teams also need a break and time to refocus on building back the normal operation.
B.5.3 Coronavirus risk on cruise ships
109 An issue in the case that is relevant in different ways is the extent to which, if at all, there is a greater risk to a person contracting COVID-19 on a cruise ship than it is in the general community. As will be seen, this is relevant to the question whether Henry Karpik contracted the virus on the voyage and to questions that arise in the consumer guarantee claims (whether it was possible for cruise services at the relevant time to be reasonably fit for a safety purpose) and the tort claim (the scope and content of the duty of care and the probability of harm).
110 Mrs Karpik pleads that as at 8 March 2020, the risk of contracting coronavirus on a cruise ship was heightened as compared to the risk of contracting coronavirus in the community generally. This is denied by the respondents. [CRT.001.001.0275 [19A]; CRT.001.001.0408 [19A]] That dispute led to Joint Report 3 of the experts Professors Wilder-Smith, Rocklöv, Bennett and McCaw and Associate Professor Vally which reveals remarkable agreement. The question that they sought to answer was:
Was the risk of contracting COVID-19 on a cruise ship compared to the risk of contracting COVID-19 in the general community heightened as at 8 March 2020, including what was known at that time?
111 Save where I indicate the contrary, the findings recorded in this section are based on the agreement of the experts as recorded by them in Joint Report 3.
112 A cruise ship is different from the community in general as cruise ships carry a large number of people (about 4,000 on Ruby Princess) for 1-3 weeks, with some of that time in relatively confined shared spaces, and likely more of such time than that same person would spend in similar spaces when in the general community. The higher density of persons, including the more meeting places, such as restaurants, gyms, social gatherings, and so on, leads to higher contact rates. Contact frequency, contact proximity and contact duration are the main drivers for transmission of the virus. [JNT.001.001.0019 [2], [15]]
113 Passengers and crew on cruise ships generally originate from diverse geographic regions and embark and often disembark multiple times during the voyage, and therefore reflect the epidemiology of COVID-19 from different regions. This puts cruise ships at risk of multiple sources of potential introduction of the virus. Factors that facilitate spread on cruise ships include mingling of travellers from multiple geographic regions and the closed nature of a cruise ship environment. Crew on cruise ships are a known potential vector for infection as they link cohorts when continuing from voyage to voyage. [JNT.001.001.0019 [4], [6], [16], [18]]
114 Also, the risks associated with contracting an infection in a setting where there are more older persons present will be higher due to their increased vulnerability to the virus. [JNT.001.001.0019 [5]] I accept the evidence of Professor Wilder-Smith that cruise ship populations tend to be skewed towards older people compared to the general population. The respondents’ own risk assessment on 25 February 2020 identified that their “guest demographics” (ie, older people) could lead to a higher risk of severe infection, “the older demographic on cruise ships are more susceptible to contract the illness and develop severe disease” and that “the predominantly older demographic will require more ICU admissions.” [PCL.001.006.7128]
115 The same document recognised that “cruise ships, like aircraft, are semi-contained, population dense environments which facilitate disease spread via droplets” and that “[r]apid amplification events from a super-spreader can create hotspots within days such as has been seen on Diamond Princess.” It was also recognised that respiratory diseases are the most common illnesses treated on board cruise ships throughout the year and that coronavirus is more contagious than seasonal flu and has a higher mortality rate. [PCL.001.006.7128]
116 By early March 2020, the contagiousness of the virus had been measured across a range of settings with a range of estimated average R0 values of 1.9-6.5 – where R0 is the reproduction number of an infectious disease, being the average number of new infections caused by one infected individual in a population where everyone is susceptible to the disease. The most common estimate for R0 for ancestral variants was between 2-3, albeit with substantial uncertainty. The WHO estimates of R0 in the community were around 2. [JNT.001.001.0019 [10]]
117 General population R0 estimates comprise the measures of transmission of the virus across a range of risk settings within the population studied. Thus, estimates of individual R0 values across settings within the same population would be expected to vary and to range from very low (including < 1) to very high depending on the characteristics of the setting. Cruise ships’ R0 estimates would be expected to fall within the range of R0s measured in a variety of settings within the general community, because it includes settings with high R0s. Nevertheless, cruise ship R0 is highly likely at the high end of the spectrum. [JNT.001.001.0019 [11]-[12]]
118 I accept the evidence of Professor Wilder-Smith that it is more likely for the virus to be introduced and cause an outbreak on a cruise ship compared to in the community in general. Further, because of the generally higher R0 on cruise ships the spread would likely be more efficient in this setting. [JNT.001.001.0019 [17]]
119 Professors Bennett and McCaw and Associate Professor Vally highlight that the factors that facilitate spread on cruise ships are also present in other venues and settings in the community, including accommodation facilities, or holiday resorts with limited options for dining and other indoor activities, or at which people spend a week or more in residence. They also point to settings other than cruise ships where people from multiple country destinations congregate, such as holiday resorts and travel terminals, which are at a higher risk of having an infectious person present – because of attendees being from different countries including countries with higher prevalence of infection. [JNT.001.001.0019 [7], [19]]
120 I find these examples to be unhelpful, and essentially argumentative, because they do not reflect the community generally which is the relevant comparator, ie, the notional passenger going about their ordinary business of life in the community for 13 days compared to going on a cruise ship for that period of time. The experts agreed on the obvious, namely that there are settings within the community generally with confined spaces, overcrowding and repeated or extended exposures such as holiday resorts, aged care facilities, prisons and boarding schools, and that, if there is seeding in one of these settings, people attending them are at a higher risk of rapid transmission of the virus than in other settings in the community or in the community generally. [JNT.001.001.0019 [21]] That may mean that there are particular duties in respect of those high risk settings, but it does not mean that cruise ships offer the same or similar risk relative to the community generally.
121 If the virus is introduced by a single infected individual on a cruise ship, take-off of the virus is more likely than on average in the general society. Super-spreading was suspected as at 8 March 2020 and is now well established as a feature of the virus. Cruise ships are particularly conducive to super spreading potential, although that is not exclusive to cruise ships. A cruise ship with multiple introductions is more likely, and possibly highly likely, to have an outbreak. [JNT.001.001.0019 [8], [40]]
122 A number of positive assertions were made to Mrs Karpik in cross-examination that are relevant to the question of the heightened risk of transmission of coronavirus on cruise ships. Such positive assertions in cross-examination can be taken to be the respondents’ case at trial, and can therefore be taken as implicit admissions against the respondents’ interests and taken into account in the process of fact-finding: R v Robinson [1977] Qd R 387 at 394 per Dunn J, Wanstall ACJ and Douglas J agreeing; Spiteri v Visyboard Pty Ltd [2005] VSCA 132 at [41] per Ormiston JA, Charles and Chernov JJA agreeing; R v Baring and Leonard [2005] SASC 262; 92 SASR 117 at [70] per Sulan J, Doyle CJ agreeing. These assertions include the following:
(1) A characteristic of cruise ships, like indoor venues, is that they have inherently confined spaces which means they have a heightened risk of contracting coronavirus when compared to outdoor venues (T144:42-47).
(2) It is a characteristic of cruise ships that passengers and crew travel to the cruise from a diversity of geographic regions (T145:4).
(3) It is a characteristic of cruise ships that recreational, health and dining facilities are shared between passengers which leads to frequent physical interaction between crew and passengers and numerous shared high-touch surfaces (T145:36-47).
(4) It is a characteristic of cruise ships that they offer and promote recreational entertainment activities, requiring physical interaction between crew and passengers and reduced physical distancing (T146:1-6).
(5) It is a characteristic of cruise ships that if passengers fall ill with a highly infectious illness, they may not be able to be removed from the ship for several days, or at all, depending on the nature of the voyage (T146:8).
(6) As at 8 March 2020, there were reports that a significant number of people who had tested positive for coronavirus did not have symptoms at the time of testing (T146:21-22).
(7) There was a not insignificant risk that one or more of the passengers or crew who had been on voyage RU2006 on the Ruby Princess might have been infected with coronavirus (T146:39).
(8) As at 8 March 2020, there was a not insignificant risk that there were active contagious coronavirus particles on the Ruby Princess (T148:17).
(9) There was a risk that passengers on the Ruby Princess on the voyage in question could be infected with the virus by a crew member who had been on the previous voyage or by a fellow passenger (T148:33).
123 Notably, the CDC in its “No Sail Order” referred to at [84] above, identified several features of cruise ships that increase the risk of coronavirus transmission. These include: the number and the variety of person-to-person contacts an individual passenger may have daily; the dynamics of passenger-to-passenger, passenger-to-crew, crew-to-passenger, and crew-to-crew intermingling in semi-closed settings; frequent events that bring passengers and crew close together, including group and buffet dining, entertainment events and excursions; cruise ship cabins are small, increasing the risk of transmission between cabin mates; close quartering for crew, who typically eat and sleep in small, crowded spaces; infection of crew may lead to transmission on sequential cruises on the same vessel; crew from one ship may in turn serve on-board multiple different ships for subsequent voyages, potentially amplifying transmission; the difficulty of de-contaminating numerous surfaces and common areas; the high volume of people on-board a cruise ship and wealth of high-touched surfaces make successful control of fomite transmission very difficult; quarantine and isolation measures are difficult to implement effectively on board a cruise ship; if a ship is at capacity, it may not be feasible to fully separate ill and well persons on board the ship, particularly among the crew; and because crew are required to continue working to keep a ship safety operating, effective quarantine for crew is particularly challenging. [PUB.010.003.0001]
124 In the light of all of the above, I have no hesitancy in finding that cruise ships are peculiarly susceptible to coronavirus infection and transmission and compare very poorly with the community generally in that regard, and that the respondents knew that. The respondents’ contentions to the contrary are rejected.
B.6 The Ruby Princess voyage RU2007
B.6.1 Communications with passengers
125 Passengers were required to log in to the respondents’ “Cruise Personalizer” portal some time before their cruise. On doing so, they were shown a notification signed by Jan Swartz as President of Princess Cruises. The notification was headed “Our Commitment to Safety” and included the following: [LAY_SKA.001.001.0083 [43]; LAY_SKA.001.001.0273 pp 20-21]
When you sail with Princess, you entrust us with your safety, and we take that responsibility very seriously. Nothing is of greater importance than the safety and security of our guests.
Our fleet operates under a safety management system that is certified under the International Safety Management Code and provides the foundation for operating our Safety, Health, Environmental and Security programs; we are vigilant in our dedication to these.
126 On 24 February 2020, passengers for the forthcoming cruise were sent an “Emergency Notification” (that being its heading) by the respondents that included the following: [LAY_SKA.001.001.0273 p 22]
IMPORTANT NOTICES
We’re monitoring the situation with the coronavirus that originated in mainland China, and our medical experts are working with global health authorities. As a precaution, anyone who has traveled [sic] from or through mainland China, Macau or Hong Kong (including airport transits), or has had contact with a suspected or confirmed case of coronavirus (2019-nCoV) within 14 days of the start of this cruise will not be allowed to board the ship. If this applies to you or your client, please contact us with proof of this travel for a full refund of the amount paid to Princess Cruises. All guests will also be subject to pre-boarding health reporting and enhanced screening at check-in. Due to changing circumstances, it is possible that authorities in the countries on your cruise may change their entry requirements on short notice. Please check all entry requirements prior to your arrival to the ship to ensure you are not impacted. Guest passports will be scanned to verify compliance. False responses on forms will result in immediate debark at the next opportunity, and you may face legal consequences. We may change requirements to safeguard guests and crew.
127 On or about 5 March 2020, passengers received an email (addressed, in the case of the Karpiks, to “Dear Henry”) from Ms Swartz reaffirming the respondents’ commitment to the health and safety of their passengers, offering a refund for cruises departing on and from 9 March 2020 (being the day after the Ruby Princess was scheduled to and did depart), and encouraging even those passengers to keep their booking by offering them onboard credits: [SKA.001.001.0017]
We continue to implement increased monitoring, screening and sanitation protocols to protect the health of our guests, crew and the residents of the destinations we serve. Our measures are designed to be flexible to adapt to changing conditions and recommended best practices. For your reference, you can read our Guest Travel Advisory.
Nevertheless, we know you have questions about your upcoming cruise. Princess would like to share some policy updates that provide options and flexibility should you want to reschedule your currently booked vacation that sails between now and May 31, 2020.
Sailings departing between March 9 and April 3*: booked guests can cancel up to 3 days prior to departure, receive a Future Cruise Credit for 100% of the cancellation fee amount, and move your booking to any voyage that departs by December 31, 2021.
…
We appreciate your loyalty and look forward to welcoming you onboard.
128 Email communications between the respondents’ different brands show that there were “no issues” with making the policy change with regard to full refunds in the form of Future Cruise Credits effective immediately (ie, from 5 March) other than a concern about it generating too many calls to customer services. No witness from the respondents dealt with this policy change so no one could be asked about it. In the absence of any explanation from the respondents, I infer that there were no operational impediments to allowing cancellations on RU2007 with full refunds and that the principal reason for not doing so was financial. I return to this issue in section F.4.2 below. [PCL.001.005.6798]
129 As I deal with in more detail in section B.8.1 below, the scheduled boarding for RU2007 on 8 March 2020, which should apparently have commenced in the morning, was delayed until the evening because of the health screening that was necessary for passengers disembarking from RU2006 and for cleaning the vessel.
B.6.3 Pre-embarkation screening
130 On 7 March 2020, Traveller’s Health Declarations consistent with Revision 5 were sent to the printer for use during boarding for the voyage on 8 March 2020. On 8 March 2020, the Hotel General Manager on the Ruby Princess had another version of the Traveller’s Health Declarations prepared which added Indonesia and Cambodia to the countries listed in question 3, to be consistent with the countries of interest previously identified by NSW Health. Both versions came to be used during embarkation on 8 March 2020.
131 On 8 March 2020, embarkation for the voyage on Ruby Princess was carried out apparently consistently with the requirements of Revision 5. Ms Loren Budd, Customer Services Director on the Ruby Princess, gave evidence as to the printing of the Traveller’s Health Declarations for use in boarding RU2007 and as to witnessing the screening process of passengers prior to boarding. Ms Budd deposed to having seen passengers being provided with the Traveller’s Health Declaration by shore-side staff, with some guests required to proceed to an area separated by a screen. [LAY_RES.001.001.0433] Ms Budd’s evidence concerning the pre-boarding screening process was not challenged in cross-examination and I accept it.
132 Thirty-four guests were denied boarding based on their answers to the questions posed in the Traveller’s Health Declarations completed by passengers and crew prior to embarkation. Fifty-nine guests who had transited through Singapore underwent secondary health screening and were thereafter permitted to board. [SBM.020.004.0001 [46], [360]] That secondary screening involved being asked to declare whether in the past 14 days the person (or any children under the age of 18 travelling with them) had experienced fever, cough or difficulty breathing, and being assessed by a Registered Nurse from the ship’s medical team, which involved a person’s temperature being taken, any reported respiratory symptoms being reviewed, and a form being completed by the Registered Nurse entitled the “Novel coronavirus (2019-NCoV) patient investigation form.” [CRT.500.004.0001 [107G], [107H]]
133 The 59 passengers who were subjected to additional screening had all reported recent travel through Singapore. Fifty-eight passengers reported that they had transited through Singapore for a period of between 30 minutes and 3.5 hours, and 1 passenger reported that they had travelled through Singapore and Indonesia 6 weeks prior to RU2007 but had subsequently travelled back to the United States. Each of the 59 passengers had a recorded temperature of between 35.8 and 37.25 degrees Celsius (ie, normal). None of the passengers reported experiencing fever or chills, a cough, shortness of breath or difficulty breathing, except for one guest who reported a cough due to chronic bronchitis and was referred to an independent medical practitioner, who issued the passenger with a medical certificate. All 59 passengers who underwent the additional screening were permitted to board. [CRT.500.004.0001 [109], [109A]]
134 There is no evidence, one way or the other, with regard to the extent to which the information provided by passengers in their health declarations against any travel history apparent in their passports was checked.
135 No temperature screening was conducted other than in connection with the supplementary screening of the 59 passengers already referred to.
136 For completeness, it should be mentioned that crew that were due to join the vessel for RU2007, having not been on RU2006, were also screened prior to boarding based on their Traveller’s Health Declarations. Three crew were denied boarding and arrangements were then made for them to return to their home countries. Some crew who had been due to join the vessel were advised that they would not be allowed to board in time for them to not even leave their home countries to fly to Australia. [LAY_RES.001.001.0593]
137 Despite the efforts of the ship’s personnel to order additional swabs and masks in advance, when the Ruby Princess departed from Sydney on 8 March 2020 it had in stock only 27 viral swabs, a limited number of rapid influenza testing kits (each of which contained a viral swab) and approximately 250 surgical face masks. [CRT.001.001.0275 [84]; CRT.001.001.0408 [84]] Orders had been placed for further supplies to be delivered on board during the voyage, but none materialised, at least in part because the lead-in time for such orders was 2-4 weeks. [GEN.001.001.4763]
138 Emails from the ship’s medical personnel indicate that they appreciated that the ship sailed with inadequate medical supplies in the respects mentioned. In particular, only 250 disposable face masks for a ship with about 3,800 people on board for a 13-day cruise in the circumstances of the evolving, at that time, epidemic, was hopelessly insufficient. For example, on 9 March 2020, two passengers who had transited through Singapore and had airway infections were suspected of having COVID-19. When asked how many masks could be provided “for situations like this”, Dr von Watzdorf, the Senior Physician on board the Ruby Princess, responded that she had no masks to give out and that they had almost run out following the events of the previous cruise. [PCL.001.001.1801] On 10 March 2020, Dr von Watzdorf reported that they had only “a FEW surgical masks left.” [CAU.001.004.3091]
B.6.5 Cleaning, hygiene and sanitation measures
139 The respondents adduced evidence of cleaning, hygiene and sanitation measures that were deployed on board the Ruby Princess in answer to Mrs Karpik’s claims that the risk of COVID-19 could have been avoided or reduced by ensuring that the ship was “thoroughly cleaned” prior to the passengers boarding on 8 March 2020 and by “adequately cleaning” the ship during the voyage RU2007, requiring passengers and crew to engage in hand washing and sanitizing, and preventing self-service and communal service of food. [CRT.001.001.0275 [42(a)], [43(a)-(e)]] The evidence of the respondents’ general cleaning, hygiene and sanitation procedures included evidence about procedures adopted on “turnaround” days (when one voyage disembarked and another voyage embarked, relevantly in this case, the “turnaround” of RU2006 on 8 March 2020).
140 Mr Artur Ferreira, Acting Executive Housekeeper, gave evidence that the sanitation and cleaning procedures applicable to the Ruby Princess were guided by a classification system which determined what processes were to be followed, the dilution of cleaning chemicals and the frequency of sanitation and cleaning [LAY_RES.001.001.0199 [27]]. Mr Ferreira explained that the classification system involved the following sanitation levels:
(1) Baseline level (or Green level), which required standard cleaning procedures;
(2) Elevated level (or Yellow level), which required increased concentration of chemicals and increased frequency of sanitation and cleaning; and
(3) Maximum level (or Red level), which required maximum chemical concentration and continuous and consistent sanitation of all areas of the ship.
141 The primary chemical used by the respondents to clean and sanitise non-food areas on the Ruby Princess was Virox, which was dispensed through a machine located in a chemical locker on Deck 4, and which was managed by the Crew Supervisor. The concentration of Virox dispensed via the chemical locker depended upon the sanitation level at which the ship was operating at any given time, with Green demanding the lowest concentration and Red the highest. Mr Ferreira gave evidence that the Virox dispenser operated in such a way that Red levels of Virox could be dispensed at any time (because Red level Virox was continuously used by certain medical and specialised employees irrespective of the prevailing sanitation level), but that only one of the Yellow level or Green level Virox solutions could be dispensed at any one time because the level not in use was required to be locked by the Crew Supervisor. Changes to the Virox dispenser were recorded in a log. [LAY_RES.001.001.0199 [39]-[45]]
142 The Virox log appears to show that on 7 March 2020, Virox solution was dispensed at only the Baseline and Maximum levels. From 8 March to 14 March, Virox solution was dispensed at only the Elevated and Maximum levels. [LAY_RES.001.001.0187] Given the explanation that a Red level dispenser was always available, this indicates that the general sanitation level was raised from Green to Yellow from 8 March 2020. That change was confirmed by the witness evidence.
143 The Virox log appears to show a further raising of the sanitation level on board the Ruby Princess from 16 March 2020 to the Maximum or Red level. The ship appears to have remained at Maximum sanitation level for at least the remainder of March. Witness evidence and internal emails confirm this change at that time. Although there was a challenge to some of the evidence of Mr Claudio Iezzoni, Food & Beverage Supervisor, on this issue in cross-examination, Mrs Karpik makes nothing of it in closing submissions and I accept the witness’s evidence.
144 As noted above (see [105]), the respondents introduced “Enhanced Public Health Protocols” from 7 March 2020 that Hotel General Manager Mr Verwaal asked staff on board the Ruby Princess to adhere to. [CAU.001.001.0012; CAU.001.001.0013] The Enhanced Public Health Protocols called for staff on board to, among other things:
Engage in daily communication with all crew reinforcing use of appropriate PPE, frequent hand washing with soap and running water for at least 20 seconds, avoid hand contact, follow sanitising standards, refrain from serving drinks to guests in reusable tumblers, encourage crew to report any guests who may show signs of illness (coughing, sneezing, runny nose, etc);
Enforce hand washing at all crew food venues;
Monitor hand washing at food venue entrances and administer hand sanitiser or direct guests to wash their hands at nearest available sinks;
Increase availability of hand sanitiser dispensers at food outlets;
Increase frequency of sanitising for high traffic hand touch surfaces in public areas especially during crowd gathering events;
Enhance sanitation of frequent touch points (ie, hand rails, door handles, chairs, stools, tables, bar counters and gangways);
Provide small/portable hand sanitiser in each guest stateroom; and
Prop open doors to all public lounges and restrooms to reduce door handles hand touch.
145 The respondents’ policies describe the responsibilities of various members of staff, and outline detailed procedures to be followed and cleaning chemicals to be used, including when cleaning particular areas of the vessel such as bathrooms and the medical centre. [RES.001.001.0215]
146 In addition to standard cleaning of public and accommodation areas, there was a “Hit Squad” of crew members who attended to the particular cleaning and sanitation of areas in which there had been a public health incident, such as cabins in which guests had been isolating due to illness. [LAY_RES.001.001.0176 [16]] The Hit Squad was required to use Red level concentration of Virox when cleaning affected areas. [LAY_RES.001.001.0199 [52]-[53]]
147 Affidavit evidence adduced by the respondents speaks to the cleaning and sanitation that occurred on board RU2007. Mr Ferreira gave evidence that in view of the Enhanced Public Health Protocol, he directed staff to frequently sanitise high touch points on board, frequently wash hands, and wear appropriate PPE when attending to cleaning duties. [LAY_RES.001.001.0199 [77]] Ms Javier, Assistant Housekeeper, gave evidence that, in line with the elevated sanitation level prevailing on RU2007, she instructed her staff to implement, and she personally observed, increased sanitation frequency of touch points such as elevator buttons, handrails, toilets, stairs, chairs, armrests, door handles and bars. [LAY_RES.001.001.0176 [46]-[48]] In respect of food and beverage areas, Mr Iezzoni gave evidence about the provision of hand sanitiser to guests and the regular sanitisation of dining tables. [LAY_RES.001.001.0001 [45]-[54]] I accept all that evidence.
148 The respondents adduced evidence of particular measures taken to encourage hand hygiene in view of Mrs Karpik’s pleading that the risk of transmission of coronavirus could have been avoided or reduced by requiring passengers and crew to wash their hands or use appropriate hand sanitiser when entering or leaving public areas, preventing the self-service of food by passengers and the use of common implements and communal bowls.
149 One such measure was the stationing of crew and hand sanitiser dispensers in appropriate areas. Mr Iezzoni gave evidence that staff were stationed at the entrances to dining areas and directed to request that passengers sanitise their hands prior to entering using nearby dispensers. According to Mr Iezzoni’s evidence, this was standard practice even when the ship was operating at Green level sanitation. Consistently with the Enhanced Public Health Protocol circulated by Mr Verwaal, Mr Iezzoni gave evidence that, on RU2007, changes were implemented to the service of food such that guests were not required to touch any utensils or condiments at the buffet line but would instead be assisted by staff. [LAY_RES.001.001.0001 [45], [74], [103]-[109]] I accept this evidence.
150 Passengers who travelled on RU2007 gave varying evidence of whether they witnessed staff directing passengers to sanitise their hands. For example, Ms Dianne Carroll, a passenger on RU2007 and group member, gave evidence that staff were ensuring that passengers sanitised their hands before entry to food service areas and in cross-examination confirmed that staff stood in entrance ways and directed guests to hand sanitisers (T129). [LAY_SKA.002.001.0001 [80]] However, Mrs Karpik gave evidence in cross-examination that she witnessed passengers in food service areas failing to sanitise their hands and serving themselves with shared utensils (T183). Similar evidence was given by Ms Carmel Avis that although she observed a staff member encouraging passengers to sanitise their hands before attending the buffet, some passengers did not do so, and some passengers served themselves with shared utensils. [LAY_SKA.002.001.0061 [16]-[26]] I accept that the staff did generally direct passengers to sanitise their hands, although some passengers sometimes ignored such direction.
151 Another measure directed toward hand hygiene was directions and reminders given to crew and passengers to sanitise their hands. In addition to the Enhanced Public Health Protocol referred to above, communications reinforcing the importance of hand washing were made to crew via email, public health and safety training sessions, briefings, and signage in crew areas. [PCL.002.036.1115; LAY_RES.001.001.0355 pp 13-14; LAY_RES.001.001.0028 [13]-[16]; LAY_RES.001.001.0016 [40]-[42]; LAY_RES.001.001.0016 [43]]
152 In respect of the passengers, the respondents distributed written guidance during the cruise which contained recommended hand hygiene practices. One such written guidance was a letter entitled “Coronavirus Health Advisory”, which Ms Carroll deposed to having received on or about 11 March 2020, which recommended, as a precaution, that passengers “[w]ash [their] hands often with soap and water for 20 seconds, and help young children to do the same. Where soap and water are not available, use an alcohol-based hand sanitizer.” [PCL.002.006.4418; LAY_SKA.002.001.0001 [53]] Similar advice was contained in the daily “Princess Patter” newsletter distributed to guests on 17 March 2020. [SKA.005.001.0078]
153 Mr Verwaal also gave unchallenged evidence that he heard multiple announcements on board reminding guests to wash their hands. [LAY_RES.001.001.0342 [47(d)]]
154 Mrs Karpik claims that the respondents should have introduced physical distancing on board the Ruby Princess and failed to do so. [CRT.001.001.0275 [42(l)], [43(f)], [43(g)]] Apart from the cancellation of the Ultimate Ship Tour and Galley Tour on RU2007 as directed by the respondents’ Enhanced Public Health Protocol, a measure which appears to have been taken to avoid having guests in crew areas, there is no evidence that the respondents encouraged or implemented any meaningful physical distancing. [LAY_RES.001.001.0355 pp 20, 33-34]
B.6.8 Management of persons with respiratory symptoms
155 In answer to pleaded deficiencies concerning the respondents’ management of persons with respiratory symptoms on board, the respondents adduced evidence of their standard practices for managing passengers and crew presenting with symptoms consistent with ARI or ILI and also of particular practices adopted on RU2007.
156 The respondents maintained a policy entitled “PHS-1120 – Management of Acute Respiratory Disease (ARD)” which set out the procedures to be followed with regard to the medical management of individual cases of ARD and the prevention and control of influenza outbreaks. [CAU.001.018.0173] The policy addresses the definitions of ARI and ILI, required sanitation response to the presence of ILI on board, reporting and record-keeping requirements (including the maintenance of the ARD log), and recommended treatment and management steps. Under the heading, “Medical Management”, the policy provides as follows:
All patients who report to the Medical Center with ILI symptoms should be triaged appropriately and separated from other patients. Illness transmission can be significantly reduced if patients are also provided a surgical mask to wear.
…
All patients who meet the ILI case definition should be isolated for at least 24 hours post resolution of fever, not influenced by the use of antipyretics, and major symptoms.
…
Isolation is not required for patients who meet the ARI case definition.
…
Management of the case should be completed in accordance with PHS-1105 Case Management of Communicable Illness.
157 The policy entitled “PHS-1105 Case Management of Communicable Illness”, under the heading “General Management” provides that: [CAU.001.018.0225]
Appropriate and standardized clinical management of any patient must take precedence over any other measures. If the clinical condition necessitates, patients should be treated in isolation in the Medical Center.
…
Patients in isolation (either in cabin or in Medical Center) must be given:
Written instructions on isolation requirements and services available during isolation
Written hand washing information and any other relevant health advice
…
All patients in isolation must be followed up on a daily basis by a member of the medical staff. The follow up must be documented and include:
Identifying any new symptoms
General well-being
Anticipated time of release from isolation
158 When a passenger was placed into isolation, crew in the Food & Beverage, Security and Accommodation departments were notified via email to ensure that the person received meals in their cabin, the Hit Squad sanitised the person’s cabin, and that medical staff were informed if the person was not in their cabin. An email of this kind was sent to crew in respect of Mr Karpik being placed in isolation on 17 March 2020. [CAU.001.004.4473]
159 Under the “PHS-1120 – Management of Acute Respiratory Disease (ARD)” policy, the use of PPE by medical staff was governed by the policy “Med-3601 Infection Control.” [CAU.001.018.0002] That policy provided that the use of PPE is “essential for the health and safety of medical staff to reduce risk of transmission of microorganisms” and directed that the selection of appropriate equipment should be based on “the nature of the patient interaction, the suspected infectious agent and the risk of contamination of the healthcare worker’s clothing, skin, and mucous membranes.”
160 During RU2007, the respondents directed passengers and crew to contact the medical centre if they were experiencing respiratory symptoms, including via an announcement made over the ship’s PA system. [CRT.500.004.0001 [119]; RES.001.001.0215 p 115 (“Health Advisory – Coronavirus”), CAU.001.011.7910; LAY_SKA.001.001.0083 [116]] As at 19 March 2020, 124 persons, including Mr Karpik, were listed on the ARD log. [CAU.001.003.0021] Charges incurred by passengers who presented to the medical centre with symptoms consistent with ARI or ILI were waived by the respondents. [CAU.001.004.4480]
161 Mrs Karpik deposed to three affidavits which were read in the proceeding as her evidence in chief. She was cross-examined at length by senior counsel for the respondents on issues relevant to liability and, with leave, by junior counsel for the respondents on issues relevant to her medical history and quantum.
162 As will be seen, Mrs Karpik’s affidavit evidence and her evidence in cross-examination, and indeed on occasion different parts of her evidence in cross-examination, were at times inconsistent. I do not take Mrs Karpik to have been wilfully dishonest. Her experience of the cruise and its aftermath, in particular, were highly stressful for her and indeed traumatic. Thereafter there was considerable publicity about the problems on the cruise, including a public inquiry, much of which was streamed live and some of which was watched by her (T172:35). It is therefore perhaps unsurprising that her recollection of events may have been superimposed with things she learnt later. Moreover, she has a clear belief in the justness of her case, her enthusiasm for which may also have infected the reliability of her evidence.
163 In those circumstances, Mrs Karpik at times gave evidence – both in her affidavits and in answer to questions in the witness box – which was inaccurate and even false. As a result, I approach her evidence with caution and in particular look to see whether it is confirmed by, or at least consistent with, other evidence and whether it is consistent with the overall probabilities and human experience.
164 As mentioned, at the time of the cruise in March 2020, Mrs Karpik was 69 years of age and was residing with her husband of nearly 50 years, Henry, in Figtree, an inner suburb of Wollongong, New South Wales.
165 Mrs Karpik has a Diploma in Nursing, a Bachelor of Nursing and a Masters of Science – Mental Health. While she undertook those studies, she was employed by NSW Health Wollongong and Shellharbour services as a registered nurse. She worked in a variety of clinical and management roles within NSW Health for more than 50 years. [LAY_SKA.001.001.0083 [6]-[7]]
166 Mr and Mrs Karpik have four adult children who were born in the 70s and 80s. [LAY_SKA.001.001.0083 [5]]
167 From about 2015, Mrs Karpik retired from full-time nursing and worked on a part-time basis as an Official Visitor under the Mental Health Act 2007 (NSW). That role required her to regularly visit a selection of mental health facilities to engage with consumers, carers and healthcare providers to ensure the provision of humane and respectful services in line with contemporary clinical practice standards. By March 2020, she was working seven to eight days per month, seven to eight hours per day. [LAY_SKA.001.001.0083 [10]]
168 Mr and Mrs Karpik have a long history of taking holidays together on cruise ships. By the respondents’ records, Mrs Karpik had undertaken nine Princess cruises since 2008, with a total of 114 cruising days. Mrs Karpik said that she and her husband had undertaken approximately 11 cruises together. [LAY_SKA.001.001.0083 [25]; T135]
169 Mrs Karpik first learnt of the cruise from a Princess Cruises brochure and advertisements she received via email. By the time of trial, Mrs Karpik no longer had copies of the brochure or advertisements and could not recall precisely which brochure she reviewed. However, she had since reviewed a number of Princess Cruises brochures for cruises in Australia and New Zealand around that time and confirmed that they are similar to the brochure she reviewed before booking the cruise. Unsurprisingly, the brochures present images of a relaxing and pleasurable holiday experience. They also use the respondents’ registered trade mark, “come back new.” [LAY_SKA.003.001.0047 p 2]
170 The Karpiks’ tickets for the cruise were booked via Travel Associates travel agency on 5 September 2019. The total cruise price was $8,746.00, with $2,208.13 being paid on deposit at the time of booking. [LAY_SKA.001.001.0083 [39]] Mrs Karpik received a booking confirmation by email from the respondents dated 9 December 2019 which set out the details of the booking. [LAY_SKA.001.001.0273 p 18]
171 It is common ground that the Karpiks’ booking was subject to particular terms and conditions with Carnival. I will return to those where relevant.
172 In paragraph 48 of her first affidavit, Mrs Karpik said the following: [LAY_SKA.001.001.0083 [48]]
I had assumed that Princess Cruises would be extra vigilant on our Voyage, and have good strategies in place to reduce the risk of a Coronavirus outbreak. I assumed that if any risk in relation to Coronavirus existed, they would cancel the Voyage so as not to repeat the events of the Diamond Princess.
173 Those two sentences are in tension with each other in as much as the first speaks of the respondents having strategies to “reduce the risk” of a COVID-19 outbreak, which implies that the cruise would go ahead even if there was some risk, and the second says that if there was any risk of such an outbreak the respondents would cancel the cruise. Fairly read, the paragraph must be understood to say that the cruise would be cancelled if there was any material or significant risk, rather than any risk at all.
174 Mrs Karpik also said in her first affidavit that, in the weeks leading up to the voyage, she followed the news closely and had many discussions with her family, many of whom are health workers, about the potential threat of coronavirus. [LAY_SKA.001.001.0083 [45]] In relation to her family members, one of her daughters-in-law was working as a secretary to a cardiologist and two of her daughters were registered nurses, one of whom was married to a consultant in the emergency departments at a number of hospitals (T137). In cross-examination, she said that her son-in-law had questioned whether her and her husband’s decision-making with regard to going on the voyage was sensible and whether they had thought about the risk of coronavirus. He told them that cruise ships, from his perspective, were “petri dishes” and the risk of infection was high for any illness or any condition. He said that he was aware of what happened on the Diamond Princess (T140:35).
175 In that context, including that she was herself qualified and had worked as a nurse, it is no surprise that in her first affidavit Mrs Karpik said that she had “a heightened awareness of the risk of transmission of infectious diseases such as Coronavirus.” Mrs Karpik also said in her affidavit that during the trip to Circular Quay, she and her travelling companions had a conversation regarding the potential risk of coronavirus on the voyage. She gave advice to the others on a range of personal protective strategies she believed that they should use during the voyage. [LAY_SKA.001.001.0083 [55], [65]]
176 In those circumstances, Mrs Karpik must have understood and appreciated that there was some risk of a coronavirus outbreak on the cruise. She could not reasonably or credibly have thought or understood that there was no risk of coronavirus on the cruise. In my assessment, Mrs Karpik maintained her “no risk” position in cross-examination in order to defend what she had said in the second sentence of paragraph 48 of her first affidavit and because, in the heat of the moment under cross-examination, she perceived that to be advantageous to her case.
177 Time and again in cross-examination, Mrs Karpik said that she thought that there would be no or zero risk to passengers on the cruise (T145:10, T147:23, T148:29, T148:40, T151:43). She also said that she believed that the respondents had a system that could eliminate the risk of coronavirus (T148:46). In view of her training and her knowledge about infectious diseases, including coronavirus, and what her son-in-law had said to her, those answers lack any credibility. I do not accept them. The truth is that Mrs Karpik knew there to be a risk, but she thought that the respondents would take all reasonable measures to minimise the risk and, if they were unable to do so, they would cancel the cruise. That is to say, she took comfort from the reassuring communications from the respondents and that the cruise was going ahead.
178 At one point in cross-examination, Mrs Karpik answered affirmatively to the proposition that when she and her husband decided to go on the cruise on 8 March 2020, they did so accepting that there was a risk that either or both of them could be infected with coronavirus (T150:43). The respondents sought to make much of this on the basis that it meant that her “no risk” position in the second sentence of paragraph 48 of her first affidavit and in earlier answers in cross-examination was incorrect. When pressed, Mrs Karpik stuck with her “no risk” position and explained her affirmative answer to her and her husband having accepted “a risk” when they went on the cruise as arising from her having misunderstood the question – having thought that it referred to influenza and not coronavirus (T153:26). Such a misunderstanding is credible because the question followed a sustained series of questions about norovirus and influenza, without drawing particular attention that the subject matter was reverting to coronavirus. However, it remains incredible, and I do not accept, that Mrs Karpik thought that there was no risk of coronavirus on the cruise. In boarding the vessel, Mr and Mrs Karpik inevitably accepted some risk of coronavirus on board.
179 In her attempts to explain her agreement that she and her husband had accepted that there was a risk of coronavirus on the voyage, Mrs Karpik said that she believed that if there was “any evidence” of coronavirus on the ship, or if the respondents “were aware” that there was coronavirus on the ship, then they would have cancelled the voyage or at least informed passengers so that they could make their own decision (T152:8-34). I accept that evidence. It is sensible and stands to reason. It is not in conflict, or even tension, with her understanding, as I have found, that there was some risk of the virus being on the cruise.
180 Sometime before the cruise, Mrs Karpik logged-in to the respondents’ “Cruise Personalizer” portal where she viewed and read the document quoted at [125] above. In her first affidavit, Mrs Karpik said that the document made her feel assured that the respondents had a good safety management system in place and took the safety of their guests very seriously. [LAY_SKA.001.001.0083 [43]]
181 In cross-examination, Mrs Karpik said that it was from reading in that document about the International Safety Management Code, which she understood to be an accreditation process for ships, that she thought that the respondents could eliminate the risk of coronavirus on board T148-9, T184-5). She said that since the respondents were “working against safety codes”, if there was going to be a risk of coronavirus, then it was her assumption that the cruise would not have gone ahead, or the passengers would have been given information that the risk was there (T185:28-31).
182 For reasons I have already canvassed, I reject Mrs Karpik’s evidence that she thought that the risk of coronavirus on the vessel could be eliminated. Moreover, there is nothing in the document in question that suggests that the respondents were making such a claim, and there is no reasonable basis to any belief about coronavirus risk based on the International Safety Management Code. However, I accept that Mrs Karpik expected that the respondents would cancel the voyage if there was a significant or material risk of coronavirus, and that the passengers would be informed of such a risk.
183 In paragraph 50 of her first affidavit, Mrs Karpik dealt with her understanding of the “Emergency Notification” email that she received from the respondents on 24 February 2020 (quoted at [126] above). She said that it made her feel as if the respondents were taking the safety of passengers seriously and that they had things under control. She understood it as informing her that the respondents were taking steps to ensure her safety and that she “did not need to worry about Coronavirus as it would not be on the Voyage.”
184 However, in cross-examination, Mrs Karpik characterised the communication in question as being “reassuring” and not as telling her that she did not need to worry about coronavirus or that there would be no coronavirus on the voyage. She accepted that it would be absurd to suggest that the communication was saying that coronavirus would not be on the voyage (T154). When confronted with what she had said in her affidavit, she changed her evidence to say that she understood the communication to say that she did not have to worry about coronavirus as it would not be on the voyage, ie, to revert to what she had said in paragraph 50 of her affidavit (T155). To say that she thought that “coronavirus would not be on the voyage” is in substance the same as to say that there was no risk that there would be coronavirus on the voyage. For the reasons already given, that is not something that Mrs Karpik could have believed. Indeed, Mrs Karpik later accepted in cross-examination that the statement in her affidavit that she understood from the communication that she did not need to worry about coronavirus as it would not be on the voyage was incorrect (T160).
185 I therefore reject the evidence that before the voyage Mrs Karpik understood the communication in question to be telling her that she did not need to worry about coronavirus as it would not be on the voyage. I accept that she understood the communication to be reassuring to her about the risk of coronavirus on the cruise, in particular because the respondents were taking the safety of passengers seriously, they had things under control, they were taking steps to ensure the passengers’ safety and they were putting in place strategies to minimise the risk of infected passengers bringing the virus on board.
186 In her first affidavit, Mrs Karpik said that she took the “Dear Henry” email from the respondents dated 5 March 2020 (quoted at [127] above) to mean that the voyage “was safe and there was no risk that people would become infected by Coronavirus.” She said that she understood that the respondents would be taking steps to protect the health and safety of passengers by implementing increased monitoring, screening and sanitation. She believed that she would be able to have a relaxing and enjoyable cruise with her husband and her friends without having to worry about coronavirus. [LAY_SKA.001.001.0083 [53]]
187 Mrs Karpik initially confirmed in cross-examination that she took the email to mean that the voyage was safe and there was no risk that people would become infected by coronavirus (T160:45). She, however, accepted that there was no part of the email that told her that and that it would be absurd to have thought that the respondents could do something to eliminate the risk of people becoming infected with coronavirus on a cruise ship (T161:1-17). I accept that evidence, and reject the statement in her affidavit which she initially confirmed in cross-examination that she took the email to mean that there was no risk that people would become infected by coronavirus.
B.8 The Karpiks’ experience of the cruise and thereafter
188 Mr and Mrs Karpik were collected from their home at about 10.00am on 8 March 2020 by private limousine. They picked up four friends of theirs (two couples) and travelled to Circular Quay to board the Ruby Princess. The Karpiks’ friends were due to embark at noon and the Karpiks were themselves scheduled to embark at 2.00pm. [LAY_SKA.001.001.0083 [64], [68]]
189 As it turned out, embarkation was delayed because of the delayed disembarkation of the previous voyage, RU2006, due to health screening taking place and cleaning of the vessel. The Karpiks had lunch at a café and dinner at a pub or a hotel in The Rocks area adjacent to the Overseas Passenger Terminal while they waited for their rescheduled embarkation time. They ultimately boarded at about 8.00pm (T163-4).
190 Mr and Mrs Karpik completed, and signed, the requisite health declaration before boarding. In doing so they confirmed that they had not travelled from, or through, Mainland China, Hong Kong, Macau, South Korea, Iran, Italy, Japan, Singapore, Taiwan or Thailand. By completing the health declarations, they would have appreciated that other passengers who had travelled from or through those countries were being screened in some way. The Karpiks also confirmed that they had not, in the past 14 days, had a fever, cough or difficulty breathing (T164-5).
191 The Karpiks were assigned to cabin B301, a cabin for disabled passengers because of Mr Karpik’s vision impairment. [LAY_SKA.001.001.0083 [85]]
192 In their cabin, referred to as a “stateroom”, was a health advisory notice to all passengers. It included advice with regard to preventing the spread of infectious diseases including influenza and norovirus. There was no mention of coronavirus. The advice included strong encouragement to adopt the following measures (T167:47):
washing hands regularly with soap and water particularly before eating;
using hand sanitiser after and not instead of hand washing, particularly before eating at the buffet;
trying not to use the public toilet facilities;
minimising direct contact, such as handshaking, with others;
covering one’s nose and mouth with a tissue when coughing or sneezing, or coughing or sneezing into the top of one’s arm; and
returning immediately to one’s stateroom on experiencing any symptoms of vomiting or diarrhoea and immediately reporting the illness to the medical staff.
193 Shortly after embarkation, the Karpiks were directed by their cabin steward to attend a safety muster in the Wheelhouse Bar. Mrs Karpik also heard an announcement over the PA system directing passengers to attend the safety muster. Mrs Karpik’s evidence, which was not challenged, was that the safety muster was extremely crowded with passengers and crew, and everyone was standing or sitting very close to one another. There were approximately 200 people in the Wheelhouse Bar. There was not enough sitting space for everyone in attendance and some people were sitting on the arms of the lounge chairs. There were no procedures in place to implement physical distancing, nor were there any hand sanitiser stations or masks available. [LAY_SKA.001.001.0083 [89]]
194 Aside from Mr Karpik becoming ill and the voyage being cut short, to which I will return, and during the last day of the voyage Mrs Karpik feeling ill herself, the voyage in many respects was undertaken as expected. Mrs Karpik says that she attended the Crooner’s Bar and the International Café approximately six times each with her friends. She attended the laundry facilities twice, the Explorer’s Lounge twice, a trivia event held in a theatre approximately six times, bingo in a theatre twice, shopping stalls, a number of clothing boutiques, various other shops and the Princess Theatre on one occasion to see a Rod Stewart impersonator perform. She also attended the da Vinci Dining Room every night for dinner where she, Mr Karpik and their friends had a table. [LAY_SKA.001.001.0083 [95], [132]]
195 Towards the end of the voyage, Mrs Karpik attended the buffet area approximately six to eight times in order obtain food and liquid for Mr Karpik while he was in isolation. [LAY_SKA.001.001.0083 [96]]
196 The vessel was at sea on 9 and 10 March 2020. On 11 March, it moved through the Fiordland for a day of scenic cruising. Mrs Karpik spent most of the day on the top deck, walking around and taking photographs. Other passengers did much the same. [LAY_SKA.001.001.0083 [97]-[98]]
197 For the first three days of the cruise, whilst the vessel was at sea, Mr Karpik felt well. He went to look at shops on the ship, attended the dining rooms for meals and trivia, walked along the top deck, and met up with friends. [LAY_SKA.003.001.0001 [22]-[23]; LAY_SKA.001.001.0083 [93]-[97]]
198 On 12 March 2020, the vessel arrived at the first port, Port Chalmers in Dunedin. Mr Karpik began to feel weak, tired and lethargic. His bones were aching and he felt off-colour. After telling Mrs Karpik how he felt, she encouraged him to disembark to get some fresh air. In Dunedin, after a one-hour sightseeing trip, Mr Karpik sat in the park by himself while the rest of the group went shopping and sightseeing. Later, Mr Karpik and his friend had a few drinks at a nearby hotel and then boarded the ship. At dinner time on the ship, Mr Karpik was feeling weak, lethargic and had lost his appetite. [LAY_SKA.003.001.0001 [25]-[26]; LAY_SKA.001.001.0083 [99]-[100]]
199 On 13 March 2020, they arrived at the next port, Akaroa. Mr Karpik complained that he was feeling unwell, but Mrs Karpik again encouraged him to disembark thinking it would be beneficial. [LAY_SKA.001.001.0083 [101]] When they returned from sightseeing, Mr Karpik was still feeling unwell and told Mrs Karpik that he wanted to return to the ship. Mr Karpik had aching bones, felt tired, was becoming increasingly irritable and did not feel like eating. Mrs Karpik observed Mr Karpik’s health deteriorating, and checked on Mr Karpik often to see if he had a temperature. On the way to dinner that night, Mr Karpik leant against the wall, and was shaking, feeling very weak and had a temperature. He excused himself from dinner to return to bed. Mrs Karpik gave Mr Karpik Panadol (paracetamol) approximately every six hours from this point onwards. [LAY_SKA.003.001.0001 [27]-[28]; LAY_SKA.001.001.0083 [102]-[103]]
200 On 13 March 2020, the Karpiks also learnt of an announcement that New Zealand was going to close its borders to protect against the threat of the coronavirus pandemic. It was then that the gravity of the pandemic began to feel real to Mrs Karpik. [LAY_SKA.001.001.0083 [104]]
201 During the evening of 13 March 2020, there was an announcement made by the Commodore of the Ruby Princess over the ship’s PA system to the effect that the vessel had been granted permission by the New Zealand government to complete its planned itinerary. Mrs Karpik says that although other passengers began applauding, she felt very concerned because the fact that New Zealand would be closing its borders indicated that there was a real risk of coronavirus. She felt uncomfortable continuing the cruise. [LAY_SKA.001.001.0083 [105]]
202 On 14 March 2020, the ship docked in Wellington. The Karpiks again disembarked with some of their friends and did some sightseeing including visiting a museum. Mr Karpik, however, felt too ill to continue and returned to the ship. Mr Karpik began experiencing high temperatures which were only mildly relieved by Panadol. He did not have a cough or sore throat. Mrs Karpik encouraged Mr Karpik to seek medical attention, however he refused, and wanted to stay in the stateroom resting. [LAY_SKA.003.001.0001 [30]; LAY_SKA.001.001.0083 [107]-[108], [109]-[110]]
203 On 15 March 2020, the ship docked in Napier. Again, the Karpiks disembarked for sightseeing. However, shortly after arriving in the town by shuttle bus, Mr Karpik said that he needed to return to the ship because he was feeling too unwell. [LAY_SKA.001.001.0083 [113]-[114]]
204 Also on 15 March 2020, Mrs Karpik heard an announcement from the Commodore of the ship over the PA system to the effect that the Australian Government had directed that the ship was to return to Sydney as soon as possible as the Australian borders were going to be closed. It was announced that, upon arrival in Sydney, passengers would be required to isolate at home for 14 days from the last international port. Mrs Karpik says that given Mr Karpik’s deteriorating state of health, she was very relieved when she heard this announcement. [LAY_SKA.001.001.0083 [115]]
205 On 16 March 2020, Mrs Karpik heard an announcement over the ship’s PA system directing passengers with flu-like symptoms to report to the medical centre. Also on that day, Mr Karpik had a high temperature and had developed a slight dry cough and a sore throat. As a result, he and Mrs Karpik attended the ship’s medical centre. [LAY_SKA.001.001.0083 [116]-[118]]
206 Mrs Karpik says that an attendant at the medical centre took Mr Karpik’s temperature and Mrs Karpik filled in a form for Mr Karpik. She explained Mr Karpik’s symptoms, including very high temperatures and aches and pains to the attendant. The attendant said that Mr Karpik would be called if the ship’s doctor wished to see him, but that he could otherwise leave and was not required to stay in isolation. [LAY_SKA.001.001.0083 [120]-[121]]
207 That afternoon, Mr Karpik received a phone call asking him to attend the medical centre for examination, which he did. A nasal swab was taken. He was told to stay isolated in his cabin other than to return to the medical centre twice a day for medical review. [LAY_SKA.001.001.0083 [122]]
208 On 17 or 18 March 2020, Mr Karpik was informed that the results of the nasal swab showed that he had influenza A. On those days, being the final two days of the cruise, Mr Karpik reported twice daily to the medical centre as instructed. He was unwell, weak, breathless, and was experiencing continuing high fevers. [LAY_SKA.001.001.0083 [124]-[127]]
209 As dealt with in more detail in the section of these reasons dealing with the question of whether Mrs Karpik got COVID-19 (see section C.2), on or about 18 March 2020 she began to experience headaches and diarrhoea. [LAY_SKA.001.001.0083 [130]]
210 Mrs Karpik said that the final three days of the voyage were a very difficult time for her as she was worried about Mr Karpik and, on the last day, she was not feeling well herself. She nevertheless attended dinner with her friends on the last evening, 18 March 2020. [LAY_SKA.001.001.0083 [132]-133]]
B.8.4 Disembarkation and thereafter
211 Mr Karpik does not remember much of the disembarkation process on 19 March 2020. [LAY_SKA.003.001.0001 [41]]
212 That morning, Mrs Karpik observed that Mr Karpik had high temperatures, complained of aches and pains, appeared to be extremely fatigued, and was breathless, sweating, shaking and trembling. He also complained of a sore throat and had an occasional cough. He was barely able to walk and unable to carry his hand luggage. On the shuttle bus trip back home to Wollongong, Mr Karpik was delirious, continuously tried to remove his mask, did not speak, was restless, had a very high temperature and had difficulty breathing. [LAY_SKA.001.001.0083 [149]-[150], [155]]
213 When the Karpiks arrived home on 19 March 2020, Mr Karpik was feverish, breathless, very weak and was barely able to walk into the house. Mr and Mrs Karpik’s daughter, Fiona, who is a registered nurse, assisted Mr Karpik into the house and checked his temperature, pulse, respiration and blood pressure. Fiona expressed to Mrs Karpik that she was very concerned about Mr Karpik’s health. Mr Karpik had only been home resting for 30 minutes or so before Mrs Karpik drove him to the Coronavirus Testing Clinic at the Wollongong Hospital. [LAY_SKA.003.001.0001 [42]-[45]; [LAY_SKA.001.001.0083 [155], [161], 164]]
214 Acting on the advice of Mr Karpik’s General Practitioner, after Mr Karpik had been tested for coronavirus, Mrs Karpik took Mr Karpik to the Wollongong Hospital Emergency Department. Mr Karpik does not remember the conversation he had with the doctor there. Mrs Karpik explained to the doctor that she feared that Mr Karpik may have contracted COVID-19. Mr Karpik was assessed as well enough to go home, and Mrs Karpik was told to bring him back to the Emergency Department if his condition worsened. [LAY_SKA.003.001.0001 [46]] At home, Mrs Karpik managed Mr Karpik’s high temperatures with Panadol and encouraged fluid intake and soft foods. [LAY_SKA.001.001.0083 [165]-[166]]
215 On 20 March 2020, Mr Karpik was extremely weak and recording high temperatures of between 39.5 and 39.8 degrees. Mr Karpik’s oxygen saturation readings were about 94%. Mrs Karpik sat with Mr Karpik into the early hours of the morning, giving him Panadol to try to reduce his fever. [LAY_SKA.001.001.0083 [167]]
216 On the morning of 21 March 2020, it was clear to Mrs Karpik that Mr Karpik had deteriorated further. He was unable to sit upright in bed, and he was shaking so much that he was unable to hold a glass of water without spilling it. Mrs Karpik decided to call an ambulance and paramedics arrived at the house wearing full PPE. The paramedics examined Mr Karpik, performed tests including an electrocardiogram, and commenced intravenous fluids, before taking him to the Emergency Department at Wollongong Hospital. Mrs Karpik was unable to accompany Mr Karpik to hospital as she was required to remain in self-isolation at home. [LAY_SKA.001.001.0083 [170]-[171]]
217 Mr Karpik does not recall when he was told, or who told him, that he had tested positive for COVID-19. Mr Karpik’s last memory is being taken through the hospital doors by the paramedics. [LAY_SKA.003.001.0001 [47]-[48]]
218 In the afternoon of 21 March 2020, Mrs Karpik was informed that Mr Karpik had been admitted to the isolation section of the ICU at Wollongong Hospital. Mrs Karpik was also informed later that afternoon that Mr Karpik had tested positive for coronavirus and that his condition remained critical but stable. [LAY_SKA.001.001.0083 [173]-[174]]
219 On the afternoon of 22 March 2020, Mr Karpik called Mrs Karpik from the hospital. Mrs Karpik’s impression from the phone call was that his condition was improving. Shortly afterwards, Mrs Karpik received a call from an ICU Consultant who advised that Mr Karpik was doing quite well and that his condition remained critical but stable. [LAY_SKA.001.001.0083 [175]-[176]]
220 Mr Karpik was intubated at approximately 8:40pm that night. Later that evening, Mrs Karpik was informed that Mr Karpik had been intubated and ventilated, and that he had been placed in a medically induced coma. Mrs Karpik was shocked and completely devastated that no one had told her that this was going to happen at that time. The doctor apologised to Mrs Karpik and it was agreed that an ICU Consultant or their representative would call Mrs Karpik daily to update her on Mr Karpik’s condition. This period was incredibly distressing for Mrs Karpik, made worse by not being able to see her husband or speak face to face with his ICU team. Due to being overwhelmed by the situation, Mrs Karpik arranged for her son-in-law to communicate with hospital doctors on her behalf. [LAY_SKA.001.001.0083 [177]-[181]]
221 During a family teleconference on 27 March 2020, hospital staff advised Mr Karpik’s family that Mr Karpik’s condition was critical and deteriorating, his coronavirus infection markers were increasing, the infection had infiltrated his lungs and kidneys and was likely to infiltrate all vital organs. The medical team was finding it increasingly difficult to maintain his ventilation and there was no way that the medical team could stop this process. The family was advised that Mr Karpik only had about a 10% chance of survival, and probably only had three days to live.
222 Clinical notes from 27 March 2020 record that Mr Karpik had a “poor prognosis given ARDS and likely severe Cytoline [sic] storm.” [EXP.002.001.1516 p 59] Hospital staff indicated that the ICU team was considering transferring Mr Karpik to palliative care so that at least one family member, being someone not in isolation, could say goodbye to him on behalf of the family. Mrs Karpik was advised that she needed to nominate the relevant person and she was required to give a “Not for Resuscitation” order for Mr Karpik. Mrs Karpik described this day as the worst day of her life. She attempted to arrange a priest to visit Mr Karpik, who was still contagious, and began thinking about how she could arrange a funeral when she was in isolation and funerals were limited by proclamation to 10 people. Mrs Karpik also felt terrible that she could not comfort her children or other family members, including Mr Karpik’s 94-year-old mother, due to the fact that she was in isolation. [LAY_SKA.001.001.0083 [183]-[187]]
223 On 28 March 2020, a doctor informed Mrs Karpik that the ICU team had conducted video conferencing with ICU and infectious disease experts around the world to ascertain if there were any additional medical interventions that might assist Mr Karpik. On advice they had received, the ICU team proposed some additional interventions to give Mr Karpik a final chance of survival, being vigorous renal failure interventions and a different ventilation strategy. Mrs Karpik was warned that such interventions were “experimental” and that she should not get her hopes up. [LAY_SKA.001.001.0083 [188]]
224 Over the following days, Mr Karpik’s condition began to improve in small increments. His respiratory function stabilised, his inflammation reduced and his kidney function improved. [LAY_SKA.001.001.0083 [189]]
225 On 4 April 2020, when Mrs Karpik was permitted to come out of isolation, Mr Karpik remained in isolation. During this time, the ICU nurses assisted Mrs Karpik to FaceTime Mr Karpik. He was still ventilated and heavily sedated, however, on a few occasions, he was able to momentarily open his eyes. Around 6 April 2020, Mrs Karpik was advised by doctors at the hospital that they would start to begin gradually weaning Mr Karpik off the ventilator, but that this would be difficult as he had been anaesthetised and sedated for so long with consequent significant muscle de-conditioning. On 11 April 2020, Mr Karpik’s endotracheal tube was replaced with a tracheostomy tube to assist in weaning Mr Karpik off the ventilator. [LAY_SKA.001.001.0083 [190]-[193]]
226 On 12 April 2020, Mrs Karpik was able to visit Mr Karpik in hospital as he had returned two negative coronavirus tests. She had not seen him since 21 March 2020 (approximately three weeks). Mr Karpik was still heavily sedated and was ventilated via the tracheostomy. [LAY_SKA.001.001.0083 [194]-[195]]
227 From 12 April 2020 onwards, Mrs Karpik was able to visit Mr Karpik for one hour each day. Mr Karpik was totally reliant on nursing care, had no control over any part of his body, could not lift any part of his body off the bed, was confused and delirious, and could not eat, speak or drink because of the tracheostomy. [LAY_SKA.001.001.0083 [196]]
228 Mr Karpik was taken off sedation and commenced physiotherapy. Initially, the physiotherapy focused on helping Mr Karpik raise his head and arms off the bed, then repeat actions of sitting and lying, sitting on the side of the bed and, after a week or so, standing with assistance. Mr Karpik’s four children were able to visit him for the first time on 21 April 2020, his birthday. Mr Karpik was still ventilated and had a tracheostomy. [LAY_SKA.001.001.0083 [200]-[203]]
229 On 25 April 2020, Mr Karpik ceased ventilation support and his tracheostomy was removed. He was then able to speak and commence oral intake of thickened fluids, and was starting to be able to walk short distances, shower and toilet himself. [LAY_SKA.001.001.0083 [204]]
230 On 6 May 2020, after five and a half weeks in hospital, Mr Karpik was transferred to Figtree Private Hospital for rehabilitation, which involved physiotherapy to improve his muscle strength and mobility and occupational therapy to assist him with activities of daily living. [LAY_SKA.001.001.0083 [205]]
231 On 16 May 2020, Mr Karpik was discharged from Figtree Private Hospital and returned home. He had spent nearly two months in hospital. [LAY_SKA.001.001.0083 [209]]
232 After being discharged from hospital, Mr Karpik continued to suffer from reduced strength, breathlessness, an inability to close his fists and numbness in his fingers, a right shoulder injury and intense fatigue. He was unable to walk without the assistance of a four-wheel walker and, even when using the walker, he could only walk about 100 metres. Mrs Karpik had to guide Mr Karpik constantly when they were outside of their home. [LAY_SKA.001.001.0083 [210]-[211]]
233 After Mr Karpik had returned home, Mrs Karpik observed that he appeared distressed, anxious and depressed about how he was feeling physically, how much assistance he required and his lack of independence. From when Mr Karpik arrived home until mid-July 2020, Mrs Karpik was required to provide Mr Karpik with ongoing care and had to assist him with most daily activities including dressing, showering and supervising his eating. [LAY_SKA.001.001.0083 [212], [217]]
C. WERE MR AND MRS KARPIK INFECTED WITH CORONAVIRUS ON THE RUBY PRINCESS?
234 Mrs Karpik’s case turns in large part on whether Mr Karpik contracted COVID-19 on board the vessel during the cruise, ie, during the provision of the services by the respondents, and whether she contracted COVID-19 at all. There is a small part of her case which would survive even if those two questions were answered against her, but most of her case for damages turns on them.
C.1 When was Mr Karpik infected with coronavirus?
235 In the two weeks prior to boarding the Ruby Princess on 8 March 2020, Mr Karpik had not left the Wollongong Local Government Area. As mentioned, the Karpiks and their friends arrived at Circular Quay at approximately noon ahead of their scheduled boarding at noon and 2pm respectively. The Karpiks had lunch at a café and, due to the delayed embarkation, dinner with their friends at a hotel in The Rocks (T164:8-27). In the intervening period, Mr Karpik mostly sat on a bench, listened to music and attended to emails on his phone (T164:3-6). [LAY_SKA.001.001.0083 [64], [68]; LAY_SKA.003.001.0001 [9], [11], [12], [14]]
236 It will be recalled that Mr Karpik first experienced symptoms of being unwell on 12 March 2020 at around 8am when the vessel arrived at its first port of call, Port Chalmers in Dunedin. His symptoms that morning included feeling weak, tired and lethargic, and his bones were aching. Later that evening, he had no appetite for dinner. On 13 March 2020, he had a fever. On 14 March 2020, he was experiencing high temperatures. On 16 March 2020, Mr Karpik was swabbed on board the vessel to be tested for influenza A. That test returned a positive result on 17 March 2020. On 19 March 2020, after the Karpiks disembarked from the vessel, Mr Karpik was taken by Mrs Karpik to Wollongong Hospital to be tested for COVID-19. That test returned a positive result on 21 March 2020. [LAY_SKA.001.001.0083 [99], [103], [110], [164], [174]; LAY_SKA.003.001.0001 [25], [26], [29], [36], [39], [45]]
237 Associate Professor Yakob was instructed by the respondents to provide an opinion as to whether Mr Karpik contracted COVID-19 prior to boarding the vessel and he produced an expert report addressing this topic. Professor Holmes and Professor Wilder-Smith gave opinion evidence in reply to Associate Professor Yakob’s report. They were joined in conclave on this topic by Professors Rocklöv and Paterson, following which a joint report (Joint Report 6) was produced.
238 There are numerous expert reports that are relevant to the determination of this issue. They include: Associate Professor Yakob’s report; Professor Holmes’ report; Professor Wilder-Smith’s report in reply; Joint Report 1, which concerns the characteristics of coronavirus; Joint Report 3, which concerns the risk of contracting COVID-19 on a cruise ship as compared to in the community generally; and Joint Report 6, which directly addresses the question of the probability that Mr Karpik was infected prior to boarding.
239 The relevance of Joint Report 1 is the respondents’ reliance on the experts’ agreement that the median incubation period for the Wuhan strain of the virus was considered to be 5-6 days as at 8 March 2020. [JNT.001.001.0001 [7]] Joint Report 3 is relevant to the evidence given by Professor Wilder-Smith concerning contact rates and the heightened risk of contracting COVID-19 on a cruise ship when compared to the general community, which issues I have already determined in favour of Mrs Karpik in section B.5.3 above.
(1) Associate Professor Yakob’s report
240 The respondents instructed Associate Professor Yakob. As mentioned, he is Associate Professor of Infectious Diseases at the London School of Hygiene & Tropical Medicine.
241 Associate Professor Yakob was instructed to provide an opinion in answer to the following question:
Please calculate the likelihood that Mr Henry Karpik was infected with COVID-19 prior to boarding the Ruby Princess on 8 March 2020.
(Emphasis added.)
242 Associate Professor Yakob’s approach to answering that question may be summarised as follows.
243 He observed that there is a range of possible values which the incubation period (ie, the time between exposure to the virus and exhibiting symptoms of infection) of any pathogen in any particular individual may take. He therefore needed a comprehensive range of incubation period values reported for coronavirus. Because incubation periods were reported to have shortened with subsequent variants of the virus, he only reviewed the reported incubation periods for infections prior to the voyage. He also limited his review to include only studies reporting cases where the exposure window and date of symptom onset were clearly defined. [EXP_RES.001.001.1326 [21]; EXP_RES.001.001.1326_Fig5]
244 On the basis of data pooled from studies he reviewed in accordance with those limitations, he produced a probability distribution of incubation periods depicting the likelihood of an incubation period for all values (ie, days) within a range. The shape of the distribution, which is right-skewed log normal, was determined by two parameters that were calculated from the mean and the standard deviation as reported in those studies. [EXP_RES.001.001.1326 [22]-[24], [26]]
245 The probability distribution thus produced was used to determine an average incubation period of 5.8 days, which Associate Professor Yakob observed to be in line with the estimates of other studies. The distribution can also be used to determine the likelihood of an incubation period shorter than any given length of time. [EXP_RES.001.001.1326 [25], [27]-[28]]
246 In the present case, Associate Professor Yakob assumed that if Mr Karpik was infected after boarding the vessel, his incubation period was shorter than 3.5 days. That was on the basis that he boarded the vessel at 8pm on 8 March 2020 and began experiencing symptoms at 8am on 12 March 2020 (T620:18-26). He calculated the likelihood of an incubation period of shorter than 3.5 days at 22.5% (with a 95% confidence interval of 14%-31.4%, the point estimate of 22.5% expressed to be the mean). [EXP_RES.001.001.1326_Fig2] On that basis, he found that 77.5% of COVID-19 cases had an incubation period of longer than 3.5 days. He then concluded as follows: [EXP_RES.001.001.1326 [31]-[32]]
I find there to be a 77.5% probability (95% CI 68.6-86.0) that Mr Karpik was already infected when he boarded the Ruby Princess cruise.
247 Mrs Karpik instructed Professor Holmes in reply to Associate Professor Yakob’s evidence. As mentioned, Professor Holmes is Professor of Biology and Medicine at the University of Sydney.
248 Professor Holmes was instructed to provide an opinion in answer to the following question:
What is the likelihood that Mr Henry Karpik contracted COVID-19 prior to boarding the Ruby Princess on 8 March 2020.
(Emphasis added.)
249 Professor Holmes approached this question by responding to Associate Professor Yakob’s report, noting that Professor Holmes was not asked to “calculate” the likelihood of Mr Karpik having contracted COVID-19 on the voyage, but rather to express its likelihood. Professor Holmes criticises Associate Professor Yakob’s report in two primary respects.
250 First, Professor Holmes says that Associate Professor Yakob wrongly assumes that the symptoms first experienced by Mr Karpik on the morning of 12 March 2020 were caused by COVID-19. Because there was no ability to test for the virus on the vessel, and because the symptoms of influenza A and COVID-19 are similar, it is not clear on the evidence as to whether (a) Mr Karpik first contracted influenza A and then COVID-19 only later, (b) Mr Karpik first contracted COVID-19 and then influenza A only later, or (c) Mr Karpik was co-infected with both COVID-19 and influenza A at a similar time.
251 Professor Holmes considers it likely that Mr Karpik’s symptoms on 12 March 2020 were caused by influenza and that he was only infected with COVID-19 later in the voyage. That is on the basis of the positive influenza test taken on 16 March 2020, and the far higher prevalence of influenza as compared to COVID-19 in NSW at the time. [EXP_SKA.003.003.0141 [25]]
252 Secondly, Professor Holmes criticises Associate Professor Yakob for failing to consider the fact that the prevalence of COVID-19 cases in Australia at 8 March 2020 was very low. That low prevalence means that the probability of Mr Karpik being infected with COVID-19 in the general population prior to boarding the vessel was also very low. [EXP_SKA.003.003.0141 [27], [30]]
253 Further, Professor Holmes considers that the risk that Mr Karpik was infected prior to boarding would still be very low even taking into account undetected cases, of which he agreed in cross-examination (T555:27-30) and in Joint Report 6 that there must be some. [JNT.001.001.0045 [8]; EXP_SKA.003.003.0141 [32]]
254 Finally, Professor Holmes observed that although an incubation period of 3.5 days for the virus is shorter than the mean, it is nonetheless within the usual distribution. Indeed, in Associate Professor Yakob’s own calculations, more than 1 in 5 people have an incubation period of less than or equal to 3.5 days. [EXP_SKA.003.003.0141 [33]]
255 Professor Holmes concluded that, on the balance of probabilities, Mr Karpik was infected on board the vessel. [EXP_SKA.003.003.0141 [20]]
(3) Professor Wilder-Smith’s reply
256 Professor Wilder-Smith was also instructed to provide an opinion in reply to Associate Professor Yakob’s evidence. Her comments are broadly similar to the criticisms made by Professor Holmes.
257 First, she says that Mr Karpik’s onset of fever on 13 March 2020 could either be due to COVID-19 or influenza. However, because there were no COVID-19 tests on board, it cannot be determined whether or not his symptoms early in the voyage were caused by COVID-19 or influenza. In any event, she says that even assuming that the onset of his symptoms was caused by coronavirus infection, the incubation period would nonetheless be within the reported range of the Wuhan variant. [EXP_SKA.003.003.0226 [73]]
258 Secondly, she says that Associate Professor Yakob’s singular focus on the incubation period is misplaced and that the more pertinent question is the probability of Mr Karpik being exposed and thereby infected prior to boarding the vessel. She points out that the number of reported cases in NSW at that time was very low (40) and that, in any event, most of the cases were in Sydney and there were none in Wollongong. On that basis, she concludes that Mr Karpik’s risk of exposure before boarding was “exceedingly low.” On the other hand, she observes that there were approximately 4,000 people on board the vessel and that, given that a COVID-19 outbreak occurred on board, there must have been at least one case on board. That higher incidence rate, coupled with a higher concentration of people having regard to the floor area on the vessel, meant that Mr Karpik’s risk of exposure was far higher once on board in comparison to the risk in the community in NSW. [EXP_SKA.003.003.0226 [74]-[79]]
259 On the basis of Mr Karpik’s incubation period being within the reported range even if the symptoms he first experienced were caused by COVID-19 and the higher risk of exposure on the vessel, Professor Wilder-Smith concluded that it is much more likely that Mr Karpik contracted COVID-19 on the vessel than prior to boarding. [EXP_SKA.003.003.0226 [80]-[81]]
260 Professor Wilder-Smith was cross-examined on both the incubation period issue and the cruise ship risk. I have already dealt with the risk of contracting COVID-19 on a cruise ship when compared to the general community above. In relation to the incubation period, a topic on which considerable time was spent in cross-examination, Professor Wilder-Smith did not accept that a median incubation period was the most probable. Nor did she accept that selecting a period of one day either side of the median entailed moving outside of the confidence interval (T533:41-534.9). She emphasised that the most important factor in relation to the incubation period is the range (ie, interval in confidence or credible interval) and that the precise median does not matter (T536:15-20).
261 As mentioned, Associate Professor Yakob and Professors Holmes and Wilder-Smith were joined by Professors Rocklöv and Paterson in conclave. Notwithstanding that only Associate Professor Yakob and Professors Holmes and Wilder-Smith opined in their individual reports on the likelihood that Mr Karpik was already infected with COVID-19 prior to boarding vessel, the question which they (ie, all five experts) addressed in conclave was “the probability that Mr Karpik was infected prior to boarding RU2007.” Save for Professor Rocklöv, who generally agreed with Professors Holmes and Wilder-Smith, each of the experts provided different reasons for their disagreements with each other on the topics on which they disagreed. [JNT.001.001.0045 [32]]
262 The experts were in agreement as to the following: [JNT.001.001.0045 [3]-[8]]
(1) There were more documented cases of influenza than COVID-19 in NSW on 8 March 2020.
(2) The prevalence of COVID-19 in Wollongong prior to boarding the vessel was “at least low.”
(3) The symptoms of influenza and COVID-19 are similar.
(4) Coinfection with influenza and coronavirus is rarer than an infection with either alone, although concurrent infections are reported.
(5) The likelihood of Mr Karpik getting infected prior to boarding the vessel is dependent on his risk of exposure to the virus in the general population of NSW and does not only depend on the viral incubation period.
(6) The true prevalence of COVID-19 at 8 March 2020 was underreported both in the general community as well as on cruise ships due to the general lack of and access to testing and seroprevalence data.
263 There were four areas of disagreement between the experts. They were:
(1) the level of risk in Wollongong;
(2) the true prevalence of COVID-19 in NSW;
(3) the significance of the Karpiks’ trip to The Rocks prior to boarding; and
(4) the significance and reliability of the influenza test taken by Mr Karpik.
264 I will consider each of these areas of disagreement in turn, taking (1) and (2) together.
(a) Prevalence and risk of COVID-19 in Wollongong and NSW
265 The experts disagreed about the level of risk in Wollongong. As mentioned, they agreed that the level of risk was “at least low.” Associate Professor Yakob and Professor Paterson were of the view that the risk was “low”; Professors Wilder-Smith, Holmes and Rocklöv were of the view that the risk was “very low.” This is a question of semantics that is ultimately unhelpful in finding the right answer to the question at hand.
266 Professor Wilder-Smith says that what really matters to the probability of whether Mr Karpik was infected prior to boarding the vessel is the relative risk of exposure. In that regard, Associate Professor Yakob agreed in cross-examination that relative risk of exposure is a relevant factor which he did not consider (T620:44-46).
267 In respect of NSW, all the experts agreed that the true prevalence of COVID-19 in NSW at 8 March 2020 was underreported. In that regard, Professor Wilder-Smith opined that the same reasons for that apply equally to reporting in other countries from which the passengers that boarded the vessel came, as well as settings such as the voyage itself – ie, she says that true cases were underreported everywhere. [JNT.001.001.0045 [16]] The pertinent disagreement recorded in this section of Joint Report 6 is that between Associate Professor Yakob and Professor Holmes concerning the extent to which COVID-19 was prevalent in NSW.
268 In that regard, Associate Professor Yakob argued that the extent of underreporting of the actual prevalence of COVID-19 in NSW at the time was significant. He came to that view on the basis of an assumption concerning delays between the time of infection and notification to health authorities, and published serosurvey findings. [JNT.001.001.0045 [12]]
269 Dealing first with the timing of infections, Associate Professor Yakob observed that although the peak of reported infections for the first wave of COVID-19 in NSW was between 24-28 March 2020, adopting a notification delay of between 2-3 weeks, which was the delay reported by the Government of the United Kingdom, meant that the true peak of transmission was sometime between 3-14 March 2020. [JNT.001.001.0045 [12(c)]]
270 In respect of the serosurvey findings, Associate Professor Yakob referred to a journal article reporting the results from data (ie, blood specimens) collected between 19 June 2020 and 6 August 2020 from general pathology testing, antenatal screening and blood donors. In total, 11,317 specimens were collected from all Australian jurisdictions. The authors of that article estimated that the cumulative COVID-19 infections nationally was 64,100 (with a 95% credible interval of 7,700-138,500). In percentage figures, that is 0.25% (with a 95% credible interval of 0.03-0.54%). That is in contrast to the cumulative number of reported infections being 7,636. [JNT.001.001.0045 [12(d)]]
271 In the report, Associate Professor Yakob referred to data that was said to corroborate a COVID-19 outbreak in Australia in March 2020 of over 60,000 infections. That data included a study that estimated the fatality rate of COVID-19 at around 0.47% (with a 95% confidence interval of 0.22-0.84), which would equate to around 300 excess deaths (ie, deaths exceeding historic averages) in late March/early April 2020. In respect of the number of excess deaths in Australia at the time, Associate Professor Yakob referred to data from the Australian Bureau of Statistics that indicated that the deaths in the weeks ending 24 March 2020, 31 March 2020 and 7 April 2020 exceeded historic averages by 624 in total. The conjunction of those two sets of data was said to support a conclusion that there was an outbreak of over 60,000 COVID-19 infections in Australia in March 2020. [JNT.001.001.0045 [12(e)-(h)]]
272 In response, Professor Holmes considered it to be inappropriate to generalise the reporting delay in the UK of 2-3 weeks to NSW. He said that not only is there no evidence that the reporting delay in Australia or NSW was the same as the UK, but comprehensive modelling analysis suggests otherwise. [JNT.001.001.0045 [13(a)(vi)]] Professor Paterson also agreed that the reporting delay in Australia would have been shorter than 2-3 weeks. [JNT.001.001.0045 [15]]
273 Associate Professor Yakob was cross-examined on this point. He conceded that he did not know if the reporting delay in the UK applied in Australia. He also gave evidence that since he had prepared his report he had come across information which suggested a delay in reporting time in Australia of closer to 10 days. He accepted that if the reporting delay in Australia was in fact 10 days, then the peak of infections in NSW would be 14-18 March 2020, which is well after the vessel had departed (T622:33ff).
274 In relation to the inferences Associate Professor Yakob sought to draw from the serosurvey findings, Professor Holmes observed that the reported confidence intervals are “huge” and that the lower bound of undetected cases was only 7,700 cases. He also referred to comprehensive modelling analysis that concluded that there were fewer than 100 new COVID-19 infections in Australia on 8 March 2020 (that being the top end of a 95% confidence interval) and the mean estimate was approximately 50 infections. [JNT.001.001.0045 [13(a)(iv)], [14]] That modelling analysis, in conjunction with the reported data on infections in NSW and the fact that the majority of reported cases were acquired overseas, led Professor Holmes to opine that the risk of infection in the general population of NSW at the time of the vessel’s departure was “very low.” [JNT.001.001.0045 [13(b)]]
275 In cross-examination, Associate Professor Yakob confirmed that he considered the credible intervals of the serosurvey’s conclusions to be “large” (T623:34). He also clarified that he did not adopt the study’s conclusions and that his only contention in respect of the true number of infections was that there was a large number of unreported cases (T622:5-21). That is to say, he did not adopt the figure of 60,000 true infections in Australia in the first wave; he intended his reference to the study as “another piece of evidence” (T623:16). He went on to concede that the study is not a very good indicator of the extent of COVID-19 as at March 2020, in part because of the time at which blood specimens were collected (T624). He also agreed that even if the findings of the serosurvey study were correct, an infection rate of 0.25% is still a low prevalence (T623:29-32).
276 In my view, Associate Professor Yakob’s reasoning relies on too many unfounded assumptions. First, as Professor Holmes points out, there is no evidence to support the assumption that the reporting delay in Australia was the same as in the UK. Secondly, as Associate Professor Yakob accepted, the credible intervals of the serosurvey that he cites have a significantly large range: from 7,700 (which is barely more than the reported cases) to 138,500. In any event, he does not adopt the findings of the serosurvey and conceded that it is not a very good indicator of the extent of COVID-19. Further, even if it were, he accepted that the 0.25% estimate would still constitute a low prevalence. For those reasons, I prefer the analysis of Professor Holmes.
277 I therefore find that although the true prevalence of COVID-19 in NSW as at 8 March 2020 was underreported, it was nonetheless very low. I also find that the level of risk in Wollongong was very low. That means that with reference to the level of risk and prevalence, and leaving other considerations to one side for the time being, it is highly unlikely that Mr Karpik was infected with the virus in Wollongong.
(b) The Karpiks’ trip to The Rocks prior to boarding
278 The experts disagreed on the significance of Mr Karpik’s excursion to The Rocks whilst awaiting embarkation of the vessel.
279 Joint Report 6 records that the disagreement between Professor Holmes and Associate Professor Yakob follows from their disagreement concerning the true prevalence of COVID-19 in NSW. [JNT.001.001.0045 [22]] However, it does not actually record what their respective views are and nor do their individual expert reports address this question. Their views can nonetheless be inferred from the ultimate conclusions they advance: namely, that Professor Holmes considers Mr Karpik’s excursion to be insignificant and Associate Professor Yakob considers the excursion to be significant.
280 Professor Holmes contends that if, on the basis of Associate Professor Yakob’s assumed views concerning the significance of Mr Karpik’s excursion, Associate Professor Yakob were to propose that Mr Karpik was infected during his excursion prior to boarding, then that would still mean that Mr Karpik’s incubation period was shorter than the mean. The point he makes is that Associate Professor Yakob cannot argue that Mr Karpik was infected in The Rocks whilst consistently maintaining his reasoning as to why Mr Karpik was already infected prior to boarding the vessel. [JNT.001.001.0045 [23]]
281 Professor Wilder-Smith considers that it is not possible to conclusively pinpoint when Mr Karpik’s infection occurred. However, she says that the probability of Mr Karpik’s exposure to the virus was far higher at or after boarding than it was prior to boarding. In reaching that conclusion, she relies on the following: [JNT.001.001.0045 [24]]
(1) The contact rates, contact frequencies and number of contacts were higher during and after boarding than in any restaurant setting in The Rocks: nearly 3,000 passengers boarded over several hours and various witnesses reported overcrowding during the safety muster.
(2) Even on an estimate of one COVID-19 positive case only, that would mean one case in a limited geographic area of approximately 0.32 km2.
(3) There were 40 reported cases in NSW, most of which were in Sydney. New South Wales has a population of approximately 8.1 million people and Sydney has a population of approximately 5.312 million people.
(4) Even on an underreporting factor of 5, there would have been roughly 200 cases in Sydney over a geographic area of approximately 12,368 km2 (which in any event does not take account of duplicated floor areas in multiple-level buildings).
(5) The risk exposure of spending a few hours in Sydney was therefore far lower than the risk of exposure whilst boarding and remaining on the vessel.
282 Both Professors Wilder-Smith and Paterson observe that both potential exposures (ie, The Rocks excursion or boarding and remaining on the vessel) are within the same incubation period. Perhaps at least partly for this reason, the respondents in their closing submissions place no reliance on the hypothesis (debated by the experts) that Mr Karpik was infected on 8 March 2020 at The Rocks as opposed to at or after boarding. For that reason, it is unnecessary to consider the risk at The Rocks separately from NSW more generally. That is to say, the question remains whether Mr Karpik contracted COVID-19 before boarding the vessel, or on the vessel.
(c) The influenza test taken by Mr Karpik
283 Neither side of the case relies on Mr Karpik’s influenza swab in their closing submissions. For that reason, the disagreements between the experts on this topic need not be canvassed. It is, however, accepted by the experts that it is possible that Mr Karpik’s initial symptoms were from an infection of influenza and that he only later contracted COVID-19.
284 The respondents submit that the experts agree in Joint Report 1 that the median incubation period was 5-6 days, which they observe is consistent with Associate Professor Yakob’s evidence of a mean incubation period of 5.8 days. They submit that 5.8 days should be the incubation period adopted for Mr Karpik. They further say that, in circumstances where Mrs Karpik does not challenge Associate Professor Yakob’s calculation per se, the conclusion that there is a 77.5% probability that Mr Karpik contracted COVID-19 prior to boarding the vessel should be accepted, with the result that the Court should find that Mr Karpik was infected with COVID-19 prior to boarding the vessel.
285 On the issue of the true prevalence of COVID-19 in the community, they observe that all the experts agree that the true prevalence in the community was underreported and that the extent of the disagreement was “in essence, as to the intensifier to be applied to the description of the prevalence as low” and, as such, Associate Professor Yakob was quite right in deciding not to incorporate uncertain data into a probability analysis.
286 Putting to one side the point that a median of some point between 5-6 days is not necessarily consistent with a mean of 5.8 days, and noting that the cross-examination of Professor Wilder-Smith concerned, in part, the issue of whether the median incubation period is the most probable, the contention now advanced that the mean incubation period should be adopted as Mr Karpik’s likely incubation period cannot be accepted. That demonstrates a misunderstanding of the concept of mean (and median). A mean is merely the average value within a set of data, whereas the median is the middle value in the set of data and is therefore not affected by extreme values (or outliers). It is elementary mathematics that a mean is sensitive to outliers that can skew the distribution. There is no basis at all on which it can be said that, because the value produced by adding up the individual values in a set of data and dividing by the total number of values results in 5.8, that then should be taken to be Mr Karpik’s likely incubation period. Acceptance of that would entail accepting that Mr Karpik was most likely infected in Wollongong on 6 March 2020, which is a conclusion that is not credible in circumstances where, as at 8 March 2020, there were no reported cases of infected persons residing in the Wollongong Local Government Area and Mr Karpik was not suggested to have been in a high risk environment at that time.
287 Turning now to Associate Professor Yakob’s opinion in respect of the probability of Mr Karpik being infected with the virus prior to boarding the vessel, that opinion takes as its basis a probability distribution based on raw data published in other studies of observed incubation rates. The “probability” distribution must therefore be a frequentist distribution and the probability that it expresses is equivalent to frequency. In that regard, it may be accepted that, on a statistical analysis of the coronavirus variant then circulating within the community, the average incubation period was 5.8 days and that in only 22.5% of cases (or, more accurately, between 14% and 31.4% of cases) is the incubation period shorter than 3.5 days. As is apparent from the summary of Associate Professor Yakob’s report above and also accepted by him in cross-examination, that is the kind of probability he was calculating (T620:31-32).
288 On the basis of that statistical distribution, Associate Professor Yakob then asserts that the probability of Mr Karpik having been infected with the virus prior to boarding the vessel is 77.5%. That conclusion of probability being expressed could not be a frequentist probability; rather, it could only be either a propensity or a Bayesian probability. The respondents then seek to rely on that conclusion in submitting that I should find, on the balance of probabilities, that Mr Karpik was already infected with the virus when he boarded the vessel. Such reasoning and the respondents’ reliance on it as such is untenable.
289 The problematic use of such statistical evidence to reason to a conclusion on the balance of probabilities has been discussed in cases of medical negligence concerning loss of a chance. In that regard, in Gregg v Scott [2005] UKHL 2; [2005] 2 AC 176 at [28] Lord Nicholls (in dissent) observed:
Statistical evidence … is not strictly a guide to what would have happened in one particular case. Statistics record retrospectively what happened to other patients in more or less comparable situations. They reveal trends … They are general in nature. The different way other patients responded in a similar position says nothing about how the claimant would have responded. Statistics do not show whether the claimant patient would have conformed to the trend or been an exception from it. They are an imperfect means of assessing outcomes even of groups of patients undergoing treatment, let alone a means of providing an accurate assessment of the position of one individual patient…
290 Similarly, in Naxakis v Western General Hospital [1999] HCA 22; 197 CLR 269 at [35], Gaudron J observed that “a statistical chance is not the same as a personal chance.” And in State Government Insurance Commission v Laube (1984) 37 SASR 31 at 33, King CJ said that “the statistical fact that a particular proposition is true of the majority of persons cannot of itself amount to legal proof on the balance of probabilities that the proposition is true of any given individual.”
291 Those observations apply equally to the use sought to be made of Associate Professor Yakob’s statistical evidence in the present case. That more than half but fewer than 4 in 5 people infected with the relevant coronavirus variant had an incubation period longer than 3.5 days says nothing about Mr Karpik’s probabilities: neither the probability of his infection having an incubation period of 3.5 days or less nor the probability of him having been infected with the virus prior to boarding the vessel. There is no evidence in the case going to the former (eg, evidence concerning what factors cause incubation periods to be longer in some people and shorter in others and whether those factors were present in the case of Mr Karpik) and Associate Professor Yakob says nothing about relative exposure risk such as to have been able to form any opinion about the latter. I therefore reject the conclusion Associate Professor Yakob expresses in his report and the respondents’ identical submission.
292 Nonetheless, Associate Professor Yakob’s evidence that 77.5% (95% CI, 68.6-86.0) of those infected with the virus have a longer incubation period than 3.5 days is of some (limited) value in determining whether Mr Karpik was infected prior to boarding the vessel. In that regard, I accept the evidence of Professors Holmes and Wilder-Smith to the effect that a hypothesised incubation period of 3.5 days for Mr Karpik is still within the normal distribution. I also accept that, in 4 out of 5 cases, the incubation period would have been longer.
293 As mentioned, Associate Professor Yakob conceded in cross-examination that relative risk of exposure is a relevant factor which he did not consider. Nonetheless, the respondents seek to justify his failure in taking those factors into account as being too uncertain. I reject that contention; that data is simply unquantified or, perhaps, unquantifiable. That does not thereby make it uncertain that, as I have already found, the risk of exposure in Wollongong and in NSW generally was very low at the time. Nor does it make it uncertain that there is a heightened risk of coronavirus on board cruise ships by reason of higher population density leading to higher contact rates. On any view, the geographical size of Sydney or NSW is at least many thousands, if not tens or even hundreds of thousands, of times larger than the surface area of the vessel. That observation holds true without even taking into account the many different floors of buildings onshore.
294 As reliance on the supposition that Mr Karpik was infected in The Rocks was not pressed by the respondents, the alternatives presented to me are either that he was infected on 6 March 2020 in Wollongong or on 8 March 2020 on the vessel. Because the risk exposure on the vessel was far higher than in Wollongong and, indeed, in Sydney, and because an incubation period of 3.5 days is within the usual range calculated by Associate Professor Yakob, I find that it is more probable than not that Mr Karpik was infected with coronavirus on board the vessel.
C.2 Was Mrs Karpik infected with COVID-19 at all?
295 The parties disagree on whether Mrs Karpik was infected with coronavirus at all. As will be seen, that arises principally out of a disagreement between the parties’ experts about how to interpret the results of the various tests that she undertook, although there is also disagreement on whether she suffered symptoms of COVID-19 when still on board the vessel.
296 It is common ground that if Mrs Karpik contracted COVID-19, she most likely contracted it from Mr Karpik (T857:30). After all, she shared a cabin and a bed with him throughout the voyage, and she did not wear a mask when she was in the cabin with him (T178:15).
297 Given the relatively mild symptoms that Mrs Karpik suffered if she did have a COVID-19 infection, and the relatively mild and short-lived Long COVID symptoms she suffered even if she did suffer from Long COVID, the parties put disproportionate resources into the question of whether Mrs Karpik contracted COVID-19. On any view, the resolution of this issue one way or the other cannot have very significant monetary value. Be that as it may, in order to resolve the issue, the competing expert evidence must be grappled with.
298 Mrs Karpik’s evidence in chief was that on 18 March 2020, she began to experience headaches and diarrhoea on the cruise which at the time she attributed to something she had eaten or the stress that she was experiencing due to Mr Karpik’s poor health. [LAY_SKA.001.001.0083 [130], [227]]
299 At about midday on 19 March 2020 when she arrived home with Mr Karpik, Mrs Karpik was “still not feeling well.” When she took her husband for a coronavirus test that afternoon she sought to be tested herself but was refused a test. [LAY_SKA.001.001.0083 [162]-[164]]
300 On 21 March 2020, Mrs Karpik reported that she was very tired, was experiencing headaches, was not sleeping, had diarrhoea and that she was not sure whether these were symptoms of the virus or of her anxiety. [LAY_SKA.001.001.0083 [229]]
301 On 22 March 2020, she was highly distressed and totally exhausted and continued to experience headaches and diarrhoea. She was also experiencing nausea and breathlessness when walking up the internal staircase and around the exterior of her home – bearing in mind that she was in isolation at that time. [LAY_SKA.001.001.0083 [231]]
302 On 24 March 2020, Mrs Karpik noticed that she had a “scratchy” throat and an occasional dry cough. [LAY_SKA.001.001.0083 [234]]
303 Mrs Karpik was challenged in cross-examination on her evidence that she experienced symptoms while on board the vessel. There were in essence two challenges.
304 The first challenge was in relation to her evidence that it did not occur to her at the time that her symptoms might be from the same illness as her husband, who had by then tested positive for influenza A. That was notwithstanding that she was trained as a nurse, she had shared a cabin and a bed with her husband for many days, he was ill with a potentially life-threatening disease, and his early symptoms included headaches which she said she was suffering from. She had to say that it had not occurred to her that she was ill, as opposed to having eaten something off and/or suffering from stress, because she could not otherwise explain why she had not reported to the medical centre and she had continued to dine with her friends, including a friend who had compromised health.
305 The second challenge was in relation to her failure to mention any symptoms suffered by her when on board the vessel in a statement that she made to the NSW Police for the purposes of the Special Commission of Inquiry into the Ruby Princess.
306 The statement was taken by a police officer in interviews with Mrs Karpik at the Wollongong Police Station on 13 and 29 April 2020 (T172:5-10). It was ultimately signed on 2 May 2020. Mrs Karpik’s evidence, which I accept as inherently probable, is that she was “in an awful pickle” at that time of her life (T171:35). [SKA.003.001.0001; SCI.001.001.2731]
307 The police statement does not say anything about Mrs Karpik reporting that she had suffered symptoms when on board the vessel, although it is not apparent that she was asked anything that might have caused her to report such symptoms if she had had any. However, in the statement Mrs Karpik said that by 22 March 2020 she was totally exhausted and distressed and that she had symptoms of fatigue, diarrhoea, nausea and headaches but that she did not know if they were from COVID-19 or stress. [SCI.001.001.2731 [69]]
308 I accept Mrs Karpik’s evidence that she first started experiencing symptoms of diarrhoea and headaches on 18 March 2020 when still on board. That is for the following reasons.
309 First, she reported that Mr Karpik’s first symptoms were that he was “feeling very tired and achy” and “not feeling [him]self” (12 March), “unwell”, “tired and achy”, “aches and pains” and irritable and loss of appetite and running a temperature (13 March), and weak with aches and pains and having a high temperature (14 March). He did not complain specifically of headaches, and he did not complain of diarrhoea at all. It is therefore not surprising that Mrs Karpik did not think that her symptoms might be from the same illness as his. [LAY_SKA.001.001.0083 [99]-[110]]
310 Secondly, I accept that Mrs Karpik was feeling highly stressed towards the end of the voyage so it is quite plausible that she thought that her symptoms arose from that.
311 Thirdly, she was not asked how severe the symptoms were at that time. It may be that they were not particularly acute. That would explain why she did not mention them to the police officer, who in any event may not have asked any question of her that might naturally have caused her to mention symptoms at that stage – her symptoms, if any, were not of any particular relevance to the purpose of the police statement. In contrast, it is highly plausible that in preparing her statement her lawyers specifically asked her when she first started suffering from symptoms as that is a relevant matter in the proceeding.
312 Fourthly, it was not established that Mrs Karpik thought that symptoms of headaches and diarrhoea were consistent with influenza A or COVID-19, in particular where she said that she considered COVID-19 to be a respiratory disease, about which she did not know much in particular at the time (T141:47, T143:10-17). On that basis it is not surprising that she did not consider that she was ill (other than stress and/or having eaten something that caused the diarrhoea).
313 Finally, she reported various symptoms including headaches and diarrhoea on 21 and 22 March 2020. She was not challenged on that evidence which I therefore accept. If she suffered those symptoms then, it is quite possible, and even probable, that she also suffered them a few days before.
C.2.3 Mrs Karpik’s SARS-CoV-2 tests
314 On 27 March 2020, Mrs Karpik decided to get tested for coronavirus as soon as possible so as not to be in isolation if Mr Karpik was transferred from hospital to palliative care where she would otherwise be able to visit him. [LAY_SKA.001.001.0083 [236]]
315 On 28 March 2020, 10 days after her reported symptom onset on 18 March, Mrs Karpik underwent a reverse transcriptase polymerase chain reaction (PCR) test for SARS-CoV-2, which detects the presence of a virus genome in a specimen. A few days later, the test returned a “not detected” result. The test was done on a nasopharyngeal swab. [JNT.001.001.0056 [10]; RESsub_WLH.001.001.0001 p 28]
316 Mrs Karpik reported that from about 19 April 2020, she started to leave the house to exercise by walking. It was then that she noticed that the breathlessness that she had previously experienced had persisted and was worse than she had anticipated. On expressing her concern to her general practitioner (GP), Dr Crocker, that her PCR test was a false negative, she was referred for a coronavirus antibodies test. [LAY_SKA.001.001.0083 [241]-[243]]
317 On 20 April 2020 and 19 September 2020, Mrs Karpik’s blood was collected for serological testing. The serological assays (ie, tests) used on each occasion were different. A serology test does not detect the presence of a virus genome, but rather measures antibodies, also known as immunoglobulins, which are proteins produced in response to a specific antigen. In that regard, they are diagnostic of past infection rather than present infection (T516:28-31). [EXP_RES.002.001.0001 [8.24], [8.28]; EXP_SKA.003.003.0001 [72]]
318 The blood specimen taken on 20 April 2020 was tested using an immunofluorescence assay (IFA) at Westmead Hospital. [EXP_SKA.003.003.0001 [7]-[8]] The results were reported as follows: [RESsub_CFM.003.001.0001 p 321]
Sars-COV-2 IgA IF 20
Sars-COV-2 IgM IF <10
Sars-COV-2 IgG IF 80
These results are suggestive of recent infection with SARS-CoV-2 virus.
319 IgA, IgM and IgG in the left-hand column refer, respectively, to Immunoglobulin A, Immunoglobulin M and Immunoglobulin G. [EXP_SKA.003.003.0001 [9]-[11]] They are measured in the right-hand column above in “titres”, which measure the relative (ie, not absolute) quantity of antibody in the specimen. [EXP_SKA.003.003.0001 [12]] Titres greater than 10 are consistent with detection of anti-coronavirus antibodies. [EXP_SKA.003.003.0001 [12]]
320 The blood specimen taken on 19 September 2020 was tested first by Southern Pathology using two commercial assays, namely the Roche Elecsys Anti-SARS-CoV-2 and the Diasorin Liaison SARS-CoV-2 S1/S1 IgG assays. Its report dated 22 September 2020 provides as follows: [RESsub_CFM.003.001.0001 p 327]
SARS-CoV-2 Antibody Detected
SARS-CoV-2 IgG Not Detected
…
Discordant results have been obtained for SARS-CoV-2 antibody on two different assays. Serum has been referred to the reference laboratory for additional testing and a further report will follow.
321 The reference laboratory to which the specimen was referred was Pathology West, Westmead, which performed an IFA. It produced a report on 6 October 2020, which provides as follows: [RESsub_CFM.003.001.0001 p 328]
SARS-COV-2 IgA IF <10
SARS-COV-2 IgM IF <10
SARS-COV-2 IgG IF 20
…
These results suggest past infection…
322 Mrs Karpik submits that these results, together with the surrounding circumstances, establish that she contracted COVID-19 prior to the end of the voyage. She says that the negative PCR result can be explained, first, by the fact that a virus sheds over time so that by 28 March there was insufficient presence of the virus for it to be detected, and, secondly, that even if the virus was still present in her system the test result may have been a false negative. She submits that the test results in any event cannot be considered in isolation from the surrounding circumstances, namely that she was caring for, and sharing a small cabin and bed with, her husband during the period in which he was highly symptomatic which means that it is highly likely that she was infected.
323 The respondents rely heavily on the result of Mrs Karpik’s PCR test. They submit that, assuming a symptom onset date of 18 March 2020, it is highly unlikely that Mrs Karpik’s negative PCR test on 28 March 2020 was a false negative. They say that the results of the serological testing must therefore be interpreted in that light as false positives. They also say, as mentioned, that Mrs Karpik’s lay evidence in respect of her experiencing symptoms is implausible. I have already dealt with and rejected that submission in section C.2.2 above.
324 As that brief summary reveals, there is profound disagreement as to what the various test results ultimately mean on the question of whether Mrs Karpik was infected with coronavirus during the voyage. In essence, is the PCR test result a false negative, or are the serology results false positives?
C.2.4 Interpretation of the PCR result
325 On the question of the interpretation of the PCR result, the respondents rely on the evidence of Professor Paterson. Mrs Karpik relies on the evidence of Professor Kesson.
326 The experts agreed that there is no coronavirus test that is both 100% sensitive (ie, correctly designates all infected individuals as positive) and 100% specific (ie, correctly designates all individuals who are not infected as negative). [JNT.001.001.0056 [2]] In that regard, Professor Paterson points out that there is no “gold standard” for coronavirus testing; the sensitivity of PCR testing has been evaluated by performing the test multiple times and assuming that a positive result is a true positive. [EXP_RES.002.001.0001 [8.9]] He referred to numerous studies that concluded that coronavirus PCR tests return false negatives at rates of 2% to 29% with an aggregated false negative rate of 13% (Arevalo-Rodriguez), 9.3% (Kanji et al) [EXP_RES.002.001.0001 [8.10]] and 12% (Pecoraro). [JNT.001.001.0056 [12]-[13]; EXP_RES.002.001.0001 [8.10]] In each of those studies, a false negative was determined by a positive test upon repeat testing.
327 Professor Paterson also explained that the probability of a PCR test returning a false negative increases over time. He explained that the reason for that is that the viral load in the upper respiratory tract declines over time. [JNT.001.001.0056 [14(a)]; EXP_RES.002.001.0001 [8.11]]
328 In respect of Mrs Karpik’s negative PCR test 10 days after first reporting symptoms, Professor Paterson opined in Joint Report 7 that “we could be more than 95% certain that Mrs Karpik’s negative result at 10 days after symptom onset was not a false negative.” [JNT.001.001.0056 [16]] I shall refer to this as the 95% opinion. In cross-examination, Professor Paterson clarified that by “false negative” he means that the PCR test has returned a negative result in circumstances where the subject is actually infected. There is a different possibility which is sometimes also referred to as a false negative, namely that a PCR test returns a negative result notwithstanding that the patient had recently been infected because at the time the test was taken the patient had shed the virus (T575:29-31).
329 Two studies in particular were said to support the 95% opinion. Those studies are, first, Wikramaratna PS, et al, “Estimating the False-Negative Test Probability of SARS-CoV-2 by RT-PCR” (2020) 25(50) Euro Surveillance pii:2000568 and, secondly, Kucirka LM, et al, “Variation in False-Negative Rate of Reverse Transcriptase Polymerase Chain Reaction-Based SARS-CoV-2 Tests by Time Since Exposure” (2020) 173(4) Annals of Internal Medicine 262. [PUB.005.003.0757; PUB.007.010.0001]
330 The 95% opinion expressed by Professor Paterson in Joint Report 7 departs from the opinion he expressed in his initial report. In his initial report, Professor Paterson opined that “had Mrs Karpik truly been infected there was a 75% probability that her PCR test 10 days after symptom onset would have been positive.” [EXP_RES.002.001.0001 [8.11]] I shall refer to this as the 75% opinion, for which Professor Paterson also cited the Wikramaratna study in support.
331 The authors of the Wikramaratna study conducted an analysis of seven antecedent studies with the aim of determining how the probability of obtaining a false negative PCR test is affected by time since symptom onset and swab type. They reported their results as follows: [PUB.005.003.0757 p 4]
Oropharyngeal swabs taken immediately upon symptom onset were predicted to be 5.64% less likely to yield a positive result than a nasopharyngeal swab (logit-scale effect size −1.00 (95% CI: −1.54 to 0.46)). The probability of a positive test decreased with number of days past symptom onset. For a nasopharyngeal swab, the percentage chance of a positive test declined from 96.40% (95% CI: 90.98 to 98.6) on day of symptom onset to 75.47% (95% CI: 66.88 to 82.51) on day 10 since symptom onset (SSO), and only a 3.30% (95% CI: 0.53 to 17.90) chance of a positive result on day 31 SSO. For an oropharyngeal swab, the probabilities were 90.76% (95% CI: 77.84 to 96.52), 53.00% (95% CI: 38.27 to 67.46) and 1.23% (95% CI: 0.18 to 7.86) for day of symptom onset and days 10 and 31 SSO, respectively.
…
As shown above, the probability of a false-negative test result depends on the number of days since symptom onset…
(Emphasis added.)
332 Those results were illustrated in Figure 1 – from which it can be seen that for a nasopharyngeal swab test at 10 days after symptom onset the probability of the test giving a positive result is “0.75”, ie, 75%:
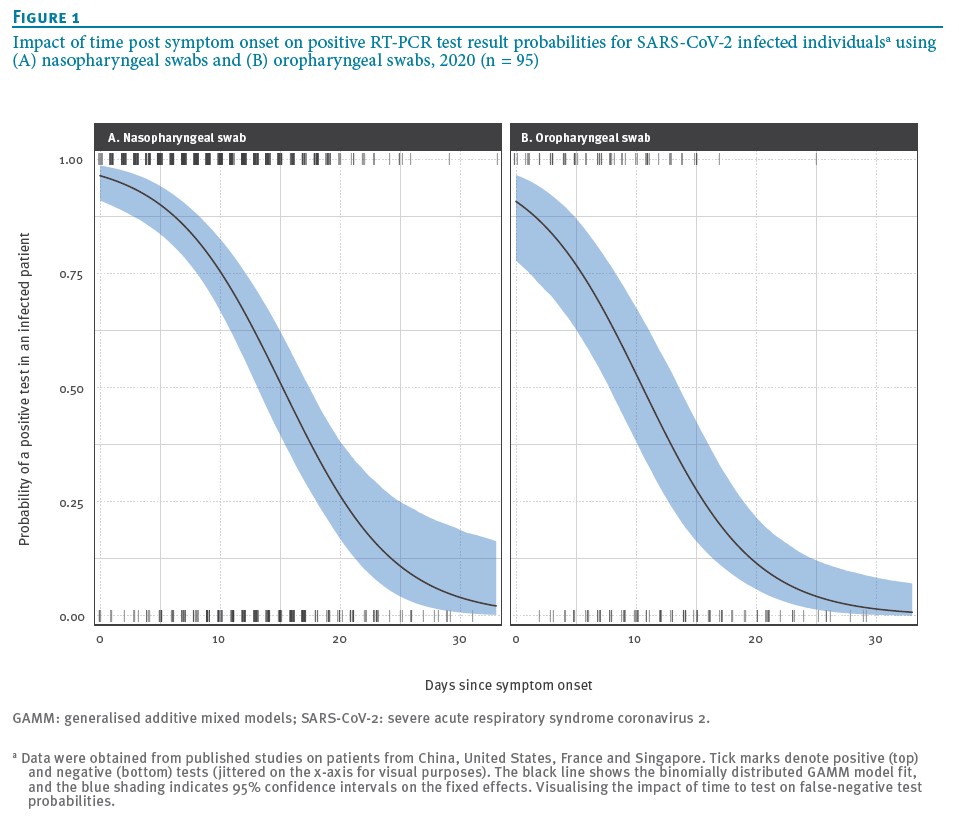
333 In relation to the 95% opinion, Professor Paterson explained that the authors of the Wikramaratna study conducted a further analysis that “showed different results” to the 75% opinion. The further analysis and the different results said by Professor Paterson to derive therefrom were based on data from a study published as Bi Q, et al, “Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzhen, China: a retrospective cohort study” (2020) 20(8) The Lancet Infectious Diseases 911 (T576:40-578.5). From that further analysis, Professor Paterson concluded: [JNT.001.001.0056 [14(c)]]
In this setting of known transmission (analogous to the Ruby Princess), the overall false negative probability for a single test was calculated to be 16.7%. At 10 days after symptom onset Wikramaratna found the false negative rate was less than 5%.
(Emphasis added.)
334 Professor Paterson was cross-examined on the source of the 5% and 16.7% figures. The 5% figure was said to derive from Figure 3 of the Wikramaratna article by identifying the probability on the Y-axis that corresponds with the 10-day mark on the X-axis (T578:26-35). Figure 3 depicts the following graph:
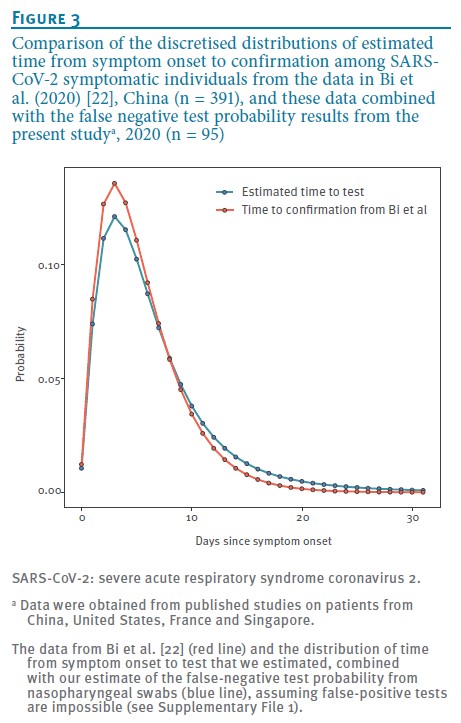
335 The 16.7% figure was said to derive from the following passage in the article (T578:17-24):
Estimating the number of false negatives in a cohort of tested individuals
We estimated the distribution of time from symptom onset to taking a test by coupling an estimate of the time from symptom onset to positive test result with our results on false negative test probabilities. Figure 3 shows the result, which has a heavier tail than the original distribution from Bi et al because the false-negative test probability increases with time. We used this result to calculate the average false negative test probability for a population whose time from symptom onset to test is as shown in Figure 3 and now demonstrate how this result (a false-negative test probability of 16.7%), together with assumptions about the false-positive test probability, may affect testing outcomes in practice.
(Emphasis added; endnotes omitted.)
I shall refer to this passage as the 16.7% passage.
336 Professor Kesson disagrees with Professor Paterson’s 95% opinion for essentially the following reasons: [JNT.001.001.0056 [17]]
(1) A negative PCR test 10-20 days after infection is possible (the 20 days assuming an infection date of 8 March 2020 – ie, on the first day of the RU2007 voyage).
(2) A PCR test does not return a “positive” or “negative” result but instead a “detected” or “not detected” result, where not detected means that the virus genome has not been detected in the sample.
(3) 25% of the population in the 70-79 year-old age group who are infected stop shedding the virus by 18 days after symptom onset and 25% of that group are still shedding the virus more than 37 days after symptom onset.
337 Professor Kesson therefore opined that an alternative explanation consistent with the PCR result and past infection is that Mrs Karpik was no longer shedding the virus by 28 March 2020. In her view, the probability of that being the case is less than 25% but not naught. On the basis of that, as well as the articles referred to by Professor Paterson, she arrived at a rough estimate of there being a 5-20% chance that Mrs Karpik would have had a PCR result of “not detected” on 28 March 2020, assuming she was infected and the onset of her symptoms occurred 10-11 days prior. [JNT.001.001.0056 [18]]
338 Professor Kesson was cross-examined on her evidence in respect of viral shedding (identified at [336(3)] above). She explained that that data was taken from a study published as Phillips SP, et al, “Duration of SARS-CoV-2 shedding: A population-based, Canadian study” (2021) 16(6) PLoS ONE e0252217, which reported a median shedding duration for those aged 70-79 of 28 days, with an interquartile range of 18-37 days. She further explained that her rough estimate was based on the fact that the timing of tests reported in the Phillips study was different to the time that Mrs Karpik had her PCR test (T518:22-519:11). I infer that the reference to the different timing in the Phillips study is a reference to the fact that the authors defined the duration of documented resolution of the virus as the time between an initial positive PCR test and a second of two negative PCR tests.
339 Professor Kesson also explained in cross-examination that viral shedding is an alternative explanation for Mrs Karpik’s not detected result. That is, assuming that Mrs Karpik was infected, her negative result could have been due to a false negative or it could have been because she had sufficiently shed the virus such that it was a true negative (T521:26-37).
340 In respect of other factors that may lead to a false negative result, Professor Kesson points out that inadequate sampling or other sampling errors can also lead to an incorrect “not detected” result. [JNT.001.001.0056 [17(e)]]
341 As mentioned, Professor Paterson relies on the Wikramaratna and Kucirka studies in support of the 95% opinion.
(a) Professor Paterson’s reliance on the Wikramaratna study
342 Dealing first with his reliance on the Wikramaratna study, Professor Paterson’s interpretation of Figure 3 cannot be correct. As mentioned, on Professor Paterson’s interpretation of Figure 3, the chance of a PCR test returning a false negative 10 days after symptom onset is 5%. If that interpretation is correct, it would follow from Figure 3 that the chance of a false negative is at its highest 3 days after symptom onset and it would be less than 1% at 20 days after symptom onset. That is not only highly doubtful as being counter-intuitive, it directly contradicts Professor Paterson’s own evidence and the express findings in the study itself, namely that the rate of false negatives increases as the time from symptom onset increases.
343 Professor Paterson did not explain (and, in fairness, was not asked) how his interpretation of Figure 3 could possibly be reconciled with the authors’ express conclusion and, indeed, Professor Paterson’s own earlier opinion that the percentage chance of a positive test is 75% 10 days after symptom onset. The only topic traversed in cross-examination in respect of the Wikramaratna study was the source of the data (ie, the Bi study) for the further analysis that led to the 16.7% passage.
344 In order to understand how these obviously inconsistent conclusions might (or might not) be reconciled, it is necessary to understand what exactly Figure 3 is depicting and the 16.7% passage is referring to. That necessitates consideration of the article itself.
345 The 16.7% passage is the only paragraph in the Wikramaratna article that refers to Figure 3. It is headed “Estimating the number of false negatives in a cohort of tested individuals” and appears in a part titled “Results” on page 5. On page 3 of the article, there is another section titled “Estimating the number of false negatives in a cohort of tested individuals.” That section appears in a part titled “Methods.” It is apparent (if not clear), therefore, that the 16.7% passage and Figure 3 are the results of the task described in the identically titled section on page 3. That task is described as follows:
Estimating the number of false negatives in a cohort of tested individuals
Results from Bi et al suggest that the probability of an infected individual having a positive RT-PCR test for SARS-CoV-2 after a given number of days since symptom onset follows a gamma distribution with shape 2.12 and rate 0.39 (see both Figure 2 and Table S2 in Bi et al). We used these data with our results on RT-PCR sensitivity and applied Bayes’ Theorem to recover the distribution of the time from symptom onset to RT-PCR test (see Supplementary File 1).
We then integrated this distribution over time from symptom onset to time of test in order to calculate the population average false negative test probability (ie taking account of the fact that the false negative test probability depends on time from symptom onset). We used this estimate alongside a realistic range of false positive test probabilities to illustrate by how much the true number of infections in a cohort of tested individuals can differ from the number of positive tests (see Supplementary File 1 for more details), based on data from the United Kingdom (UK) and South Korea as of 20 March 2020 (UK: 5.1% positive (3,277/64,621); South Korea: 2.7% (8,652/316,664).
(Emphasis added; endnotes omitted.)
346 For clarity, I reproduce the 16.7% passage, which reports the results of the task set out:
Estimating the number of false negatives in a cohort of tested individuals
We estimated the distribution of time from symptom onset to taking a test by coupling an estimate of the time from symptom onset to positive test result with our results on false negative test probabilities. Figure 3 shows the result, which has a heavier tail than the original distribution from Bi et al because the false-negative test probability increases with time. We used this result to calculate the average false negative test probability for a population whose time from symptom onset to test is as shown in Figure 3 and now demonstrate how this result (a false-negative test probability of 16.7%), together with assumptions about the false-positive test probability, may affect testing outcomes in practice.
(Emphasis added; endnotes omitted.)
347 Contrary to Professor Paterson’s interpretation, the bolded passages of those identically-headed sections make it tolerably clear that what Figure 3 is estimating is not the probability of a false negative test plotted against time since symptom onset. Rather, what the authors sought to do was to use their results on PCR test sensitivity (ie, the results on which Professor Paterson based his initial 75% opinion) and the data from the Bi study to “recover” or estimate, using Bayes’ Theorem (ie, a theorem concerning epistemic probability), “the distribution of time from symptom onset to taking a test.” That interpretation of Figure 3 not only accords with what the authors say they were doing and the explanations of what the coloured lines represent in Figure 3 itself, but it also accords with human experience. It is intuitively plausible and highly believable that the probability of a person undertaking a PCR test spikes within the first few days after symptom onset and then decreases thereafter in the manner depicted in Figure 3. It is, on the other hand, highly implausible and not believable that the probability of a PCR test producing a false negative spikes within the first few days after symptom onset and then decreases thereafter in the manner Professor Paterson understood Figure 3 to depict.
348 Although it is not strictly necessary to deal with the 16.7% passage, for the sake of clarity, it is prudent to set out how Figure 3 relates to the 16.7% figure.
349 As is apparent in the italicised passages of those sections of the Wikramaratna article extracted above, the distribution of time from symptom onset to taking a test as depicted in Figure 3 was then used to calculate false negative probability in, as the heading states, a cohort of tested individuals. Much of the work and explanation appears to be set out in Supplementary File 1. That File explains that the conclusion that PCR tests have a false negative probability of 16.7% depends, in part, on the fact that, within a cohort of tested individuals, some will have been tested soon after symptom onset and others will have been tested later. That methodology of arriving at a false negative chance as set out in the File is relevantly different to the studies arriving at different figures and adverted to at [326] above; it is intended to demonstrate differences in testing outcomes in real world applications.
350 For those reasons, the Wikramaratna study provides no support for the 95% opinion; Professor Paterson appears to have simply misunderstood Figure 3.
(b) Professor Paterson’s reliance on the Kucirka study
351 Turning now to Professor Paterson’s reliance on the Kucirka study, that too is misplaced.
352 In Joint Report 7, Professor Paterson states:
Similar findings [ie, to the 95% opinion] were made by Kucirka and colleagues. These authors sought to determine the predictive value of the test according to time since symptom onset. Figure 2 of their paper (below) also shows that the false negative rate at 10 days after symptom onset was less than 5%.
He then reproduced only a part of Figure 2 as follows:
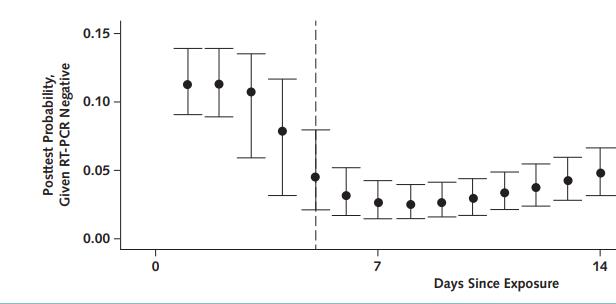
353 The part of Figure 2 reproduced by Professor Paterson does not convey any information about the false negative rate at 10 days after symptom onset. As the extracted image itself makes clear, the X-axis represents days since exposure, which is relevantly different to days since symptom onset. The Y-axis also does not represent the probability of a false negative, but rather what is described as “post-test probability, given RT-PCR negative.”
354 As with the Wikramaratna article, it has been necessary to go the article itself. Figure 2 in its entirety is as follows:
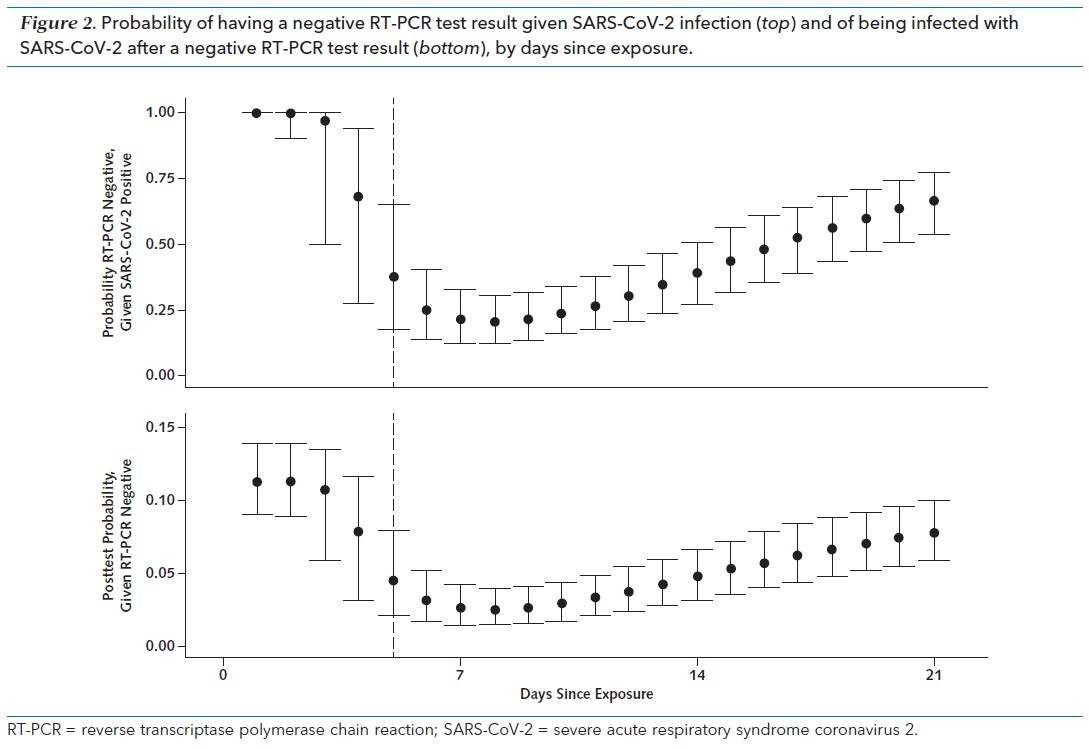
355 It is the data plotted on the top graph that represents the probability of a false negative, albeit given days since exposure rather than days since symptom onset. The bottom graph, which Professor Paterson deployed in support of his 95% opinion, instead provides the post-test probability of being infected with coronavirus given a negative PCR result. As explained on page 3 of the Kucirka article, that post-test probability varies with the pre-test probability of infection – which pre-test probability is explained by the authors as “how likely infection is on the basis of the magnitude of exposure or clinical presentation.” The bottom graph is therefore not the relevant graph from Figure 2.
356 The authors of the Kucirka study reported their results on the probability of a false negative PCR with reference to the top graph in Figure 2 as follows:
Probability of a False-Negative Result Among SARS-CoV-2–Positive Patients, by Days Since Exposure
Over the 4 days of infection before the typical time of symptom onset (day 5), the probability of a false-negative result in an infected person decreases from 100% (95% CI, 100% to 100%) on day 1 to 67% (CI, 27% to 94%) on day 4, although there is considerable uncertainty in these numbers. On the day of symptom onset, the median false-negative rate was 38% (CI, 18% to 65%) (Figure 2, top). This decreased to 20% (CI, 12% to 30%) on day 8 (3 days after symptom onset) then began to increase again, from 21% (CI, 13% to 31%) on day 9 to 66% (CI, 54% to 77%) on day 21.
(Emphasis added.)
357 That passage explains the meaning to be attributed to the dashed vertical line in each of the graphs in Figure 2 at day 5, namely that it is what the authors took to be the typical day of symptom onset. It also explains, importantly, that the lowest probability of a false negative PCR result on an infected person was 20% at 3 days after symptom onset (ie, day 8 post exposure).
358 The bottom graph in Figure 2 is explained in the study as follows:
Post-test Probability of Infection if RT-PCR Result is Negative (1 Minus Negative Predictive Value)
Translating these results into a post-test probability of infection, a negative result on day 3 would reduce our estimate of the relative probability that a case patient was infected by only 3% (CI, 0% to 47%) (for example, from 11.2%, the rate seen in a large study of household contacts, to 10.9%) (Figure 2, bottom). Tests done on the first day of symptom onset are more informative, reducing the inferred probability that a case patient was infected by 60% (CI, 33% to 80%).
359 Because Professor Paterson based his opinion on the likelihood of a false negative PCR test 10 days after symptom onset, the data that is relevant in the Kucirka study to his opinion is the data from the top graph in Figure 2 in the column immediately to the right of 14 (ie, 10 days since symptom onset being 15 days since exposure given the assumed typical time of symptom onset). The data there plotted is between 38% (being the identified probability at day 5, or the day of symptom onset) and the 50% mark on the Y-axis.
360 The results of the Kucirka study are therefore contrary to Professor Paterson’s evidence and do not support the 95% opinion. Indeed, the study supports an opinion more favourable to Mrs Karpik than that which either expert offered, namely probability of a false negative of about 44% (or >40% but <50%).
361 Because the Wikramaratna study and Kucirka study do not support the 95% opinion, and because they are the only two studies said to support it, I reject Professor Paterson’s evidence in that respect. I turn to consider the remaining evidence on this topic.
362 As mentioned, Professor Kesson gave evidence that, assuming Mrs Karpik was infected, her PCR test could have returned a negative result for two reasons: the one is that it was a false negative; the other is that she had shed the virus by the time the swab was taken. In respect of the second of those two possibilities, she gave evidence that 25% of people aged 70-79 would stop shedding the virus by 18 days after symptom onset. However, she was unable to offer any further guidance and, in particular, was unable to offer any guidance as to the probability of individuals aged 70-79 shedding the virus at 10 days after symptom onset.
363 I am prepared to accept Professor Kesson’s evidence to the effect that the probability was non-zero and statistically significant. Acceptance of that fact seems to me nonetheless to be of limited utility.
364 In my view, of far greater utility are the results of the Wikramaratna study itself, it being the only primary source cited by the parties’ experts that sought to determine the probability of a false negative PCR test depending on the number of days since symptom onset. As explained earlier, the Wikramaratna study found that, given a positive infection, the probability of testing positive 10 days after symptom onset is 75.49%. That figure was used by Professor Paterson in his initial report to conclude that “had Mrs Karpik truly been infected there was a 75% probability that her PCR test 10 days after symptom onset would have been positive.” I accept that evidence. I will return to the question of its significance in due course.
C.2.5 Interpretation of the serological results
365 Turning now to Mrs Karpik’s serological results, as mentioned, she provided blood specimens on two dates: 20 April 2020 and 19 September 2020. Only one assay was performed on the first specimen, namely the first IFA; three assays were performed on the second specimen, namely two commercial assays and, subsequently, the second IFA.
366 Dealing first with what is not contentious, the experts were agreed that the results of the commercial assays performed on the second specimen provide no meaningful information on their own. Each of Professor Kesson and Professor Paterson however considered that the results are consistent with their evidence: Professor Kesson on the basis of the patient losing antibodies and Professor Paterson on the basis of no coronavirus antibodies ever having been present. [JNT.001.001.0056 [28]-[29]]
367 That therefore leaves the IFA results in the realm of meaningful information. The experts disagreed about how the IFA results should be interpreted.
(1) The expert evidence
368 Professor Paterson gave evidence that the diagnostic criteria of infectious diseases by serological testing is the existence of a four-fold increase in antibody titre between samples taken in the acute setting (ie, at time of illness) and the convalescent setting (ie, three or more weeks following presentation). He explained that that approach is based on the principle of paired serology. The sample taken during the acute stage acts as a reference point for the immune system’s baseline production of a given antibody. The allowance of three or more weeks before taking the convalescent sample is to allow for the body’s immune system to produce a specific antibody response to the disease. A four-fold increase in titres from the acute sample to the convalescent sample constitutes evidence for disease exposure. [EXP_RES.002.001.0001 [8.24]]
369 Professor Paterson also gave evidence that serological assays are prone to errors arising out of cross-reactivity, which is the common phenomenon of antibodies to bind to antigens other than their cognate microorganism due to the immune system recognising similar molecular patterns or appearance. This leads to false positive results. [EXP_RES.002.001.0001 [8.16], [8.18]] He considers that one potential cause of cross-reactivity in the present case is the presence of rheumatoid factor. [JNT.001.001.0056 [25]]
370 Another issue with serological testing of SARS-CoV-2 identified by Professor Paterson is the presence of SARS-CoV-2 reactive IgG antibodies detected in blood samples taken in 2017 as reported in Anderson EM, et al, “Seasonal human coronavirus antibodies are boosted upon SARS-CoV-2 infection but not associated with protection” [2020] medRxiv 2020.11.16.20227215. [PUB.005.003.0015]
371 I will return to the issues of cross-reactivity with rheumatoid factor and the detection of coronavirus antibodies in blood specimens taken in 2017.
372 As may be apparent, Mrs Karpik’s results fail to meet the diagnostic criteria based on the principle of paired serology described above: no specimen was taken during the acute setting and the specimens that were taken were not drawn at the correct intervals. The experts are all agreed in that respect. Professor Kesson nonetheless maintains that the results show that Mrs Karpik developed a specific antibody response to coronavirus. That view depends, in particular, on: [EXP_SKA.003.003.0001 [29], [58], [62], [63]]
(1) the accuracy of the IFA;
(2) the fact that a vaccine was not available until early 2021 such that the existence of the antibodies could not have been caused by vaccination; and
(3) the loss of IgM from the first IFA to the second IFA and the continued detection of IgG in the second IFA is consistent with previous infection.
373 Professor Kesson therefore concluded that Mrs Karpik was infected with coronavirus prior to 20 April 2020. [EXP_SKA.003.003.0001 [64]]
374 As Professor Kesson placed particular reliance on the accuracy of the IFA, it is convenient to set out the evidence in that respect.
375 Professor Kesson gave evidence that the IFA has a sensitivity of 91.3% and a specificity of 98.9%. She also gave evidence that the IFA’s negative predictive value (ie, the probability that subjects with a negative screening test truly do not have the disease) is 99.6% and, in circumstances where IgG and IgA are detected, its positive predictive value (ie, the probability that subjects with a positive screening test truly have the disease) is 96.8%. [EXP_SKA.003.003.0001 [14]-[20]] That data is taken from a study published as Hueston L, et al, “The Antibody Response to SARS-CoV-2 Infection” (2020) 7(9) Open Forum Infectious Diseases ofaa387. [PUB.005.003.0326] In Table 1 on page 4 of the Hueston study, the specificity values are produced for all combinations of results of the IFA ranging from 98.9% to 99.9%. Professor Kesson explains that the result is that the false positive rate is therefore between 1.1% and 0.1%. [JNT.001.001.0056 [21]]
376 Professor Paterson was firmly of the view that the serological results must be interpreted in the context of Mrs Karpik’s negative PCR result. [JNT.001.001.0056 [11]] On that basis, he opined that Mrs Karpik would have been classified as a “negative reference case” in the Hueston study and that her first IFA would therefore have been recorded as a false positive. [JNT.001.001.0056 [22(d)]] The study defined the “negative reference standard” as follows:
Negative reference cases were defined as persons with suspected COVID-19 who had ≥1 negative SARS-CoV-2 NAT [ie, PCR]. Negative reference cases were classified as having false-positive serology if an IFA titer of ≥10 was detected on initial or follow-up serology; otherwise in these cases an IFA titer of <10 was classified as true negative.
377 Professor Kesson disagreed with Professor Paterson on the basis that the reference cases in that study “would probably all have had a SARS-CoV-2 PCR and initial blood taken for serology testing performed at the same time and close to the patient’s symptom onset.” [JNT.001.001.0056 [23(a)]] As mentioned, Mrs Karpik’s PCR test was undertaken 10 days after first reporting symptoms and the blood sample was taken 23 days after that PCR test.
378 In Joint Report 7, one of the points on which Professor Paterson challenged Professor Kesson’s opinion was that, of the nine individuals in the Hueston study who returned a negative PCR but a positive IFA, five had negative virus neutralisation assays, which assays Professor Kesson stated are considered to be the most specific. On that basis, he reasons that most patients with negative PCR tests but with a positive IFA are negative by the most specific of serological assays. [JNT.001.001.0056 [22(e)]] A virus neutralisation assay was not performed on Mrs Karpik’s specimen.
379 Under cross-examination, Professor Paterson agreed that in the Hueston study, there were in truth 29 individuals who returned a negative PCR but a positive IFA, and that only nine of those 29 had a virus neutralisation assay performed. It was of those nine that only five returned negative neutralisation assays (T579:18-44). It follows that his evidence that most patients with negative PCR tests but positive IFAs are negative by the most specific of serological assays is incorrect; five of 29 is very much less than “most.”
380 Professor Kesson accepted under cross-examination that five false positives out of a sample size of 29, as determined by a negative virus neutralisation assay, is statistically significant (T520:20-23). Nonetheless, she explained that those five negative results could be explained by a neutralisation assay’s higher specificity and lower sensitivity.
381 Professor Kesson also addressed Professor Paterson’s concerns about cross-reactivity. She gave evidence that, although rheumatoid factor is always a possibility, that possibility only exists for a false positive IgM result and only if there is IgG present. She opined that, because Mrs Karpik’s SARS-CoV-2 IgM titre on her first IFA was <10, there was no rheumatoid factor present to give a false positive result. [JNT.001.001.0056 [26]] The Hueston article to which she referred also addresses cross-reactivity. Relevantly, it states that cross-reactivity with SARS-CoV was observed in many samples, all of which had an IgG titre of ≥160. It also reports that no samples from a specificity panel consisting of specimens positive for, inter alia, rheumatoid factor had detectable SARS-CoV-2 antibodies by IFA. [PUB.005.003.0326 p 5]
(2) Discussion
382 The key issue to resolving the reliability of the serological tests is the accuracy of the IFA, since it is the result of that test that calls for interpretation.
383 Dealing first with the issue of the existence of blood specimens taken in 2017 that tested positive for antibodies reactive to coronavirus, I observe that the Anderson article on which Professor Paterson based that evidence is marked as a “preprint” and is specifically stated to not have been peer reviewed. The subsequently published and, I presume, peer reviewed article is not in evidence. In any event, its relevance to the accuracy of the IFA performed on Mrs Karpik’s blood specimens is highly doubtful in circumstances where the study reports that those antibodies were detected from an enzyme-linked immunosorbent assay (ELISA) and not an IFA. There is no evidence concerning the difference between an ELISA and an IFA, although I note that the authors of the Hueston study note that ELISAs need to be subject to robust evaluation. [PUB.005.003.0326 p 7] In circumstances where there is specific evidence concerning the accuracy of the IFA and no evidence concerning the ELISA the subject of the Anderson article, I consider the fact that SARS-CoV-2 antibodies were detected by an ELISA from specimens taken in 2017 to be irrelevant. They may be explained by Professor Paterson’s generalised concerns around the cross-reactivity of serological testing.
384 In relation to the issue of cross-reactivity of the IFA, Professor Paterson’s general concern about the cross-reactivity of assays is not specific to the IFA. In that regard, I prefer the opinion of Professor Kesson. She gave specific evidence as to why there was no rheumatoid factor present in Mrs Karpik’s first blood specimen. In any event, the Hueston article itself provides direct evidence to reject the supposition advanced by Professor Paterson regarding the IFA cross-reacting with rheumatoid factor, namely that no sample specimens positive for rheumatoid factor returned a positive IFA. [PUB.005.003.0326 p 5]
385 As for the balance of Professor Paterson’s generalised evidence concerning the nature of serological testing, I do not consider those remarks to be particularly persuasive and relevant to the determination of how to interpret Mrs Karpik’s IFA results. That is because there is specific evidence concerning the accuracy of the IFA and that specific evidence must outweigh any generalised shortcomings (if such there are) that serological testing might have.
386 Turning now to Professor Paterson’s opinion that Mrs Karpik would have been classified as a negative reference case and, therefore, the IFA regarded as a false positive, that is based purely on the definition provided in the Hueston study itself as extracted at [376] above. Although, ex facie, the application of that definition is correct, it cannot be applied in such a way for at least two reasons.
387 First, as mentioned at the start of the Hueston study, one of the purposes of serology testing is “to make a retrospective diagnosis in individuals who have already recovered from acute illness and are no longer NAT positive.” That is, the IFA is used to diagnose patients with COVID-19 even when they have returned a negative PCR test. It would make the IFA wholly redundant if, in all cases where a subject had truly been COVID-19 positive, those IFAs would be regarded as false positives. Clearly, that is an absurd result. That is nonetheless the result of literally applying the reference definition used in the study to a real world application. The error in the reasoning is that, because the authors of the Hueston study treated (most of) the PCR tests as accurate in order to determine the accuracy of the IFA, that is also true in the present case: ie, because the PCR test was accurate, the IFA must be incorrect. However, to assume the accuracy of the PCR would to be assume in the respondents’ favour one of the essential steps to the conclusion that I am called upon to decide, namely whether Mrs Karpik was infected with COVID-19.
388 The reason why “most of” is parenthesised in the above paragraph leads me to the next point. There is one respect in which the definition in the article is incomplete by reason of an inconsistency within the text. It states that PCR tests were utilised as the reference standard for comparison to serology. [PUB.005.003.0326 p 6] That is, as the respondents submit, the results in the Hueston study are derived from the assumption that the PCR testing conducted on subject individuals produced accurate results. Those who tested negative on a PCR were classified as a negative reference case. If those negative reference cases then had serology results reporting a titre of ≥10, those serology tests would be classified as a false positive.
389 However, in the discussion on page 4 in a section titled “Discordant Results”, the authors state:
Twenty-nine of 2627 NAT-negative patients had SARS-CoV-2-specific antibodies from 1 or more classes detectable by IFA (IgG [n = 22], IgA [n = 4], IgM [n = 9]) (Supplementary Table 2). Two of these were symptomatic household contacts of NAT-confirmed cases, and 2 further cases had a compatible clinical illness with single NAT-negative tests on days 12 and 20 after illness onset, respectively. In these 4 cases, false-negative NATs were strongly suspected. In the remaining 25 cases with false-positive IFA, the median antibody titers were lower (IgG, 40; IgA, 10; IgM, 10) compared with true-positive cases (IgG, 160; IgA, 30; IgM, 40) (Figure 3), and 24 had only 1 positive antibody class.
390 The authors describe this result on page 6 as follows:
False-positive cases were associated with low titers of 1 antibody class only.
391 Thus, of the 29 cases where the subject was PCR negative but IFA positive, only 25 were expressly identified as returning false positive serologies and, of those 25, 24 of them had low titres of one antibody class only (ie, one antibody class ≥10 and the other two <10). The remaining four were instead considered, in light of various other contextual factors, as having false negative PCR results. Those contextual factors included, in two cases, being a household contact and, in the two other cases, having a PCR test undertaken 12 or 20 days after symptom onset in conjunction with having an illness compatible with COVID-19.
392 As extracted above, Mrs Karpik’s first IFA detected two antibody classes. She also relies on the surrounding circumstances in support of her case that she was indeed infected with COVID-19, including that she was a close contact, that she experienced symptoms compatible with COVID-19 and that her PCR test was undertaken 10 days after symptom onset. In those circumstances, it is highly doubtful that she would have been classified as having a false positive serology in the Hueston study.
393 Because, as explained above, it is illogical and absurd to disregard Mrs Karpik’s positive IFA on the basis that she would have been classified as a false-positive case in the Hueston study, it is not necessary to consider Professor Kesson’s observation that in the Hueston study reference cases would probably have had a PCR and serology tests at the same time and close to symptom onset, or the respondents’ criticisms of that observation. I note, however, that the observation is based on what the Public Health Laboratory Network recommended as recorded in the Hueston study (pp 1-2) – the study is based on respiratory tract samples for NAT and serum samples for serological testing referred to the public health laboratory at the NSW Health Pathology-Institute for Clinical Pathology and Medical Research at Westmead. It also stands absolutely to reason that members of the public would present for COVID-19 testing soon after symptom onset.
394 For those reasons, I reject Professor Paterson’s alternative classification of Mrs Karpik’s IFA results and I accept Professor Kesson’s evidence that the IFA has a false positive rate of between 1.1% and 0.1%.
395 As mentioned, in respect of the PCR testing, I accept Professor Paterson’s 75% opinion that had Mrs Karpik truly been infected there was a 75% probability that her PCR test 10 days after symptom onset would have been positive. By itself, that suggests that Mrs Karpik was not infected with COVID-19 although it is not conclusive: it could have failed to detect the presence of the virus or Mrs Karpik could have shed the virus by the time the test was undertaken. It is just another piece of evidence to consider. The IFA results, however, tell a different story. Professor Kesson’s evidence regarding the accuracy of the IFA, which I have accepted, strongly leads to the conclusion that Mrs Karpik was indeed COVID-19 positive.
396 That conclusion is fortified once the surrounding circumstances are taken into account, in particular the likelihood of Mrs Karpik having become infected from her husband given the very close contact she maintained with him for the first 7 or 8 days of his illness.
397 It is therefore my finding that it is more probable than not that Mrs Karpik contracted coronavirus. As mentioned, in that event, the parties accept that she contracted the virus from Mr Karpik. That can only have been on the voyage.
D. THE APPLICATION OF STATE LEGISLATION IN FEDERAL JURISDICTION
398 In order to resist liability on one or other cause of action, the respondents rely on numerous provisions of legislation enacted in NSW. They are:
(1) section 16 of the Civil Liability Act 2002 (NSW) (CLA), which precludes an award of damages for non-economic loss unless the severity of the non-economic loss is at least 15% of the most extreme case;
(2) section 5R of the CLA and s 9(1) of the Law Reform (Miscellaneous Provisions) Act 1965 (NSW) (LRMP Act), which concern the application of contributory negligence to a claim under statute and modify the common law;
(3) section 5H of the CLA, which provides that there is no duty to warn of an obvious risk;
(4) section 5I of the CLA, which provides that there is no liability for the materialisation of an inherent risk; and
(5) section 32(1) of the CLA, which applies a particular test of foreseeability of mental harm which includes the requirement that a person of normal fortitude might, in the circumstances of the case, suffer a recognised psychiatric illness if reasonable care were not taken.
399 The parties do not dispute that each of those provisions apply to Mrs Karpik’s claim in negligence at common law. The parties disagree, however, whether those identified provisions apply to her claim under s 267 of the ACL for failure to comply with the consumer guarantees.
400 Because the provisions of the CLA cannot apply of their own force in an action under the ACL in federal jurisdiction, the question whether those provisions apply falls to be determined by the application of s 275 of the ACL. That provision provides:
275 Limitation of liability etc.
If:
(a) there is a failure to comply with a guarantee that applies to a supply of services under Subdivision B of Division 1 of Part 3‑2; and
(b) the law of a State or a Territory is the proper law of the contract;
that law applies to limit or preclude liability for the failure, and recovery of that liability (if any), in the same way as it applies to limit or preclude liability, and recovery of any liability, for a breach of a term of the contract for the supply of the services.
401 Where paras (a) and (b) are satisfied, a law of the State or Territory of the proper law of the contract that meets the description given in s 275 – ie, that “applies to limit or preclude liability for the failure, and recovery of that liability (if any)” – is picked up and applied as a surrogate federal law. It does so by applying that State or Territory law “in the same way as it applies to limit or preclude liability, and recovery of any liability, for a breach of a term of the contract for the supply of services.” See Insight Vacations Pty Ltd v Young [2011] HCA 16; 243 CLR 149 at [22].
402 Even where a State or Territory law is so picked up, it is necessary nonetheless to determine whether it has any application to the facts of the particular case, including with regard to any geographical limitations in light of the presumption against extraterritoriality at common law and also in, for example, s 12(1)(b) of the Interpretation Act 1987 (NSW).
403 In Scenic CA at [380], Sackville AJA considered that the High Court in Insight Vacations “suggests” that the question whether a law so picked up would in a particular case limit or preclude liability is to be addressed first without reference to any geographical limitation on that law and that, once it has been determined that the law limits or precludes liability, the court must then consider any geographical limitation on the operation of the provision. Although I agree that any limitation in the application of a law so picked up must be addressed, Insight Vacations does not seem to me to require that the questions of whether the law is picked up and what limitations in the law, if picked up, have the effect that that the law does not apply to the particular facts of the case, should be dealt with in any particular order.
404 Insight Vacations decided that CLA s 5N was not picked up by s 74(2A) of the Trade Practices Act 1974 (Cth) (TPA), the predecessor to ACL s 275, as it was not a law that met the description given in that section. It was also held that, even if s 5N was picked up by TPA s 74(2A), it would not have applied to a contract for the supply of recreation services outside New South Wales – the services in question were provided in Europe. If a particular State or Territory law does not, on its proper construction, apply to the facts of the case, then it does not seem to me to be relevant when the question of any limitation in its application is addressed. The reasoning in Insight Vacations does not prescribe the order in which such questions are determined.
405 As might be appreciated, one difficult issue that can arise with respect to whether any State or Territory law so picked up applies in a given case is whether it has any geographical limitation and, if so, what that limitation is. Any such limitation would depend on the proper construction of the State or Territory law in question uninfluenced by the consideration that the ACL, which picks up and applies the State or Territory law, operates extraterritorially under Commonwealth law: Scenic CA at [382]. As this Court only exercises federal jurisdiction, the mechanism by which the CLA applies to the claim in negligence is by operation of ss 79 and/or 80 of the Judiciary Act 1903 (Cth): see Blunden v Commonwealth [2003] HCA 73; 218 CLR 330 at [16]-[18] (Gleeson CJ, Gummow, Hayne and Heydon JJ).
D.2 Non-economic loss: s 16 of the CLA
406 Section 16(1) of the CLA provides that “[n]o damages may be awarded for non-economic loss unless the severity of the non-economic loss is at least 15% of a most extreme case.” It is contained within Div 3 of Pt 2. Section 11A provides for the application of Pt 2 of the CLA, sub-s (3) of which provides that “[a] court cannot award damages, or interest on damages, contrary to this Part” (emphasis added). By s 3 of the CLA, “court includes tribunal, and in relation to a claim for damages means any court or tribunal by or before which the claim falls to be determined.”
407 Mrs Karpik submits that s 16 of the CLA, as picked up by s 275 of the ACL, does not apply to her claim under the ACL. Her argument in support of that proposition proceeds principally upon the basis that CLA s 16, read with s 11A(3), is a NSW law that commands a court as to the exercise of its jurisdiction in a claim for damages. It would therefore be invalid insofar as it purports to apply to any court exercising federal jurisdiction: Rizeq v Western Australia [2017] HCA 23; 262 CLR 1 at [61] (Bell, Gageler, Keane, Nettle and Gordon JJ). It follows, so the argument runs, that the word “court” in CLA s 11A(3) must be a reference to a court or tribunal exercising State jurisdiction in NSW because it is to be construed so as to not exceed the legislative power of the NSW Parliament: s 31 of Interpretation Act 1987 (NSW). That is to say, CLA s 11A(3) is a command to courts exercising State jurisdiction.
408 It might be thought that that contention is foreclosed by the High Court’s decision in Moore v Scenic Tours Pty Ltd [2020] HCA 17; 268 CLR 326 (Scenic HCA) which applied s 16 to an ACL claim, ie, a claim in federal jurisdiction before a State court. Mrs Karpik, however, submits that the question whether CLA s 16 applies to a claim brought in this Court (or any federal court), as opposed to in a State court, was expressly left open by Sackville AJA in Scenic CA at [388] fn 257.
409 There are at least two reasons why that submission must be rejected.
410 First, as the respondents point out, the reasoning in support of the submission is inconsistent with what was said by Sackville AJA in Scenic CA at [388]. After having found that s 16 is a law that meets the description given in s 275 of the ACL, Sackville AJA held that “the relevant matter or thing in and of New South Wales is seen to be the awarding of damages in New South Wales by a court or tribunal.” That is relevantly different to “a New South Wales court or tribunal”; it directs attention to the geographical location of the court and not to the jurisdiction exercised by the court: cf, s 80 of the Judiciary Act.
411 Secondly, the jurisdiction exercised in that case itself was federal jurisdiction. That CLA s 16 was picked up and applied by ACL s 275 as a surrogate federal law was confirmed on appeal in the High Court. Mrs Karpik’s argument that CLA s 16 applies only to courts exercising the judicial power of the State of New South Wales is inconsistent with what was held in the High Court.
412 In order to avoid that inconsistency, Mrs Karpik submits in reply that “court” does not extend to federal courts created by the Commonwealth Parliament. She cites in that respect Solomons v District Court of New South Wales [2002] HCA 47; 211 CLR 119 at [9] where Gleeson CJ, Gaudron, Gummow, Hayne and Callinan JJ referred to the “general rule of construction” that confines State enactments to State proceedings and officers.
413 It is difficult to apprehend just what assistance Mrs Karpik seeks to gain by referring to Solomons. The dispute in that case is far removed from the present case. It concerned a refusal by the District Court of NSW to grant a costs certificate under s 2 of the Costs in Criminal Cases Act 1967 (NSW) (Costs Act) to the applicant following his acquittal by direction of an offence against a Commonwealth law. His summons in the Court of Appeal for orders quashing the decision of the District Court and remitting the application for redetermination was dismissed. After referring to the general rule of construction, a majority of the High Court confirmed that:
The “Court[,] Judge [and] Justices” identified in s 2 of the Costs Act, and the phrase therein “any proceedings relating to any offence”, do not extend to federal courts created by the Parliament under Ch III of the Constitution or to this Court or to judicial officers of the Commonwealth, and the offences in question do not include offences under a law of the Commonwealth.
414 The conclusion that s 2 of the Costs Act did not extend to federal courts created by the Commonwealth Parliament or to the High Court should be understood in the context of the High Court’s earlier decision in Commissioner of Stamp Duties (NSW) v Owens (No 2) [1953] HCA 62; 88 CLR 168, in which it was held that s 79 of the Judiciary Act did not convert the function of granting indemnity certificates imposed on NSW courts by the Suitors Fund Act 1951 (NSW) onto federal courts. That is because such a function formed no part of the subject matter with which s 79 deals.
415 Expanding upon that in Solomons, the High Court held that the District Court was not empowered by s 79 of the Judiciary Act to entertain the application under the Costs Act where the offence in question was an offence against a Commonwealth law. The essential reasoning in support of that conclusion was that the provision of the Costs Act that was contended by the applicant to have been picked up by s 79 was an integral part of a State legislative scheme, which scheme could not be only partly picked up by s 79 as that would have given an altered meaning to that part of the State legislation. Section 79 could also not wholly pick up the State legislative scheme. As explained in the majority judgment, a certificate granted by a court under the Costs Act has no purpose other than to serve as a precondition for the making of an application to an officer of the Executive Government of NSW for payment out of the State’s consolidated revenue fund for costs, and s 79 could not effect a corresponding transmutation on the Costs Act that would have the effect of altering the performance by State government officials of their functions. (See [24]-[27].)
416 Thus, as explained by Branson J (Allsop J agreeing) in Williams v United States of America [2007] FCAFC 109; 161 FCR 220 at [13]:
In each case a legislative intention that the State scheme was intended to be available to defendants charged under State law and to litigants in State courts was readily discerned. It was inherently unlikely that the New South Wales legislature intended State revenues to be available to support litigation conducted in federal courts or persons charged under Commonwealth law.
417 In each of Owens and Solomons, s 79 of the Judiciary Act did not make the relevant scheme applicable because it did not pick up the provisions in question. In the present case, although the application of s 16 is couched by s 11A(3) in terms of limiting the power of a court, it does not, as the enactments in those cases do, purport to confer any power or function upon any court. Further, CLA s 16 is clearly a law that meets the description in ACL s 275 so as to be picked up by it as a surrogate federal law. In those circumstances, Mrs Karpik’s argument must be understood that, as federal law, CLA s 16 applies only to State courts exercising federal jurisdiction. There is no reason in the legislative intention of the State scheme or of the ACL to read in such a limitation to the way in which either CLA s 16 or ACL s 275 is intended to operate. To the contrary, the intention of ACL s 275 is to make laws that meet the given description applicable in federal jurisdiction, no matter whether that jurisdiction is exercised by a federal court or by a State court: see Scenic HCA at [38]. If any restriction is to be read into the application of CLA s 16 by reference to “court” in s 11A(3), the limitation must be geographical. Any jurisdictional lacuna in the application of CLA s 16 to an action under the ACL in this Court is itself filled by s 275 of the ACL.
418 There is nothing in the Attorney-General (Commonwealth) v Huynh [2023] HCA 13; 408 ALR 684, handed down since judgment in the present case was reserved, that affects the above analysis.
419 In the result, CLA s 16 applies to and limits Mrs Karpik’s consumer guarantee claims.
D.3 Contributory negligence: s 5R of the CLA & s 9(1) of the LRMP Act
420 In respect of s 5R of the CLA and s 9(1) of the LRMP Act, Mrs Karpik advances the same argument as that in respect of s 16 of the CLA. For the same reasons, the argument fails. See also Motorcycling Events Group Australia Pty Ltd v Kelly [2013] NSWCA 361; 86 NSWLR 55 at [29]-[30] per Basten JA and [177]-[179] per Gleeson JA, Meagher JA agreeing (at [46]).
D.4 Obvious risks: s 5H of the CLA
421 Section 5H(1) of the CLA provides:
A person (the defendant) does not owe a duty of care to another person (the plaintiff) to warn of an obvious risk to the plaintiff.
422 Mrs Karpik contends that the application of s 5H is limited to those risks that materialise in NSW and, as such, has no application where the materialisation of the risk occurs on the high seas. Although, by reference to Masson v Parsons [2019] HCA 21; 266 CLR 554 at [30], Mrs Karpik submits that s 5H concerns the rights and duties of persons, there appears to be no argument or submission directed to whether s 5H(1) of the CLA is a law that meets the description given in ACL s 275. That is, the parties appeared to presume that ACL s 275 operates to pick up s 5H(1) and thus the only issue in dispute is whether its application is limited geographically.
423 In my view, that assumed position is contrary to what was decided in respect of a similar provision of the CLA in Motorcycling Events. One of the issues in that case was whether s 5M(1) of the CLA was picked up by s 275 of the ACL. That provision provides:
A person (the defendant) does not owe a duty of care to another person who engages in a recreational activity (the plaintiff) to take care in respect of a risk of the activity if the risk was the subject of a risk warning to the plaintiff.
424 The NSW Court of Appeal held that CLA s 5M is not a law that meets the description given in s 74(2A) of the then TPA: at [29]-[30] per Basten JA, [44] per Meagher JA and [95]-[96] per Gleeson JA. That is because s 5M does not purport to limit or preclude liability for breach of a term of a contract implied by the TPA into the contract providing for the exercise of due skill and care. Rather, it purports to deny the existence of a duty.
425 Although, as will be explained, a so-called duty to warn should be understood as commensurate with the standard of care required to discharge a duty to take reasonable care, s 5H operates to deny the existence of a duty or to alter the standard of care required so that a failure to warn does not give rise to a breach of that duty. Section 74(2A) of the TPA only picked up those laws that “limit or preclude liability for the failure [to comply with consumer guarantees], and recovery of that liability (if any).” It therefore presupposed that the failure to comply had been established and therefore only picked up laws that affect liability once breach has been established: Insight Vacations Pty Ltd v Young [2010] NSWCA 137; 268 ALR 570 at [91] per Basten JA and [144]-[146] per Sackville AJA; Motorcycling Events at [29] per Basten JA and [94] per Gleeson JA. Those cases therefore draw a distinction between liability reducing or denying laws and duty denying laws; s 74(2A) of the TPA only picked up the former.
426 I raised this issue with the parties after judgment was reserved and invited them to file further submissions. The applicant adopts the position that, as CLA s 5H purports to exclude the duty of care to warn of an obvious risk altogether, as opposed to merely limiting or precluding liability, ACL s 275 is not engaged.
427 The respondents essentially submit that, because ACL s 60 creates a statutory guarantee rather than implying a contractual warranty like TPA s 74(2A), the “fundamental premise” of the ACL is different to the TPA and “a different analysis applies.” Consequently, authorities on s 74(2A) should be treated with caution as the reasoning cannot be “uncritically transposed” to cases concerning ACL ss 60-61 and 275. The respondents say that CLA s 5H specifies when a defendant will not owe a duty of care and that picking up that provision does not negate the existence of the statutory guarantee in s 60 because that guarantee would continue to exist regardless of what s 5H provides. Thus, the effect of s 5H where it applies is to limit or preclude the defendant’s liability under the statutory guarantee. In support of their position they cite two first instance decisions of the NSW Supreme Court in which it was held that ACL s 275 picks up CLA s 5H, namely Menz v Wagga Wagga Show Society Inc (No 3) [2019] NSWSC 541 and Tapp v Australian Bushmen’s Campdraft & Rodeo Association Ltd [2019] NSWSC 1506 (Tapp NSWSC).
428 The respondents’ submissions miss the point. The point is not that the guarantee would continue to exist, for there is no doubt that a state law could not nullify the effect of a federal law. Rather, similar to how a duty-denying provision would have the effect of there no longer being a breach of a contractual warranty implied by statute, a duty-denying provision would also have the effect of there no longer being any failure to comply with a statutory guarantee. A failure to comply with a statutory guarantee is a precondition to the application of ACL s 275. As with TPA s 74(2A), ACL s 275 presupposes that there has been a failure to comply with a statutory guarantee before any laws are picked up. It therefore only picks up laws that affect liability once a failure to comply with a statutory guarantee has been established. That cannot be established if indeed a duty-denying provision is to be picked up by ACL s 275.
429 In respect of the respondents’ reliance on Menz and Tapp NSWSC, it is true that in Menz (at [102]) Bellew J held that ACL s 275 picks up CLA s 5H and that in Tapp NSWSC (at [189]) Lonergan J expressed the same view in obiter. However, in neither of those cases do their Honours explain how they reasoned to those conclusions and there appears to have been no consideration or argument opposing those positions. In particular, their Honours made no reference to Motorcycling Events. Those cases are therefore of limited assistance in the present circumstances where the issue squarely arises and has been the subject of competing submissions.
430 In my view, the language of ACL s 275 is not apt to pick up CLA s 5H. That conclusion is reinforced when one has regard to the uniform nature of the ACL’s implementation as a Commonwealth law and in each state as a State law, the purpose of which plainly enough is to set normative standards for commercial conduct in Australia. It is inimical to that purpose that the standard of conduct required in one State is different from that required in another, as would be the case if ACL s 275 operated to pick up CLA s 5H.
D.5 Inherent risks: s 5I of the CLA
431 Section 5I of the CLA provides:
5I No liability for materialisation of inherent risk
(1) A person is not liable in negligence for harm suffered by another person as a result of the materialisation of an inherent risk.
(2) An inherent risk is a risk of something occurring that cannot be avoided by the exercise of reasonable care and skill.
(3) This section does not operate to exclude liability in connection with a duty to warn of a risk.
432 Section 5I is contained within Div 4 of Pt 1A of the CLA. Section 5, within Div 1 of Pt 1A, provides that, in Pt 1A, “negligence means failure to exercise reasonable care and skill.” Section 5A(1), also within Div 1 of Pt 1A, provides that Pt 1A applies to “any claim for damages for harm resulting from negligence, regardless of whether the claim is brought in tort, in contract, under statute or otherwise.” Thus the reference in s 5I(1) to liability “in negligence” includes an action alleging want of reasonable care and skill under the ACL.
433 Mrs Karpik submits that, in order for s 5I to apply, the materialisation of the risk must occur in New South Wales. The respondents contend that the limitation to s 5I is derived from “any claim” in s 5A(1), which is limited to “any claim in the courts of New South Wales” or “any claim where the law governing that claim is the law of New South Wales.” Those possible limitations were suggested by the High Court in Insight Vacations at [33], although the Court expressly noted that it was not necessary to decide.
434 For the following reasons, I do not consider that it is necessary to resolve the question as to what geographical limitations apply to CLA s 5I as picked up by ACL s 275.
435 Very little by way of assistance in resolving the two competing positions was proffered by the parties in their submissions. Indeed, it seems to me that there are further possibilities. In particular, in circumstances where the services supplied in the present case began in NSW and where numerous acts and omissions alleged to constitute negligence occurred in NSW, at least one further possibility is the location of the act or omission that resulted in the materialisation of the risk.
436 Further, s 5I is itself fraught with difficulties. Its application and relevance are far from certain. As a matter of construction, the issues with the ambiguity of the provision are identified comprehensively by Leeming JA in Paul v Cooke [2013] NSWCA 311; 85 NSWLR 167 at [60]-[67] and by Basten JA in Sparks v Hobson [2018] NSWCA 29; 361 ALR 115 at [42]-[44]. Basten JA went on to observe in Sparks at [45] that, since liability only arises upon establishing negligence and causation, recourse to s 5I is not required where causation cannot be established (ie, where a failure to exercise reasonable care did not cause the harm) and, conversely, s 5I is not engaged where causation is established.
437 In Capar v SPG Investments Pty Ltd [2020] NSWCA 354 at [172]-[173], Basten JA, McCallum JA and Emmett AJA agreeing (although the latter in dissent as to the result), elaborated on that idea and concluded that in practical terms, s 5I is otiose.
438 Indeed, despite submitting that s 5I would have work to do in the present case, the respondents sought to invoke s 5I by merely repeating their submissions on why factual causation was not established. As observed by Basten JA in Sparks, if those submissions are correct, then recourse to s 5I is not required; if they are wrong, s 5I is not engaged.
D.6 Normal fortitude: s 32(1) of the CLA
439 The respondents submit that CLA s 32(1) and its test of “normal fortitude” applies to Mrs Karpik’s s 60 and s 61 claims. They say that it is picked up by ACL s 275.
440 Mrs Karpik submits that a claim under the ACL s 61 consumer guarantees is not a claim in negligence within the meaning of that term in s 27 of the CLA, ie, it does not have as an element a “failure to exercise reasonable care and skill.” She submits that for that reason, CLA s 32 does not apply to the ACL s 61 claims.
441 I accept Mrs Karpik’s submission on that point. For the reasons already explained in the analysis of ACL s 61, it is not a claim in negligence. Although reasonableness is a qualifier in both s 61(1) and s 61(2), neither of the guarantees provided for in those sections requires the service provider to exercise reasonable care and skill. CLA s 32 does not apply to those claims.
442 With regard to Mrs Karpik’s ACL s 60 claim, she submits that if, as she submits, the CLA is not picked up by ACL s 275, then CLA s 32 does not apply to the ACL s 60 claim. Inherent in that submission is an apparent acceptance that if the CLA is otherwise picked up and applied to the s 60 claim, s 32 would also apply.
443 I do not think that that is right because it is not at all clear that CLA s 32(1) meets the description of being a provision to “limit or preclude liability for the failure” to comply with the guarantee. As with s 5H, further submissions were invited from the parties with respect to the application of ACL s 275 to CLA s 32(1). No distinction was drawn in those submissions between ss 5H and 32(1) of the CLA and I was not directed to any case that held that s 32(1) was picked up by either TPA s 74(2A) or ACL s 275. In those circumstances, for the same reasons as given in relation to CLA s 5H, CLA s 32(1) is not picked up by ACL s 275 – ie, s 32(1) is a provision that applies at the stage of determining the existence of a duty and not at the requisite later stage of limiting or precluding liability for a failure to comply with a consumer guarantee that is already established.
444 Be that as it may, for the reasons given in relation to the respondents’ duty of care owed to Mrs Karpik in relation to her adjustment disorder suffered as a consequence of Mr Karpik’s illness (see section F.3 below), in this case it does not matter whether one applies the “normal fortitude” test or not because the circumstances giving rise to Mrs Karpik’s recognised psychiatric illness satisfy that test in any event.
E. ACL S 61: THE PURPOSE AND RESULT CONSUMER GUARANTEES
445 Section 60 of the ACL, which is dealt with more fully in the context of the negligence claim because of the obvious overlap between the cause of action that it offers and the cause of action in negligence, provides that a supplier of services in trade or commerce guarantees that the services “will be rendered with due care and skill.” I draw attention to that here because the guarantees in s 61 must be construed harmoniously with s 60. The guarantee in s 60 can be referred to as the care guarantee.
446 Section 61 of the ACL provides for two consumer guarantees in respect of services supplied in trade or commerce.
447 The guarantee in s 61(1) is, relevantly, that if the consumer, expressly or by implication, makes known to the supplier any particular purpose for which the services are being acquired by the consumer, there is a guarantee that the services “will be reasonably fit for that purpose.” This can be referred to as the purpose guarantee.
448 The guarantee in s 61(2) is, relevantly, that if the consumer makes known, expressly or by implication, to the supplier the result that the consumer wishes the services to achieve, there is a guarantee that the services “will be of such a nature, and quality, state or condition, that they might reasonably be expected to achieve that result.” This can be referred to as the result guarantee.
449 Section 61(3), which has no equivalent in respect of s 60, provides that the section (ie, the purpose and result guarantees) does not apply if the circumstances show that the consumer did not rely on, or that it was unreasonable for the consumer to rely on, the skill or judgement of the supplier. No issue arises in relation to this provision in this case, although it may have some relevance in the task of construing ss 61(1) and (2).
450 An applicant relying on a failure to comply with the purpose guarantee must establish that the respondent:
(1) supplied services
(2) in trade or commerce
(3) to the applicant as a consumer,
and in addition:
(4) the applicant made known to the supplier a particular purpose for which the services were being acquired by the applicant; and
(5) the services were not reasonably fit for that purpose.
(See Scenic Tours Pty Ltd v Moore [2018] NSWCA 238; 361 ALR 456 (Scenic CA) at [121] per Sackville AJA, Payne JA and Barrett AJA agreeing.)
451 As mentioned, elements (1), (2) and (3) are not in dispute. Also, there is no reliance by the respondents on the defence in s 61(3).
452 An applicant relying on a failure to comply with the result guarantee must establish that the respondent:
(1) supplied services
(2) in trade or commerce
(3) to the applicant as a consumer,
and in addition:
(4) the applicant made known expressly or by implication to the respondent or to the person conducting negotiations or making arrangements in relation to the acquisition of the services, the results the applicant wished to achieve; and
(5) the services were not of such a nature and quality, state or condition that they might reasonably have been expected to achieve that result.
(See Scenic CA at [122].)
453 As with the purpose guarantee, elements (1), (2) and (3) are not in dispute, and the respondents do not rely on the defence in s 61(3).
454 Before turning in more detail to the purpose and result guarantees, it is necessary to dispose of some competing contentions with regard to the application of some New South Wales legislation to the ACL consumer guarantee claims.
E.2 The relevant services, and the terms of service
455 The threshold inquiry relevant to both the purpose guarantee and the result guarantee is to identify the benefits and facilities the supplier was to provide to the consumer, ie, to identify the relevant services. This requires an objective assessment of the dealings between the supplier and the consumer to determine the benefits or facilities the consumer could reasonably expect the supplier to provide in return for the consumer’s payment. That assessment is not confined to the terms of any contract between the supplier and the consumer. Nor is it foreclosed or limited by any contractual limitations on the supplier’s liability for failing to provide the services for which the consumer paid. See Lets Go Adventures Pty Ltd v Barrett [2017] NSWCA 243 at [4] per Basten and Gleeson JJA; Scenic CA at [176].
456 From the Karpiks’ passage contract, including the booking confirmation, the following is relevant to the inquiry: [LAY_SKA.001.001.0273 p 18; MSC.020.147.0001]
(1) The booking was for a 13-day cruise on the Ruby Princess voyage RU2007, departing Sydney on 8 March 2020 and returning to Sydney on 21 March 2020.
(2) The Karpiks would be assigned stateroom B301, which would have a balcony and be wheelchair accessible.
(3) The itinerary for the cruise was as set out in the booking confirmation, including scenic cruising in the Fiordland National Park and calls at Port Chalmers (Dunedin), Akaroa, Wellington, Napier, Tauranga, Auckland and the Bay of Islands in that order.
(4) The cruise fare included on-board accommodation, main meals, entertainment, some activities on board, and gym and some fitness classes. Additional charges would apply to some entertainment and activities, and main meals at onboard speciality restaurants. Optional extras included drink purchases, some onboard activities, short tours, shopping, wifi internet, laundry services, day spa services, fitness classes and additional dining options. (Clause 5.)
(5) The ship would have a medical centre staffed by qualified, licensed doctors and nurses, who, in addition to routine clinical hours, would be available 24 hours a day in the event of an emergency. The medical centre would be well equipped to handle most medical conditions and would be accredited to international healthcare quality standards. (Clause 28.)
(6) The medical centre would not be equipped to the same standards of a land-based hospital, nor designed for the provision of extensive or continuing treatment (cl 27).
457 As an aside, this is a convenient place to identify other terms and conditions which are not relevant to identifying the services but which are relevant to other issues that I will come to:
(1) The CCA would apply, and the terms and conditions do not alter any protection given to the Karpiks by the Act (cl 2).
(2) Carnival would use reasonable endeavours to provide a cruise in accordance with its published schedules and itineraries, but it did not guarantee itineraries, and itineraries did not form part of the contract (cl 3).
(3) The booking was subject to cancellation fees which in the period from 14 days before the departure date amounted to 100% of the total charges for the booking (cl 14).
(4) Carnival could refuse or cancel a booking if a guest had a health condition that Carnival decided might seriously affect the enjoyment, health or safety of the guest or any other person on-board (cl 27).
(5) If Carnival became aware of any matter that reasonably caused it to believe that the presence of a guest on board presented a risk to their own health or safety or to the health or safety of other guests and crew, it, or the Captain, could deny the passenger boarding and could refuse or cancel any bookings from the passenger. If a guest seriously affected the safety, well-being or enjoyment of themselves or any other person on-board, the Captain had the right to confine, sedate or disembark the guest. (Clause 32.)
(6) Carnival would do everything it reasonably could to make sure everything went according to plan; however, sometimes changes can happen that may affect the holiday experience. This could include weather, mechanical difficulties, civil unrest “or any other unforeseen circumstances.” Carnival could change the itinerary or the ship, or cancel the cruise due to operational or commercial requirements. If it was forced to cancel the cruise for any reason prior to departure, it would provide a refund. (Clause 31.)
(7) The contract was governed by the laws in force in New South Wales (cl 38).
458 Returning to the identification of the services, the respondents’ brochures for the cruise give a further indication of the nature of the services which passengers could expect. They include statements to the following effect:
(1) Take a cruise and “come back new.” [LAY_SKA.003.001.0047 pp 2-3]
(2) From learning about intriguing cultures through local experts to enjoying onboard festivities that originate from every corner of the globe, passengers will gain a richer appreciation for the places they visit. [LAY_SKA.003.001.0047 p 4]
(3) There would be the ability to experience the “unique taste sensations” of the cuisine of the places visited, and there would be destination experts and local entertainment. [LAY_SKA.003.001.0047 p 4]
(4) There would be the opportunity to participate in shore excursions to experience the destinations of the cruise. [LAY_SKA.003.001.0047 p 5]
(5) There would be “expertly crafted culinary masterpieces” by innovative and award-winning chefs to be enjoyed on board, and there would be a selection of restaurants for “discerning appetites”, and there would be “speciality dining” and “balcony dining.” [LAY_SKA.003.001.0047 pp 6-7]
(6) There would be a “wealth of activities” on board the ship, including movies, casino, sporting options, live music and other live performances and shopping. [LAY_SKA.003.001.0047 p 8]
459 The respondents accept that the pre-cruise communications by them to the passengers are also relevant for the purpose of discerning the nature of the services that passengers could expect. Those communications relevantly:
(1) Stated that passengers entrusted the respondents’ with their safety, ie, the respondents accepted that the safety of passengers was entrusted to them (the Cruise Personalizer message);
(2) Gave the assurance that the respondents were monitoring the coronavirus situation and that their medical experts were working with the global health authorities, and that requirements to safeguard guests and crew might change as the situation changed (the Emergency Notification); and
(3) Advised that the respondents were continuing to implement increased monitoring, screening and sanitation protocols to protect the health of their guests and gave notice of the option of cancellation with a full refund of all tours departing from 9 March 2020 and thereafter (the Dear Henry email).
460 The services that passengers could expect therefore included services necessary to safeguard and protect passengers’ health including from coronavirus, updated relevant information about the changing situation (ie, risk) with regard to coronavirus and the offer of cancellation and a full refund if considered advisable.
461 There is a minor difference between the parties in the description of the services in this case. The applicant describes the services as comprising everything necessary to provide a 13-day recreational cruise including accommodation, meals, transportation and amenities, onboard activities, cleaning services, medical services as well as services to ensure the health and safety of passengers, and the provision of information before embarkation, during the voyage and during disembarkation about circumstances that may affect those services. The respondents describe the services as those that were reasonably necessary to enable the passengers to have a safe and enjoyable cruise.
462 The trouble with the respondents’ description is that it lacks specificity. It does not even incorporate, for example, the itinerary that the Karpiks were offered and which they paid for – compare the description of the services in Scenic CA at [190]. The services reasonably necessary to enable passengers to have a safe and enjoyable cruise are, in my judgement, essentially the services described in more detail in the applicant’s description which are consistent with the services that were to be provided with reference to the passage contract, the brochures and the pre-cruise communications. The exception is in relation to what the applicant describes as “services to ensure the health and safety of passengers.” It is more accurate to say that the services would be provided in such a way as to safeguard or protect the health and safety of the passengers. I am avoiding the use of the word “ensure” because there was no absolute obligation in that regard and because “safeguard” and “protect” are the words used by the respondents in their Emergency Notification and Dear Henry email.
463 To recap, the services to be provided by the respondents to Mrs Karpik were the benefits and facilities of the 13-day cruise identified in the Karpiks’ booking confirmation and described in the respondents’ brochures, and consistent with the respondents’ pre-cruise communications. That is to say, everything necessary to provide a 13-day recreational cruise including accommodation, meals, transportation and amenities, onboard activities, cleaning services, medical services and the provision of relevant information before embarkation, during the voyage and during disembarkation about circumstances that may affect those services including with regard to the risk posed by coronavirus. The services included those necessary to safeguard and protect the health and safety of the passengers.
E.3 The particular purpose and the result wished to be achieved
464 The applicant pleads that she and the other passengers made it known to the respondents that the particular purpose for which they acquired the services was to have “a safe, relaxing and pleasurable 13-day cruise holiday and to ‘come back new’ from that holiday.” The respondents plead that the passenger group members, which include the applicant, impliedly made it known that they were desirous of having “a safe, relaxing and pleasurable cruise holiday.”
465 Similarly as in relation to the result guarantee, the applicant pleads that she and the other passengers made it known to the respondents that the desired result of the cruise services was to have “a safe, relaxing and pleasurable 13-day cruise holiday, and to come back new from that holiday.” The respondents plead that by going on the cruise, the passengers impliedly made it known that they were desirous of having “a safe, relaxing and pleasurable cruise holiday.”
466 I do not consider that the passengers, including Mrs Karpik, had an identifiable purpose, or result that they wished to achieve, to “come back new.” That is a phrase taken from the respondents’ marketing material. By booking and going on the cruise, the passengers in effect accepted that statement of promise or ambition as illustrated and amplified in the glossy brochures and thereby made known their purpose and the result that they wished to achieve, which is the usual and ordinary purpose or result associated with taking a cruise holiday, namely to have a safe, relaxing and pleasurable cruise. The expectation to “come back new”, whatever that really means, does not add to that purpose or result.
467 I am also not satisfied that the purpose or desired result was specifically to have a 13-day cruise holiday. Certainly the purpose of acquiring the services that was made known was to have a cruise holiday, and there was an expectation that that would be in accordance with the advertised itinerary. That is also the result that was sought. It might be said that part of the purpose and desired result in making the booking was to have a cruise holiday substantially in accordance with the advertised and planned itinerary, but if it had been a day or two shorter, a port or two had been omitted or the rotation of ports had changed, I am not sure that it could be said that the “purpose” or the desired “result” of the booking was not fulfilled or was defeated.
468 It seems to me that the purpose and result guarantees necessarily offer something more than what the contract offers on its terms. That is to say, it does not particularly assist to identify the purpose of acquiring services to be the provision of the contracted for services – that is circular and adds nothing to what the law of contract in any event offers. The same can be said for the result – it is circular and unhelpful to say that the result intended to be achieved by acquiring particular services is that the services are provided. It is necessary to ask, why were the services acquired? – ie, what was their intended purpose and what result was wished to be achieved?
469 In the circumstances, in so far as identifying a relevant purpose that was made known to the respondents is concerned, I consider that Mrs Karpik by making the booking and going through with it, including by turning up to embark on the vessel, made known to the respondents that her particular purpose in acquiring the cruising services was to have a safe, relaxing and pleasurable cruise holiday substantially in accordance with the advertised and booked itinerary. Exactly the same can be said for the desired result that was impliedly made known by Mrs Karpik to the respondents.
470 Something should be said about safety in particular. There are two aspects to a passenger’s implied purpose in booking a cruise holiday that they have a “safe” cruise, or that they wish for a “safe” result – what can conveniently be referred to as navigational and operational safety and health safety. It is the latter that is relevant to this case. The fact that the services to be provided included certain health services, at least in respect of health conditions materialising on the cruise, and that the services included those necessary to protect the passengers’ health, shows that health safety is tied up in the services and is not some extraneous matter. Further, a ship has certain characteristics that make it inevitable that passengers must look to those who operate the ship to be responsible for protecting and maintaining their health. Passengers and crew are to a significant extent captive on the ship, and their daily needs including those concerning their health and the possible transmission of disease – such as food preparation, cleaning, sanitation and waste disposal – are not within their control. In putting their health safety, like their navigational and operational safety, in the hands of the cruise line – as the cruise line acknowledges in its pre-cruise communications – they impliedly make known that part of their purpose in acquiring the services, and part of the result that they wish to achieve, is that the cruise be safe. I will return to this aspect when discussing the duty of care in relation to the negligence claim, but it has some limited application here too.
471 The respondents submit that that usual and ordinary purpose is not a “particular” purpose as required by s 61(1). They submit that it is necessary for a “particular” purpose, rather than the general or usual and ordinary purpose for which the services in question are supplied, to be made known to the supplier in order for the care guarantee to have any work to do beyond what would otherwise be covered by the purpose guarantee. They also submit that there is no good reason to construe s 61(2) in a manner that would allow the desired result to be any less particular or communicated with any less precision.
472 However, in Scenic CA (at [209]-[226]), with reference to authorities dealing with sale of goods legislation with analogous guarantees, the primary judge’s identified particular purpose was upheld. It was expressed in a general way (quoted at [210]) as follows, namely that in making the booking:
… Mr Moore was impliedly making known to Scenic that he and his wife wanted to enjoy the cruise upon which they had booked with all of the benefits which Scenic said that it would provide and that was the particular purpose for which the services were being supplied by Scenic.
(Emphasis added.)
473 That part of the purpose was to “enjoy” the cruise was also recognised at [212] and [238]. I will return to this. Also, the desired result was dealt with in the same way (at [280]-[283]), so what I say below with regard to particular purpose applies equally to the desired result.
474 Statements in the authorities to the following effect were relied on and impliedly adopted in the context of s 61(1) by the Court of Appeal in Scenic CA:
(1) “a particular purpose is ‘a definite purpose, expressly or impliedly communicated to the seller, for which the buyer buys the goods’… it is not necessarily distinct from a general purpose” – at [221] quoting Starke J in David Jones Ltd v Willis [1934] HCA 47; 52 CLR 110 at 121;
(2) “it is settled that the purpose for which goods are supplied may be ‘particular’ within the meaning of this provision, although it is the sole use for which goods of that kind are adapted. The purpose need not be some special use or requirement” – at [221] quoting McTiernan J in David Jones at 128;
(3) the “particular purpose” for which goods are acquired might be the only purpose for which someone might want to acquire them, at [225] citing Lord Wright in Grant v Australian Knitting Mills Ltd [1935] UKPCHCA 1; 54 CLR 49 at 60.
475 Specifically, the Court of Appeal in Scenic CA held (at [226]) that it is not necessary to show a more specific purpose than the only purpose for which such services are generally acquired. It was also held that the purpose was to “enjoy” the services as promised.
476 I acknowledge that the respondents advance arguments before me with regard to the need for a specific purpose to be conveyed that is different from the general or usual purpose for which the services in question are supplied that are different from the arguments advanced on behalf of the service provider in Scenic CA. Nevertheless, as I am not convinced that Scenic CA is plainly wrong, I must not depart from the interpretation of s 61(1) by the NSW Court of Appeal as to the nature of the “particular” purpose that is required to be made known to the supplier: Farah Constructions Pty Ltd v Say-Dee Pty Ltd [2007] HCA 22; 230 CLR 89 at [135] per Gleeson CJ, Gummow, Callinan, Heydon and Crennan JJ.
477 The respondents also submit that there is no authority for the proposition that by booking or going on a holiday, a statutory guarantee or a contractual term arises by implication that the consumer will have a “safe, relaxing and pleasurable holiday.” They seek to distinguish Scenic CA on the basis that Mr Moore’s purpose identified there included specifics of the cruise, ie, “to enjoy an all-inclusive five-star luxury river cruise experience with the additional services promised by Scenic.” However, a purpose in acquiring services being to “enjoy” the identified experience is much the same as the purpose of having a safe, relaxing and pleasurable experience; an unsafe experience, or one that is neither relaxing nor pleasurable, would not be enjoyable. Scenic CA therefore supports the applicant’s submission that the Karpiks impliedly made known that their purpose in booking the cruise was to have a safe, relaxing and pleasurable cruise. That is also the result that they wished to achieve and which they impliedly made known to the respondents.
478 The respondents also rely on Baltic Shipping Co v Dillon [1993] HCA 4; 176 CLR 344. They make the point that damages were awarded there for distress and disappointment for negligent navigation in breach of an implied term of the passage contract to provide the navigational services with due care and skill, and not for breach of any term to provide an enjoyable holiday. That, however, is the wrong point to draw from the case in the present context which is not about contractual terms but the purpose for which the contract is concluded. There it was recognised (by Mason CJ at 363 and 365) that where the object of a contract, such as the contract for cruise services in that case, is to provide enjoyment or relaxation then damages for distress and disappointment are claimable. It was held (at 366) that the object of the “pleasure cruise” contract must be characterised as being “to provide for enjoyment and relaxation.” There was nothing express about that object, or purpose. It arose by implication from the nature of the contracted services. Exactly the same is true of the present case.
479 Other “holiday” cases referred to by the respondents also recognise that the implicit purpose or object of booking a holiday is enjoyment, relaxation and pleasure: Athens-Macdonald Travel Service Pty Ltd v Kazis [1970] SASR 264; Jarvis v Swans Tours Ltd [1973] QB 233 at 238 per Denning MR, 239-240 per Edmund Davies LJ and 241 per Stephenson LJ; Jackson v Horizon Holidays Ltd [1975] 1 WLR 1468 at 1473 per Denning MR, Orr LJ agreeing, and 1474 per James LJ; and Steiner v Magic Carpet Tours Pty Ltd [1984] FCA 323 at pp 33-34; ATPR ¶40-490 at 45,642 per Wilcox J.
480 The respondents submit that it should not be accepted that the passengers’ obvious desire to have a pleasurable cruise amounts to the communication of that as a particular purpose because both passenger and cruise line may be reasonably expected to have known that there are innumerable circumstances where the cruise line could not guarantee that purpose. They submit that at most there was a communicated expectation that the cruise line would exercise due care and skill to achieve that purpose. I reject that because, as I will move on to now, the purpose guarantee is not an absolute guarantee; the services are guaranteed to be reasonably fit for the purpose and to be of such a nature and quality as might reasonably be expected to achieve the desired result; the purpose and the result are not what is guaranteed.
E.4 Reasonably fit for purpose
481 There are a number of cases in different statutory contexts which assist in giving the right meaning to the requirement that the services be “reasonably fit for purpose.”
482 In E v Australian Red Cross Society [1991] FCA 20; 27 FCR 310, the applicant had been infused with blood plasma that was infected with the human immunodeficiency virus (HIV) as a consequence of which it was anticipated that he would soon develop the acquired immune deficiency syndrome (AIDS). One of the causes of action asserted against the hospital that had provided health care and nursing services, including the transfusion, to the applicant relied on s 74(1) of the TPA which relevantly provided that in a contract for the supply of services there is an implied warranty that any materials supplied in connection with those services will be “reasonably fit for the purpose for which they are supplied.” The question was whether the blood plasma was reasonably fit for the purpose for which it was supplied.
483 Although the claim on that cause of action ultimately failed because the then applicable definition of “services” in s 74(3) did not include services of the type in question (at 356), Wilcox J nevertheless dealt with the meaning of “reasonably fit” for purpose. It was submitted on behalf of the hospital (at 355) that the blood plasma supplied to the applicant was “reasonably fit for the purpose for which [it was] supplied” because the purpose was to achieve coagulation to stop the applicant’s life-threatening bleed. It was submitted that it succeeded in achieving coagulation as the bleeding stopped. It was also submitted that the quality of fresh frozen plasma cannot be guaranteed and that the word “reasonably” imports a balancing process, setting the immediate benefits of the material against a possible adverse long-term effect.
484 His Honour rejected those submissions, observing (at 356) that most people would be surprised at the suggestion that HIV infected blood was “reasonably fit” to use as a coagulant. His Honour drew on Henry Kendall & Sons v William Lillico & Sons Ltd [1969] 2 AC 31 (the Hardwick Game Farm case), a case dealing with the expression “reasonably fit” for purpose with regard to the sale of goods governed by the Sale of Goods Act 1893 (UK). Meal sold for feeding poultry contained traces of a substance that was toxic to poultry. The House of Lords held that the meal was not “reasonably fit” for use as poultry food. Justice Wilcox observed that it does not seem to have occurred to anyone that the meal should be regarded as “reasonably fit” to be supplied to poultry since it was suitable for the immediate purpose of providing nourishment, although it would ultimately kill them.
485 In Gharibian v Propix Pty Ltd (t/as Jamberoo Recreation Park) [2007] NSWCA 151; (2007) ATPR ¶42-171, the appellant had suffered an injury while tobogganing at the respondent’s recreational park when the toboggan came off the tracks after rain suddenly started to fall. That was because the toboggan brakes did not work when the tracks were wet because in those conditions the toboggan would aquaplane. The respondent was not liable in negligence but was liable under s 74(1) of the TPA for failing to supply materials (in connection with the supply of services) that were reasonably fit for the purpose for which they were supplied.
486 It was held (at [47] per Ipp JA, Mason P and Tobias JA agreeing), that the services in question were the recreational services provided by the respondent at its recreational park, and that the materials supplied in connection with those services included the toboggan run, as a whole, and the toboggan that the appellant rode. It was held (at [49]) that the purpose for which those materials were supplied was to enable the respondent’s customers, including the appellant, to undertake the toboggan run safely. To be reasonably fit for the purpose for which they were supplied, the structure of the run and the toboggans had to be “reasonably safe” when operated by a customer (at [56]).
487 The respondent had put in place several measures to prevent the run being used when there was rain, and to warn customers to immediately stop their toboggan and get off in the event that rain unexpectedly commenced. Those measures were sufficient to avoid a finding of negligence (a point on which Tobias JA dissented), or that the services had not been provided with due care and skill, but it was held (at [54]) that that said nothing about the fitness of the structure of the run and the toboggans for the purpose for which they were supplied; they were, indeed, measures taken in an attempt to protect users because the toboggans were not fit for their purpose when rain caused the tracks to become wet.
488 Adopting Lord Steyn in Slater v Finning Ltd [1997] AC 473 at 486, it was held (at [62]) that while the implied warranty that the goods are reasonably fit is “inherently a relative concept, it is well-established that the liability … is strict in the sense that the [supplier’s] liability does not depend on whether [it] exercised reasonable care.”
489 With regard to s 74D of the TPA which required goods to be of merchantable quality, which was defined as being “as fit for the purpose or purposes for which goods of that kind are commonly bought as it is reasonable to expect”, in Medtel Pty Ltd v Courtney [2003] FCAFC 151; 130 FCR 182 at [70], Branson J (Jacobson J agreeing) held that the assessment must be undertaken in the light of information concerning the goods available at the time of trial. That has been followed by N Adams J in Prestige Auto Traders Australia Pty Ltd v Bonnefin [2017] NSWSC 149 at [132]-[134], Katzmann J in Gill v Ethicon Sàrl (No 5) [2019] FCA 1905 at [3540], Wheelahan J in ACCC v Jayco Corp Pty Ltd [2020] FCA 1672 at [27] and O’Callaghan J in ACCC v Mazda Australia Pty Ltd [2021] FCA 1493; 158 ACSR 31 at [101]. Nothing said by Lee J in Williams v Toyota Motor Corporation [2022] FCA 344 at [164]-[171] is to the contrary.
490 In Moore v Scenic Tours Pty Ltd (No 2) [2017] NSWSC 733 (Scenic No 2) at [395], Garling J reasoned that the use in the ACL of the qualification “reasonably” when considering fitness for purpose shows that not every small lapse or shortfall in the provision of services will result in a breach of the purpose guarantee. A supply of services will not be in breach of such a guarantee unless the services are not reasonably fit for the identified purpose. The use of the term “reasonably” also introduces an objectively referable measure. It is a qualitative rather than a quantitative one. It requires an overall evaluation of the services provided, and a determination of their fitness for purpose, qualified by the word reasonable.
491 No disagreement with that was expressed in Scenic CA, where it was accepted (at [233]) that a contravention of the purpose guarantee is not established merely by proving that the service failed to supply one component or even several components of a large suite of services the passenger expected to receive, provided the failure relates to services that are not central to the fulfilment of the particular purpose made known to the service provider.
492 The objective qualification to the services means that services may still be reasonably fit for purpose if the loss suffered is attributable to an abnormal susceptibility or idiosyncrasy on the part of the plaintiff. For example, in Griffiths v Peter Conway Ltd [1939] 1 All ER 685 the plaintiff brought an action in respect of dermatitis which had developed after she had begun to wear a Harris Tweed coat which she had purchased from the defendant retailer. The action was dismissed because the irritant was not likely to affect a normal person. By way of comparison, the claim in Australian Knitting Mills for dermatitis suffered as a result of underwear containing excess sulphites, a hidden and latent defect, was successful.
493 I accept the applicant’s submission that s 61 reflects a legislative choice to allocate the risk to suppliers of services not being reasonably fit for purpose when suppliers enter into contracts with consumers and consumers make known the purpose for which the services are being acquired. Save that “reasonably fit” does not mean “absolutely fit” and thus a small departure may be permitted, the guarantee is that the services will be fit to achieve the desired purpose.
494 Illustrations of the kind of minor variations from the promised services which would not amount to them not being reasonably fit for service, and of the role of events outside the control of the service provider, are given in Scenic CA at [235]-[236]. The concept of reasonableness may allow matters such as the service provider’s inability to control weather, water levels and unexpected transport restrictions (being factual matters relevant in that case) to be taken into account. Thus, a holiday in the sun may be reasonably fit for purpose notwithstanding that it rains incessantly, unless, perhaps, the service provider knew that the holiday was scheduled for the monsoon season. Similarly, a cruise is not necessarily rendered unfit for purpose simply because the local authorities require the vessel to dock at a secondary port on one or two days of a 10-day cruise or because one or two of the land tours cannot take place as scheduled. In each case, an assessment has to be made of the services actually provided, making due allowance for the inevitable vicissitudes that can affect even the most meticulous travel and touring arrangements.
495 It was also said in Scenic CA (at [184]) that it may be that the requirement of “reasonably” as a control mechanism built into the purpose and result guarantees does not protect a supplier of services from all the consequences of circumstances beyond its control. That is because Parliament has chosen to allocate to the supplier risks that neither the supplier nor the consumer could have anticipated. Whether or not that is an appropriate policy choice is not for a court to determine.
496 The respondents advance submissions that it would be absurd and cannot have been intended by Parliament to apply to every provision of services a guarantee that they be safe, and that it would transform every service provider into an insurer. But those submissions miss the point. It is not safety that is guaranteed. What is guaranteed is that the services will be reasonably fit to meet the safety purpose. That is quite different.
497 To summarise from the above analysis:
(1) Services will not be reasonably fit for purpose if they achieve some narrow and immediate purpose but otherwise have a catastrophic result which defeats that purpose: E v Australian Red Cross Society and the Hardwick Game Farm case.
(2) Services may not be reasonably fit for purpose even though the service provider acted with due skill and care: Jamberoo.
(3) The assessment of whether services were reasonably fit for purpose must be undertaken in light of all the relevant information available at the time of trial: Medtel and Gill v Ethicon.
(4) That assessment requires an overall evaluation of the services provided, and a determination of their fitness for purpose, qualified by the word reasonable: Scenic No 2.
(5) The objective qualification to the services means that services may still be reasonably fit for purpose if the failure of the purpose is attributable to an abnormal susceptibility or idiosyncrasy on the part of the plaintiff, or something otherwise peculiar to the plaintiff: Griffiths v Peter Conway.
(6) In each case, an assessment has to be made of the services actually provided, making due allowance for the inevitable vicissitudes that can affect even the most meticulous service arrangements: Scenic CA.
(7) It may be that services are not reasonably fit for purpose even though the failure of the purpose arose from circumstances beyond the control of the service provider and that neither it nor the consumer could have anticipated: Scenic CA.
E.5 The nature, and quality, state or condition
498 There is little to be said in abstract about the “nature, and quality, state or condition” that is required of the services such that they might be reasonably expected to achieve the desired result. If services are “reasonably fit for purpose”, then it would seem that they are likely to be of the requisite nature or quality, and if they are not reasonably fit for purpose then they are likely not to be of the requisite nature or quality. It is in the specific facts of the case that one can consider these matters in a meaningful way. In the present case, what I have said about the purpose guarantee in the previous section applies equally to the result guarantee.
499 Mrs Karpik did not have a safe, relaxing or pleasurable cruise. As I have found, her husband and travelling companion, Mr Karpik, contracted COVID-19 which negatively affected Mrs Karpik’s enjoyment of the cruise because she worried about him, she had to care for him, his ability to participate in excursions and other activities with her was restricted, and she contracted COVID-19 from him. For those reasons, the purpose that Mrs Karpik made known for acquiring the cruise services was not realised – she did not have a safe, relaxing and pleasurable cruise holiday. But, was that because the services were not reasonably fit for that purpose, or because the services were not of such a nature or quality that they might reasonably be expected to achieve that result?
500 That is not a straightforward question, but I have ultimately concluded that the answer is “yes.” These are my reasons.
501 To start with the context at the time of the cruise’s departure, by 8 March 2020 the SARS-CoV-2 virus had spread globally. There were over 100,000 laboratory confirmed cases of COVID-19 worldwide, of which nearly 25,000 were outside China in more than 100 countries. Australia had 74 confirmed cases of COVID-19, three deaths and confirmed local transmission. There were 696 cases on the Diamond Princess, including seven deaths. [PUB.005.001.0425] It was known that the virus is highly contagious and was at that time without a vaccine or even developed means of treating the disease caused by the virus. I refer to my earlier findings in section B.4.5 above in this regard. Further, the risk of transmission was heightened on cruise ships because of the level of socialisation of passengers and crew, the confined indoor spaces, the length of the journey, and the large numbers of international passengers and crew: see section B.5.3 above.
502 In short, the world was in the grips of a global pandemic (although the WHO had not yet named it as such) and the nearly 4,000 guests and crew on board the Ruby Princess had travelled from all around the world. There had already been outbreaks on the Diamond Princess and the Grand Princess, and the Nile River cruises, when the global numbers of COVID-19 infection were significantly lower. There was a significant risk that one or more of the passengers or crew on board may have COVID-19 irrespective of whether they displayed symptoms. An outbreak on board was likely to result in passengers experiencing distress and disappointment and it was likely that the death or serious illness of a passenger could cause close family members of the passenger to experience nervous shock and financial detriment. These were lessons from the earlier tragedies on the Diamond Princess and the Grand Princess.
503 Moving to a narrower focus, it became known in the days and weeks following the cruise that substantial numbers of people who had been on the cruise contracted COVID-19 and many died. By 21 April 2020, NSW Health had announced that 559 people who had been on the Ruby Princess voyage in question had contracted COVID-19, of whom 190 were crew members, and eight people had died. Those figures exclude people who had left NSW after the cruise and before testing positive, of whom there is likely to have been a significant number. [SBM.010.002.0001 [126]; PUB.001.014.0001] As in the case of Mr Karpik, it may be that in any individual case there is room for debate as to whether the person in question contracted the disease on the vessel, but however one looks at it, it is highly probable that a very substantial number of people contracted COVID-19 on the cruise, and some of those people died. That speaks to the services not being reasonably fit for the safety purpose. To put it rhetorically, how can the services have been reasonably fit to keep passengers safe when so many became infected with COVID-19?
504 In light of what was known about the virus at the time, including the experience gained from the Diamond Princess and Grand Princess, it is doubtful that it was possible to provide cruising services that were reasonably fit for the purpose of providing a safe cruise that was also relaxing and pleasurable – quarantining everyone in their cabins might have provided safety but would otherwise have ruined the cruise. That conclusion is supported by:
(1) the respondents’ decisions, first, to offer full refunds on cancellations of cruises departing from 9 March 2020 and thereafter and, second, to suspend all cruises worldwide from 13 March 2020;
(2) the CDC’s “No Sail Order” on 14 March 2020, including its recordal of its prior advice and that of the US Department of State against cruise travel; and
(3) the Australian Government’s decision on 15 March 2020 to, in effect, stop all cruising from and to Australian ports.
505 In relation to (1), the respondents adduced no evidence to explain their decision on 13 March 2020 to suspend all cruises worldwide for 60 days, which period was then subsequently extended. I infer that such evidence would not have assisted the respondents by showing, for example, that the decision was taken for some reason other than because in the environment then pertaining in relation to the pandemic, it was not possible for them to provide safe cruises. The same situation pertained on 8 March 2020. The services were not, and could not be, reasonably fit to achieve their purpose and they were not, and could not be, of such a nature or quality to achieve their result.
506 To the extent that any hindsight reasoning applies here, it is permissible given that information known at the time of trial is to be taken into account in considering whether services were fit for purpose at the time they were supplied. In the weeks and months following the cruise, a lot more was learnt about the virus, its modes of transmission, steps that should be taken to guard against its transmission (eg, far more rigorous screening, physical distancing and masks), and the drastic measures of social control that would be implemented. The legislator put the risk of such matters becoming known only after the relevant services were provided at the door of the service provider, not the consumer. In that sense, the purpose and result guarantees are a little like statutory warrantees of merchantable quality allocating the risk of latent defects to the vendor – to the extent that it could not have been known at the time of the cruise that the services were inadequate to keep the passengers safe from coronavirus, the services were latently defective for which the supplier is liable under the statutory guarantees. Thus, even if there was no negligence by the respondents in their provision of the services, by the statutory provisions they bore the risk of the services not being reasonably fit or not being of the requisite nature and quality.
507 The outbreak of COVID-19 on the Ruby Princess, and hence the failure to achieve the safety, relaxation and pleasure purposes, was not unrelated to the services that the respondents were to provide to Mrs Karpik and the other passengers; the services included safeguarding and protecting the health of passengers. The respondents’ argument that the purpose guarantee cannot operate in relation to such purposes as relaxation or pleasure because they are too susceptible to other influences – eg, marital tension or idiosyncratic tastes – accordingly has no application.
508 It is true, as the applicant complains of, that the respondents failed to provide a 13-day cruise as promised – instead the cruise was only 10 days and it cut out several advertised ports. However, I do not find that aspect to have the result that the purpose guarantee was not met. Not only was the substance of the cruise maintained and the passengers were given a partial refund (and later, a complete refund), but the cruise was necessarily cut short because of Government action, not because of anything related to the provision of the services. There is also nothing to show that the respondents knew, or ought to have known, in advance of the cruise that that was likely to occur, making the failure to deliver what was booked quite different from Scenic No 2. Finally, if there was a failure to comply with the s 61 guarantee in this respect (ie, the loss of three days of the cruise), the defence in ACL s 267(1)(c)(i) is in any event made out, ie, action against the supplier of the services is not available because the failure to comply occurred only because of an act of a person other than the supplier.
509 Insofar as specific shortcomings in the services as to their fitness for purpose and their quality and nature, are relevant, it will be recalled that it is said that the following were deficient: (1) pre-embarkation screening, (2) hand hygiene, and (3) cleaning. It does not seem helpful to consider each of these measures in isolation – if it were necessary I would find deficiencies in pre-embarkation screening of passengers and crew as dealt with in the negligence case below but no particular deficiency in hand hygiene and cleaning. The point is that the services as a whole were required to be reasonably fit for the purpose of providing a relaxing, safe and pleasurable cruise, and they were not. They failed to keep the passengers safe, and they could not reasonably have been expected to keep the passengers safe in light of what we know about the virus and what occurred in the days and weeks following the cruise.
510 In the circumstances, I find that the respondents failed to comply with the purpose and result guarantees.
511 It is common ground that Mrs Karpik’s claim in negligence is governed by the law of New South Wales including, where relevant, the CLA (see [457(7)] above).
512 It is elementary that, in order to succeed in an action in negligence, Mrs Karpik must establish that the respondents owed her a duty of care, that the standard of care required of the duty was breached by acting in a manner inconsistent with what a reasonable person would do by way of response to a foreseeable risk, and that she suffered a compensable injury which was caused by the respondents’ breach: see Graham Barclay Oysters v Ryan [2002] HCA 54; 211 CLR 540 at [230] per Kirby J.
513 As mentioned, the alleged personal injuries for which she claims in negligence include: her COVID-19 infection, Long COVID and adjustment disorder suffered as a consequence of Mr Karpik’s infection and illness. The claimed COVID injuries, being the alleged infection and consequential Long COVID, are said to be caused by a breach of a duty of care owed to Mrs Karpik as a passenger on the cruise ship owned and operated by the respondents. The claimed adjustment disorder injury is not consequential upon her own infection but rather Mr Karpik’s infection. It is therefore not “consequential mental harm” but rather “pure mental harm”: see CLA s 27. The duty said to be owed and breached by the respondents in respect of the adjustment disorder injury is one that is said to be owed to all close family members of passengers.
514 Mrs Karpik contends that the alleged breaches constituted by the respondents’ failure to cancel the cruise, warn passengers of the heightened risk on board, screen passengers for COVID-19 symptoms and introduce physical distancing measures on board were causative of her loss. The remaining alleged breaches are argued for the benefit of group members.
515 The respondents deny that each of the elements of the claim in negligence is satisfied. They also rely on a number of what I shall loosely refer to as “defences”, namely, that there is no duty to warn of an obvious risk (CLA s 5H), that they are not liable for the materialisation of an inherent risk (CLA s 5I), and contributory negligence.
516 In relation to the claim for damages under ACL s 267 that relies on establishing a breach of s 60, Mrs Karpik contends that, save for the fact that the respondents undoubtedly owe a statutory duty to provide services with due care and skill, the question of breach of s 60 is to be resolved consistently with the question of breach of the common law duty of care. See Alameddine v Glenworth Valley Horse Riding Pty Ltd [2015] NSWCA 219; 324 ALR 355 at [59] per Macfarlan JA, Simpson JA and Campbell AJA agreeing; Lets Go Adventures at [6] per Basten and Gleeson JJA, cf [90] per Adamson J.
517 The respondents accept that the question of breach of s 60 is to be resolved together with the negligence claim. However, they do not accept that the question of the duty of care is to be resolved in the way contended by Mrs Karpik. They say that s 60 invites a determination of what due care and skill was required and that if the common law would not have imposed a duty to exercise due care and skill, then no due care and skill is required (T884:30-35).
518 Because of the conclusion that I have reached in respect of the existence and scope of a duty of care at common law, it is unnecessary for me to resolve the parties’ disagreement about whether s 60 imposes a duty of care in circumstances where the common law does not. Accordingly, unless otherwise stated, the conclusions to which I will come in respect of Mrs Karpik’s action in negligence apply equally to her claim under s 267 for breach of s 60.
F.2 Duty of care to passengers
519 In Caltex Refineries (Qld) Pty Ltd v Stavar [2009] NSWCA 258; 75 NSWLR 649 at [101]-[102], Allsop P summarised the development of the common law of Australia’s rejection of any particular formula to determine the existence of a duty of care. The result, his Honour explained, was that if the circumstances fall within an accepted category of duty, little or no difficulty arises. If, however, the posited duty is a novel one, the proper approach is to undertake a close analysis of the facts bearing on the relationship between the plaintiff and the putative tortfeasor by references to the “salient features” or factors affecting the appropriateness of imputing a legal duty to take reasonable care to avoid harm or injury.
520 Mrs Karpik pleads that the respondents owed her a duty to exercise due care and skill in supplying the services. That duty is said to arise out of the well-recognised relationship of occupier and entrant as it applies in the context of a ship operator and passenger. She says that the duty extends to passenger health and safety. She sites in that respect Cruise Group Pty Ltd v Fullard [2005] NSWCA 161 and Qantas Airways Ltd v Cameron [1996] FCA 349; 66 FCR 246. That the relationship between Mrs Karpik and the respondents falls within an accepted category of duty is, she says, the end of the inquiry. There is considerable further common law authority in support of the proposition that a carrier who has undertaken to carry a passenger for reward is under a duty to take reasonable care for the passenger’s safety: Henderson v Stevenson (1875) LR 2 HL Sc 470 at 476 per Lord Chelmsford; Hood v Anchor Line (Henderson Bros) [1918] AC 837 at 844 per Viscount Haldane; Wong Mee Wan v Kwan Kin Travel Services Ltd [1996] 1 WLR 38 at 41-42 (PC). See Lewins K, International Carriage of Passengers by Sea (Sweet & Maxwell, 2016) (Lewins) at [4-006] and Lewins K, “Cruise Ship Operators, Their Passengers, Australian Consumer Law and State Civil Liability Acts – Part 1” (2015) 29(2) Australian and New Zealand Maritime Law Journal 93 at 94.
521 Although the respondents admit in their defence that “the second respondent owed a common law duty of care … to exercise due care and skill when providing services … during the Voyage”, they submit that the duty that is admitted is not the duty on which Mrs Karpik sues. They say that the duty contended for by Mrs Karpik is a novel duty for which reference to the “salient features” or multifactorial approach of imputing such a duty is required. Putting to one side the distinction between the first and second respondents, they say the duty is novel because the relationship of occupier and entrant on which Mrs Karpik sues is a duty with respect only to the “condition of the premises”: Kuhl v Zurich Financial Services Australia Ltd [2011] HCA 11; 243 CLR 361 at [22] per French CJ and Gummow J. In the context of cruise ships, that is a duty in relation to, for example, harm suffered by reason of tripping over a coaming: Fullard at [3]-[6].
522 More than 30 pages of the respondents’ written submissions are dedicated to this issue. The approach appears to have been to identify passages written in judgments concerning wholly different issues (such as the liability for harm caused by third party criminal conduct and the liability of public authorities) and then apply those passages to the different factual context of the present case. As such, they failed to heed the warning of Windeyer J in Mount Isa Mines Ltd v Pusey [1970] HCA 60; 125 CLR 383 at 400 that “[w]e must always beware lest words used in one case become tyrants over the facts of another case.”
523 As a preliminary point, it is beyond question that the respondents owed Mrs Karpik and other passengers a duty of care – the respondents accept that. However, that does not entail that the respondents were required to take reasonable care to avoid all risks of harm to her: Collins v Insurance Australia Ltd [2022] NSWCA 135; 109 NSWLR 240 at [10] per Kirk JA. Nonetheless, the respondents’ various submissions that there is no such duty or that the duty sued upon is a different duty than the duty that is owed serves only to obfuscate the fact that the relevant inquiry is whether the scope of the duty owed by the respondents to Mrs Karpik extends to the kind of harm for which she claims in negligence.
524 The respondents accept that cruise ships are relevantly analogous to airlines. In that respect, the Full Court in Cameron held that an airline owes a duty to all its passengers to take reasonable care for their health and safety: at 250B per Davies J and 290F per Lindgren J (Lehane J agreeing). Cameron was a case in which a group of passengers claimed against Qantas for the discomfort and ill-health caused by inhalation of environmental tobacco smoke in circumstances where they had requested seats in the non-smoking section. It was found by Beaumont J at first instance that Qantas owed the passengers a duty of care: Cameron v Qantas Airways Ltd [1995] FCA 1304; 55 FCR 147 at 187-88. Although Qantas successfully appealed from Beaumont J’s judgment on other grounds, there was no appeal from the finding of the existence or the scope of a duty of care and the Full Court did not express any doubt about that finding. To the contrary, Beaumont J’s conclusions on the scope of the duty of care Qantas owed to its passengers were endorsed by Lindgren J at 290F (Lehane J agreeing).
525 The reasoning in Cameron is instructive. The harm for which damages were claimed was discomfort and ill-health caused by the inhalation of tobacco smoke produced by other passengers. The duty of care was framed as a duty to take reasonable care for the health and safety of passengers. It was not Qantas that produced the tobacco smoke. The duty extended to the risk of harm caused by tobacco smoke produced by other passengers.
526 As against that, the respondents seek to cast the duty posited by Mrs Karpik as a duty to “prevent the spread of contagious diseases” or a duty to “protect patrons from one another”, each characterisation of which they say is foreclosed by the authorities. In respect of a duty to prevent the spread of contagious disease, they say that Cameron is distinguishable because an airline can ban smoking on board thereby eliminating the risk of inhalation of tobacco smoke and that no court has ever found such a duty in relation to disease. In respect of contact between human beings, they rely on Modbury Triangle Shopping Centre Pty Ltd v Anzil [2000] HCA 61; 205 CLR 254.
527 Each of those characterisations is wrong as it is addressed at an inappropriate level of specificity. By characterising the relevant duty with such specificity, the determination of Mrs Karpik’s case would be circumvented by having the issues decided at the duty stage in circumstances where the crux of the dispute in the negligence case is whether they failed to take reasonable care and whether that failure caused her harm.
528 The question of the existence or non-existence of a duty of care is to be considered at a higher level of abstraction, or generality, than questions of breach: Shirt v Wyong Shire Council [1978] 1 NSWLR 631 at 639 per Glass JA; Graham Barclay Oysters at [106] per McHugh J; Harriton v Stephens [2006] HCA 15; 226 CLR 52 at [69]-[70] per Kirby J and [226] per Crennan J (with whom Gleeson CJ and Gummow and Heydon JJ agreed). That higher level of abstraction involves expressing the duty in terms of a want of reasonable care. As explained by McHugh J in Vairy v Wyong Shire Council [2005] HCA 62; 223 CLR 422:
25 … [T]he duty in negligence is generally described as a duty to take reasonable care… In negligence cases involving physical injury … the duty is always expressed in terms of reasonable care. As Prosser and Keeton have pointed out, “the duty is always the same — to conform to the legal standard of reasonable conduct in the light of the apparent risk.”
26 As a result, the duty owed by motorists to other users of the highway, for example, is expressed in terms of the duty to take reasonable care for the safety of other users of the highway having regard to all the circumstances of the case. The duty is not subdivided into categories such as a duty to keep a proper lookout or sound a warning or to keep a safe distance away from the car in front. In the particular circumstances of the case, failure to do one or more of these things may constitute a breach of the duty to take reasonable care. But they are not themselves legal duties for the purpose of the law of negligence. If they were, a trial judge would be bound to direct a jury in the circumstances of a particular case that the defendant had a duty to keep a proper lookout or sound his or her horn, as the case may be. Given such a direction, the only question for the jury would be whether or not a motorist had complied with the duty specified by the judge. But it is the jury, not the judge, that determines whether reasonable care required the motorist to keep a proper lookout or to sound the horn…
(Emphasis added.)
529 Justice McHugh also explained that the so-called “duty to warn”, which is a “duty” which the respondents argue against, is not properly concerned with the existence or non-existence of a duty of care but rather the standard of care at the breach stage: Vairy at [29]. See also Collins at [9] per Kirk JA.
530 Although McHugh J was in dissent in Vairy, it cannot be disputed, as the respondents seem to do (SBM.020.005.0001 [181], T858:44), that those passages are an accurate summary of the law. They have been cited with approval in numerous High Court judgments, including most recently by a unanimous court in Electricity Networks Corporation t/as Western Power v Herridge Parties [2022] HCA 37; 406 ALR 1 at [20], as well as Roads and Traffic Authority v Dederer [2007] HCA 42; 234 CLR 330 at [49] per Gummow J; Neindorf v Junkovic [2005] HCA 75; 222 ALR 631 at [56] per Kirby J; Harriton v Stephens [2006] HCA 15; 226 CLR 52 at [69] per Kirby J.
531 It is therefore incorrect to characterise the duty as one requiring the respondents to prevent the spread of contagious disease. Such a characterisation suffers from the “vice of retrospective over-specificity” in the way identified by Hayne J in CAL No 14 Pty Ltd v Motor Accidents Insurance Board [2009] HCA 47; 239 CLR 390 at [68].
532 Nor do I think is it correct to characterise the duty in terms of the protection of patrons from one another, at least in the way contended for by the respondents and in the circumstances of the present case. As mentioned, the submission that the duty contended for by Mrs Karpik is such a duty is founded upon the High Court’s decision in Modbury Triangle. That case concerned an employee of a video shop business in a shopping centre who was attacked and injured whilst walking to his car in the car park late at night. He commenced proceedings against the occupier of the car park alleging a breach of its duty of care by failing to leave floodlights on in the car park. It was held that the duty of care owed by an occupier of a shopping centre with an adjacent car park did not extend to harm suffered by employees of its tenants at the hands of third party criminal conduct.
533 The respondents seek to characterise a duty that extends to harm caused by a virus that transmits through human-to-human contact as a duty that extends to controlling third party conduct (albeit not criminal conduct) and thereby bring themselves within Modbury Triangle. They also rely on the following passage from the judgment of Dixon J in Smith v Leurs [1945] HCA 27; 70 CLR 256 at 262:
It is, however, exceptional to find in the law a duty to control another’s actions to prevent harm to strangers. The general rule is that one man is under no duty of controlling another man to prevent his doing damage to a third.
534 Critical to the reasoning in reaching the conclusion in Modbury Triangle that the occupier of a car park owed no duty of care to entrants upon the land in respect of third party criminal conduct was that the occupier had no control over the unpredictable and random behaviour of unknown thugs who attacked the employee and no knowledge or forewarning of what they planned to do: see at [19]-[29] per Gleeson CJ, Gaudron J and Hayne J agreeing, and at [108] per Hayne J. Thus, the case has been distinguished in subsequent decisions of intermediate appellate courts in circumstances where an occupier has knowledge (actual or constructive) of the real potential for third party criminal conduct in circumstances where the occupier controls access to the premises: see, eg, Club Italia (Geelong) Inc v Ritchie [2001] VSCA 180; 3 VR 447 at [34]-[36] per Brooking, Charles and Chernov JJA and Rooty Hill RSL Club Ltd v Karimi [2009] NSWCA 2 at [34] and [58]-[59] per Bell JA, Allsop P and Basten JA agreeing; cf Ashrafi Persian Trading Co v Ashrafinia [2001] NSWCA 243; [2002] Aust Torts Reports ¶81-636 at [70]-[81] per Heydon JA, Mason P and Handley JA agreeing.
535 Insofar as the posited duty can be characterised as one that involves controlling third party conduct, the present case is far removed from the circumstances of Modbury Triangle. Unlike the occupier of an unsecured car park that had no relevant control over the conduct of the thugs or knowledge of their actions, the respondents in the present case had direct control over at least the following: who they let on board the vessel and the conditions on which they did so; how many people they let on board; the cabins assigned to both the passengers and crew; the number of entertainment events being held and the conditions of entry to those venues; the systems and policies in place to reduce contact between people; cleaning regimes; conditions of service of food; provision of PPE and measures such as face masks and hand sanitiser; etc. Indeed, the respondents accept in their submissions that they had the power to create and implement policies on board directed at addressing the risk of coronavirus.
536 The submission that the respondents’ duty does not extend to controlling the conduct of those on board the vessel sits awkwardly with their actual policies and conduct with regard to confining ill passengers to their cabins. It is contradicted by clause 32 of the applicable terms and conditions which provided that if a guest seriously affects the safety or well-being of any other person on board, the master had the right to confine, sedate or disembark the guest (see [457(5)] above). It also sits awkwardly with the power of the master of a ship at common law to detain and confine passengers or crew where the master has reasonable cause to believe, and does in fact believe, that the relevant detention or confinement is necessary for the preservation of order and discipline, or for the safety of the vessel or persons or property on board: Royal Caribbean Cruises Ltd v Rawlings [2022] NSWCA 4; 107 NSWLR 51 at [20]-[23] per Meagher JA, Bell P and Leeming JA agreeing. Although the present case was not presented on the basis of a master’s common law power, it seems likely that the master could quarantine any individual reasonably suspected of being infected with coronavirus by confining them to their cabin, it being highly doubtful that the safety of passengers (and crew) does not extend to the risk of contracting communicable and potentially fatal diseases.
537 In any event, the risk of coronavirus infection on board does not come only from other passengers. It comes from the respondents’ employees, the crew, and from surfaces contaminated by passengers or crew on a previous voyage. In that context, to say that the respondents cannot owe a duty to protect passengers from each other would be like saying that a supermarket owner owes no duty to protect customers from slipping and falling on food carelessly spilled by other customers. We know that to be wrong.
538 The quotation from Leurs (at 262) relied on by the respondents does not assist. The remarks of Dixon J were made in the context of his Honour’s acceptance of the existence of a duty of care of parents (or those in loco parentis) owed to strangers with respect to harm caused by the actions of children under their care. Immediately preceding that quote, his Honour referred to circumstances where a person may be responsible for harm done to another the direct cause of which was the actions of a third party:
[H]e may be responsible on the ground that the act of the third person could not have taken place but for his own fault or breach of duty. There is more than one description of duty the breach of which may produce this consequence. For instance, it may be a duty of care in reference to things involving special danger. It may even be a duty of care with reference to the control of actions or conduct of the third person.
539 Such duties arise out of a “special relationship” of an exceptional kind. Such relationships exist between, for example, school principals and pupils (see, eg, Geyer v Downs [1977] HCA 64; 138 CLR 91), bailor and bailee (see, eg, Pitt Son & Badgery Ltd v Proulefco SA [1984] HCA 6; 153 CLR 644), and gaolers and prisoners (see, eg, New South Wales v Bujdoso [2005] HCA 76; 227 CLR 1) to name a few. In my view, the relationship between a ship’s operator – being the party in possession or having the management and control of the ship – and its passengers is also such a special relationship.
540 Like passengers on an aircraft, passengers on a cruise ship are “captives”: see Cameron at 290E per Lindgren J. As mentioned, the fact that aircraft are relevantly similar to cruise ships is accepted by the respondents. Indeed, in an internal memorandum drafted by the President of Princess and Carnival Australia, Ms Swartz, addressing the risk of coronavirus circulated on 25 February 2020, it is said that “[c]ruise ships, like aircraft, are semi-contained, population dense environments.” [PCL.001.006.7127; PCL.001.006.7128 p 2]
541 However, unlike airline passengers, cruise passengers are generally “captives” for a much longer period of time. Certainly that is the case with voyages of the kind supplied as a service by the respondents in the present case. Once passengers have boarded, they are necessarily reliant on the ship’s operator to provide all services, from basic shelter from the elements and necessities such as food and water, to medical assistance. They are also necessarily reliant on the ship operator to take them safely back to shore. Thus, as explained by the Full Court (Black CJ, Emmett and Allsop JJ) in ASP Ship Management Pty Ltd v Administrative Appeals Tribunal [2006] FCAFC 23; 149 FCR 261 at [98] (albeit in the context of an oil tanker), a ship is:
a working commercial enterprise, often both the home and workplace, for long periods, to the ship’s complement. The ship is engaged in activity that has inherent danger to those on board, and is a potential source of environmental and other danger to her physical and human surroundings. For those reasons, those having the management and control of the ship have responsibilities concerning the commercial deployment of the ship, the technical safety and adequacy of the ship as a complex integrated working entity, and of the choice, supervision, care and discipline of the master and crew on board the ship.
542 In respect of a passenger vessel, one must add to that analysis the passengers who are on holiday in an environment from which they cannot readily escape and from which they cannot readily access any services, resources or support beyond what is provided by the ship’s operator.
543 It is recognised that the peculiar nature of a ship influences the nature and content, including the scope, of a duty of care that is owed in a maritime context. That reflects the realities of maritime activities and commerce: CSL Australia Pty Ltd v Formosa [2009] NSWCA 363; 261 ALR 441 at [64] per Allsop P, Basten JA and Handley AJA and the cases there cited. For example, in Kermarec v Compagnie Generale Transatlantique (1959) 358 US 625, the United States Supreme Court held that the distinction then drawn by the common law between a licensee and an invitee was not only inapt but “entirely alien” in a maritime context. The Court found that that a shipowner owed a higher standard of care to the invited guest of a crewmember than that owed to a gratuitous licensee of a land-based premises because a shipowner owes a duty of exercising reasonable case to all who are on board for purposes not inimical to the owner’s legitimate interests (see 629-632). In a similar vein, in CSL Australia, the Court stressed that the general principle that an occupier need not give warnings of defects in the premises to invitees who are tradesmen or experts is qualified in a maritime context because stevedores coming aboard the ship carry out their work in the environment of, and with the equipment and machinery provided by, the ship and in circumstances where the master and officers of the ship retain a right to direct their work (see [63]-[74]).
544 The reliance by the passengers of the Ruby Princess on the respondents for their safety cannot be negated merely because the passengers voluntarily decided to board the vessel. The necessity of such reliance is what gives rise to the power of a master to arrest, detain and confine passengers and crew in certain circumstances (see Rawlings at [25]-[26] and the authorities there cited), as well as the scope of a ship operator’s duty of care for the safety of its passengers extending to rescuing them from overboard – “the employee or passenger, who falls overboard from whatever cause, should be entitled to look for succour to the operators of the ship because of necessary dependency on them for return to shore”: Horsley v Maclaren (The Ogopogo) [1972] SCR 441 at 461-462 per Laskin J (in dissent on whether there was negligence and hence the outcome, but all of the judges of the Supreme Court of Canada agreed on there being a duty on the operator of a cabin cruiser to rescue an invited guest), cited with approval in Frost v Warner [2002] HCA 1; 209 CLR 509 at [60] per Gaudron J. That duty is recognised in circumstances where the common law does not otherwise recognise a duty to rescue, save in cases of a “special relationship”: Ibrahimi v Commonwealth of Australia [2018] NSWCA 321; 366 ALR 341.
545 There is also the fact of the respondents’ peculiar knowledge (as compared with ordinary passengers such as the Karpiks) of facts relevant to: the nature of the virus, its transmissibility and consequences of infection by it; the absence of a vaccine and limited treatment options; the risk of the spread of coronavirus on cruise ships, and on the Ruby Princess voyage RU2007 in particular; the precautions actually being taken by the respondents; the developing situation worldwide, including relevant protocols, guidance and advice. Those matters have been canvassed at length in sections B.4 and B.5 above. That knowledge means that the respondents were in a special position to appreciate the risks facing their passengers, and the facts underlying the knowledge establish that it was reasonably foreseeable that passengers might contract COVID-19 on board from other passengers or crew.
546 Each of the foregoing matters strongly supports the conclusion that the respondents owed Mrs Karpik a duty to take reasonable care for her health and safety, including with regard to the risk of harm caused by coronavirus infection. I shall deal briefly with the respondents’ remaining arguments contending against the existence of such a duty.
547 The respondents submit that the fact that governments had the legislative power, or pursuant to legislation had the executive power to make instruments, to regulate the risk caused by coronavirus, which they later exercised to impose draconian restrictions on basic liberties, tends strongly, if not decisively, against a duty that extends to the risk of harm caused by coronavirus. They say that the absence of the exercise of that public power as at 8 March 2020 in Australia is a strong reason not to overlay common law obligations in negligence with additional and inconsistent obligations. They say that the point was made by the High Court in Sullivan v Moody [2001] HCA 59; 207 CLR 562 at [60], where the following was said:
The circumstance that a defendant owes a duty of care to a third party, or is subject to statutory obligations which constrain the manner in which powers or discretions may be exercised, does not of itself rule out the possibility that a duty of care is owed to a plaintiff. People may be subject to a number of duties, at least provided they are not irreconcilable. A medical practitioner who examines, and reports upon the condition of, an individual, might owe a duty of care to more than one person. But if a suggested duty of care would give rise to inconsistent obligations, that would ordinarily be a reason for denying that the duty exists.
(Respondents’ emphasis.)
548 The submission must be rejected.
549 First, there is no authority cited for the proposition that government involvement in legislating or regulating certain activities tends against the existence of a duty. Indeed, the quoted passage itself says that “[p]eople may be subject to a number of duties, at least provided they are not irreconcilable.”
550 Secondly, the fact that the law of negligence might require a duty of reasonable care that is more onerous than any statute or legislative instrument does not thereby make those duties irreconcilable or inconsistent. The apparent inconsistency in the present case concerns the fact that no Australian government had yet imposed any restrictions with respect to cruise ships and indoor gatherings. Acceptance of the respondents’ submission would entail accepting that the law of negligence imposes no obligations in addition to those imposed by statute or legislative instrument. That would make the entire body of law otiose.
551 Thirdly, it is difficult to identify the relevance, if any, of the remark emphasised by the respondents. Sullivan v Moody was a case about the existence of a duty of care of employees of a public authority. It was held that the existence of a duty that was contended for in that case would be inconsistent with the proper and effective discharge of the statutory responsibilities of those employees. The respondents are not public authorities or employees of public authorities. Nor do they conduct their voyages in the exercise of a statutory obligation or power.
552 The respondents also raise a number of “floodgates” arguments. First, they say that the duty would not be limited to coronavirus. Secondly, they say that the duty would exist in perpetuity – ie, that even on cruises departing today and into the future, cruise operators would owe duties of care to passengers extending to the risk of COVID-19 infection. Thirdly, they say that the duty would not be limited to cruise ships – it would apply to other providers of mass transit and other businesses such as hotels, gyms, offices, etc. I apprehend that these arguments seek to rely upon “the law’s concern to avoid the imposition of liability ‘in an indeterminate amount for an indeterminate time to an indeterminate class’”: Bryan v Maloney [1995] HCA 17; 182 CLR 609 at 618 per Mason CJ, Deane and Gaudron JJ, citing Ultramares Corporation v Touche (1931) 225 NY 170 (NY Ct App) at 179 per Cardozo CJ.
553 However, none of the arguments is addressed to the issue of indeterminacy. In Perre v Apand Pty Ltd [1999] HCA 36; 198 CLR 180, McHugh J explained:
106 … Concern about indeterminacy most frequently arises where the defendant could not determine how many claims might be brought against it or what the general nature of them might be…
107 However, it is not the size or number of claims that is decisive in determining whether potential liability is so indeterminate that no duty of care is owed. Liability is indeterminate only when it cannot be realistically calculated. If both the likely number of claims and the nature of them can be reasonably calculated, it cannot be said that imposing a duty on the defendant will render that person liable “in an indeterminate amount for an indeterminate time to an indeterminate class”.
109 … If the defendant knows or has the means to know who are the members of an ascertainable class affected by its conduct and the nature of the likely losses to members of that class, its liability is not indeterminate.
(Emphasis added; footnotes omitted.)
554 The duty owed by the respondents is to take reasonable care for the health and safety of their passengers. Although the risk to the health and safety of passengers will take myriad forms, there is nothing indeterminate about the nature of the harm that might befall them. The respondents complain that there are numerous other diseases that collectively infect and kill millions of people each year. It may be asked: so what? Insofar as the complaint is that they might be held liable for unforeseeable risks, it is necessary (but not sufficient) for a risk of harm to be reasonably foreseeable in order for a duty to arise: Sydney Water Corporation v Turano [2009] HCA 42; 239 CLR 51. Suppose that a cruise operator became aware that a passenger on board was infected with the Ebola virus. On the respondents’ case, they would have no duty of care extending to the risk of harm that that deadly disease would spread throughout the ship. They would, on their case, be entitled to stand by and do nothing, notwithstanding knowledge of the infection and their admitted control in the power to create and implement policies on board directed at addressing the risk. That could not possibly be the law.
555 In respect of the complaint that the duty would exist in perpetuity, that characterisation ignores the fact that each of the passengers to which the duty is owed are all paying customers of the respondents that they have invited on board their vessels. Large though that class may be, it is clearly ascertainable and, therefore, not indeterminate in number or time.
556 The respondents’ arguments with regard to the novelty, floodgates and burden of the duty are somewhat undermined by the fact that a significant number of countries have ratified or acceded to, or otherwise made applicable (eg, Bermuda, Canada and China – Lewins [3-017]), the Athens Convention relating to the Carriage of Passengers and their Luggage by Sea, 1974 (Athens 1974) or the Protocol to that Convention, 2002 (Athens 2002). As at the time of writing, Athens 1974 has about 28 ratifications or accessions and Athens 2002 has 30. These countries include countries with substantial passenger fleet tonnage. Article 3(1) of Athens 1974 provides that the carrier shall be liable for the damage suffered as a result of the death of or personal injury to a passenger if the incident which caused the damage so suffered occurred in the course of the carriage and “was due to the fault or neglect of the carrier.” That is to say, it imposes a duty on the carrier to act reasonably in preventing injury to passengers. Athens 2002 alters that regime by imposing strict liability for injuries and death up to a certain amount (250,000 SDRs) and imposing liability up to a higher amount (400,000 SDRs) unless the carrier can disprove negligence – SDRs being Special Drawing Rights of the International Monetary Fund. These matters are explained in Lewins, Ch 3.
557 The point is that in substantial parts of the world, including in Bermuda where the Ruby Princess is flagged, a duty such as that disputed by the respondents in the present case on the basis that it would be novel and burdensome is imposed either by Convention or domestic law. There is no suggestion that that has imposed intolerable burden on cruise lines. What it means is that the focus of any claim is on the conduct of the cruise line and whether it was negligent, which is where the focus of attention should be in the present case. An example is Nolan v TUI (UK) Ltd [2016] 1 Lloyd’s Rep 211 (Central London County Court) where the claims arising from a norovirus outbreak on board were dismissed on the basis that the defendant had discharged its duty of care to the claimants – the ship had correctly followed its own policy, which included detailed provisions as to cleaning and food handling (at [91]). Another example is Swift v Fred Olsen Cruise Lines [2016] EWCA Civ 785. There, the cruise line was held liable for the claims arising from a norovirus outbreak on the basis that it had not adequately implemented its own norovirus outbreak plan.
558 The third argument with respect to other providers of mass transit and other businesses is incorrect. In respect of other businesses, different considerations apply. Without purporting to decide the scope of any duty owed by the other types of businesses referred to by the respondents, there are different levels of control, knowledge, reliance and dependence in respect of patrons of those other businesses. In particular, save for passengers of airlines, none of them can be said to be captives in the same way as passengers of a cruise ship, or to have the same level of dependence.
559 In the result, I find that the respondents owed Mrs Karpik a duty to take reasonable care for her health and safety. By reference to the authorities cited at [528] above as well as Cameron, I consider that to be a sufficient description of the duty. However, for the avoidance of doubt, that duty extends to the risk of harm caused by COVID-19 infection. It also extends to Mr Karpik as another passenger on the cruise.
F.3 Duty of care to close family members
560 As mentioned, Mrs Karpik’s claim for damages for her contended-for adjustment disorder is based upon an alleged breach of a duty of care owed by the respondents to her as a close family member of Mr Karpik. “Close family member” is defined in the further amended statement of claim (FASOC) by reference to the definition of “close member of the family” in s 30(5) of the CLA. That definition includes “the spouse or partner of the victim.”
561 As an aside, I observe that it is not apparent that liability arises under ACL s 60 in circumstances where the harm that is suffered by the applicant (mental harm) arises from a breach of the obligation to supply services with due care and skill to a different consumer. It may be thought that the guarantee under s 60 is a guarantee to the consumer as consumer, and not to a person as a close family member of a different consumer. This point was not, however, raised by the parties and I therefore put it to one side.
562 The question whether the respondents owed Mrs Karpik, as a close family member, a duty of care with respect to mental harm falls to be decided, on the common law negligence claim, by the operation of CLA s 32: Wicks v State Rail Authority of New South Wales; Sheehan v Same [2010] HCA 22; 241 CLR 60 at [22]-[24].
563 Section 32 of the CLA relevantly provides:
32 Mental harm—duty of care
(1) A person (the defendant) does not owe a duty of care to another person (the plaintiff) to take care not to cause the plaintiff mental harm unless the defendant ought to have foreseen that a person of normal fortitude might, in the circumstances of the case, suffer a recognised psychiatric illness if reasonable care were not taken.
(2) For the purposes of the application of this section in respect of pure mental harm, the circumstances of the case include the following—
(a) whether or not the mental harm was suffered as the result of a sudden shock,
(b) whether the plaintiff witnessed, at the scene, a person being killed, injured or put in peril,
(c) the nature of the relationship between the plaintiff and any person killed, injured or put in peril,
(d) whether or not there was a pre-existing relationship between the plaintiff and the defendant.
(3) For the purposes of the application of this section in respect of consequential mental harm, the circumstances of the case include the personal injury suffered by the plaintiff.
564 By providing that a duty is not to be found unless certain conditions are satisfied, s 32 operates as a condition for the establishment of a duty of care: Wicks at [22]. That is, s 32 defines or controls what would otherwise be a duty of care arising under the common law. As explained in section D.6 above, s 32 has no application to Mrs Karpik’s claim for failure to comply with ACL ss 60 and 61.
565 It was explained in Wicks at [24] that s 32 must be understood against the background provided by the common law of negligence in relation to psychiatric injury as stated in Tame v State of New South Wales; Annetts v Australian Stations Pty Ltd [2002] HCA 35; 211 CLR 317. In Tame it was held that the central question in determining whether a duty at common law is owed to take reasonable care to avoid mental harm (or, more accurately, recognised psychiatric injury) is whether, in all the circumstances, the risk of sustaining such an injury is reasonably foreseeable in the sense that the risk was not far-fetched or fanciful: [12], [29] per Gleeson CJ, [89]-[90] per McHugh J, [201] per Gummow and Kirby JJ and [275] per Hayne.
566 It is admitted by the respondents that there was a foreseeable risk that passengers would contract COVID-19 and as a consequence would become severely ill or die. They also admit that at all material times prior to and during the voyage, there was a risk that close family members of passengers would suffer a recognised psychiatric injury arising wholly or in part from mental or nervous shock in connection with those passengers dying or becoming severely ill by reason of contracting COVID-19. They deny, however, that that admitted risk was reasonably foreseeable.
567 That denial is contrary to long-established authority: see Jaensch v Coffey [1984] HCA 52; 155 CLR 549; Gifford v Strang Patrick Stevedoring Pty Ltd [2003] HCA 33; 214 CLR 269 and King v Philcox [2015] HCA 19; 255 CLR 304. There is little to distinguish the present case from those cases insofar as the foreseeability of psychological harm is concerned.
568 The respondents advance three arguments as to why CLA s 32 otherwise precludes the finding of a duty in the present case.
569 First, they say that they ought not to have foreseen that if passengers contracted COVID-19 on the voyage, other passengers would suffer a recognised psychiatric illness. This argument, directed as it is to other passengers, is entirely irrelevant to the question whether a duty was owed to close family members of passengers. Mrs Karpik claims to have suffered pure mental harm (ie, not mental harm that is a consequence of a personal injury of any other kind – CLA s 27) as a close family member of Mr Karpik.
570 Secondly, the respondents say that Mrs Karpik’s alleged harm was not suffered “as a result of sudden shock” (CLA s 32(2)(a)). Thirdly, they say that Mrs Karpik is not someone who “witnessed, at the scene, a person being killed, injured or put in peril” (CLA s 32(2)(b)).
571 As explained in Wicks at [26] and [31], neither of those circumstances is necessary to found the existence of a duty. They are merely aspects of the “circumstances of the case” that are relevant to the inquiry directed by s 32(1), namely whether the respondents ought to have foreseen that a person of “normal fortitude” might suffer a recognised psychiatric injury if reasonable care were not taken. They are to be treated as relevant to the assessment of the foreseeability of risk of harm as a necessary condition to the existence of the duty of care: King v Philcox at [13] per French CJ, Kiefel and Gageler JJ.
572 In the present case, it is not suggested that mental harm was suffered as a result of a sudden shock (s 32(2)(a)) or that Mrs Karpik witnessed Mr Karpik being killed, injured or put in peril (s 32(2)(b)). However, Mrs Karpik is the spouse of Mr Karpik who is the person injured and put in peril (s 32(2)(c)) and Mrs Karpik had an existing relationship with the respondents (s 32(2)(d)) – she was a passenger on the respondents’ ship. That deals with the aspects of the circumstances of the case mandated by s 32(2), but what of other relevant circumstances?
573 The parties dealt with the question of “normal fortitude” in their liability submissions, where it properly belongs, but also in their quantum submissions. That approach may have been driven by the fact that it is in the quantum submissions that detailed consideration is given to the nature of Mrs Karpik’s “psychiatric illness.” I will come to those matters in some detail when addressing the question of quantum, but in the meantime further “circumstances of the case” should be identified. In that regard, the need to consider “the circumstances of the case” is not to ask whether the circumstances were reasonably foreseeable, but whether, given those circumstances, a person of “normal fortitude” might suffer psychiatric illness. That question is not appropriately answered by saying that the circumstances of the case were not foreseeable: Capar at [92] per Basten JA, McCallum JA agreeing.
574 The relevant circumstances might be said to include that the applicant’s husband was infected with COVID-19, a potentially life-threatening disease, as a result of which he was hospitalised for a long time, intubated and ventilated and placed in an induced coma, and came so close to death due to widespread organ failure that the applicant was informed that he had only a 10% chance of survival with about three days to live.
575 The respondents rely on evidence given by Dr Samuels that it would be entirely expected that a person of normal fortitude would experience depression, anxiety, distress and anticipatory grief in relation to their husband’s potentially life-threatening illness, but where there has been a favourable clinical outcome as evidenced by Mr Karpik recovering and returning home, Dr Samuels “would not have expected these symptoms to progress to a clinical syndrome such as experienced by Mrs Karpik.” There are two difficulties with that evidence forming the basis for rejecting a duty of care in the present circumstances. First, Dr Samuels was asked, and answered, the wrong question – the right question is whether a person of normal fortitude might suffer a recognised psychiatric illness, and not if they would do so. It is quite possible within the evidence otherwise given by Dr Samuels that had he been asked the right question he would have agreed that a person of normal fortitude might suffer a recognised psychiatric illness.
576 Secondly, expert evidence about the foreseeability of a risk of psychiatric injury is not decisive. The question of reasonable foreseeability involves an assessment respecting the foresight of a reasonable person in the respondents’ position; that foresight may differ from the foresight of qualified psychiatrists. The judgement belongs, ultimately, to the court which will draw on its reserves of common sense and reasonableness. See Tame at [234] per Gummow and Kirby JJ, and [115] per McHugh J. The test required by s 32 requires an objective and prospective judgement, and the question as to what might be expected of a person of normal fortitude in the circumstances of the case could be the subject of expert evidence but helpful evidence may not be easy to come by given that the concept of “normal fortitude” is scientifically inexact: Capar at [93]-[94].
577 Both sides of the case draw attention to previous cases in which it was found that the normal fortitude test was not satisfied. To my mind, the circumstances of the present case with reference to the severity of Mr Karpik’s illness that impacted on Mrs Karpik, a close family member of the person injured, are notably more serious than those cases. For example:
(1) In Tomisevic v Menzies Wagga Wagga Southern Pty Ltd [2005] NSWCA 178 (at [39]), it was not reasonably foreseeable that a person of normal fortitude might suffer a recognised psychiatric illness as a result of being splashed in the face by water contaminated with faeces.
(2) In Crump v Equine Nutrition Systems Pty Ltd [2006] NSWSC 512 (at [257]), it was not reasonably foreseeable that a person of normal fortitude might suffer from a psychiatric injury as a result of the death of a horse because by contaminated feed purchased from the defendant.
(3) In Hollier v Sutcliffe [2010] NSWSC 279 (at [232]), it was not reasonably foreseeable that a person of normal fortitude might suffer from a recognised psychiatric illness as a result of a contraceptive implant being incorrectly inserted in the plaintiff’s upper arm in a relatively simple procedure taking a matter of minutes.
(4) In Thompson v NSW Land and Housing Corporation [2011] NSWSC 941 (at [68]), it was not reasonably foreseeable that a person of normal fortitude might suffer from a recognised psychiatric illness as a result of exposure to household pesticides, the defendant having engaged a pest control company to carry out termite eradication.
578 Comparing those cases to the cases referred to at [567] above, I am satisfied that a person of normal fortitude might suffer a recognised psychiatric illness if exposed to the circumstances of the present case. The duty of care is therefore not excluded by CLA s 32(1).
579 In the result, I find that the respondents owed Mrs Karpik a duty of care with respect to a recognised psychiatric illness arising from Mr Karpik contracting COVID-19 on the voyage. That is the case in respect of the claim in negligence because the “normal fortitude” test or requirement in CLA s 32(1) is satisfied. As I have explained above, ACL s 275 does not pick up CLA s 32 so it does not apply to the ACL claims.
580 Sections 5B and 5C of the CLA provide:
5B General principles
(1) A person is not negligent in failing to take precautions against a risk of harm unless—
(a) the risk was foreseeable (that is, it is a risk of which the person knew or ought to have known), and
(b) the risk was not insignificant, and
(c) in the circumstances, a reasonable person in the person’s position would have taken those precautions.
(2) In determining whether a reasonable person would have taken precautions against a risk of harm, the court is to consider the following (amongst other relevant things)—
(a) the probability that the harm would occur if care were not taken,
(b) the likely seriousness of the harm,
(c) the burden of taking precautions to avoid the risk of harm,
(d) the social utility of the activity that creates the risk of harm.
5C Other principles
In proceedings relating to liability for negligence—
(a) the burden of taking precautions to avoid a risk of harm includes the burden of taking precautions to avoid similar risks of harm for which the person may be responsible, and
(b) the fact that a risk of harm could have been avoided by doing something in a different way does not of itself give rise to or affect liability for the way in which the thing was done, and
(c) the subsequent taking of action that would (had the action been taken earlier) have avoided a risk of harm does not of itself give rise to or affect liability in respect of the risk and does not of itself constitute an admission of liability in connection with the risk.
581 It is common ground that CLA ss 5B and 5C apply in the determination of whether the respondents were in breach of their duty of care to Mrs Karpik, and also Mr Karpik insofar as Mrs Karpik’s claim for damages for her contended-for adjustment disorder is concerned. It is also common ground that the applicable principles with respect to breach of duty for Mrs Karpik’s ACL s 60 claim are the same, as those provisions are essentially a statutory enactment of the common law position: cf Wyong Shire Council v Shirt [1980] HCA 12; 146 CLR 40 at 47-48 per Mason J.
582 Satisfaction of the conditions in s 5B(1) is a necessary, but not sufficient, prerequisite for civil liability to arise: Penrith Ruby League Club Ltd v Elliot [2009] NSWCA 247 at [22] per Sackville AJA, with whom Ipp and Basten JJA agreed. Nevertheless, satisfaction of the three preconditions in s 5B(1) will almost invariably result in a finding of negligence: Laresu Pty Ltd v Clark [2010] NSWCA 180 at [44].
583 The necessary first step is to properly identify the risk of harm because it is only by identifying the relevant risk of harm that one can then proceed to ascertain its foreseeability, and the appropriate response of a reasonable person to that risk: Tapp v Australian Bushmen’s Campdraft & Rodeo Association Ltd [2022] HCA 11; 399 ALR 535 (Tapp HCA) at [106] per Gordon, Edelman and Gleeson JJ. It is said that a risk is real and foreseeable if it is not far-fetched or fanciful, even if it is extremely unlikely to occur. Also, the precise and particular character of the injury or the precise sequence of events leading to the injury need not be foreseeable; it is sufficient if the kind or type of injury was foreseeable, even if the extent of the injury was greater than expected. See Tapp HCA at [109] citing Rosenberg v Percival [2001] HCA 18; 205 CLR 434 at [64] per Gummow J.
584 In the present case, the relevant risk of harm is of a passenger contracting COVID-19 and becoming seriously ill or dying as a consequence, and a close family member of such a passenger suffering a recognised psychiatric injury. I have already discussed those matters. They were plainly foreseeable.
585 It is also pleaded, and admitted, that there was a risk that passengers would suffer distress by being aware of being in close contact with a person who contracted COVID-19. It is, however, denied that that risk was reasonably foreseeable. This part of the case was not pressed at trial so nothing more need be said about it.
586 The question then is whether, in the circumstances, a reasonable person in the respondents’ position would have taken the precautions against the risk that the applicant says they should have taken. That requires consideration of the factors identified in s 5B(2), which subsection essentially codifies what Mason J said in Shirt at 47.
587 Plainly, the factors required for consideration by paras (a), (b) and (d) (namely, the probability of harm and its seriousness, and the social utility of, here, cruising) are the same in respect of each of the precautions that Mrs Karpik alleges a reasonable person in the position of the respondents ought to have taken.
588 Dealing first with the likely seriousness of the harm, there can be no doubt that, if passengers were to become infected with the virus and thereby contract COVID-19, the consequences could not be more serious. As mentioned, the not insignificant risk that those who contracted COVID-19 would become severely ill or die is admitted by the respondents.
589 In respect of the probability of harm occurring, although the risk of harm in the general community was at the time very low, the risk was not inherently unlikely to materialise. The virus was highly contagious. As I have found in section B.5.3 above, cruise ships are peculiarly susceptible to coronavirus infection and transmission when compared to the community generally, including by reason of the demographics of those on board. Indeed, there had already been confirmed cases on board two Princess vessels over three voyages prior to the departure of RU2007, which outbreaks led to the deaths of numerous people. There had also been an outbreak of ARI/ILI on board RU2006, which, as I have found at [80] above (see also items (7) and (8) at [122]), further increased the risk of coronavirus on board RU2007.
590 In those circumstances, although the probability of harm was not such as to be an inevitability, the risk and its grave consequences were nonetheless inherently likely to materialise unless the respondents took precautions against the materialisation of that risk. Given the probability and seriousness of harm, the standard of care imposed upon the respondents could not have been anything other than high. The respondents admit that the factors relevant to determining their standard of care include the fact that they are specialists in providing passenger cruises that employed medical professionals on board the vessel, and that they employed medical staff who had specialised knowledge tailored to their business operations in which outbreaks of various viruses were a constant risk.
591 Finally, with respect to the social utility of cruising, Mrs Karpik submits that there is no societal imperative for recreational passenger cruises to operate. Although the respondents make no submission against it or otherwise directly address s 5B(2)(d), they do refer to the position of other venues analogous to cruise lines and providers of mass transit. It is sufficient to observe that almost all of those other examples, such as prisons, food production venues, worker dormitories, airplanes, buses and trains, are either essential or significant for society to function. The same cannot be said for pleasure cruising, as illustrated by the respondents’ own suspension of cruising a few days after the commencement of the voyage in question and the Commonwealth Government’s effective ban on international cruising a few days after that.
592 It will be recalled that Mrs Karpik says that the reasonable precautions that a person in the respondents’ position would have taken are the following:
(1) cancel the cruise;
(a) warn passengers that the risk of contracting COVID-19 on the cruise was heightened as compared to the community generally and to cruise ships generally;
(b) screen passengers and crew with relevant symptoms and not permit travellers with such symptoms to board regardless of what countries they had recently travelled from or through;
(c) reduce the number of passengers on board and take steps to ensure that appropriate physical distancing was observed;
(d) isolate guests and crew members with relevant symptoms for 14 days and isolate their roommates for 14 days in separate cabins;
(e) maintain sufficient medical supplies on board, and in particular face masks so that medical staff, symptomatic passengers and their close contacts could be provided with face masks;
(f) keep up-to-date with and implement all relevant guidelines and protocols; and
(g) consistent with those guidelines, isolate and quarantine passengers and crew who were experiencing symptoms that were consistent with COVID-19; or
(3) further alternatively, warn passengers that the risk of contracting COVID-19 on the cruise was heightened as compared to the community generally and to cruise ships generally and that the reasonable precautions set out in (2)(b)-(g) could or would not be implemented.
593 In order to determine whether, in the circumstances, a reasonable person in the position of the respondents would have taken each of the precautions Mrs Karpik alleges the respondents ought to have taken, the burden of taking each of the above alleged reasonable precautions will need to be considered (s 5B(2)(c)) and weighed against the fact that grave harm was probable.
594 It will be observed that measure (2)(g) flows from (2)(f), and that (2)(d) and (2)(g) are essentially the same. They can accordingly be considered together.
595 Mrs Karpik’s primary case on breach is that a reasonable person in the position of the respondents would have cancelled RU2007. The remaining alleged breaches are argued in the alternative. It is therefore appropriate to consider the cancellation case first.
596 Mrs Karpik submits that it is obvious that a reasonable person in the position of the respondents would have cancelled the cruise. As mentioned, the respondents had allowed passengers to cancel their cruises departing on and from 9 March 2020, the very next day, without penalty and on 13 March 2020, five days after the departure of RU2007, they decided to suspend all cruising worldwide. The respondents were also apparently prepared to cancel RU2007 with a full refund if one positive COVID-19 case had been found on RU2006. Mrs Karpik relies upon these decisions and submits that the fact that the respondents made the decision to suspend cruising only five days later is evidence of how un-burdensome it would have been to cancel the voyage on 8 March 2020. She says that, in circumstances where there had not been any intervening event in the meantime, a reasonable person in the position of the respondents would have made that same decision well before 8 March 2020.
597 In relying on subsequent action taken by the respondents, she says that, although CLA s 5C(c) provides that:
the subsequent taking of action that would (had the action been taken earlier) have avoided a risk of harm does not of itself give rise to or affect liability in respect of the risk and does not of itself constitute an admission of liability in connection with the risk[,]
the subsequent taking of action is nonetheless relevant as evidence of the practicability of that action. She says that subsequent taking of action is relevant to there being a want of any burden of cancelling the cruise on 8 March 2020 in particular because the respondents called no witnesses to give evidence about how burdensome that course of action would have been. She cites in that respect Caledonian Collieries Ltd v Speirs [1957] HCA 14; 97 CLR 202 at 224 and Kuhl at [38].
598 The respondents submit that, on the basis of community practices and expectations, and information available as at 8 March 2020, it was not unreasonable to proceed with the voyage. The practices, expectations and information to which the respondents refer may be summarised as follows:
(1) In none of the guidelines and protocols that had been published by the CDC, WHO, and Commonwealth and NSW Government bodies was the prospect of cancelling cruise ship voyages canvassed. The respondents say that each of them implicitly assumed the ongoing operation of the recreational cruise industry and were made (whether with or without industry consultation) with the intention of facilitating its ongoing operation during the pandemic. None of them identified a process whereby ships would be recommended or compelled to cancel particular voyages depending on the factors that pertained to a particular ship. They say that, importantly, each of those bodies or authorities would have been cognisant of the Diamond Princess outbreak which, by 20 February 2020, had over 600 confirmed cases of COVID-19.
(2) The Commonwealth Government did not use the powers under the Biosecurity Act 2015 (Cth) to regulate the operation of cruise ships until 18 March 2020. They say that there was no suggestion as at 8 March 2020 that the Commonwealth intended to exercise those powers.
(3) They say that their screening procedures, which adopted the WHO and CDC recommendations then published, were reasonable. For reasons to which I will come in section F.4.4 below, I disagree with that characterisation.
(4) They say that the heightened risk of COVID-19 on RU2007 has not been established. I have already rejected that contention at [80] above.
(5) With respect to the outbreak on the Grand Princess, they say they knew of only 21 cases by 7 March 2020 (8:00am on 8 March 2020 AEDT). The full extent of the outbreak was not known until much later and only after RU2007 had departed. They submit therefore that the outbreak on the Grand Princess cannot justify a submission that the voyage ought to have been cancelled on or prior to 8 March 2020.
(6) Finally, they say that any breach of duty by failing to cancel would be a duty that applied to all other similar premises and providers of mass transport. They say, for example, that on 6 March 2020, the Prime Minister and Treasurer were actively encouraging people to attend the final of the Women’s World Cup at the Melbourne Cricket Ground, which took place on 8 March 2020 with a crowd of 86,174 people. For reasons similar to those which I have given at [120], [558] and [591] above, I reject that submission. The example given of an event at a sports stadium, taking place in the open air and for a limited period of time where an attendee may elect to leave at any time, is not at all analogous to being a passenger on a multi-day cruise voyage. It is unhelpful to enter into a debate about whether or to what extent the judgement of the Prime Minister and the Treasurer could or should be taken as a benchmark of reasonableness.
599 From that summary, it can be seen that (1), (2) and (5) remain to be addressed. Frustratingly, none of the respondents’ submissions or evidence is directed at the burden of taking the precaution of cancelling the voyage. I will return to that issue.
600 In relation to (1), I accept that the fact that various guidelines did not explicitly envisage that any particular voyage should be cancelled is a relevant factor to take into account. It does not, however, take the respondents very far. Suppose that the respondents had discovered, during the turnaround of the vessel, that a number of crew on board had contracted COVID-19. It could not seriously be maintained that, because those guidelines did not envisage cancellation, the respondents ought not to have cancelled the following voyage or that the fact that those guidelines did not consider what ought to be done in such a circumstance would be a factor that weighed against cancellation of the following voyage. In any event, the point sought to be made is undermined by the fact that the respondents planned to cancel RU2007 if one positive COVID-19 test was returned from RU2006. Clearly, they had contemplated that cancellation would be necessary in circumstances almost identical to the circumstances actually known to them on 8 March, the difference being one positive COVID-19 test result.
601 Item (2) goes nowhere. The action taken on 18 March 2020 (although announced by the Prime Minister on 15 March 2020) was the promulgation of the Biosecurity (Human Biosecurity Emergency) (Human Coronavirus with Pandemic Potential) (Emergency Requirements) Determination 2020, s 5 of which banned the entry of international cruise ships into an Australian port. By s 4, “international cruise ship” was defined as a foreign vessel that, relevantly, “is on a voyage from a port outside Australian territory.” As explained in the Explanatory Statement to that Determination, if it were not already self-evident, the purpose of the Determination was to “prevent or control the entry, emergence, establishment or spread of COVID-19 in Australian territory.” That is quite a different purpose to that to which the duty imposed upon the respondents is directed, namely the protection of the Australian public at large rather than passengers on board a cruise ship. Indeed, the Determination did not ban cruise ships from operating domestically. In those circumstances, it does not appear to me to be relevant whether and when the Commonwealth determined that international cruise ships should be prevented from entering Australian ports.
602 In relation to (5), I accept that as at 8 March 2020, the full extent of the Grand Princess outbreak was not known. But, as I have found in section B.5.1(2) above, material facts about the outbreak were known. They included that nearly 50% of people presenting with ILI subsequently tested positive for COVID-19, that a single index case led to scores of people getting sick, and one even dying, across two cruises, and that the likely transmission mechanism from one cruise to the next was infected crew.
603 Returning now to the burden of cancelling the voyage, Mrs Karpik as mentioned relies upon Caledonian Collieries at 224 and Kuhl at [38].
604 Caledonian Collieries was an action by a widow in relation to the death of her husband caused by a collision between his vehicle and a train at a level crossing. It was alleged that the appellants were negligent in failing to have installed catch points on the railway line, which would have prevented the tragedy by derailing the train. It was relevantly held (at 224 per Dixon CJ, McTiernan, Kitto and Taylor JJ) that although the installation of catch points subsequent to the incident could not be regarded as an admission, it nevertheless had significance to the practicability of taking that action earlier. It was also held (at 225) that although derailment was a drastic measure, when the danger to be guarded against is a level crossing collision, it was open to the jury to find that drastic measures are within the limits of reasonable care.
605 Kuhl was an action by a worker who suffered severe injuries when his arm was sucked into an industrial vacuum. One of the pleaded breaches was that the respondent was negligent in failing to install a break box near the head of the vacuum hose. A break box had been installed soon after the incident and the respondent adduced no evidence to suggest that implementation of the break box would have been burdensome or impractical. Both the majority (at [94] per Heydon, Crennan and Bell JJ) and the dissentients (at [38] per French CJ and Gummow J) referred to the judgment of Gibbs J in Nelson v John Lysaght (Australia) Ltd [1975] HCA 9; 132 CLR 201 at 214-215, where the following was said:
The onus of proving that it was unreasonable not to take the precaution, of course, lay on the [plaintiff]. However, when the [defendant], which must have had full knowledge of the nature, cost and practical consequences of the new installation, gave no evidence, and by its counsel asked no questions, to suggest that it was inordinately expensive or in any other way disadvantageous, the jury was entitled to infer at the very least that the advantages of the method which the [defendant] has since adopted were not outweighed by any disadvantages.
606 Those cases make it plain that the fact that the respondents in the present case adduced no evidence of, and by their counsel asked no questions about, the burden and practicability of cancellation is relevant in that it is open to infer that any burden that would have attended the cancelling of the cruise is not outweighed by the probability of grave harm. Whether that inference should be drawn is an altogether different question.
607 In my view, the fact that the respondents decided to suspend cruising worldwide merely five days later is relevant, and it shows that the burden of cancelling the cruise would not have been intolerable; it was clearly within the scope of available options. Although cancellation is a drastic measure, to cancel one cruise at the last minute is a very minor measure compared to suspending all cruising worldwide. It is also to be recalled that the respondents later refunded all the passengers on RU2007 in full, so the ultimate outcome was comparatively financially worse for the respondents. That is, the respondents incurred expenses that even a last-minute cancellation would have saved – bunker fuel being an obvious one as well as non-perishable food and beverages – and lost all income for the cruise.
608 As against that must be weighed the probability of grave harm. What the respondents as at 8 March 2020 knew of the likelihood of that probability eventuating on RU2007, as compared to other voyages, was as follows. First, although the outbreak on the Grand Princess was then taking place, the true extent of it was not yet known. Nonetheless, the respondents ought to have known that their procedures for screening of passengers and crew were deficient. Secondly, there was a heightened risk on board the Ruby Princess given the outbreak of ARI/ILI on board voyage RU2006. That was a lesson that was already clear from the Grand Princess experience.
609 In those circumstances, in my view, the reasonable cruise operator would have cancelled RU2007 on 8 March 2020. The respondents were in breach of their duty of care to the passengers, including Mr and Mrs Karpik, in not doing so.
610 That said, there is an interaction between cancellation and other protective measures because if sufficient other measures had been taken, cancellation would not have been necessary. However, for whatever reason, protective measures that could have significantly reduced the risk of infection on RU2007 were not taken – I will go on to consider some of these measures shortly. Since they were not taken, the voyage should have been cancelled.
F.4.3 Warn passengers of coronavirus risk
611 As an alternative to her cancellation case, Mrs Karpik contends that a reasonable person in the position of the respondents would have warned her that:
(1) the risk of contracting COVID-19 on board the Ruby Princess was heightened compared to the community generally;
(2) the risk of contracting COVID-19 on board the Ruby Princess was heightened compared to cruise ships generally; and/or
(3) the respondents either would not or could not implement the pre- and post-boarding precautions she alleges they ought to have taken.
612 As mentioned, the third of the warnings pressed for above is argued in the further alternative – ie, if the respondents were not in breach by failing to implement one or more of the precautions, then they ought to have warned Mrs Karpik that they could not or would not implement that precaution. As will be seen, I find the respondents to have been in breach of their duty of care in certain respects with regard to pre-embarkation screening and post-embarkation precautions with the result that I do not find it profitable to deal with the third contended-for duty to warn.
613 The respondents rely on CLA s 5H. It will be recalled that that section provides that a defendant does not owe a duty of care to warn of an “obvious risk” to the plaintiff. It will also be recalled that I have decided that s 5H of the CLA is not picked up by ACL s 275, with the consequence that s 5H only applies to Mrs Karpik’s common law negligence claim: see section D.4 above. Nonetheless, even in the absence of the statutory provision, the obviousness of a risk is relevant to whether there is a duty to warn: see Romeo v Conservation Commission (NT) [1998] HCA 5; 192 CLR 431 at [25] per Brennan CJ, [56] per Toohey and Gummow JJ, [123] per Kirby J and [157] per Hayne J. The position with respect to the s 60 claim and the common law negligence claim is therefore much the same.
614 The meaning of “obvious risk” is defined by s 5F. That section provides:
(1) For the purposes of this Division, an obvious risk to a person who suffers harm is a risk that, in the circumstances, would have been obvious to a reasonable person in the position of that person.
(2) Obvious risks include risks that are patent or a matter of common knowledge.
(3) A risk of something occurring can be an obvious risk even though it has a low probability of occurring.
(4) A risk can be an obvious risk even if the risk (or a condition or circumstance that gives rise to the risk) is not prominent, conspicuous or physically observable.
615 The respondents contend that the following risks are obvious risks within the meaning of s 5F:
(1) the risk that a passenger on the voyage might contract a contagious disease from another passenger; and
(2) the risk that the voyage might be shortened or altered to comply with the policies and lawful directions of government authorities.
616 However, as Mrs Karpik points out, she does not allege that she ought to have been warned of those risks. Her case on the duty to warn, which has not narrowed or changed from the pleadings, is that the respondents ought to have warned of the heightened risk on the Ruby Princess when compared to both the community generally and also to other cruise ships.
617 In my view, the heightened risk of coronavirus on board cruise ships when compared to the community generally was an obvious risk notwithstanding that the respondents deny that there is such a heightened risk at all (see [110] above). Various outbreaks had been widely reported in the news, in particular that of the Diamond Princess. Various health bodies, including the CDC, WHO, and bodies of the NSW and Commonwealth Governments each published their own guidelines and protocols specific to the cruise line industry. The differing treatment of cruise lines was not based on any specialised knowledge but rather on what may be described as general knowledge which anyone could obtain simply by turning their mind to what occurs on board a typical cruise voyage: see, for example, the features identified by the CDC No Sail Order as set out at [123] above. Indeed, so obvious was the heightened risk that Mrs Karpik’s son-in-law, who had no reported experience on cruise ships, had expressed the view that cruise ships are “petri dishes” for disease.
618 In those circumstances, I find that the respondents were not negligent by reason of failing to warn of the heightened risk on board the Ruby Princess when compared to the community generally. That conclusion applies both to the common law negligence claim and under the ACL s 60 claim.
619 In respect of the remaining alleged failure to warn, the respondents also contend that there was no duty to warn because the conduct required to discharge that duty would be coextensive with s 18 of the ACL. They rely in that respect upon the judgment of Gaudron J in Graham Barclay Oysters.
620 In that case, Gaudron J considered the relationship between the then TPA and the law of negligence. Her Honour considered that where the supply of a product without warning as to its possible dangers or defects does not constitute misleading or deceptive conduct contrary to s 52(1) of the TPA (as was held by the trial judge in that case), it would be difficult to conceive that, nonetheless, the general law would impose a duty to warn of those dangers or defects. Her Honour was there concerned that the law of negligence would impose more onerous obligations than the requirements of the TPA.
621 It is sufficient for present purposes to make two observations. First, that reasoning has not been followed or cited since and none of the other judgments express the same concern. Secondly, the reasons expressed for Gaudron J’s concern are inapplicable to the ACL, for the ACL now contains, whereas the TPA did not, a statutory guarantee of due care and skill, the discharge of which, as the respondents accept, is coextensive with the common law of negligence. That is to say, there is no issue of the common law imposing more onerous obligations than those that the ACL imposes. And, even if the law of negligence does impose more onerous obligations, for reasons similar to those given at [550] above, I reject that that would thereby be a reason not to find a breach by reason of a failure to warn.
622 The question nonetheless remains whether a reasonable person in the position of the respondents would have warned of the heightened risk on the Ruby Princess when compared to other cruise ships. The respondents rely on Modbury Triangle and submit that the common law does not ordinarily impose liability for omissions. So much may be accepted. Its relevance however to the present case on breach is far from clear; Modbury Triangle is distinguishable on at least two bases: the first is that there was no duty in respect of the relevant risk of harm in that case and the second is that, even if there were a duty, the occupier had no knowledge of the particular risk. See [533]-[545] above.
623 The position of the respondents is analogous to that of an occupier. In that respect, it has long been held that occupiers owe a duty to warn licensees of the existence of hidden dangers known to the occupiers that a reasonable person could not anticipate or suspect: see, eg, Lipman v Clendinnen [1932] HCA 24; 46 CLR 550. In Hoyts Pty Ltd v Burns [2003] HCA 61; 201 ALR 470 at [70], Kirby J explained the social considerations that the law is seeking to advance by requiring warnings in certain circumstances:
From the point of view of the occupier, it is seeking to encourage attention to, and consideration of, accident prevention by the party ordinarily with the superior means and interest to “keep abreast of publicly available or expert knowledge concerning the risks of injury in such activities.” From the point of view of the entrant, the law is seeking to uphold that person’s entitlement to make informed choices concerning the kind of risks in which he or she will participate on the basis of knowledge provided by the occupier. At the heart of the latter objective lies a conception of respect for individual autonomy that probably has its source in notions of fundamental human rights and human dignity.
624 The heightened risk of contracting COVID-19 on board the Ruby Princess when compared to other cruise ships is analogous to a hidden danger. Unlike the heightened risk on cruise ships generally, the risk on board the Ruby Princess was further heightened by reason of the outbreak of ARI/ILI on board RU2006, an outbreak of which Mrs Karpik was not aware. As mentioned, the respondents knew that a person could be infectious with mild symptoms or with no symptoms and that, of the 366 passengers who presented for screening, only nine were tested for COVID-19 by NSW Health. Despite none of those nine returning a positive test, there was nonetheless a substantial risk that there was a COVID-19 case on board RU2006. Indeed, the respondents had prepared for that eventuality by preparing to cancel the next cruise if one of those nine returned a positive test.
625 In my view, Mrs Karpik ought to have been warned of the heightened risk of COVID-19 on board RU2007 because of there being an outbreak of ARI/ILI on board the previous voyage, most of the crew remaining on board for the next voyage and that only nine of the 366 individuals that presented themselves in response to a call for screening were tested for COVID-19. That information was vital to understanding that there was a heightened risk of COVID-19 on board the Ruby Princess. The respondents had access to that information, but the passengers did not. Mrs Karpik was entitled to make an informed choice regarding whether or not she accepted that heightened risk before embarking on a 13-day journey, mostly in the confines of the vessel. There would have been no burden to the respondents in affording her that choice.
F.4.4 Screening of passengers and crew
626 Mrs Karpik says that the principal measure that the respondents introduced in response to the COVID-19 risk was pre-embarkation screening, which screening she submits was woefully inadequate. As mentioned, that screening involved requiring passengers to declare whether they had travelled from or through particular countries or been in contact with a suspected or confirmed case of COVID-19. She submits that the respondents knew this to be ineffective because a similar screening process was in force and had been undertaken in respect of the Grand Princess.
627 She submits that a reasonable person in the respondents’ position would, at the very least, have included in the Traveller’s Health Declaration a question asking all prospective passengers to declare whether or not they exhibited any symptoms (ie, a fever, cough or difficulty breathing) and all travellers who answered “yes” should have been denied boarding. She further says that the remaining passengers should have been medically screened for symptoms consistent with COVID-19, by which I understand her to mean to have at least their temperatures checked, in small groups throughout the day. She says that such measures would not have been particularly onerous.
628 The respondents contend that the pre-boarding screening was reasonably appropriate to address the risk of COVID-19 in the circumstances that prevailed on 8 March 2020 when boarding occurred. The respondents contend that their policy of automatically denying boarding to passengers who had travelled through China, Hong Kong, Macau, South Korea or Iran was more onerous than what was recommended by the CDC Guidance for Ships (which recommended that boarding be denied to passengers or crew “suspected to have COVID-19 infection based on signs and symptoms plus travel history in China or other known exposure at the time of embarkation”) or the WHO Ship Interim Guidance (which recommended deferred or rescheduled boarding of any “close contact[s]” of persons with COVID-19). [CAU.001.107.0003; PUB.005.001.0325]
629 The respondents submit that it may be inferred from the revisions to the Instructional Notice HEA/01/2020 that the respondents monitored and took into account CDC-issued Travel Warnings in designing and updating their pre-boarding screening process. Further, the respondents submit that the pre-boarding screening process, in screening for fever and respiratory symptoms dependent on travel history, was consistent with the definition of a “suspect case” of COVID-19 that prevailed at the time, such as that contained within the Communicable Diseases Network Australia’s (CDNA, a body of the Commonwealth Department of Health) National Guidelines for Public Health Units dated 6 March 2020, which defined a “suspect case” as a patient who satisfies “epidemiological and clinical criteria” (emphasis added), being travel history or close contact with a confirmed case and fever or respiratory symptoms. [PUB.006.001.0020]
630 The respondents also reiterate that the pre-boarding communications sent to passengers contained a notice advising them that they would be required to submit to pre-boarding screening and warning that false declarations would result in disembarkation and potential legal consequences. [LAY_SKA.001.001.0273]
631 It is to be observed that the respondents’ primary case is that they adhered to the CDC and WHO’s guidelines and protocols, and adopted definitions of COVID-19 suspect cases consistently with the advice of various health bodies. Indeed, they submit that Revision 3 (and, therefore, Revision 5) was more onerous than at least the WHO Ship Interim Guidance. There are two reasons why reliance on adherence to those guidelines and protocols fails.
632 First, although adherence to relevant guidelines and protocols is a relevant fact to consider in determining whether a defendant breached their duty of care, it remains the case at common law (cf, in the case of professional negligence, CLA s 5O) that the ultimate question is not whether a defendant adhered to industry or relevant guidelines and protocols but whether their conduct conforms to the standard of reasonable care. As observed by the Full Court of the Supreme Court of Victoria in Thompson v Johnson and Johnson Pty Ltd [1991] 2 VR 449 at 494, the views of other bodies are:
not determinative of the question of reasonable care, for to accept that proposition would permit the respondents to abrogate the duty of reasonable care owed by them. It is not the response of such [bodies] which determines whether a person in the position of the respondents is or is not negligent. That is for the courts to decide.
See also F v R (1983) 33 SASR 189 at 194 per King CJ, as endorsed by the High Court in Rogers v Whitaker [1992] HCA 58; 175 CLR 479 at 488-489.
633 Secondly, and in any event, adherence to the various guidelines, protocols and definitions failed to prevent the outbreak of COVID-19 on board the Grand Princess. Clearly, they had proven to be ineffective and, by 7 March 2020 at the latest, the respondents knew that to be so. [PCL.001.003.6200] It may readily be inferred that the ineffectiveness of screening in accordance with those guidelines is what, in part, gave rise to the view expressed by Sture Myrmell, President of Carnival Australia, on 11 March 2020 that implementing temperature screening was a number one priority. As will be recalled, Mr Myrmell also expressed in the same email that “we are way behind”, having spoken about such screening for four weeks by that time.
634 The respondents were “way behind” not only in accordance with their own internal protocol, but also by reference to what other cruise lines were doing. In respect of their internal protocol, it will be recalled that the recognition amongst the respondents that more stringent screening processes were required was formalised in protocols from as early as 27 February 2020, being the date on which the respondents’ Enhanced Cleaning Protocols providing for, inter alia, thermal screening was issued.
635 In respect of what other cruise lines were doing, on 3 March 2020, the CLIA advised its members (including the respondents) that its Global Executive Committee wanted to implement a policy of temperature screening for all persons at embarkation (ie, passengers, crew and other visitors). Members were asked to indicate by 5 March 2020 when they would be able to implement such a policy. That deadline for response was subsequently accelerated to 4 March 2020. Members were asked which of them could or could not implement global temperature screening by 5, 6 or 7 March. [PCL.002.032.2207 pp 2, 4]
636 On 4 March 2020, Virgin Voyages replied saying that it was already compliant with the proposed policy. On 5 March 2020, MSC replied that it already had “thermal temperature controls” in place for all embarking people (guests, crewmembers, visitors, technicians, port pilots, etc). [PCL.002.032.2207 p 1]
637 The failure of the pre-screening process then in place to adequately detect potential cases of COVID-19 ought to have given any reasonable person in the respondents’ position pause to reassess their procedures by, for example, accelerating the rollout of thermal screening. However, rather than continue to require temperature screening of prospective passengers, the amended Enhanced Public Health Protocols issued for the boarding of RU2007 instead deleted that requirement.
638 The respondents called no witness who could explain the amendment to the Protocols for the departure of RU2007. The documentary evidence reveals that the earliest action that appears to have been taken in accordance with the protocol was 6 March 2020, on which date Carnival announced internally that it would be piloting thermal screening of all guests and visitors embarking on its ships in North America “home ports” from the next day and that a number of agents would utilise a hand-held non-contact thermometer. It was said that any guest or visitor identified with elevated temperatures would be further evaluated by a member of the onboard medical team, and that that process would be in addition to the guest screening initiative then in place utilising the Traveller’s Health Questionnaire. It was said to the “AUS Team”, which I take to be Carnival Australia, that efforts would be made to source infrared thermometer units in Australia and that further information would be forthcoming. [CAU.001.039.8328 p 6]
639 On 7 March 2020, Milly Martin, the Senior Director of Guest Port Services for Carnival, reported that temperature checks “at all ports rolled out thus far are running very smoothly; with no delays or issues.” Also on 7 March, Dr Tarling told a press briefing about the Grand Princess that because the index case on that vessel had likely contracted the virus in California and not in one of the countries identified as having widespread community transmission (being the countries on which screening of passengers had been based), PCL was henceforth “looking for any form of fever illness anywhere, on any person coming onboard.” Dr Tarling explained that temperature checks were being rolled out by PCL world-wide as equipment was acquired, and that that was in accordance with an agreed CLIA protocol. [PCL.001.003.6200]
640 On 9 March 2020, Ms Martin reported that all ports had rolled out the temperature checks successfully at embarkation, except Australia which was still awaiting receipt of the infrared thermometer units. The following day, Ms Martin reported that the units for Australia had been shipped but that they would not arrive until 14 March and that temperature checks would be in place by 16 March.
641 On 11 March 2020, Peter Little, Senior Vice President, Guest Experience of P&O Australia wrote to Mr Myrmell, copying in Mr Goodman (Carnival Australia’s Supply Chain Director), providing delivery dates of thermometers to each of the vessels in the HA Group in Australia or New Zealand. Mr Myrmell replied stating that he also wanted thermal cameras. It was explained by Mr Goodman in further correspondence that he was still working with a vendor in that regard. [CAU.001.039.8328; PCL.001.004.9490]
642 I make the following observations arising from the above.
643 First, although there was a protocol of thermal screening in place as at 27 February 2020, the evidence does not reveal what action, if any, was taken by the respondents to implement the protocol until 6 March 2020. By that time, the respondents’ competitors had already implemented such screening.
644 Secondly, by 8 March 2020 the thermal screening policy was only implemented in North American home ports.
645 Thirdly, the respondents’ internal communications acknowledge that they ought to have implemented temperature screening much earlier.
646 Fourthly, as at 6 March 2020, the respondents were attempting to source hand-held infrared thermometers locally in Australia, but there is no evidence as to what steps were taken locally and whether there were any supply chain issues sourcing similar such units locally. The respondents, having full knowledge of the nature, cost and impediments of sourcing similar such units locally for deployment on RU2007, gave no evidence to suggest that such steps would have been burdensome or impractical. Although the burden of proof is on the applicant, the evidential burden on this issue is on the respondents given that their protocol required thermal screening and only they could know what steps were taken and what obstacles were encountered. They have elected not to adduce such evidence, from which I infer that it would not have been helpful to their case. I therefore infer that purchasing thermometers and using them to screen passengers embarking on RU2007 would not have been unduly burdensome.
647 Turning now to the other aspect of pre-embarkation screening that Mrs Karpik alleges was wanting, she submits that a reasonable person in the respondents’ position would have included a question on the Traveller’s Health Declaration asking prospective passengers to declare whether they exhibited any symptoms (ie, a fever, cough or difficulty breathing) and that any passenger who answered “yes” ought to have been denied boarding. It will be recalled that, in accordance with Revision 5, only passengers who answered “yes” to having travelled from or through certain countries or had been in contact with a suspected case of COVID-19 were required to declare any symptoms.
648 I have no hesitation in finding that such a requirement would not have been burdensome or impractical, requiring as it would simply the re-wording and re-printing of the relevant forms. Indeed, in the Enhanced Public Health Protocols distributed for RU2007, one of the requirements was “respiratory symptom screening, including screening for contact with a suspected or confirmed case of coronavirus” yet, on the evidence, respiratory symptom screening was only undertaken in respect of those passengers who declared that they had travelled from or transited through the countries listed in Question 3.
649 In the circumstances, I find that the respondents breached their duty of care by failing to provide for adequate screening of passengers and crew. A reasonable person in the respondents’ position would have implemented temperature screening by 8 March 2020, and would have asked passengers seeking to board the Ruby Princess for RU2007 whether they exhibited any symptoms of COVID-19 and denied boarding to any passenger who answered “yes.” That is because the burden of taking those precautions can only be described as slight when weighed against the very serious harm that was probable if those precautions were not taken. That such action was reasonable is supported by the fact that the respondents themselves had implemented temperature screening in their North American ports and numerous competitors had reported that they had implemented temperature screening across the board. And, as the respondents well knew, the pre-boarding screening procedures that had hitherto been followed in line with various health body guidelines, protocols and definitions had been proven to be ineffective.
F.4.5 Enforce physical distancing
650 Mrs Karpik contends that the respondents were further in breach by failing to implement and advise passengers to practise physical distancing on board RU2007. In accordance with the FASOC, implementation is said to entail limiting the number of people within all parts of the ship so as to allow for physical distancing (ie, 1.5 metres per person) and closing such parts which could not permit it.
651 As mentioned in section B.6.7 above, save for cancelling the Ultimate Ship Tour and Galley Tour, there is no evidence that any meaningful physical distancing was encouraged or implemented. Indeed, even after the Determination banning international cruise ships from entering Australian ports was in effect, on 16 March 2020, activities continued as usual on board, including various dancing, exercise, movie screening, karaoke and live music events. [PCL.001.001.7591] And, even after the Prime Minister announced a ban on non-essential indoor gatherings of greater than 100 people on 18 March 2020, such non-essential events continued on the Ruby Princess with “Dancing through the Decades” held at 8:15pm and “Farewell Dance Party with High Tide Party Band” at 10:15pm that night. [PCL.001.001.7605]
652 The respondents admit that there were no physical distancing measures introduced or encouraged, and that passengers were encouraged to attend activities. They deny, however, that they knew or ought to have known that the risk of contracting COVID-19 could have been avoided or reduced by implementing physical distancing. They submit that the concept of physical distancing as it is now understood – ie, maintaining 1.5 metres from other people (or, alternatively, 6 feet in the US) – was not a recommended measure at the time and was not a measure that had been implemented in respect of previous outbreaks of novel coronaviruses. They say that there were no recommendations directed at cruise ships or the general public to engage in such a practice as at 8 March 2020 or at any time prior to 18 March 2020. They urge that caution needs to be taken in referring to documents that pre-date 8 March 2020 because references in such documents to physical or social distancing were not references to the 1.5 metre rule.
653 I do not accept that the respondents did not know either of physical distancing or of its effectiveness as at 8 March 2020. As a preliminary point, any suggestion that the practice of staying away from people who are sick is a new phenomenon, or newly discovered to be an effective measure, is obviously wrong. Indeed, as the respondents themselves submit:
The simple, informal practices by which humans can reduce the risk of contracting an infectious disease are very old. There are records of quarantine, physical distancing and masks dating at least as far back as the bubonic plague in the 14th century.
(Emphasis added.)
654 In any event, the CDC’s “Guidance for Cruise Ships on Influenza-Like Illness (ILI) Management” (revision dated 22 August 2016) (CDC ILI Guidance 2016) recommends that passengers and crew with ILI should be encouraged to remain at least 6 feet from other people. [PUB.010.001.0001 p 2]
655 As mentioned, the CDC COVID Ship Guidance (revised on 18 February 2020) provided that the primary mode of COVID-19 virus transmission was believed to be through respiratory droplets that are spread from an infected person through coughing or sneezing to a susceptible close contact within about 6 feet. On the basis of communications published by the CDC and WHO, Professor Wilder-Smith opined in Joint Report 9 that prior to the departure of the voyage it was known that respiratory droplet transmission was the “predominant mode of transmission.” Professor Paterson accepted that it was known that respiratory droplet transmission was “an important mode of transmission.” Further, the CDC COVID Ship Guidance recommended that crew who have contact with passengers with fever or ARI maintain a distance of 6 feet from the sick person while interviewing, escorting, or providing other assistance.
656 On 5 March 2020, Joshua Leibowitz, Chief Strategy Officer of Carnival, sent an email addressed to Dr Grant Tarling, among others, circulating the latest revision of CDC’s general COVID-19 Guidance (ie, guidance that was not directed specifically at cruise operators). In that Guidance, social distancing was defined as: [PCL.002.031.7071]
remaining out of congregate settings, avoiding local public transportation (eg, bus, subway, taxi, ride share), and maintaining distance (approximately 6 feet or 2 meters) from others. If social distancing is recommended, presence in congregate settings or use of local public transportation should only occur with approval of local or state health authorities.
The Guidance records that a revision was issued on 8 February 2020 updating the definition of the term “social distancing.” No update to the definition is recorded for the revision dated 5 March 2020. It may therefore be inferred that the definition quoted above was adopted on 8 February 2020. The same Guidance also provided that those who had no identifiable risk of COVID-19 should, if experiencing symptoms consistent with COVID-19, practice social distancing.
657 As mentioned, on 7 March 2020, the respondents conducted a conference call with the media concerning the then developing events on board the Grand Princess. Those from the respondents who were present were Arnold Donald, President and Chief Executive Officer of Carnival, Jan Swartz, President of Princess and Carnival Australia, and Dr Grant Tarling. Ms Swartz stated that “we are taking our learnings from our operational response for Diamond Princess and implementing them immediately. These include immediately implementing safe social distancing ….” [PCL.001.003.6200 p 6] And Dr Tarling stated: [PCL.001.003.6200 p 26]
So, there are more enhanced measures going on at the moment around the vessel. As you know, we’ve taken more extreme measures for this current cruise because we’ve implemented initially the social distancing methods before we ask the guests to all remain in their cabins.
So social distancing was practiced, including asking guests to remain at least one feet away from their dining companions while this was going on. So, we tried to promote a lot of social distancing practices, prior to them all being asked to stay in their staterooms.
658 Later that evening, Jen Wright, Director of Trade Reservations at PCL, provided an updated Q&A for the Grand Princess coronavirus response, which included the following: [PCL.001.002.9453]
2. How are you handling this situation differently than Diamond Princess?
A. We’ve taken successful learnings from Diamond Princess and implemented them immediately. This includes:
Immediately implementing safe social distancing (6 feet)
Delivering prescription request forms
Increasing entertainment options
Increasing fresh air mix into the ventilation system in the staterooms
Working with CDC to determine fresh air breaks
659 Thus, regardless of whether there were any specific recommendations directed at cruise ships, the respondents said that they implemented physical distancing on board the Grand Princess prior to 8 March 2020. On that basis, I infer that they knew that physical distancing was an important measure to reduce transmission of the virus. The respondents may have taken what they learnt from the Diamond Princess and applied that to the Grand Princess, but they did not take what they learnt from the Diamond Princess and the Grand Princess and apply that to the Ruby Princess.
660 The respondents further submit that, in any event, physical distancing would not have had the effect of eliminating or materially reducing the risk of transmission on a cruise ship. They say that Mrs Karpik is obliged as a matter of pleading and as a matter of law to demonstrate that implementing and encouraging physical distancing could have avoided the risk of transmission of COVID-19 on the vessel.
661 Insofar as the submission concerns Mrs Karpik needing to prove that physical distancing would have eliminated or, to similar effect, avoided the risk of contracting COVID-19, Mrs Karpik has not pleaded that and the respondents have not cited any authority in support of the submission that she is required to establish such a fact. Indeed, authority is to the contrary; the law of negligence imposes a duty only to take reasonable care. As Gleeson CJ explained in Swain v Waverley Municipal Council [2005] HCA 4; 220 CLR 517 at [5]:
… the standard of conduct necessary to discharge the duty is usually expressed in terms of what would be expected of a reasonable person, both as to foresight of the possibility of harm, and as to taking precautions against such harm. Life is risky. People do not expect, and are not entitled to expect, to live in a risk-free environment. The measure of careful behaviour is reasonableness, not elimination of risk. Where people are subject to a duty of care, they are to some extent their neighbours’ keepers, but they are not their neighbours’ insurers.
662 Insofar as the submission concerns Mrs Karpik’s burden of establishing a factual matter alleged in the pleadings, I reject it. The respondents admitted in their defence that requesting passengers to engage in physical distancing and limiting passenger numbers on board the ship and in all parts of the ship to allow for physical distancing could have reduced the risk of passengers contracting COVID-19, although they deny that the risk could have been avoided. The FASOC pleads that those precautions could have avoided or reduced the risk of COVID-19. As the respondents have admitted that the risk could have been reduced, they have admitted one of the disjuncts.
663 It is important to recall that the respondents knew that coronavirus is highly contagious and potentially lethal, and that human-to-human transmission can occur via respiratory droplets (section B.4.4 above). It stands to reason, as explained by Professors Wilder-Smith and Paterson in Joint Report 9, that the highest concentrations of respiratory droplets are in close proximity to the exhaling person. Therefore, the highest risk of transmission is within 1.5 metres. On that basis, I accept that close and prolonged contact, lack of physical distancing, being indoors and in under-ventilated areas, and increased social interaction between different people through on-board activities, increases the risk of transmission. It follows that even aside from the respondents’ admission, it is established on the evidence – a point on which Professors Wilder-Smith and Paterson agree – that physical distancing as a measure to reduce proximity between people decreases the risk of transmission.
664 Finally, as with each of the precautions previously considered, the respondents adduced no evidence and advance no submissions directed to the burden of implementing physical distancing measures. As disclosed by their executives in the conference call on 7 March 2020, physical distancing on the Grand Princess was introduced “immediately.” I infer that introducing such measures on board the Ruby Princess would not have been burdensome.
665 In circumstances where the respondents knew that physical distancing was an effective measure to reduce the grave risk of COVID-19 and had in fact implemented physical distancing on board the Grand Princess, I find that the respondents were negligent in failing to encourage and implement physical distancing on board RU2007.
F.4.6 Monitor & implement relevant guidelines and protocols
(1) Quarantine and isolation as at 8 March 2020
666 The respondents adduced evidence that their policies and procedures were responsive to certain relevant guidelines and protocols concerning the identification and treatment of COVID-19. Revision 5 relevantly directed that CDC and WHO guidelines be regularly reviewed and followed. [CAU.001.040.7332] The respondents were also aware of the Enhanced NSW Cruise Procedures. As mentioned, there were two versions of those Procedures that pre-date the departure of the voyage: the first dated 22 February 2020 and the second dated 3 March 2020. They acknowledged receipt of the 22 February version by email to NSW Health on 26 February 2020 advising that “[o]verall, we are continuing to … adapt our processes to meet the requirements of the enhanced policy.” [CAU.001.040.6308] They were also aware of the 3 March version by 7 March 2020 at the latest. [PCL.001.005.6517]
667 I consider that a reasonable cruise operator in the position of the respondents would follow such guidelines to prevent, or at least minimise, the spread of COVID-19 and keep passengers safe. In early March 2020, there was great uncertainty about COVID-19 and the situation was developing fast. Even well-resourced cruise operators like the respondents would be in danger of failing to keep up with relevant developments in the state of knowledge about the virus and appropriate measures to guard against its spread unless they drew on the knowledge and resources of leading public health authorities.
668 The relevant question is therefore whether relevant guidelines and protocols were followed by the respondents with regard to quarantining and isolating passengers and crew who showed or reported relevant symptoms.
669 As ultimately advanced, Mrs Karpik submits that a reasonable person in the position of the respondents would have isolated guests and crew with symptoms consistent with COVID-19 for 14 days, and also roommates of those persons for 14 days, in a separate cabin in circumstances where the ship did not have sufficient face masks on board. Rather than isolating symptomatic passengers and their roommates, she says that the respondents informed symptomatic passengers and their roommates that there was no need for them to isolate and thereby breached their duty of care.
670 The respondents submit that each of the relevant bodies only recommended isolation in circumstances where a suspected case of COVID-19 had been identified. They say that the definition of a suspect case included both clinical (ie, symptoms) and epidemiological (ie, international travel or close contact) criteria. Accordingly, not every symptomatic passenger was a suspect case and, therefore, not every symptomatic passenger was required by the relevant guidelines to isolate.
671 The CDC ILI Guidance 2016 provides that passengers with ILI should remain isolated in their cabins or quarters, with the exception of clinic visits, until at least 24 hours after resolution of fever without the use of fever-reducing medications. It further provides that, while temporarily in common areas, passengers and crew with ILI should be encouraged to remain at least 6 feet from other people and either wear face masks or cover their mouths and noses with tissues. [PUB.010.001.0001 p 2]
672 The CDC COVID Ship Guidance relevantly included that passengers and crew who from their symptoms and risk of exposure were suspected of having COVID-19 should be isolated on board in single-occupancy cabins with the doors closed until their symptoms improved. It was also advised that medical follow-up should ideally take place in the isolated person’s cabin and that the sick person should wear a face mask before leaving their cabin.
673 The WHO Interim Ship Guidance contained recommendations for managing a “suspected case” of COVID-19. The Guidance provided, inter alia, that a suspect case was required to wear a medical mask, requesting that they follow cough and hand hygiene measures, isolating the suspect case in an isolation ward, cabin, room or quarters, with the door closed. A suspect case was defined, as the respondents rightly point out, by reference to clinical and epidemiological criteria, namely “a history of travel to or residence in China or in another country with established community transmission of COVID-19 disease during the 14 days prior to symptom onset.”
674 The Enhanced NSW Cruise Procedures that were initially issued on 22 February 2020 relevantly required that passengers “who may be infectious are appropriately isolated.” That procedure was listed under the heading “Procedures to identify and manage cases of respiratory infection” (emphasis added). [CAU.001.040.6314] The version dated 3 March 2020 clarified the isolation requirement as applying to passengers with ARI/ILI who may be infectious. It also provided that isolated passengers should be provided with alcohol hand rub and face masks and, if sharing a cabin, that their roommates be provided with the same materials and education on how to protect themselves. [PCL.001.005.6518]
675 Contrary to Mrs Karpik’s submissions, none of the guidelines required that asymptomatic roommates of any passenger with ARI/ILI also be isolated. Nor, in my view, did any of the relevant guidelines require that a passenger with either ARI or ILI be isolated in a single-occupancy cabin. The only guideline that required such a course was the CDC COVID Ship Guidance. That requirement applied to “suspect cases” of COVID-19. A suspect case was to be determined by “signs and symptoms plus travel history in China or other known exposure at the time of embarkation.” The single-occupancy isolation requirement therefore did not apply to all cases of ARI or ILI.
676 In relation to the 14-day duration, no such duration is mentioned in any of the guidelines. Instead, Mrs Karpik submits that that was the period of self-isolation that had hitherto been imposed by the Commonwealth Government for overseas arrivals from countries with large numbers of COVID-19 positive cases. As at 8 March 2020, those countries were China, Iran, and South Korea. She further says that a 14-day duration is consistent with the recommendation by the respondents’ own epidemiologist, Dennis Peyton Jr, who on 11 March 2020 advised all of the Senior Doctors on HA Group vessels, including Dr Ilse von Watzdorf, the Senior Physician on the Ruby Princess, that any passenger who had a travel history through countries listed in question 3 of the Traveller Health Declaration (ie, Italy, Japan, Singapore, Taiwan or Thailand) and subsequently develops respiratory symptoms should be isolated for at least 14 days. [PCL.002.001.1972]
677 In those circumstances, I find that a reasonable person in the position of the respondents would have isolated passengers who presented with ARI and ILI. Those passengers and their roommates would have been provided with alcohol hand rub and face masks to be used when moving about in common areas. Further, a reasonable person in the position of the respondents would have directed such persons to isolate until 24 hours after symptoms subsided or, in the case of passengers who had transited through Italy, Japan, Singapore, Taiwan or Thailand, for the remainder of the voyage if they presented with symptoms after 11 March 2020. Passengers who had travelled from or through China, Hong Kong, Macau, South Korea and Iran should have been prevented from boarding, but if such a passenger was on board and was showing relevant symptoms, then they should also have been required to isolate after 11 March 2020. Again, there was no evidence led of the burden of taking any such precautions.
678 The respondents did not act in accordance with those guidelines and their internal recommendations.
679 Insofar as isolating passengers presenting with ARI/ILI is concerned, there were 124 entries in the ARD log for RU2007, of which 123 were classified as either ARI or ILI (one entry being marked as negative for both). [CAU.001.003.0021] Only fifty-nine passengers and crew were placed into isolation for varying periods of time. There is no evidence as to what the catalyst for discontinuing isolation in each case was.
680 In respect of the provision of alcohol hand rub and face masks, although Mr Karpik was provided with a face mask to use when moving from his cabin to the medical centre, Mrs Karpik was not provided with any such materials and nor was she educated on how she could protect herself from infection. [LAY_SKA.001.001.0083 [123]]
681 The respondents therefore further breached their duty of care by failing to isolate passengers who presented with ARI/ILI and by failing to provide roommates of those passengers with face masks, alcohol hand rub and information on how they could protect themselves from disease.
(2) Further updated guidelines
682 There is a second aspect to Mrs Karpik’s case that the respondents failed to monitor and implement relevant guidelines. She says that a reasonable person in the position of the respondents would have implemented the following definitions and guidelines as and when they became applicable:
(1) the CDNA’s revised definition on 10 March 2020 for a “suspect case” of COVID-19, which relevantly amended the epidemiological criteria to any international travel in the 14 days prior to symptom onset, had the result that large numbers of passengers on board RU2007 satisfied the definition of a suspect case; [PUB.003.001.0001 p 306]
(2) the Prime Minister’s announcement on 15 March 2020 requiring that all international arrivals would need to self-isolate for 14 days irrespective of symptoms and banning non-essential gatherings of more than 500 people; [PUB.010.005.0001] and
(3) the Prime Minister’s announcement on 18 March 2020 banning non-essential indoor gatherings of more than 100 people and requiring venues maintain a distance of 1.5 metres between patrons. [PUB.005.003.0048]
683 In relation to the revised CDNA definition, Mrs Karpik claims that the respondents knew or ought to have known that the CDNA had updated its definition of a suspect case on 10 March 2020. She says that the respondents have admitted in their defence that they knew about the earlier guidelines published by the CDNA containing a definition of a suspect case, and that the CDNA was providing the Commonwealth Government with advice about appropriate restrictions.
684 I am not persuaded that the respondents ought to have monitored and implemented the CDNA’s updated definition. The CDNA guidelines assume much prominence in Mrs Karpik’s claim, but those guidelines are self-described as guidance to public health units (PHUs); the various versions did not purport to be directed to the public generally or occupiers of commercial premises in particular, let alone cruise ships. As explained in the Commonwealth Department of Health’s Emergency Response Plan, the CDNA was one of a number of advisory groups that was to support decision making by providing surveillance, analysis and recommendations to the AHPPC. [PUB.005.001.0021 part 4.2.4] The only reference to the CDNA in emails to the respondents and between their staff appears to be an email from an officer of the Department of Health attaching the approved National Cruise Ship Protocol on 6 March 2020, which included the following: [PCL.001.002.3357]
Of note, references to specific countries have been removed and replaced with reference to the higher and moderate risk countries and a link to the published countries on Health’s website. This is to link risk assessments with CDNA COVID-19 SoNG guidance going forward.
685 The National Cruise Ship Protocol itself is self-described as a “border operations protocol.” The only reference in that 12-page document to the CDNA is buried on page 10 in which it is said that certain travellers “may be allowed to undertake domestic travel consistent with the CDNA COVID-19 SoNG.” [PCL.001.003.0313]
686 Neither of those references should be understood as a direction to the respondents to read and comply with the CDNA guidelines. Nor was there any reference to the CDNA guidelines in the Department of Health’s “Information for the cruise industry” fact sheet. [PUB.006.001.0015]
687 As mentioned, the situation in early March 2020 was fast developing and even well-resourced operators like the respondents would be in danger of failing to keep up. The CDNA was revising its guidelines on an almost daily basis. For example, version 1.15 was issued on 3 March 2020, version 1.16 was issued on 4 March 2020, version 1.17 was issued on 5 March 2020, version 1.18 was issued on 10 March 2020 and version 2.0 was issued on 13 March 2020. In those circumstances, it would have been too burdensome for the respondents to monitor and keep up to date with guidelines published by an advisory body whose purpose was to advise the AHPPC and whose guidelines were self-described as directed to PHUs.
688 In relation to the Prime Minister’s announcements on 15 and 18 March 2020, it is not apparent just what point Mrs Karpik seeks to make. On one view, the entire cruise could be viewed as a non-essential indoor gathering. Insofar as reference to those announcements is a complaint about a failure to enforce physical distancing within venues on the ship, I have already addressed that in section F.4.5 above. Insofar as it is a complaint about the number of people in particular venues breaching a hard cap regardless of whether the cap permits fewer people in a particular venue than what would otherwise be permitted in accordance with physical distancing (ie, 1.5 metres per person), it is not established that there have been any such breaches. In any event, given that the entire cruise could be viewed as a non-essential indoor gathering, and that I have already found that a reasonable person in the position of the respondents would have implemented physical distancing, I am not persuaded that a reasonable person in the position of the respondents would have introduced further capacity limits on venues within the ship.
F.4.7 Maintain adequate medical supplies
689 Mrs Karpik submits that the respondents further breached their duty of care by failing to maintain sufficient quantities of face masks on board. She says that both the CDC COVID Ship Guidance and the Enhanced NSW Cruise Procedures advised that cruise ships should have sufficient quantities of medical supplies on board. She points out that an epidemiologist in the NSW PHU had specifically advised Dr von Watzdorf that more masks should be purchased.
690 The respondents advance two submissions. First, they say that Mrs Karpik’s pleading does not identify what is alleged to have been an “adequate” stock of face masks. Secondly, they say that they had done all that a reasonable person in their position could have done, given the well-documented worldwide shortage of face masks and other PPE at that time. They refer in particular to a statement by Dr Tedros Adhanom Ghebreyesus, the Director-General of the WHO, on 3 March 2020 in which he said: [PUB.005.001.0412]
Shortages are leaving doctors, nurses and other frontline healthcare workers dangerously ill-equipped to care for COVID-19 patients, due to limited access to supplies such as gloves, medical masks, respirators, goggles, face shields, gowns, and aprons…
Prices of surgical masks have increased six-fold, N95 respirators have more than tripled, and gowns cost twice as much.
Supplies can take months to deliver, market manipulation is widespread, and stocks are often sold to the highest bidder.
691 The respondents seek to rely on what are said to be similar remarks made by Professor Brendan Murphy, the Commonwealth’s Chief Medical Officer, in a public newsletter circulated on 13 March 2020, but that is not in evidence and must therefore be disregarded.
692 Although I have previously found that the stock of face masks on board was hopelessly insufficient and was acknowledged to be so by Dr von Watzdorf (see section B.6.4 above), I also accept that the respondents did all that a reasonable person could do in the circumstances then prevailing in obtaining and maintaining an adequate stock of face masks. The documentary evidence in that regard reveals the following.
693 On 6 March 2020, Dr von Watzdorf was advised by an epidemiologist in the NSW PHU, Ms Ressler, that any passenger or crew requiring assessment for the arrival of RU2006 would need to wear a surgical mask and that all staff assisting should be masked. [CAU.001.011.6803 p 6]
694 Early in the morning on 7 March 2020, Mary White RN, the Senior Nurse on the Ruby Princess voyage RU2006, placed an order via the ship’s ordering system for medical supplies including 2,000 face masks. [GEN.001.001.4746] She then emailed HA Group’s supply chain team at 1:12am AEDT seeking expedition of the order. [CAU.001.105.0002]
695 That evening, Dr von Watzdorf replied to Ms Ressler advising that the ship had provided masks to passengers the previous day and throughout the cruise and that she could not guarantee that there would be enough masks for the assessment process the following day as well as having sufficient stock for RU2007. She asked whether additional masks could be brought on board by NSW Health. Ms Ressler advised that NSW Health would bring its own masks and swabs and would be able to leave any that were not used. She further advised Dr von Watzdorf that supplies should be purchased at one of the vessel’s next ports of call as it was “important [to] have a good supply going forward.” [CAU.001.011.6803 p 2] Dr von Watzdorf replied thanking Ms Ressler for the assistance. In that email, she disclosed that she had tried to obtain supplies in New Zealand during voyage RU2006 but had been unsuccessful. [GEN.001.001.4763] That of course is not at all surprising given the global shortage of such supplies at that time.
696 As mentioned, the order placed by Nurse White for additional supplies was not received by the time the Ruby Princess departed for voyage RU2007 on 8 March 2020. [CRT.001.001.0275 [83]; CRT.001.001.0408 [83]] When the ship departed, it only had stock of approximately 250 face masks. [CRT.001.001.0275 [84]; CRT.001.001.0408 [84]]
697 Subsequent to the vessel’s departure, further efforts were made to both expedite the order placed on 7 March 2020 and source further face masks in New Zealand. Each consignment of supplies was initially scheduled to be delivered to the vessel when it called at Auckland on 17 March 2020. They were then diverted to Tauranga arising out of a concern that the vessel would not call at Auckland due to weather. As it happened, the vessel did not call at Tauranga or Auckland but ultimately returned early to Sydney. [SBM.020.004.0001 [445(d)-(g)]]
698 It is to be observed that orders for face masks had been placed and that Dr von Watzdorf had attempted, both during RU2006 and RU2007, to source face masks for delivery to the Ruby Princess when it called at ports in New Zealand. In those circumstances, the respondents did all that a reasonable person could have done in the circumstances then prevailing.
699 Given that I have found that the respondents were not in breach by failing to maintain sufficient quantities of face masks on board, there remains to consider the alleged breach, pleaded in the further alternative, that the respondents ought to have warned passengers that they could not maintain a sufficient quantity of face masks for the voyage.
700 There is a dearth of submissions from either side regarding the reasonableness of warning passengers whether a particular precaution could not or would not be taken. The inadequate stock of face masks was clearly a material fact. Both the CDC COVID Ship Guidance and the Enhanced NSW Cruise Procedures provided that cruise ships should maintain an adequate quantity of face masks on board. The ship’s medical personnel acknowledged, both in internal correspondence and with external parties such as Ms Ressler, that the ship had inadequate supplies. Those circumstances might be thought to give rise to a duty to warn passengers that the Ruby Princess had an inadequate stock of face masks.
701 The material effect of the inadequate stock of masks was that it contributed to further heightening the risk of coronavirus on board the Ruby Princess. It did so because those passengers who were required to be isolated and their roommates were required to be given face masks so as to reduce transmission of what could potentially be a deadly disease. Thus, the warning I have already found that the respondents ought to have given covers the heightened risk of harm to which the shortage of masks gives rise. I therefore find that there was no further breach by failure to warn specifically of the inadequate stock of face masks.
702 For the reasons I have given, I find that the respondents breached their duty of care by failing to:
(1) cancel the cruise;
(2) warn passengers about the heightened risk of contracting COVID-19 on board the Ruby Princess as compared with other cruise ships (by reason of the outbreak of ARI/ILI on the previous voyage and the insufficient quantity of face masks available for use on board);
(3) provide temperature screening of passengers and crew prior to boarding the Ruby Princess for RU2007;
(4) ask all passengers and crew whether they were experiencing symptoms consistent with COVID-19 and deny boarding to those who answered yes;
(5) encourage passengers and crew to physically distance (ie, remain 1.5 metres from other people) on board the vessel;
(6) limit numbers of people within all parts of the ship so as to allow for physical distancing (ie, 1.5 metres per person) and closing such parts which could not permit it;
(7) isolate all passengers and crew who presented with ARI or ILI until 24 hours after their symptoms subsided;
(8) from 11 March 2020, isolate passengers and crew who had travelled from or through designated countries and who presented with ILI or ARI for 14 days (ie, for the remainder of the cruise); and
(9) provide roommates of isolated passengers with face masks, alcohol hand rub and information on how they could protect themselves from disease.
G. MISLEADING AND DECEPTIVE CONDUCT
703 In closing submissions, Mrs Karpik indicated that she did not press her claim under s 29(1)(b) of the ACL. That leaves her claim under s 18(1) of the ACL in respect of which she must establish that:
(1) the respondents engaged in conduct;
(2) in trade or commerce; and
(3) the conduct was misleading or deceptive or likely to mislead or deceive.
704 It is only the third element that is in dispute, namely whether the conduct relied on by Mrs Karpik was misleading or deceptive or likely to mislead or deceive in the respects in which she alleges. Before identifying that conduct, it is convenient to identify some relevant principles that are not in dispute.
705 A representation is to be understood in the sense in which it would reasonably be understood by the representee: Krakowski v Eurolynx Properties Ltd [1995] HCA 68; 183 CLR 563 at 576-577. “Prima facie the meaning conveyed is the primary, ie, the ordinary and natural, meaning which would be conveyed to a normal person”: Owston Nominees No 2 Pty Ltd v Clambake Pty Ltd [2011] WASCA 76; 248 FLR 193 at [218]. The process of characterising relevant conduct includes considerations such as the context of the impugned conduct, the character of the transaction, the nature of the parties and what they knew about each other or may be taken to have known: Butcher v Lachlan Elder Realty Pty Ltd [2004] HCA 60; 218 CLR 592 at [37].
706 Where an alleged representation has been made to a class of consumers, as in the present case, the correct approach is to isolate and focus upon the hypothetical “ordinary” or “reasonable” members of that class: Campomar Sociedad, Limitada v Nike International Ltd [2000] HCA 12; 202 CLR 45 at [102]; Google Inc v ACCC [2013] HCA 1; 249 CLR 435 at [7]. The court should disregard reactions to the alleged conduct or representation that may be regarded as extreme or fanciful: Kraft Foods Group Brands LLC v Bega Cheese Ltd [2020] FCAFC 65; 377 ALR 387 at [236].
707 Whether or not there has been a contravention is determined by reference to the alleged conduct in the light of the relevant surrounding facts and circumstances. It is an objective question that the court must determine for itself. It invites error to look at isolated parts of the conduct. Where the alleged contravention relates primarily to a document, the effect of the document must be examined in the context of the evidence as a whole. The court is not confined to examining the document in isolation. It must have regard to all the conduct in relation to the document including the preparation and distribution of the document and any statement, action, silence or inaction in connection with the document. See Campbell v Backoffice Investments Pty Ltd [2009] HCA 25; 238 CLR 304 at [102].
708 For conduct to be misleading or deceptive or likely to mislead or deceive it must convey a meaning which is inconsistent with the truth: World Series Cricket Pty Ltd v Parish [1977] FCA 77; 16 ALR 181 at 200-201. The conduct must thereby “lead into error [or] … cause to err” (Henjo Investments Pty Ltd v Collins Marrickville Pty Ltd (No 1) [1988] FCA 42; 39 FCR 546 at 555) or have a tendency to lead a person into error: Campbell v Backoffice at [25].
709 The words “likely to mislead or deceive” in s 18 make it clear that it is not necessary to demonstrate actual deception to establish a contravention of the section. Conduct causing confusion and wonderment is not necessarily co-extensive with misleading or deceptive conduct. Section 18 is not confined to conduct which is intended to mislead or deceive; a corporation could contravene the provision even though it acted reasonably and honestly. See Google Inc at [6], [8]-[9].
G.2 The pleaded conduct and what it conveyed
710 The specific conduct relied on by Mrs Karpik is the following:
(1) the promotional and marketing material that was distributed by the respondents advertising the cruise, and in particular the use in that promotional material of the respondents’ trademark “come back new” to promote and market cruises on the Ruby Princess (see [169] above);
(2) the Dear Henry email sent on 5 March 2020, and in particular the statement that “We continue to implement increased monitoring, screening and sanitation protocols to protect the health of our guests, crew and the residents of the destinations we serve. Our measures are designed to be flexible to adapt to changing conditions and recommended best practices” (see [127] above); and
(3) the fact that passengers were permitted by the respondents to board the Ruby Princess on 8 March 2020.
711 Mrs Karpik says that that conduct conveyed the following:
(1) it was safe to board the Ruby Princess for the voyage;
(2) the respondents would adequately protect the health of the passengers during the voyage;
(3) the respondents had implemented adequate protocols to protect the health of passengers that were designed to be flexible to adapt to changing conditions and recommended best practices; and
(4) the passengers would have a relaxing, pleasurable and enjoyable time on the Ruby Princess and would come back feeling new.
712 The respondents deny that the conduct conveyed those representations, but admit that it conveyed the following to Mrs Karpik and the other passengers:
(1) Princess would take reasonable care for the safety of passengers during the voyage;
(2) Princess had implemented increased monitoring, screening and sanitation protocols to protect the health of passengers which measures were designed to be flexible to adapt to changing conditions and recommended best practice; and
(3) Princess would take reasonable steps to supply passengers with goods and services reasonably necessary to enable them to have a safe and enjoyable cruise.
713 Mrs Karpik maintains that her claim for misleading and deceptive conduct still succeeds on the representations as characterised by the respondents.
714 It must be borne in mind that the conduct occurred in circumstances of the growing epidemic (later, pandemic), and growing concern about the transmission of the virus, in particular on cruise ships. The Cruise Personalizer message received by passengers sometime before the cruise had told them that the respondents had accepted the trust that passengers placed in them for their safety and that nothing was of greater importance to the respondents than the safety and security of the passengers (see [125] above). The Emergency Notification sent on 24 February 2020 told passengers that the respondents were monitoring the situation with regard to coronavirus, working with global health authorities, and that screening requirements to safeguard passengers and guests might change.
715 The Dear Henry email of 5 March 2020 then told passengers that the respondents continued to implement increased monitoring, screening and sanitation protocols “to protect the health of [their] guests.” Passengers were also told that if they were departing on 9 March and thereafter they could cancel and get a full refund, and by implication that they could not cancel and get a refund if they cancelled their booking for the cruise in question.
716 In that context, in relation to the third aspect of the respondents’ allegedly misleading or deceptive conduct in [710] above, I consider that by welcoming passengers on board late on 8 March 2020, the respondents represented to the passengers that it was reasonably safe for the passengers to embark on the cruise, ie, that they would be reasonably safe on the cruise. Given the state of uncertainty at that time with regard to the epidemic, I do not consider that an ordinary or reasonable passenger would perceive the respondents to be saying more in relation to the safety of the cruise than that the respondents considered it to be safe. The respondents were not in a position to guarantee that there would be no coronavirus on board, or to give any absolute assurance in that regard, and a reasonable person would not have understood them to be doing so. That is consistent with my finding (at [617]) above that cruise ships presented an obviously greater risk of coronavirus than the community generally.
717 The contended-for representation that “the respondents would adequately protect the health of the passengers during the voyage” is not materially different from the admitted representation that the respondents “would take reasonable care for the safety of passengers during the voyage.” It is not apparent what “adequately” conveys; it could be construed to mean an absolute assurance of protection because anything less might be regarded as inadequate, or, it could be construed to mean “reasonably.” In contrast, it is relatively settled, in law at least, what “reasonable care” entails. That is the general norm that the law applies to people in respect of whom others depend for their safety, and would therefore readily be regarded as “adequate.” In the circumstances, I consider that the respondents’ contended-for representation more properly and helpfully captures what was conveyed by them, ie, that they “would take reasonable care for the safety of passengers during the cruise.” That must, of course, be understood to include the passengers’ health safety.
718 The contended-for representation that “the respondents had implemented adequate protocols to protect the health of passengers that were designed to be flexible to adapt to changing conditions and recommended best practices” is barely any different from the admitted representation that the respondents “had implemented increased monitoring, screening and sanitation protocols to protect the health of passengers which measures were designed to be flexible to adapt to changing conditions and recommended best practice.” The only difference is that the respondents limit the representation to be in respect of monitoring, screening and sanitation protocols rather than protocols more broadly. Given that the subject of the Emergency Notification and the Dear Henry email, insofar as it deals with protocols, is limited to monitoring, screening and sanitation, and to the extent that it matters, I accept the respondents’ characterisation of the representation. That is to say, the respondents represented that they “had implemented increased monitoring, screening and sanitation protocols to protect the health of passengers which measures were designed to be flexible to adapt to changing conditions and recommended best practice.”
719 The contended-for representation that “the passengers would have a relaxing, pleasurable and enjoyable time on the Ruby Princess and would come back feeling new” is different from the admitted representation that the respondents “would take reasonable steps to supply [the passengers] with goods and services reasonably necessary to enable them to have a safe and enjoyable cruise.” The applicant submits that the respondents by their conduct made a “promise or a prediction” that the passengers would have a relaxing, pleasurable and enjoyable time and would come back feeling new in the sense of being relaxed and reinvigorated. The applicant submits that the fact that a statement may be “mere puffery” under the general law does not mean that it does not have the character of conduct proscribed by s 18 of the ACL: Collier Constructions Pty Ltd v Foskett Pty Ltd [1990] FCA 562; 97 ALR 460 at 470 per Gummow J; Zhang v VP302 SPV Pty Ltd [2009] NSWSC 73; 223 FLR 213 at [97] per White J.
720 For the reasons already given with regard to the particular purpose made known by the passengers on acquiring the services (see section E.3 above), in my view the marketing language of “come back new” is relatively meaningless and adds nothing to having a safe, relaxing and pleasurable cruise. Also, a reasonable person in the position of a passenger would not have understood the respondents to represent that the passenger would have a relaxing, pleasurable and enjoyable time. That is because the respondents were plainly not in a position to make such a representation or promise – to any reasonable passenger’s knowledge or appreciation, whether or not such a promise would be realised would depend on factors beyond the respondents’ control and anticipation. All that the respondents could be understood to be saying is that they would supply the promised cruising services as set out in their advertising brochures and passenger contracts and in doing so would do all things reasonably within their ability to enable the passengers to have a safe, relaxing and pleasurable cruise.
721 To recap, I find the following representations to have been made by the respondents’ relevant conduct:
(1) it was reasonably safe for the passengers to embark on the cruise (Safe to Board Representation);
(2) the respondents would take reasonable care for the safety of passengers during the cruise (Reasonable Care Representation);
(3) the respondents had implemented, and would continue to implement, increased monitoring, screening and sanitation protocols to protect the health of passengers which measures were designed to be flexible to adapt to changing conditions and recommended best practice (Best Practices Representation); and
(4) the respondents would supply the promised cruising services as set out in their advertising brochures and passenger contracts and in doing so would do all things reasonably within their ability to enable the passengers to have a safe, relaxing and pleasurable cruise (Pleasurable Cruise Representation).
G.3 Future and continuing representations
722 Section 4(1) of the ACL provides that a representation is taken to be misleading if a person makes a representation with respect to any future matter and the person does not have reasonable grounds for making the representation. Section 4(2) provides that a person is taken not to have reasonable grounds for making the representation unless evidence is adduced to the contrary. Section 4(3) states that to avoid doubt, s 4(2) does not (a) have the effect that, merely because such evidence to the contrary is adduced, the person who made the representation is taken to have had reasonable grounds for making the representation, or (b) have the effect of placing on any person an onus of proving that the person who made the representation had reasonable grounds for making the representation. At face value, there appears to be some tension between ss 4(2) and (3).
723 In relation to s 51A(2) of the TPA, which was the equivalent to s 4(2), in North East Equity Pty Ltd v Proud Nominees Pty Ltd [2012] FCAFC 1; 285 ALR 217 at [28]-[30], the Full Court (Mansfield, Greenwood and Barker JJ) said that s 51A(2) imposed an “evidential burden” on the respondents to adduce evidence, but that no persuasive burden (onus) falls upon the respondents to prove they had reasonable grounds. The question of whether a respondent had, at the time of making the representation as to the future matter, reasonable grounds for making it, is particularly illuminated by the knowledge, understanding, or reasoning of the respondent. Section 51A(2) therefore cast an evidentiary burden on the respondents to adduce evidence on that issue, failing which the deeming effect of s 51A(2) was engaged thus making it unnecessary for the applicant to prove the second integer of s 51A(2) (ie, that the person had reasonable grounds for making the representation). However, if the evidentiary onus is met, it remains the applicant’s onus to prove that there were no reasonable grounds for the representation. See ACCC v Geowash Pty Ltd (Subject to Deed of Company Arrangement) (No 3) [2019] FCA 72; 368 ALR 441 at [625]; Director of Consumer Affairs Victoria v Gibson [2017] FCA 240 at [201].
724 As noted in Gate Gourmet Australia Pty Ltd (in liq) v Gate Gourmet Holding AG [2004] NSWSC 149 at [281], a representation may be a representation with respect to a future matter even if it is also, impliedly, a representation as to the existing state of mind of the maker: Ting v Blanche [1993] FCA 781; 118 ALR 543 at 553; Sykes v Reserve Bank of Australia [1998] FCA 1405; 88 FCR 511 at 514-515.
725 With respect to determining whether the maker of a representation had reasonable grounds to make it, the question is not as to the maker’s subjective belief. The question is whether, when made, the maker had reasonable grounds for making the representations to be determined in light of what the maker actually then knew and whether those grounds, objectively, were reasonable: ACCC v Dateline Imports Pty Ltd [2015] FCAFC 114 at [99]-[102]; ACCC v Mazda Australia Pty Ltd [2023] FCAFC 45 at [108].
726 As the Court (Bowen CJ, Lockhart and Fitzgerald JJ) observed in Global Sportsman Pty Ltd v Mirror Newspapers Ltd [1984] FCA 167; 2 FCR 82 at 88, the non-fulfilment of a promise when the time for performance arrives does not of itself establish that the promisor did not intend to perform it when it was made or that the promisor’s intention lacked any, or any adequate foundation. That position applies whether or not the promise is contractual: Concrete Constructions Group v Litevale Pty Ltd [2002] NSWSC 670; 170 FLR 290 applied in Fonterra Brands (Aust) Pty Ltd v Viropoulos (No 3) [2015] FCA 1050; 109 ACSR 242 at [98].
727 The applicant says that her contended-for representations were future representations as they were directed to events that were to occur in the future – namely the voyage – and accordingly the representations were capable of being relied upon by the passengers at the time that they boarded the cruise. The respondents say that to the extent that their contended-for representations were representations with respect to future matters, which they deny, the second respondent had reasonable grounds to make them.
728 The applicant pleads that insofar as her contended-for representations were not future representations, they were continuing representations as they were not expressly or impliedly confined by time and the respondents failed to correct or qualify the representation at any time before and up to the time of boarding. The applicant refers to Gate Gourmet at [284] where Einstein J explained that a representation may, depending on the precise circumstances in which it was made and upon later circumstances, have a continuing effect during the period of time following the date upon which it was made and until it is acted upon. See also McGrath v Australian Naturalcare Products Pty Ltd [2008] FCAFC 2; 165 FCR 230 at [147]-[148] per Allsop J, Stone J agreeing.
729 The applicant also says in submissions that the respondents dispute that the representations were continuing representations. However, it is not clear from the respondents’ pleadings or submissions that the respondents actually dispute this. Instead, it appears that the respondents merely deny that the applicant’s contended-for representations were made at all, and do not plead in the alternative that if the representations are found to have been made that they were not continuing representations.
730 The Safe to Board, Reasonable Care, Best Practices and Pleasurable Cruise Representations were all representations as to future matters as they related to the respondents’ conduct in relation to the cruise and the passengers’ safety on the cruise all of which was to occur in the future relative to when the relevant conduct occurred. The Best Practices Representation can be characterised as both a representation as to the current state of things as well as a representation as to future matters, as the representation conveys that the respondents had already implemented various protocols to protect passengers, and would continue to do so until embarkation and on the cruise, with the intention to adapt those protocols to future changing conditions and recommended best practice.
731 In my view, all the representations as to future matters (ie, the state of safety on the voyage and the standards of care and services to be provided on the voyage), unless resiled from or corrected, were continuing up until the time of the relevant future event or circumstance, being the cruise. That finding that the representations were continuing introduces consideration of whether the respondents’ non-disclosure of any change in circumstances, or failure to warn, amounts to misleading or deceptive conduct.
732 A failure to warn may amount to misleading conduct where, in all the circumstances, there is a reasonable expectation that a warning would be given: H Lundbeck A/S v Sandoz Pty Ltd [2022] HCA 4; 399 ALR 184 at [69]; Miller & Associates Insurance Broking Pty Ltd v BMW Australia Finance Ltd [2010] HCA 31; 241 CLR 357 at [14]-[23]. In Miller, French CJ and Kiefel J held (at [20]) that in commercial dealings between individuals or individual entities, characterisation of whether conduct is misleading will be undertaken by reference to its circumstances and context including silence, the knowledge of the person to whom the conduct is directed, and the existence of common assumptions and practices established between the parties or prevailing in the particular profession, trade or industry.
733 In Addenbrooke Pty Ltd v Duncan (No 2) [2017] FCAFC 76; 348 ALR 1 at [482], Gilmour and White JJ summarised the principles concerning misleading and deceptive conduct by non-disclosure or silence which emerge from the authorities. Their Honours said that it was not possible to categorise all of the circumstances in which a reasonable expectation of disclosure may arise, but that such circumstances may exist when either the law or equity imposes a duty of disclosure, when a statement conveying a half-truth only is made, when the representor has undertaken a duty to advise, when a representation with continuing effect, although correct at the time it was made, has subsequently become incorrect, and when the representor has made an implied representation.
734 Applying these principles to the present case, I find that, in the context of the continuing representations made to the passengers who were reasonably relying on the particular knowledge of the respondents in relation to the services they would provide on the cruise, there was a reasonable expectation that the respondents would disclose if they were no longer able to provide the services or protect the safety of the passengers as originally promised.
G.4 Misleading or deceptive or likely to mislead or deceive
G.4.1 Safe to Board Representation
735 It will be recalled that this representation by the respondents was that it was reasonably safe for passengers to embark on the cruise.
736 I have already found that the respondents were negligent not to have cancelled the cruise because of their knowledge of the risks and dangers, as well as the inadequate measures to minimise those risks – including with respect to screening, isolation, physical distancing and face masks. In those circumstances, it follows that the respondents did not have a reasonable basis to represent, at least on 8 March 2020 before the passengers boarded, that it was reasonably safe for passengers to board the vessel.
737 Moreover, the respondents offered no witness evidence to justify their representation. Indeed, they adduced no evidence to establish that they had reasonable grounds for making the representation. Under s 4(2), they are therefore to be taken as having had no such grounds.
738 The Safe to Board Representation was therefore misleading.
G.4.2 Reasonable Care Representation
739 It will be recalled that this representation by the respondents is that they would take reasonable care for the safety of passengers during the cruise.
740 Once again, having found that the respondents were negligent in certain respects with regard to their care of the passengers while on the cruise, notably in their pre-embarkation screening, lack of implemented or even encouraged physical distancing and inadequate isolation regime, it must follow that they did not have reasonable grounds for making the representation. That is because as at the time of the passengers boarding, the respondents knew what care they were going to provide, in the sense of what measures they were going to take to minimise the risk of COVID-19 infection during the cruise. I have found that those measures were inadequate relative to what the reasonable person would have done. Since the care was not going to be up to what the standard of reasonableness required, there was no reasonable basis to say that it would be.
741 Further, as with the Safe to Board Representation, because the approach of the respondents was to deny the representation, they adduced no evidence to show that they had reasonable grounds to make it. Hence, s 4(2) again has the result that they are to be taken not to have had reasonable grounds.
742 The Reasonable Care Representation was therefore misleading.
G.4.3 Best Practices Representation
743 As I have found, this representation by the respondents is that they had implemented, and would continue to implement, increased monitoring, screening and sanitation protocols to protect the health of passengers which measures were designed to be flexible to adapt to changing conditions and recommended best practice. As I have noted above, this representation was one as to the state of things at the time it was made, as well as to future matters.
744 The applicant submits that this representation is properly characterised as a statement of fact rather than opinion. The applicant refers to Tobacco Institute of Australia Ltd v Australian Federation of Consumer Organics Inc [1992] FCA 962; 38 FCR 1 in which the representation that there was “little evidence and none which proves scientifically that cigarette smoke causes disease in non-smokers” was held to be a misleading statement of fact. This conclusion was reached by the Court even though it found that the evidence of the scientists called clearly demonstrated that “in the universe of scientists there is no objective criterion upon which the truth of the assertion in the advertisement can be judged”, because a not insignificant section of the target audience, even if well informed, would perceive the statement to be an assertion of fact as to the state of the evidence: Tobacco at 27 and 30 per Foster J and 47 per Hill J.
745 I accept that, insofar as the representation is one as to the current state of things, the representation directed towards the passengers would have been understood by them as a statement of fact that the respondents had implemented protocols designed to be flexible and in accordance with recommended best practice. Insofar as the representation is a future representation, it is best characterised as a promise that the respondents would continue to do so.
746 Whether or not this representation was misleading requires consideration of what would have been understood by a reasonable passenger by “flexible” and “best practice” in the circumstances of the evolving pandemic.
747 The applicant submits that the respondents’ measures were not “flexible”, as important developments during the course of the cruise such as the announcement of COVID-19 as a global pandemic, the introduction of mandatory social distancing requirements, a requirement for all overseas arrivals to self-isolate, a ban on cruises, and a change in the CDNA’s definition of a suspected case had no impact on the way in which the cruise was operated. The respondents contend that the applicant’s submission that the measures were not “flexible” was not pleaded and is therefore not open to be raised for the first time in closing submissions.
748 In my view, any dispute as to whether the measures introduced were “flexible”, or “designed to be flexible”, or more to the point whether there were any reasonable grounds to represent that, is clearly raised by the pleaded misleading and deceptive conduct case in relation to the Best Practices Representation. However, Mrs Karpik’s misleading representation claim is confined to the time during which the representation could have been relied on by Mrs Karpik, which is the period from the date of the 5 March Dear Henry email to the time of embarkation – the fact of the respondents’ failure to implement flexible or adaptive measures after embarkation and during the cruise is not relevant except insofar as the respondents knew prior to embarkation that they would fail in that regard, or they had no reasonable basis to think that they would not.
749 The applicant submits that the measures introduced by the respondents did not reflect “best practice” as they failed to implement the measures the subject of Australian and US government protocols. The respondents say that reliance on this alleged failure is misconceived, as there is nothing in the material said by the applicant to give rise to the Best Practices Representation that warranted rigid adherence to each and every recommendation. I accept that rigid adherence to every recommendation from every relevant Australian and US government source is not what was represented or promised; what the passengers would have reasonably understood by the representation is that the respondents had and would continue to substantially adhere to the “best practice” recommendations that were directed to cruise ship operators and which specifically related to the health and safety of passengers on cruise ships.
750 As I have found in relation to the negligence case, although the respondents did introduce some monitoring, screening and sanitation protocols to protect passengers that were in accordance with various guidelines and protocols, the respondents were aware as at 5 March 2020 and until the time of embarkation that those protocols were ineffective in protecting the health of passengers. Prior to embarkation, the respondents were aware (and the passengers were not) of an outbreak of ARI/ILI on the previous voyage, that the monitoring and screening processes on that voyage had been ineffective, and that there was a heightened risk of COVID-19 on board the vessel. The respondents were also aware of internal operational and resourcing issues which meant that they were unable to implement specific monitoring, screening and sanitation protocols that could protect the passengers in accordance with best practice, such as introducing temperature screening and maintaining adequate supplies of face masks for crew and passengers.
751 Although I found in the context of the negligence case that the respondents had done all things reasonably within their ability in the circumstances to obtain medical supplies, the inadequacy of the supplies prior to embarkation was well known to the Ruby Princess’s medical personnel, and it was known to the respondents that both the CDC COVID Ship Guidance and the Enhanced NSW Cruise Procedures provided that cruise ships should maintain an adequate stock of face masks on board. Further, prior to embarkation, the respondents did not implement the specific measures of asking all passengers and crew if they were experiencing symptoms associated with COVID-19, and if so, denying boarding to them.
752 There was therefore no reasonable basis for making the representation on 5 March 2020 that the respondents had implemented increased monitoring, screening and sanitation protocols to protect the health of passengers which measures were designed to be flexible to adapt to changing conditions and recommended best practice, and no reasonable grounds on which to maintain that representation until the time of embarkation. On that basis I find that the representation was misleading.
753 Further, as with the above two representations, because the respondents adduced no evidence to show that they had reasonable grounds to make the representation, s 4(2) again has the result that they are to be taken not to have had reasonable grounds.
G.4.4 Pleasurable Cruise Representation
754 As will be recalled, this representation is that the respondents would supply the promised cruising services as set out in their advertising brochures and passenger contracts and in doing so would do all things reasonably within their ability to enable the passengers to have a safe, relaxing and pleasurable cruise.
755 The Pleasurable Cruise Representation is implied from the marketing and promotional material produced by the respondents about the services they would provide. The applicant submits that to the extent that the representation was true at the time that it was made, ie, when the advertising brochures and passenger contracts were provided to Mrs Karpik (and the other passengers), it had become false in the weeks and days before passengers boarded the Ruby Princess on 8 March 2020. The applicant submits that she had a reasonable expectation that if the representation was no longer true and correct, she would be informed of the change.
756 The applicant submits that in order for the representation to be misleading or deceptive, it was not necessary for the respondents to later learn that the cruise would not necessarily be safe or pleasurable or that they would not take reasonable steps to enable passengers to have a safe or pleasurable cruise, citing Fraser v NRMA Holdings Ltd [1995] FCA 9; 55 FCR 452 at 467 and Advance Building Systems Pty Ltd v Ramset Fasteners (Aust) Pty Ltd [1995] FCA 236; ATPR ¶46-144 at 53,136. Those judgments are good authority for the proposition, noting that the second was overturned on appeal but on a different point. However, the applicant submits that, in any event, the respondents were aware of the information or circumstances which rendered the representation misleading or deceptive.
757 The respondents accept that the act of permitting passengers to board the vessel carried an implied representation that “the second respondent would take reasonable steps to supply them with goods and services reasonably necessary to enable them to have a safe and enjoyable cruise”, which is not substantially different to the Pleasurable Cruise Representation I have identified. The respondents say that that representation was true because the second respondent took such reasonable steps.
758 As noted at [169] above, by the time of the trial Mrs Karpik no longer had copies of the brochure or advertisements from which she first learnt of the cruise, and could not recall precisely which brochure she had received. Nonetheless, I accept that the relevant brochures and advertising material were published before Mrs Karpik booked her ticket for the cruise on 5 September 2019 and received her passenger contract.
759 The respondents did not make any submissions or adduce any evidence as to whether they had reasonable grounds for making the Pleasurable Cruise Representation prior to and at 5 September 2019. In the absence of any evidence being adduced to the contrary, pursuant to ACL s 4(2) the respondents would be deemed not to have had reasonable grounds for making the representation. However, as at the time that the representation was made in September 2019, the global COVID-19 pandemic had not yet begun. There is no apparent reason why the respondents would not have reasonably held the belief that they would, in accordance with their usual business, provide the promised cruising services as set out in their advertising brochures and passenger contracts and in doing so would do all things reasonably within their ability to enable the passengers to have a safe, relaxing and pleasurable cruise. Evidence other than that of the parties found to have made the relevant representations as to a future matter may be relied on in concluding, on the overall probabilities, that there were reasonable grounds for the representations: Cummings v Lewis [1993] FCA 190; 41 FCR 559 at 566 per Sheppard and Neaves JJ; City of Botany Bay Council v Jazabas Pty Ltd [2001] NSWCA 94; [2002] ANZ ConvR 300 at [83] per Mason P, Beazley JA agreeing at [105].
760 Despite the absence of any evidence adduced by the respondents on the point, I find that considering the overall circumstances of the case, including the absence of any submission or evidence from the applicant, that the respondents did have reasonable grounds to make the Pleasurable Cruise Representation in September 2019.
761 However, as noted above, the Pleasurable Cruise Representation is properly characterised as a continuing one from the point that the marketing brochures and passenger contracts were provided, up until the time of embarkation.
762 Given the relationship between the applicant and the respondents as being between consumer and service-provider, and the attendant disparity in knowledge about the services being provided and the changing circumstances relevant to their provision, I find that the passengers could reasonably expect that if the respondents were no longer able to supply the promised cruise and do all things reasonably within their ability to enable the passengers to have a safe, relaxing and pleasurable cruise, they would have advised the passengers of that.
763 I therefore accept the applicant’s submission that even if the respondents had reasonable grounds for making the representation at the time it was made, those reasonable grounds fell away in the weeks and days prior to embarkation, and in the absence of disclosure by the respondents that there was an appreciable risk that they would no longer be able to deliver the promised services, the representation became misleading. This is because, as identified above in relation to the other impugned representations, the respondents knew about the developing COVID-19 situation, the ineffectiveness of the screening and monitoring protocols in place on the Grand Princess, and their lack of temperature screening and medical supplies for the Ruby Princess cruise. They were aware that there was an appreciable risk that they would not be able to deliver the promised cruising services. This is reinforced by the fact that respondents offered full refunds on cancellations of cruises departing from 9 March and thereafter. It was clearly in contemplation by the respondents in the lead up to the Ruby Princess cruise that passengers on that cruise, and other imminent cruises, may find the cruising services which were to be provided unsatisfactory.
764 Further, with respect to the second part of the representation, ie, that the respondents would do all things reasonably within their ability to enable the passengers to have a safe, relaxing and pleasurable cruise, as I have found above with respect to the other representations, by the time of embarkation the respondents no longer had reasonable grounds to make such a representation. In the absence of the respondents resiling from or correcting the representation, it was misleading. As with the other representations, because the respondents adduced no evidence to show that they had reasonable grounds to make the representation, s 4(2) again has the result that they are to be taken not to have had reasonable grounds.
765 The Pleasurable Cruise Representation was therefore misleading.
H.1 ACL s 61 consumer guarantees
766 The claim for damages for failure to comply with the ACL s 61 consumer guarantees, being the purpose and result guarantees, is brought under ACL s 267(4) which provides that the consumer may recover damages for any loss or damage suffered by the consumer “because of the failure to comply with the guarantee if it was reasonably foreseeable that the consumer would suffer such loss or damage as a result of such a failure.” The use of the words “because of”, as with the use of the word “by” in s 82 of the TPA, should be understood to import the traditional notion of causation as a question of fact to be determined by reference to commonsense and experience into which policy considerations and value judgements necessarily enter: Norcast SárL v Bradken Ltd (No 2) [2013] FCA 235; 219 FCR 14 at [326] per Gordon J, and the cases there cited. Section 267(4) provides for the consequential losses component of compensation, as opposed to s 267(3)(b) which provides for the performance interest component of compensation expressed as “compensation for any reduction in the value of the services”: Scenic HCA at [63] per Edelman J.
767 I have found that both the purpose and result guarantees were not complied with. That was because both Mr Karpik and Mrs Karpik contracted COVID-19 on board the cruise which had the result that neither Mrs Karpik’s known purpose nor her known desired result was realised, and that that arose from a cause related to the services in question. It is not contested, or at least not seriously, that the loss and damage that flowed from the failure to comply with the guarantees were not reasonably foreseeable. That loss and damage, as I will come to in more detail in section JJJJ below, arises from any personal injury suffered by Mrs Karpik (relevantly her COVID-19 infection and adjustment disorder including non-economic loss and out of pocket expenses) and distress and disappointment of the nature recognised in Baltic Shipping Co v Dillon.
768 The respondents’ submissions in opposition to causation on the ACL s 61 claims are principally directed at contending that Mr Karpik did not contract COVID-19 on the cruise and that Mrs Karpik did not contract COVID-19 at all. I have already dealt with those contentions.
769 Next, the respondents submit that causation on these claims “is infected by the same fallacy as that for the negligence cause of action – namely that proof of an increase in risk is sufficient to prove causation as a matter of fact to the civil standard.” I will come to causation for the negligence claim. But the question of causation for the s 61 claims is quite different. Once it is concluded, as I have, that the services were not reasonably fit for purpose or that they were not of such a nature and quality that they might reasonably be expected to achieve the known desired result, it is necessary to ask what loss or damage was suffered “because of” those failures. It is not necessary to analyse each specific shortcoming in the services, such as pre-embarkation screening and physical distancing, and ask whether, had those individual shortcomings not occurred, the loss and damage would still have been suffered.
770 As I explained in section E.6 above, the services as a whole failed to keep the passengers safe, and they could not reasonably have been expected to keep the passengers safe in light of the evolving pandemic at that time. The quite foreseeable consequences of that failure include Mr and Mrs Karpik contracting COVID-19.
771 The respondents also submit that since the point of an award under s 267(4) is to put Mrs Karpik in the position that she would have been in had the services been reasonably fit for purpose or for the result, the failure to comply with the guarantees can give rise to, at most, damages for distress and disappointment. That submission, however, misses the obvious point that had the guarantees been complied with, Mr and Mrs Karpik would not have contracted COVID-19 and Mrs Karpik would therefore not have suffered the consequential loss and damages that she did suffer. To deny recoverability of such damages would be to put a pen through s 267(4).
772 In the circumstances, I find that Mrs Karpik’s claimed loss and damage arising from her COVID-19 infection and Mr Karpik’s COVID-19 infection were “because of” the respondents’ failure to comply with the purpose and result guarantees.
773 It is common ground that CLA s 5D applies to Mrs Karpik’s claim in negligence. The parties did not differentiate between causation under the common law and the CLA on the one hand, and the ACL s 60 claim on the other. In those circumstances, my conclusions on causation apply to both the common law and the ACL care guarantee claim.
774 Section 5D, which is within Division 3 entitled “Causation”, provides:
5D General principles
(1) A determination that negligence caused particular harm comprises the following elements—
(a) that the negligence was a necessary condition of the occurrence of the harm (factual causation), and
(b) that it is appropriate for the scope of the negligent person’s liability to extend to the harm so caused (scope of liability).
(2) In determining in an exceptional case, in accordance with established principles, whether negligence that cannot be established as a necessary condition of the occurrence of harm should be accepted as establishing factual causation, the court is to consider (amongst other relevant things) whether or not and why responsibility for the harm should be imposed on the negligent party.
(3) If it is relevant to the determination of factual causation to determine what the person who suffered harm would have done if the negligent person had not been negligent—
(a) the matter is to be determined subjectively in the light of all relevant considerations, subject to paragraph (b), and
(b) any statement made by the person after suffering the harm about what he or she would have done is inadmissible except to the extent (if any) that the statement is against his or her interest.
(4) For the purpose of determining the scope of liability, the court is to consider (amongst other relevant things) whether or not and why responsibility for the harm should be imposed on the negligent party.
775 As can be seen, s 5D(1) divides causation in negligence into two distinct elements – “factual causation” and “scope of liability”: Wallace v Kam [2013] HCA 19; 250 CLR 375. An orthodox application involves a two-step inquiry. In the present case, the first step requires Mrs Karpik to establish that the respondents’ negligence was a necessary condition of the occurrence of her harm. That is established by application of the “but for” test: Strong v Woolworths Ltd [2012] HCA 5; 246 CLR 182 at [18] per French CJ, Gummow, Crennan and Bell JJ; Wallace v Kam at [16] per French CJ, Crennan, Kiefel, Gageler and Keane JJ. The second requires a normative assessment as to whether it is appropriate for the respondents to be held liable for the harm factually caused by their negligence: Wallace v Kam at [14] per French CJ, Crennan, Kiefel, Gageler and Keane JJ.
776 The parties approached the question of factual causation as an orthodox application of CLA s 5D(1)(a). No reference was made to s 5D(2), by which legal causation might be established in an “exceptional case” where factual causation is not established.
777 Mrs Karpik addressed whether her harm was caused by the respondents’ failure to cancel the cruise, failure to warn and, separately, failure to implement reasonable precautions (ie, the failures I have found at items (3)-(9) of [702] above).
778 I have found in section F.4.2 above that the respondents breached the duty of care they owed to Mrs Karpik by failing to cancel RU2007. As such, it is beyond question that factual causation is established because, plainly, Mr and Mrs Karpik would not have contracted COVID-19 on board the Ruby Princess had the voyage been cancelled as it ought to have been. However, against the possibility that that conclusion on cancellation is wrong, I consider below whether causation is made out under the applicant’s case concerning the respondents’ failure to warn and failure to implement reasonable precautions.
779 Mrs Karpik submits that no difficult issues of causation arise in relation to the failure to warn case in circumstances where her unchallenged evidence is that:
(1) if she had not received the reassurances from the respondents leading up to the cruise, she would not have boarded;
(2) if she was offered a refund for the cruise she would have cancelled her ticket as she would have thought that there must have been a risk associated with the cruise; and
(3) if she was aware of a risk of contracting COVID-19 on board she would have cancelled her ticket.
780 The respondents do not specifically address factual causation on the duty to warn case. The only part of the submissions made by the respondents that are relevant to determination of the causal question in relation to the failure to warn case are that Mrs Karpik did not contract COVID-19 and that Mr Karpik contracted COVID-19 prior to boarding the vessel. As will be recalled, I have found that both Mr and Mrs Karpik contracted COVID-19 on board the Ruby Princess: see section C above.
781 Thus if, as Mrs Karpik submits, I find that she would not have boarded the Ruby Princess if the respondents had warned passengers about the heightened risk of COVID-19 on board voyage RU2007, then that would be the end of the inquiry in relation to factual causation. That is because, plainly enough, if the Karpiks did not board the vessel, neither would have contracted COVID-19 and Mrs Karpik would not have suffered the mental harm for which she claims damages.
782 An objection was initially taken by the respondents to the evidence given by Mrs Karpik as to what she would have done had the respondents provided the warning that she says ought to have been provided. The respondents submitted that such evidence ought to be excluded for the purpose of determining factual causation pursuant to CLA s 5D(3)(b). The applicant pressed for the admissibility of Mrs Karpik’s evidence on this topic for all purposes on the basis that s 5D(3)(b) is not picked up and applied in federal jurisdiction, citing Gill v Ethicon at [4448]-[4458]. Confronted by that authority, the respondents did not press their objection. I would in any event overrule the objection and allow the evidence on the basis of that authority.
783 Although Mrs Karpik’s hindsight evidence is admissible, it should nonetheless be treated with caution: Chappel v Hart [1998] HCA 55; 195 CLR 232 at [32] (see fn 33) per McHugh J; Rosenberg v Percival [2001] HCA 18; 205 CLR 434 at [16] per Gleeson CJ.
784 Limited weight can be attributed to Mrs Karpik’s highly self-serving counterfactual statements themselves. I have previously explained that my approach to her evidence is to test whether it is consistent with the overall probabilities and human experience. (See section B.7.1 above.)
785 It will be recalled that, at one point in cross-examination, Mrs Karpik said that she accepted that there was some risk of coronavirus on board: see [178] above. That is consistent with her heightened awareness of the risk of transmission of infectious diseases by reason of her training as a nurse, and with the various discussions she had with her friends and family members: see [174]-[175] above. I have also accepted that:
(1) she felt reassured by the respondents’ various pre-boarding communications because she understood that the respondents would be taking steps to protect the health and safety of passengers by implementing increased monitoring, screening and sanitation: see [177] and [184]-[186] above; and
(2) she believed that if there was any evidence of coronavirus on the ship or a significant risk of coronavirus on board, then the respondents would have either cancelled the voyage or informed passengers so they could make their own decision as to whether to board: see [179] and [182] above.
786 It is therefore to be observed that she was aware of some risk of coronavirus, that she felt reassured by the respondents’ communiques, and that she expected to be warned of any significant risk of coronavirus. The Karpiks were elderly and suffered from some pre-existing conditions, including Mr Karpik being legally blind. They were travelling with a friend who had been diagnosed with cancer. They were ignorant of the heightened risk on board the Ruby Princess. There is nothing to suggest that they approached risk to their health in a cavalier or reckless fashion. Indeed, as I will come to, Mrs Karpik’s medical history reveals a preoccupation with concern about her health.
787 In those circumstances, any warning by the respondents as to the heightened risk on the Ruby Princess would have been sufficient to dispel any misapprehension that Mrs Karpik may have been labouring under regarding the extent of the risk of coronavirus on board. That is to say, her evidence as to what she would have done if she had been warned is supported by the overall probabilities and human experience. I therefore find that if Mrs Karpik had been warned about the heightened risk on board the Ruby Princess, she would not have boarded the vessel and, therefore, would not have suffered the harm for which she sues. She has therefore established factual causation on the failure to warn case.
(2) Failure to implement reasonable precautions
788 Given my findings, it is not strictly necessary to address factual causation on the reasonable precautions case. Nonetheless, I consider it prudent to record what I would have held in case I am wrong. Before turning to consider that, I observe that if I am wrong that could be in finding either that: (a) the respondents were negligent in failing to warn of the heightened risk on board Ruby Princess voyage RU2007 or (b) Mrs Karpik would not have boarded RU2007 if she were warned of that heightened risk.
789 Each alternative requires a different analysis. The first posits that I am wrong in finding the respondents in breach for failing to warn. The relevant enquiry then removes that breach from what a reasonable person would have done and the counterfactual analysis. The second posits that, although I am right in finding the respondents in breach for failing to warn, Mrs Karpik failed to establish that she would not have boarded. The relevant counterfactual enquiry then supposes that the respondents ought to have warned passengers of the heightened risk, but that Mrs Karpik would not have been swayed by that warning. That of course leaves it open that other passengers might not have boarded, thereby reducing the total number of passengers on board. Indeed, human experience suggests that there would certainly have been some passengers that would have elected not to board.
790 Both sides addressed the causal enquiry in relation to the failure to take reasonable precautions without reference to the breach by failure to warn. Their submissions are therefore only relevant to the first of the two respects in which I might be wrong. In those circumstances, that is the only alternative that I propose to address.
791 Mrs Karpik submits that the failure to screen passengers and crew and the failure to introduce physical distancing measures on board were causative of her loss; the remaining breaches were pressed for the advantage of other group members.
792 Mrs Karpik contends that Mr Karpik was most likely infected during the safety muster on 8 March 2020 where some 200 people were in very close proximity to one another. She says that adequate pre-screening, and temperature checks in particular, would have reduced the likelihood of a person infected with COVID-19 being on board. That is because 80% of symptomatic cases in March 2020 had a fever and fever often presents before other respiratory symptoms. Adequately screening for symptoms would have therefore only left asymptomatic and pre-symptomatic cases on board and there is a much lower risk of transmission associated with asymptomatic cases. Mrs Karpik further submits that physical distancing would have been highly effective in reducing the risk of transmission from any case not caught by the screening of passengers for symptoms when boarding.
793 The respondents submit that factual causation is not established because:
(1) Mrs Karpik does not contend that the respondents should have kept Mr and Mrs Karpik apart from each other;
(2) physical distancing would have been ineffective in light of what we now know about aerosol transmission of the virus;
(3) in respect of the allegation that Mr Karpik was most likely infected at the safety muster, it is entirely speculative:
(a) whether the enhanced screening measures would have resulted in truly infectious individuals being denied boarding;
(b) that one or more of those infected persons would have been amongst the 200 persons at the same safety muster as Mr Karpik; and
(c) that one or more of those persons would have been sufficiently close to Mr Karpik to infect him; and
(4) the expert evidence goes no higher than showing that the failure to take the precautions only increased the risk of harm, which is insufficient to establish causation unless and until the High Court adopts the reasoning in Fairchild v Glenhaven Funeral Services Ltd [2002] UKHL 22; [2003] 1 AC 32.
794 Because Mrs Karpik does not contend that the respondents should have kept her and her husband apart, and because each of her injuries depend upon his infection, the relevant question for consideration is whether, but for the respondents’ negligence, Mr Karpik would have been infected with coronavirus. To answer that question, it will be necessary to consider what effect the implementation of symptom and temperature screening would have had, as well as the effectiveness of physical distancing.
(a) Effectiveness of screening for symptoms
795 The respondents accept that a “substantial majority” of symptomatic individuals infected with the Wuhan strain of the virus presented with a fever. The evidence of Professors Bennett, McCaw and Valley, instructed by the respondents, cite a study in which it was reported that fever often presents before other respiratory symptoms. [EXP_RES.002.001.1458 [107]] That study also identified that the most likely path of discernible symptoms for those infected with COVID-19 was fever, cough, nausea/vomiting, and then diarrhoea, and that the likelihood of first presenting with fever was 0.769 – ie, 77%. [PUB.006.001.0209 p 4]
796 Thus, even if symptomatic passengers were untruthful in declaring their symptoms to the respondents, temperature checking passengers prior to boarding would nonetheless have excluded from the voyage a vast majority of symptomatic cases.
(b) Effectiveness of physical distancing
797 Mrs Karpik submits that physical distancing is a highly effective means of reducing transmission of COVID-19. She relies on the evidence of Professors Wilder-Smith, Paterson and Bennett, each of whom gave consistent evidence that now forms part of the statement of agreed facts, namely that the risk of transmission is greatest within 1.5 to 2 metres of an infected individual as this is where the concentration of droplets and aerosol particles is greatest. That fact alone would give great credence to the submission that physical distancing is highly effective.
798 Professors Paterson and Bennett were cross-examined on the topic of physical distancing, in particular the effectiveness of it. Although Professor Bennett could not agree with the specifics of a finding reported in a scientific paper that physical distancing of 1 metre or more was effective in reducing transmission risk by five times and that the protective impact was double for every extra metre, she conceded the effectiveness of physical distancing (of 1.5 metres) under cross-examination as follows (T691:30):
I believe that that was sufficient to actually contain outbreaks and to define risk within an outbreak setting, because it’s what was applied and continued to be applied, and for the ancestral variants, it was actually very successful as a way of defining risk and managing risk with a 1.5 metre rule in place. So I think that speaks, in itself, to the effectiveness of it.
799 Professor Paterson sought to downplay the effectiveness of physical distancing. The respondents rely heavily on his evidence in that respect. Although they accept that the highest risk of exposure to coronavirus is when one is in close proximity to an infected individual, they submit that physical distancing would be ineffective given what is now known regarding the role that aerosol transmission plays in the transmission of COVID-19, in particular through the ability of aerosols to remain suspended in the air for extended periods of time. They rely in that respect on Professor Paterson’s evidence to the effect that physical distancing would not have materially reduced the risk of COVID-19 on the vessel in circumstances where the virus is primarily spread by aerosol transmission and where physical distancing would have been inadequate to mitigate the risk of aerosol transmission. That submission has a different temporal aspect to knowledge of the fact and effectiveness of physical distancing than what was considered at the breach stage in section F.4.5 above.
800 Given the deficiencies with respect to Professor Paterson’s evidence that I have previously identified (section C.2.4 above), it is important to examine his evidence critically and, in particular, not to overstate its effect.
801 Professor Paterson accepted that a distinction is to be drawn between larger short-range particles (ie, respiratory droplets) and smaller long-range particles (ie, aerosols). [EXP_RES.002.001.0001 [8.51]] He then gives the following evidence with respect to aerosol transmission in his expert report:
8.52 Morawska and colleagues [in Morawska L and Milton DK, “It Is Time to Address Airborne Transmission of Coronavirus Disease 2019 (COVID-19)” (2020) 71(9) Clinical Infectious Diseases 2311] reinforce this by stating that “although the highest exposure for an individual is when they are in close proximity, community outbreaks for COVID-19 infection in particular most frequently occur at larger distances through inhalation of airborne virus-laden particles in indoor spaces shared with infected individuals. Such airborne transmission is potentially the dominant mode of transmission of numerous respiratory infections. There is also strong evidence on disease transmission — for example, in restaurants, ships, and schools suggesting that the way buildings are designed, operated, and maintained influences transmission.”
8.53 There are now a large number of examples of these outbreaks which can only have occurred through airborne virus over longer distances than would be likely by droplet transmission. These include venues such as restaurants, gymnasiums, residential apartment blocks and churches. Transmission by the airborne route is even likely to have occurred when the infected individual is no longer in the same venue as those who become infected. The data referenced here comes from the original Wuhan strain of the virus.
(Footnotes omitted.)
802 Contrary to what the respondents submit, those passages do not say that the virus is primarily spread by aerosol (or airborne) transmission. Indeed, in the quote from Morawska and colleagues that I take Professor Paterson to be adopting at [8.52] of his report, it is said that the highest exposure for an individual is when they are in close proximity. They then add that community outbreaks most frequently occur at larger distances through aerosol transmission – ie, where community outbreaks occur at larger distances, such outbreaks occur through aerosol transmission. That such outbreaks can and do occur does not deny the effectiveness of physical distancing. Nor does it mean that, because aerosol transmission is a feature of coronavirus, all such transmission occurs through aerosol transmission. That was confirmed in cross-examination when Professor Paterson agreed that respiratory droplet transmission is “an important way by which [COVID-19 is] contracted” (T580:37-39). [PUB.005.003.0592]
803 Professor Paterson then addressed physical distancing, in light of aerosol transmission, as follows:
8.61 The proposed benefit of social distancing measures stems from early crude observations that infectious diseases that produce large respiratory droplets, with incorporated viable infectious microorganisms, travel less than 1 to 2 metres during coughing, exhalation and loud speaking (“droplet precautions”).
8.62 As noted earlier in paragraphs 8.47 to 8.53, airborne transmission is now known to be a feature of SARS-CoV-2. Indeed, airborne transmission has occurred when individuals enter a venue no longer occupied by others. Furthermore, as a result of airborne transmission, any impact of physical distancing needs to take into account a myriad of other factors such as whether it is an indoor or outdoor location, the number of people in a location and what they are doing, whether masks are being worn and the ventilation of the location. Researchers from the Massachusetts Institute of Technology have modelled their relative impacts. A person’s risk increases linearly with the number of people in a room and the duration of the event. Relative risk decreases for large, well-ventilated rooms and increases when the room’s occupants are exerting themselves or speaking loudly. Bazant and Bush conclude, “Above all, our study makes clear the inadequacy of the SixFoot Rule in mitigating indoor airborne disease transmission.” This is because in an indoor location, risk of transmission is influenced by variables (such as number of people in a room, their activities, the duration of the event and the room’s ventilation) much more likely than how closely a person is standing next to another. This is highly relevant given Mrs Karpik’s report that she visited dining rooms and other shared indoor spaces while on board.
(Footnotes omitted.)
804 None of that evidence denies that physical distancing is effective vis-à-vis respiratory droplet transmission. The closest that evidence comes to doubting the effectiveness of physical distancing is the study referred to, namely Bazant MZ and Bush JWM, “A guideline to limit indoor airborne transmission of COVID-19” (2021) 118(17) Proceedings of the National Academy of Sciences e2018995118. [PUB.005.003.0078] The premise of the study that is recorded in the introduction is that “indoor airborne transmission … plays a dominant role in the spread of COVID-19” and that “the fact that face mask directives have been more effective than either lockdowns or social distancing in controlling the spread of COVID-19 … is consistent with indoor airborne transmission as the primary driver of the global pandemic.” [PUB.005.003.0078 pp 1-2] The authors propose a time-based guideline referred to as CET – cumulative exposure time – a product of the number of occupants and their time in an enclosed space. They express CET as the following equation:
805 From that equation, the authors deduce another, the interpretation of which they say is clear: [PUB.005.003.0078 p 5]
To minimize risk of infection, one should avoid spending extended periods in highly populated areas. One is safer in rooms with large volume and high ventilation rates. One is at greater risk in rooms where people are exerting themselves in such a way as to increase their respiration rate and pathogen output, for example, by exercising, singing, or shouting. Since the rate of inhalation of contagion depends on the volume  flux of both the exhalation of the infected individual and the inhalation of the susceptible person, the risk of infection increases as
flux of both the exhalation of the infected individual and the inhalation of the susceptible person, the risk of infection increases as
806 In relation to specific parameters for COVID-19, the authors conceded that Cq, which is the product of the concentration of exhaled infection quanta by an infected individual (ie, “infectiousness”), and sr, which is relative transmissibility, are poorly constrained. From various previous outbreaks and studies, they inferred different levels of infection quanta per cubed metre of exhaled air (Cq) based on the activities that people were undertaking and produced the following graph: [PUB.005.003.0078 pp 5-6]
Although Professor Paterson did not adopt the figures as his own, he accepted under cross-examination that the graph depicts a principled and accepted difference in the likelihood of aerosol transmission based on room occupants’ activities (T586:4-22).
807 The authors then applied CET to some posited case studies that demonstrated the adequacy and effectiveness of different measures or rules; the areas beneath the lines are those the equation deems safe: [PUB.005.003.0078 p 8]
808 Finally, as ultimately made clear in the concluding section of the article, the authors note that they have focussed on aerosol transmission and “neglected the roles of both contact and large-drop [ie, respiratory droplet] transmission.” Critically, they conclude that: [PUB.005.003.0078 p 10]
Adherence to the Six-Foot Rule would limit large-drop transmission, and adherence to our guideline, Eq. 5 [ie, CET], would limit long-range airborne transmission.
809 Thus, contrary to what the respondents submit, the effect of the article and Professor Paterson’s evidence is not that physical distancing (or, as the article’s authors call it, the Six-Foot Rule) is an ineffective measure; rather, the highest the evidence goes is that physical distancing is an inadequate measure in that it does not do enough to address the risk of aerosol transmission. The graphs produced above depicting the results of the authors’ case studies make clear that, so far as aerosol transmission is concerned, although adherence to CET would be the safest option, adherence to the Six-Foot Rule nonetheless increases the duration in which it would be safe to be in the same room as an infected person.
810 The critical matters to draw from that article are therefore as follows: first, so far as respiratory droplet transmission is concerned, the authors at no point doubt the effectiveness of physical distancing and indeed reaffirm adherence to it in the conclusion and, secondly, that aerosol transmission in an indoor setting depends on air ventilation, mask usage, and the number and activity of the occupants. Of course, it is to be recalled that one of the aspects of physical distancing I have found that the respondents ought to have implemented is that they ought to have limited the numbers of people within all parts of the ship so as to allow for physical distancing and closed such parts which could not permit it.
811 Consistently with that evidence, I find that physical distancing was highly effective in preventing coronavirus transmission. Its effectiveness consists of two components. The first is that, if individuals had practised physical distancing as the respondents ought to have encouraged their passengers to do, it is highly unlikely that transmission would have occurred by respiratory droplet transmission. The second is that if capacity limits within indoor areas had been enforced so that the occupancy of those areas could accommodate physical distancing, which the respondents ought to have done, this measure would also have been effective in reducing aerosol transmission, although it would not have adequately made those areas safe for longer periods of time.
(c) The balance of probabilities and the Fairchild point
812 The respondents submit that the expert evidence goes no higher than establishing that their negligence only increased the risk of harm. Put in counterfactual terms, that is the equivalent of saying that implementation of the various measures goes no higher than giving rise to a possibility that Mr Karpik would not have been infected with COVID-19 at the safety muster. They say that proof of an increased risk of harm, being the modified test of “causation” established in Fairchild, does not satisfy factual causation under Australian law.
813 I do not understand Mrs Karpik to rely on Fairchild. It is uncontroversial that the special rule of “causation” in Fairchild does not represent the law in Australia and cannot be relied on by Mrs Karpik: Minister for the Environment v Sharma [2022] FCAFC 35; 291 FCR 311 at [320] per Allsop CJ; Amaca Pty Ltd v Cleary [2022] NSWCA 151 at [74] per Beech-Jones JA. Even if for no other reason, reliance on Fairchild in the present case is inconsistent with s 5D(1)(a) of the CLA, which requires application of the “but for” test, and Mrs Karpik does not rely on the “exceptional circumstances” provision of s 5D(2), which was envisaged in the Ipp Report (Review of the Law of Negligence (Final Report, September 2002)) at [7.26]-[7.33] to be the gateway to Fairchild. Further, although the evidence relied on by Mrs Karpik concerns possibilities and risk levels, that does not mean that she seeks to rely on Fairchild in establishing causation.
814 In determining whether, but for the failure to screen passengers’ symptoms and encourage and implement physical distancing, Mr Karpik would have contracted COVID-19, it is important to bear in mind that the standard of proof is the balance of probabilities. As explained by Kiefel J in Tabet v Gett [2010] HCA 12; 240 CLR 537 at [111]:
All that is necessary is that … the more probable inference appearing from the evidence is that a defendant’s negligence caused the injury or harm. “More probable” means no more than that, upon a balance of probabilities, such an inference might reasonably be considered to have some greater degree of likelihood; it does not require certainty.
(Emphasis added.)
815 In Kocis v S E Dickens Pty Ltd [1998] 3 VR 408, the plaintiff was injured when she slipped and fell on a pool of disinfectant in a supermarket. The supermarket had a system of checking for spillages every 30 minutes, but it was apparently not in operation on that day. The evidence did not establish when the spillage occurred, save that it was more than five minutes before the plaintiff slipped. In those circumstances, the primary judge directed the jury to return a verdict in favour of the defendant supermarket.
816 In allowing the plaintiff’s appeal and ordering a retrial, it was held by the Victorian Court of Appeal that evidence of when the spill occurred was not essential to the plaintiff’s success (at 414 per Phillips JA, Ormiston JA agreeing), and that it was open to the jury to find that, if the system had been operational, the liquid on which the plaintiff slipped would have been cleaned up (at 423 per Phillips JA and 434 per Hayne JA, Ormiston JA agreeing). In Strong v Woolworths (another slip and fall case) at [34], French CJ, Gummow, Crennan and Bell JJ cited with approval the following remarks of Hayne JA in Kocis at 430:
In my view it is of the first importance to bear steadily in mind that a plaintiff must prove his or her case on the balance of probabilities and that it is no answer to the question whether something has been demonstrated as being more probable than not to say that there is another possibility open. Thus, a jury may reasonably conclude that the probabilities are that a particular spillage would have been cleaned up by the proper application of a reasonable cleaning regime on the part of the defendant occupier while at the same time acknowledging the possibility (but not probability) that the substance was spilled only a moment before the plaintiff slipped on it. The question of causation is to be resolved by consideration of the probabilities.
817 In Seltsam Pty Ltd v McGuiness [2000] NSWCA 29; 49 NSWLR 262, Spigelman CJ (Davies AJA agreeing) addressed the use of epidemiological evidence as follows:
78 Epidemiology is, as I have noted above, concerned with the study of disease in human populations. It is not, of itself, directed to the circumstances of an individual case. For the purpose of determining whether exposure to a particular substance is the legal cause of a particular disease, epidemiology only provides evidence of possibility.
79 Evidence of possibility, including expert evidence of possibility expressed in opinion form and evidence of possibility from epidemiological research or other statistical indicators, is admissible and must be weighed in the balance with other factors, when determining whether or not, on the balance of probabilities, an inference of causation in a specific case could or should be drawn. Where, however, the whole of the evidence does not rise above the level of possibility, either alone or cumulatively, such an inference is not open to be drawn.
80 The common law test of balance of probabilities is not satisfied by evidence which fails to do more than establish a possibility…
83 The law in Australia is, in my opinion, as stated by Glass JA in in this Court in Fernandez v Tubemakers of Australia Ltd [1975] 2 NSWLR 190 at 197:
… The issue of causation involves a question of fact upon which opinion evidence, provided it is expert, is receivable. But a finding of causal connection may be open without any medical evidence at all to support it: Nicolia v Commissioner for Railways (NSW) (1970) 45 ALJR 465, or when the expert evidence does not rise above the opinion that a causal connection is possible: EMI (Australia) Ltd v Bes [1970] 2 NSWR 238; appeal dismissed (1970) 44 ALJR 360n. The evidence will be sufficient if, but only if, the materials offered justify an inference of probable connection. This is the only principle of law. Whether its requirements are met depends upon the evaluation of the evidence.
See also Carangelo v New South Wales [2016] NSWCA 126; [2016] Aust Torts Reports ¶82-275 at [71] per Emmett AJA, with whom Macfarlan and Gleeson JJA agreed.
818 Against that background, it is uncontroversial that expert evidence that expresses itself in the form of possibilities and risks, rather than probabilities, can be relevant and support an inference of causation.
819 In the present case, Mrs Karpik submits that the circumstances are such as to support a finding on the balance of probabilities that if the respondents had introduced pre-embarkation health screening for all passengers and physical distancing measures, Mr Karpik would probably not have been infected with COVID-19. I accept that submission.
820 The relevant facts and findings I have made are as follows. The prevalence of COVID-19 in New South Wales at the time of the voyage RU2007 was very low – there were only 40 reported cases. In absolute terms, the risk of exposure within the general community was also very low. Assuming a positive case on board, the risk of transmission on a cruise ship is heightened. The risk was further heightened on the Ruby Princess voyage RU2007 because of the previous outbreak of ARI/ILI and the want of an adequate supply of face masks for those who were assessed as having ARI/ILI. Nonetheless, in absolute terms, the risk was still low, as its materialisation depended necessarily on the virus being introduced on board. As it turned out, there was at least one positive case on board the vessel and Mr Karpik was infected.
821 If the respondents had implemented the pre-boarding screening that I have found a reasonable person in their position ought to have done, it is highly unlikely that there would have been a symptomatic case on board. That would then have left pre-symptomatic and asymptomatic cases on board.
822 Further, if the respondents had encouraged passengers to practise and had implemented physical distancing, that would have further reduced the likelihood of Mr Karpik coming into contact with infected respiratory or aerosol droplets, either at the safety muster or otherwise. As explained, physical distancing is an effective and “very successful” method of managing the risk of transmission of the virus.
823 In summary, when one takes into account: (1) the low prevalence of COVID-19 in the community in New South Wales; (2) it is highly unlikely that a symptomatic case would have been on board had reasonable precautions been taken; (3) the risk of transmission from asymptomatic cases is low due to their low viral load; (4) Mr Karpik was infected on board; (5) Mr Karpik’s most likely source of infection was the crowded safety muster; and (6) the effectiveness of physical distancing in further reducing the likelihood of transmission from an asymptomatic case, it is more probable than not that Mr Karpik would not have been infected with COVID-19 on board the vessel but for the respondents’ breach of the duties owed to the Karpiks.
824 To conclude as such is not to say that the mere increase in risk in failing to implement the precautions gives rise to establishing factual causation. Rather, the counterfactual posits that the respondents were not negligent because they implemented the precautions I have identified at items (3)-(9) of [702]. The implementation of those measures would have, in my view, so substantially reduced the risk of coronavirus on board that, on a balance of probabilities, the most probable result is that Mr Karpik would not have contracted COVID-19 on board. In turn, Mrs Karpik also would not have contracted COVID-19 and would not have suffered her claimed adjustment disorder.
825 The respondents submit that even if factual causation is established, normative considerations of the appropriateness of fixing liability on the respondents arise acutely in the present case. With reference to Wallace v Kam, they say that because Mrs Karpik was prepared to assume the risk of COVID-19, it would be inappropriate to find the respondents liable in respect of such harm. They also say that there are larger normative questions concerning the appropriateness of fixing liability on a private business for the consequences of contracting COVID-19. They refer, again, to submissions concerning other businesses that I have previously dealt with, and also the fact that they had been compliant with all relevant government orders.
826 It is convenient to deal with the second aspect of those submissions first. I have already addressed the same considerations at the duty stage and have rejected those arguments. Those reasons need not now be repeated. But there is a further reason why those considerations are irrelevant to the present issue.
827 The effect of the submission is that s 5D(1)(b) leaves it to courts to decide for themselves in each case whether a tortfeasor should be held liable for harm that they have caused. Although that might be a fair reading of the provision on its face, that is not what that provision provides on its proper construction. As explained in Wallace v Kam at [22], the question posed by s 5D(1)(b) is properly answered through the application of precedent in that a policy choice once made is maintained unless confronted and overruled. Those precedents include, for example, that a tortfeasor is not liable for damage that is too remote (see, eg, Overseas Tankship (UK) Ltd v Mort’s Dock & Engineering Co Ltd (The Wagon Mound) [1961] AC 388) or where a novus actus interveniens “breaks the chain of causation” (see, eg, State Rail Authority of New South Wales v Chu [2008] NSWCA 14; [2008] Aust Torts Reports ¶81-940) or where the harm suffered is not within the scope of the tortfeasor’s duty of care (see, eg, South Australian Asset Management Corporation v York Montague Ltd [1997] AC 191 and in particular the famous example given by Lord Hoffmann of the mountaineer at 213-214): Wallace v Kam at [24]. It is only in a novel case that a court is required to explain by legal policy whether or not, and if so why, responsibility for the harm should be imposed on the tortfeasor: CLA s 5D(4); Wallace v Kam at [23]. As I have explained in section F.2 above, there is nothing novel about a cruise operator’s duty of care to its passengers to take reasonable care for their health and safety. Section 5D(1)(b) is not therefore an invitation to courts to consider at large the morality, justice or otherwise of imposing liability on a tortfeasor.
828 Returning now to the reliance sought to be placed on Wallace v Kam, that case concerned the negligent failure of a neurosurgeon, Dr Kam, to warn his patient, Mr Wallace, of two material risks inherent in a recommended surgical procedure on his lumbar spine. Those risks were, first, bilateral femoral neurapraxia, which is temporary local damage to nerves within a patient’s thighs resulting from lying down on the operating table for an extended period, and, second, a 1/20 chance of permanent paralysis. The surgery was not only unsuccessful, but the first risk materialised.
829 Mr Wallace sued Dr Kam in the NSW Supreme Court claiming a negligent failure to warn of both risks and that, if he had been warned of either risk, he would have chosen not to undergo the procedure and would therefore not have suffered the neurapraxia. The primary judge found that Mr Wallace would have chosen to undergo the procedure even if warned of the risk of neurapraxia. His Honour declined to make any finding as to whether Dr Kam was negligent in failing to also warn of permanent paralysis on the basis that that could never be the “legal cause.” On appeal, the Court of Appeal considered the hypothesis that Dr Kam was negligent in failing to warn of permanent paralysis and that, if so warned, Mr Wallace would not have undergone the procedure. By majority, it was held that Dr Kam would not have been liable for the neurapraxia in those circumstances.
830 In dismissing Mr Wallace’s appeal, the High Court held that, although factual causation would be satisfied (at [29]), the determination of whether it would be appropriate to hold Dr Kam liable required consideration of the nature of the duty to warn and the policy that underlies its imposition. With reference to what Allsop P said in the Court of Appeal (Wallace v Kam [2012] NSWCA 82; [2012] Aust Torts Reports ¶82-101) at [19] and [23], their Honours said:
36 … The underlying policy is … to protect the patient from the occurrence of physical injury the risk of which is unacceptable to the patient. It is appropriate that the scope of liability for breach of the duty reflect that underlying policy.
37 The appropriate rule of attribution, or “rule of responsibility” to use the language of Allsop P, is therefore one that “seeks to hold the doctor liable for the consequence of material risks that were not warned of [and] that were unacceptable to the patient.” The normative judgment that is appropriate to be made is that the liability of a medical practitioner who has failed to warn the patient of material risks inherent in a proposed treatment “should not extend to harm from risks that the patient was willing to hazard, whether through an express choice or as found had their disclosure been made.”
831 The respondents submit that the same reasoning applies in the present case. They say that Mrs Karpik was aware of the risk of COVID-19 transmission generally and, in particular, the risk of contracting COVID-19 during the voyage but chose to accept that risk anyway. They therefore say that, following Wallace v Kam, they should not be held liable. This line of argument, if successful, would have no application to Mrs Karpik’s claim for pure mental harm; it could only apply to Mrs Karpik’s COVID injuries.
832 It will be recalled that I have rejected Mrs Karpik’s evidence to the effect that she thought that there was no risk of contracting coronavirus on the vessel: see [176] above. And, although I have accepted that her affirmative answer to the question whether she boarded the cruise accepting that there was a risk that she could have been infected with coronavirus was given on the basis of a misunderstanding, she must nonetheless have acquiesced to the risk that the virus might be present on board.
833 It is, however, important not to overstate that knowledge and consequential acquiescence. The materialisation of that risk would not necessarily have meant that either Mr or Mrs Karpik contracted COVID-19. It might have ruined their holiday in other ways by, for example, merely cutting it short and not calling at certain advertised ports (as is the case with many of the passengers) or the entire ship may have been locked down without either of the Karpiks contracting the disease. Save for the erroneous answer she gave to the misunderstood question, the extent to which Mrs Karpik accepted the risk was not explored in evidence because much of the cross-examination concerned whether she believed that there was no risk. In that respect, it is important also to bear in mind that her boarding the vessel with knowledge that there must have been some risk of coronavirus on board was in the context of reassuring communications from the respondents which encouraged Mrs Karpik’s understanding that they would take all reasonable measures to minimise the risk, which, as I have found, they did not do. It was also in the context of not knowing that there was a heightened risk on board the Ruby Princess.
834 Once those distinguishing factors are taken into account, it can be seen that the respondents’ reliance on Wallace v Kam is misplaced. The facts of that case would have to have been rather different to be applicable to the present case. First, the equivalent to the heightened risk on board the Ruby Princess might for example be that the particular operating table on which Mr Wallace was operated on had some feature, distinct from other operating tables, that made neurapraxia more likely to occur. Secondly, the equivalent to the respondents’ failure to implement reasonable pre-boarding screening and physical distancing on board might be that Dr Kam negligently placed further pressure on Mr Wallace’s thighs. There can be no doubt that if Dr Kam had negligently performed the procedure, he would have been held liable.
835 In the present case, I have found that Mrs Karpik would not have boarded the vessel if she had been warned of the heightened risk on board the Ruby Princess. She therefore did not accept any level of risk that was higher than the level of risk to which she would otherwise be exposed by a reasonably prudent cruise operator. The materiality of a heightened risk of some harm occurring cannot be in doubt. Although one might accept a 1/1000 or even a 1/100 chance of permanent paralysis, the proposition of a 1/20 risk, as in the case of Mr Wallace, is very different.
836 The harm which Mrs Karpik suffered was within the scope of the respondents’ duty of care. That is to say, the respondents had a duty of care for the health and safety of their passengers which extended to the risk of harm caused by COVID-19 infection. As the High Court pointed out in Wallace v Kam at [26], a tortfeasor’s scope of liability is often coextensive with the content of their duty that has been breached. There is no reason why that is not so in the present case.
837 In the result, Mrs Karpik has established causation in accordance with CLA s 5D not only on the cancellation case but also on the failure to warn and the failure to implement precautions cases. Those conclusions apply to the negligence and ACL s 60 claims.
H.3 Causation for breaches of ACL s 18
838 Pursuant to ACL s 236, where a person suffers loss or damage “because of” the conduct of another person and the conduct contravened s 18, the person may recover the amount of the loss or damage by action against the other person. Pursuant to CCA s 137C, Mrs Karpik cannot recover any amount of loss or damage or compensation under s 236 of the ACL for loss or damage which is, or results from, death or personal injury. It is therefore not in dispute that any award for breach of s 18 is limited to damages for distress and disappointment.
839 Relief under s 236 requires proof on the balance of probabilities of a causal link between the breach and the pleaded loss or damage. In the present case, this introduces the causal question of whether Mrs Karpik relied on the impugned representations when deciding to board the Ruby Princess cruise, leading to distress and disappointment.
840 The applicant contends that the alleged misleading and deceptive representations discussed above caused her to board the vessel, and she would not have done so but for the alleged impugned conduct. The respondents submit that the applicant’s case must rise and fall with that proposition, as she has not established that the conduct relied upon caused her to board the voyage when she otherwise would not have done so. The respondents submit that Mrs Karpik’s decision to board the voyage was an autonomous one that she made having regard to her own understanding of the risks involved. The respondents submit that the Court would not be satisfied of causation in this regard, as the applicant’s evidence discloses her sophisticated understanding of the unpredictable risk posed by COVID-19 at the time of the commencement of the voyage, with a decision by her to board the voyage in any event on the basis of the measures she herself and her companions had adopted.
841 In oral closing submissions, the applicant submits that someone being aware of the existence and risks of COVID-19 and the possibility of contracting it, as established by Mrs Karpik’s cross-examination, does not gainsay a finding that Mrs Karpik relied upon what she was told by the respondents in terms of managing that risk. She submits that the fact that she was aware of the possibility of catching COVID-19, but then proceeded to board having been told what she was told and what she took from the Dear Henry email, and by being allowed to board, reinforces that she was relying upon what she was told by the second respondent.
842 The question of causation on the ACL s 18 claim is subtly different from the question that I have dealt with at [782]-[787] above in relation to the duty to warn in the negligence case. The difference is that one does not ask what Mrs Karpik would have done had the identified warning been given, that rather whether the misleading conduct materially contributed to the loss or damage: I & L Securities Pty Ltd v HTW Valuers (Brisbane) Pty Ltd [2002] HCA 41; 210 CLR 109 at [33], [57], [62]; Henville v Walker [2001] HCA 52; 206 CLR 459 at [14], [60]-[62], [106], [109]. In the present case, the question is whether the misleading conduct materially contributed to Mrs Karpik going ahead with the cruise and boarding the vessel on 8 March 2020.
843 Mrs Karpik’s evidence is that had she not been sent the emails reassuring her that the respondents would implement increased protocols to keep passengers safe, she would have made inquiries with the travel agent as to whether it was safe to travel on the cruise. What the travel agent might have advised would be pure speculation. She also said that the reason she went on the cruise was because the respondents gave her the impression that they would ensure her safety and the fact that the cruise was not cancelled could only mean that it would be safe for everyone to travel on it. [LAY_SKA.001.001.0083 [60], [63]]
844 There can be no doubt that the communications by the respondents on which Mrs Karpik relied were intended to reassure passengers that the cruise was safe, or at least reasonably safe, and that they should go ahead with it. In those circumstances, it is hardly surprising that Mrs Karpik found the communications to be reassuring and to have that effect (see [185] above).
845 In Travel Compensation Fund v Robert Tambree t/as R Tambree and Associates [2005] HCA 69; 224 CLR 627 at [32], Gleeson CJ (with whom Gummow and Hayne JJ, at [39], and Callinan J, at [78], agreed) explained that:
Misrepresentation will rarely be the sole cause of loss. If, in reliance on information, a person acts, or fails to act, in a certain manner, the loss or damage may flow directly from the act or omission, and only indirectly from the making of the representation [Sellars v Adelaide Petroleum NL [1994] HCA 4; 179 CLR 332 at 356-357; Henville v Walker at [14]]. Where the reliance involves undertaking a risk, and information is provided for the purpose of inducing such reliance, then if misleading or deceptive conduct takes the form of participating in providing false information, and the very risk against which protection is sought materialises, it is consistent with the purpose of the statute to treat the loss as resulting from the misleading conduct.
846 This is just such a case. Although it could not be said with confidence that if the misrepresentations had not been made, Mrs Karpik would not have gone on the cruise, such a “but for” test is inappropriate to the causal connection required by “because of” in ACL s 236. It can also not be said with any confidence that if the misrepresentations had not been made, Mrs Karpik would still have gone aboard regardless. The application of a “but for” test in this case would be indeterminate. However, there can be little doubt that each of the Safe to Board, Reasonable Care and Best Practices Representations contributed to Mrs Karpik’s willingness to go aboard, and her sense of safety or security in doing so, which is exactly the effect that they were intended to have on her and the other passengers. That is sufficient to establish causation for the purposes of ACL s 236.
847 The case for causation in respect of the Pleasurable Cruise Representation is even stronger. That is because, as I have found, it was a continuing representation. That means that when the representation became misleading, the respondents were duty-bound to withdraw it. That is to say, before the passengers embarked, the respondents were duty-bound to withdraw the representation they had made that they would supply the promised cruising services as set out in their advertising brochures and passenger contracts and in doing so they would do all things reasonably within their ability to enable the passengers to have a safe, relaxing and pleasurable cruise. The effect of such a withdrawal would be much the same as the effect of giving the warning that I have found that the respondents were duty-bound to give in relation to the negligence case. For the same reasons as explained there, I am satisfied that had the respondents withdrawn the Pleasurable Cruise Representation before embarkation, Mrs Karpik would not have gone on the cruise. The reassurance that she had taken from the respondents’ various messages, and in particular the Pleasurable Cruise Representation, would have been eroded to the point that the cruise would have been too risky even for her risk appetite.
848 Barely any attention was given by the parties to the question of contributory negligence, but since it is pleaded and formally relied on by the respondents it is necessary to deal with it.
849 In response to the ACL s 60 and negligence claims, the respondents plead that if it is found that they breached a duty of care to Mrs Karpik then the damages recoverable are to be reduced to such extent as the Court thinks just and equitable having regard to Mrs Karpik’s share in the responsibility for the damage. That is with reference to s 9(1)(b) of the LRMP Act. I have already found that that section is picked up and applied as surrogate federal law to the ACL s 60 claim under ACL s 275 (see section D.3 above).
850 Leaving aside a particular with regard to self-service dining which became irrelevant during the course of the trial, the respondents particularise their contributory negligence defence by pleading that:
(1) if they breached a duty of care by failing to cancel the voyage, Mrs Karpik failed to take reasonable care for her own safety by going on the voyage;
(2) if they breached a duty of care by failing to enforce physical distancing, Mrs Karpik failed to take reasonable care for her own safety by participating in activities on the ship in close proximity to other people; and
(3) if they breached a duty of care by failing to require passengers to wear face masks in public spaces on the ship, Mrs Karpik failed to take reasonable care for her own safety by failing to wear a face mask.
851 In response to the ACL s 18 claim, the respondents plead that if they contravened that provision, loss or damage suffered by Mrs Karpik was caused by her failure to take reasonable care. That is with reference to CCA s 137B. The same particulars are identified as in relation to the ACL s 60 and negligence claims.
852 Since the ACL s 61 claims are not claims for breach of a duty of care, no contributory negligence defence is available to be pleaded in response to them.
853 The respondents submit, by way of illustration, that if they are found to have been in breach of a duty in failing to cancel the voyage, that failure to take reasonable care would be similarly attributable to Mrs Karpik as she was aware of the risk posed by COVID and yet chose to board the vessel and go on the voyage anyway. They submit that in those circumstances a substantial reduction in damages, in the order of 30%, would be appropriate.
854 The applicant submits that what a reasonable person would have done in the position of a passenger cannot be compared with what reasonable precautions a reasonable person in the position of a multinational cruise line would have implemented. The applicant also submits that CCA s 137B has no application as Mrs Karpik’s claim for damages under ACL s 18 is for distress and disappointment which is not a claim “in relation to economic loss, or damage to property.”
855 It is convenient to begin with the ACL s 18 claim. As only Dillon damages are claimed (see [1011] below), the claim is not “in relation to economic loss, or damage to property” with the result that CCA s 137B has no application.
856 With regard to the respondents’ breaches of the duty of care owed to Mrs Karpik, it is true, as I have found, that Mrs Karpik had an awareness that there was a risk of COVID-19 infection for her and her husband if they went on the cruise. There are, however, two compelling considerations that count against any finding that they were negligent which negligence contributed to them being infected with COVID-19 on the cruise.
857 First, they received the assurances from the respondents via the communications that have been discussed at length above in relation to the ACL s 18 claim. They relied on those communications and were misled by them. That caused them to go on the cruise when they otherwise would not have done so.
858 Secondly, Mrs Karpik’s state of knowledge of coronavirus before going on the cruise, including the extent of the risk that she was taking based on how contagious it is and what precautions might or should reasonably be taken, was relatively rudimentary. At that time, as emphasised by the respondents in resisting any finding of breach of duty on their part, there were no restrictions on public activity in Australia or guidance directed to the Australian public having a bearing on whether members of the public should go on a cruise, and tens of thousands of people were congregating at mass gatherings. Nearly 3,000 passengers boarded the Ruby Princess for RU2007.
859 The wisdom of passengers going on board any oceangoing cruise as at 8 March 2020 is certainly open to question. The Karpiks’ son-in-law questioned their wisdom in doing so, although he is a medical specialist, and can therefore be taken to have greater knowledge and understanding than a non-specialist, and he had not received the assurances that the Ruby Princess passengers had received. However, as I have found, passengers are entitled to rely on cruise operators to take all reasonable precautions to safeguard and protect their health. Passengers are entitled to assume, as Mrs Karpik did, that cruise operators will take such precautions and that they will cancel the cruise if they are not able to do so. There was therefore no negligence by Mrs Karpik in going on the cruise.
860 Mrs Karpik was not in a position to enforce physical distancing on the vessel. There were also no published guidelines on physical distancing addressed to her or a person in her position. It is not established that a reasonable person in her position would not have participated in any activities on board the vessel that necessarily involved being in close proximity to other people. The same is true of face masks. Although she had awareness of the value of face masks, and took masks on board, in circumstances where no public guidance was directed to her or people in her position and, apparently, virtually no one else was wearing face masks, it is not established that she was negligent in not doing so.
861 In those circumstances, I find that Mrs Karpik was not contributory negligent with regard to her infection with COVID-19, and neither she nor Mr Karpik was negligent with regard to Mr Karpik’s infection with COVID-19.
862 The contributory negligence defence therefore fails.
863 Mrs Karpik claims damages for each of her causes of action. Personal injury damages are claimed in relation to the failures to comply with the ACL consumer guarantees and the claim in negligence. Mrs Karpik claims to have suffered three personal injuries, namely infection with COVID-19, suffering from Long COVID and an adjustment disorder with mixed anxiety and depressed mood. The heads of damage claimed by her for personal injuries are non-economic loss (pain and suffering and loss of amenities of life) and past and future medical expenses. No damages are claimed for economic loss or care.
864 As mentioned, no personal injury damages are claimed in relation to the contraventions of ACL s 18 as such damages are excluded by s 137C(1) of the CCA.
865 In addition to personal injury damages, Mrs Karpik claims damages for distress and disappointment as recognised in Scenic HCA and Baltic Shipping Co v Dillon. These damages are claimed on the consumer guarantee claims and the misleading or deceptive conduct claim. Distress and disappointment damages are not claimed on the cause of action in negligence.
866 Mrs Karpik claims personal injury damages under both the common law and in accordance with the CLA. That is because she submits that in the context of the claims for damages for failure to comply with the consumer guarantees in ACL ss 60 and 61, ACL s 275 does not pick up provisions of the CLA, including s 16 which relates to the quantification of damages for non-economic loss. On that submission, the common law would apply to the quantification of damages for the failures to comply with the consumer guarantees. However, as I have held that CLA s 16 is picked up and applied as surrogate federal law by ACL s 275 (see section D.2 above), damages for non-economic loss on the consumer guarantee and negligence claims must be assessed in accordance with CLA s 16.
867 The result of that is that Mrs Karpik can be awarded damages for non-economic loss only if the severity of the non-economic loss is at least 15% of “a most extreme case” (MEC). Also, the maximum amount of damages that may be awarded for non-economic loss is limited by CLA s 16 to an amount indexed under s 17. As at the date of assessment, being the date of judgment, that amount is $722,000 (Civil Liability (Non-economic Loss) Amendment Order 2023 (NSW)).
868 It is submitted on Mrs Karpik’s behalf that her injuries should be assessed as warranting a severity assessment of between 38% and 42% of an MEC, which equates to non-economic loss damages of between $274,360 and $303,240. She submits that if she is found not to have sustained Long COVID injury, damages for the adjustment disorder injury and COVID-19 infection injury should be assessed between 33% and 37% of an MEC, which would result in non-economic damages of between $238,260 and $267,140.
869 As already dealt with (in section C.2 above), it is in dispute whether Mrs Karpik contracted COVID-19. I have resolved that dispute in her favour. She therefore suffered that injury but, as will be seen, her symptoms were very mild.
870 It is not in dispute that Mrs Karpik suffered an adjustment disorder. What is at issue is the severity of that adjustment disorder, and in particular whether it was an aggravation of an existing adjustment disorder (which the respondents contend for) or whether her pre-existing adjustment disorder had resolved prior to the subject voyage with the result that it was a new adjustment disorder (which Mrs Karpik contends for). I will deal with that dispute, but however it is resolved, the symptoms of the adjustment disorder were relatively mild leading to, at best for her, a modest award of damages.
871 It is in dispute whether Mrs Karpik suffers from Long COVID. Part of the reason for that dispute arises from her relatively mild symptoms which had in any event resolved by the time of trial. I will deal with that dispute, but as with the adjustment disorder, at best for Mrs Karpik she would be entitled to a modest award of damages.
872 Taking those matters together, even finding that Mrs Karpik suffered all three of the personal injuries claimed by her, in my estimation she would not come close to the 15% of an MEC threshold and is therefore not to be awarded damages for non-economic loss arising from her personal injuries.
873 The principal issue with regard to the distress and disappointment damages arising from breach of the consumer guarantees and misleading and deceptive conduct concerns the extent to which any personal injuries suffered by Mrs Karpik, such as anxiety and depression, can be claimed under the distress and disappointment head of damages in the event that she is awarded no damages for non-economic loss arising from her personal injuries. It is contended on her behalf that such damages can be claimed under the distress and disappointment head, whereas the respondents contend that there is a clear line to be drawn between personal injuries damages and distress and disappointment damages, such that if no personal injuries damages are awarded no aspect of that loss can be claimed under the distress and disappointment head. I will come to dealing with that dispute.
874 Assessment of the personal injuries claimed by Mrs Karpik depends to one degree or another on her medical back-story. That is because in assessing non-economic loss, it is necessary to take into account (and remove from the calculation) anything resulting from pre-existing conditions: Varga v Galea [2011] NSWCA 76 at [51] (McColl JA, with whom Beazley JA and Handley AJA agreed). It is therefore necessary to go into that in some detail.
J.2 Mrs Karpik’s medical condition prior to the voyage
875 I have already explained why I must approach Mrs Karpik’s evidence with caution and look to see whether it is confirmed by, or is at least consistent with, other evidence and whether it is consistent with the overall probabilities and human experience. That is particularly so in relation to Mrs Karpik’s medical condition prior to the voyage. That is because it was demonstrated in cross-examination of her that she had been less than forthright in the disclosure of her prior medical condition, and she was evasive in answering questions on her medical history. The clinical notes of her consultations with doctors and what she was prescribed over time are therefore of central importance. There are two principal collections of clinical notes, both produced on subpoena. One is from the Crown Medical Centre Figtree where a number of GPs consulted by Mrs Karpik over the years have their rooms, and the other is from Mrs Karpik’s treating psychiatrist, Dr McMahon. [RESsub_CFM.003.001.0001; RESsub_DDM.001.001.0001]
876 Mrs Karpik had suffered from depression for several years prior to the cruise. Going back to at least December 2014, Mrs Karpik was treated for depression (T190:20). Initially she was prescribed the antidepressant Escitalopram (10mg) by her GP. [RESsub_CFM.003.001.0001 p 15] I note that Cipramil and Escitalopram seem to have been referred to interchangeably in evidence. The pros and cons of taking Cipramil are recorded as having been discussed, but Escitalopram was prescribed.
877 Mrs Karpik’s Escitalopram dosage was doubled (to 20mg) in June 2015, and renewed from time to time. [RESsub_CFM.003.001.0001 pp 16, 18, 19, 25, 27] In January 2018, Mrs Karpik visited her GP for “Advice and listening” and “Depressed.” She was “counselled.” Because of a complaint of weight gain from Escitalopram, Valdoxan (25 mg), a substitute antidepressant, was prescribed. [RESsub_CFM.003.001.0001 pp 28-29]
878 Mrs Karpik reported feeling better on Valdoxan in February 2018, although she was given counselling and support and discussed cognitive behavioural therapy. The Valdoxan prescription was renewed. [RESsub_CFM.003.001.0001 pp 29-30]
879 The Valdoxan prescription was increased to two tablets at night in April 2018 when Mrs Karpik presented as “distressed” with a number of family issues troubling her which required “advice and listening.” [RESsub_CFM.003.001.0001 pp 31-32]
880 Valdoxan was decreased again in January 2019 to one tablet at night, it being recorded that Mrs Karpik was “ready to decrease dose” and “ready to try to wean.” It was also recorded that Mrs Karpik reported that she was “beside myself” with issues regarding her daughters and in “terrible grief.” [RESsub_CFM.003.001.0001 p 42] In June 2019, it was recorded that Mrs Karpik was “considering stopping Valdoxan soon.” [RESsub_CFM.003.001.0001 p 45]
881 A consultation took place with Mrs Karpik’s GP, Dr Croker, on 11 February 2020. [RESsub_CFM.003.001.0001 p 55] It is important because of its proximity to the voyage, so it offers some insight into her state of health at that point. The “reason for visit” is recorded as being “depression.” The script for Valdoxan (25 mg), one tablet at night, was renewed. There is no indication of any discussion about going off the antidepressant, or further reducing the dose, or indeed what she reported with regard to her mental health on that occasion.
882 Mrs Karpik explained in evidence that the reason for the visit was that she had a cervical spine issue, and that she asked for the continued script because Valdoxan helped her sleep. She said that she was thinking of going off the Valdoxan after the cruise the following month (T197:45-198). I will come back to this as it bears on the question of whether at the time of the voyage Mrs Karpik still suffered from an adjustment disorder.
883 Mrs Karpik reported to Dr Samuels, and I accept, that she was continuously on antidepressant medication from at least 2014 through to the voyage in early 2020 (T404:33).
884 In May 2016, Mrs Karpik was prescribed Diazepam (2 mg) “as necessary for anxiety.” [RESsub_CFM.003.001.0001 pp 19-29] That prescription was renewed in March 2017. [RESsub_CFM.003.001.0001 pp 25-26] The prescription was recorded as being ceased in February 2018. [RESsub_CFM.003.001.0001 pp 29-30] It was commenced again with an increased dosage (5 mg) in August 2018 of “1/2 – 1 daily or bd prn for muscle spasm” – which I take to mean “half to one tablet daily or twice daily as and when required for muscle spasm.” [RESsub_CFM.003.001.0001 p 35] As Mrs Karpik had presented on that occasion with back and associated pain, it is to be inferred that the prescription was not for anxiety but rather for muscle spasms as recorded.
885 The Diazepam prescription was ceased again in June 2019. [RESsub_CFM.003.001.0001 p 45] It was commenced again on 27 March 2020, after the voyage, for “stress.” [RESsub_CFM.003.001.0001 p 57]
886 Mrs Karpik repeatedly denied in cross-examination that she had ever taken Diazepam for anxiety, but I reject that denial. There are repeated references to her being prescribed Diazepam for anxiety in the medical records, and there could have been no reason to renew the prescriptions if she had no need for the medication. I consider that the records are more likely to be reliable than Mrs Karpik’s memory or testimony.
887 On 4 June 2015, Mrs Karpik complained to her GP of suffering from “restless legs.” Her Escitalopram prescription was increased (20mg). [RESsub_CFM.003.001.0001 p 16] This appears to be the first record of Mrs Karpik suffering from restless leg syndrome (RLS), a nervous system disorder that creates an irresistible urge to move the legs in order to avoid uncomfortable or painful sensations. The symptoms typically worsen at night and can significantly impact the sleeper resulting in fatigue, concentration issues, and depression. [EXP_RES.001.001.0055 [66]]
888 There were further consultations with regard to Mrs Karpik’s RLS complaint in August 2015, in June 2016, March 2017, July 2017, April 2018 and, after the cruise, in June 2020 and March 2022. [RESsub_CFM.003.001.0001 pp 16, 25-26, 27, 31-32, 111; RESsub_DDM.001.001.0001 p 3] Her RLS was reported to have improved at consultations in May 2018 and September 2019 on account of her having stopped taking Escitalopram. [RESsub_CFM.003.001.0001 pp 32, 46] Mrs Karpik was prescribed Ropinirole for RLS, although it was ceased in May 2018 when the RLS initially eased. [RESsub_CFM.003.001.0001 p 32]
889 In March 2022, Mrs Karpik completed a survey in which she reported that several of the symptoms of RLS that she suffered from were “severe”, including discomfort, the need to move around, and mood disturbance. She reported that she suffered “moderate” tiredness or sleepiness and sleep disturbance from RLS, got only “slight relief” from moving around and that the impact of her RLS symptoms on her ability to carry out her daily affairs was “moderate.” Her overall score on the questionnaire was “severe” on a scale of none, mild, moderate, severe and very severe. [RESsub_CFM.003.001.0001 pp 284-5]
890 In June 2022, she reported that her RLS was worse compared to previously. [EXP_RES.001.001.0055 [66]] Indeed, Mrs Karpik told Dr Chen on 27 June 2022 that she had a history of RLS “which currently feels like it has worsened.” The RLS was causing her to have difficulty getting to sleep, and she even had difficulty watching television and had to repetitively stand up and sit down because of it. She also reported not feeling rested upon waking up, and would even on occasion fall asleep during the day if reading a book or watching television, or even when driving. [EXP_RES.001.001.0055 p 83]
891 I have found that Mrs Karpik was infected with COVID-19 as a consequence of Mr Karpik being infected with COVID-19 on the voyage, and that the respondents are liable for the damages suffered by Mrs Karpik as a result of that infection in her consumer guarantee claims and her negligence claim.
892 I have dealt above (in section C.2.2) at some length with Mrs Karpik’s symptoms from her COVID-19 infection. In summary, her symptoms were mild or, as submitted on her behalf in closing, “relatively minor.” She started suffering from headaches and diarrhoea from about 18 March. On 19 March, she was feeling unwell. On 21 March, she was very tired, had headaches and diarrhoea and did not sleep well. By 24 March, she had a “scratchy” throat. She appears to have recovered thereafter.
893 On any view, Mrs Karpik’s COVID-19 infection on its own can only contribute a very small amount to her damages.
894 As mentioned, each side of the case relies on the expert evidence of a psychiatrist. Mrs Karpik relies on Dr Parmegiani, and the respondents rely on Dr Samuels. In addition to their individual reports, Dr Parmegiani and Dr Samuels produced a joint report.
895 Dr Parmegiani prepared his first report following a one and a half hour clinical assessment with Mrs Karpik on 19 February 2021. At that time, and when he produced his first report, dated 5 March 2021, he was not provided with Mrs Karpik’s clinical records from her GP’s practice. Dr Parmegiani produced a second report, dated 19 August 2022, in response to the report of Dr Samuels. There are also two reports of, or letters from, Mrs Karpik’s treating psychiatrist, Dr Daryl McMahon, dated 14 January 2021 and 4 August 2022. [LAY_SKA.003.001.0018; LAY_SKA.003.001.0030]
896 Dr Samuels examined Mrs Karpik on 4 May 2022 for the purpose of preparing his report, which is dated 29 July 2022. Dr Samuels did have the benefit of Mrs Karpik’s clinical records at the time of preparing his report.
897 The psychiatrists agree that Mrs Karpik suffered from an adjustment disorder with mixed anxiety and depressed mood with clinically significant symptoms between March and June 2020. This diagnosis is consistent with that given by the applicant’s treating psychiatrist. [JNT.001.001.0078 [1.1]; LAY_SKA.003.001.0018 p 10]
898 The definition of an adjustment disorder in the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) is: [EXP_RES.001.001.0001 p 36]
A. The development of emotional or behavioural symptoms in response to an identifiable stressor(s) occurring within 3 months of the onset of the stressor(s).
B. These symptoms or behaviours are clinically significant, as evidenced by one or both of the following:
1. Marked distress that is out of proportion to the severity or intensity of the stressor, taking into account the external context and the cultural factors that might influence symptom severity and presentation.
2. Significant impairment in social, occupational, or other important areas of functioning.
C. The stress-related disturbance does not meet the criteria for another mental disorder and is not merely an exacerbation of a pre-existing mental disorder.
D. The symptoms do not represent normal bereavement.
E. Once the stressor or its consequences have terminated, the symptoms do not persist for more than an additional 6 months.
899 The DSM-5 goes on to specify that an adjustment disorder with mixed anxiety and depressed mood is a presentation where “a combination of depression and anxiety is predominant.”
900 Drs Parmegiani and Samuels agree that Mrs Karpik suffered from a recognised psychiatric illness as a consequence of her husband’s infection with COVID-19 during that period, and at least up until the time of Dr Parmegiani’s assessment on 19 February 2021, although by that time her symptoms were at a lesser severity. The psychiatrists agree that between March and June 2020 there was a likely impact on Mrs Karpik’s social functioning, but that thereafter her social functioning had returned to normal. [JNT.001.001.0078 [1.1], [3.1], [7.1]]
901 The question of whether or not Mrs Karpik suffered from a pre-existing psychiatric injury at the time that she was affected by the respondents’ wrongdoing is significant because, in the words of Dixon CJ in Watts v Rake [1960] HCA 58; 108 CLR 158 at 160, “[i]f the disabilities of the plaintiff can be disentangled and one or more traced to causes in which the injuries [she] sustained through the accident play no part, it is the defendant who should be required to do the disentangling and to exclude the operation of the accident as a contributory cause.” Also, “[t]he fact that the person injured was peculiarly susceptible to ensuing complications that would not in a normal person have followed from the injuries received, or that the person injured already had a disability which may be injury the more disabling … does not mean that damages are not to be assessed according to the circumstances of the particular case”: Watts v Rake per Menzies J at 164. See also New South Wales v Burton [2006] NSWCA 12 at [72] per Basten JA. The question of susceptibility to injury is subject to consideration of “normal fortitude” in CLA s 32 in respect of the common law claim in negligence, a matter which I have addressed in section F.3 above.
902 A respondent cannot be liable for a pre-existing injury that was not contributed to by its conduct, provided that the respondent has first discharged its evidential burden in adducing evidence of “both the pre-existing condition and its future probable effects or is actual relationship to that incapacity … [to] … establish with some reasonable measure of precision, what the pre-existing condition was and what its future effects, both as to their nature and their future development and progress, were likely to be.” Once done, it is for the plaintiff, on all the evidence, to satisfy the court of the extent of the injury caused by the defendant’s negligence. See Purkess v Crittenden [1965] HCA 34; 114 CLR 164 at 168 per Barwick CJ, Kitto and Taylor JJ.
J.4.2 Exacerbation of a pre-existing psychiatric injury, or a new injury?
903 The psychiatrists agree that the definition of adjustment disorder involves resolution within six months of the causal stressor ending. Dr Parmegiani is of the view that Mrs Karpik’s previous stressors ended more than six months before the voyage in question, with the result that she could not be regarded as having chronic adjustment disorder at that time. [JNT.001.001.0078 [2.1]]
904 In contrast, Dr Samuels obtained a history suggesting that Mrs Karpik’s mood state was stable in the months before the voyage, but that her history of mood instability was likely to have been present before 2014 when she first consulted her GP and received treatment. Her history indicated recurrent depression and anxiety which was clinically significant in that she had required antidepressant treatment since 2014. He formed the impression that Mrs Karpik had long-standing vulnerability to anxiety and depression. Her symptoms were not severe enough to meet the definition of major depression and were more in keeping with a reactive-type depression or minor depression. [JNT.001.001.0078 [2.2.2]ff]
905 Dr Samuels opined that Mrs Karpik suffered from chronic and recurrent adjustment disorder-type symptoms with fluctuating depression and anxiety. These symptoms initially related to enduring threats to her husband and ongoing concerns about her daughter. In addition, symptoms recurred from time to time in relation to periods of study, employment and family responsibilities. Such episodes appear generally to have been of short duration and responsive to medication adjustments. [JNT.001.001.0078 [2.2.4]]
906 Dr Samuels believes that these episodes are in keeping with a diagnosis of recurrent adjustment disorder. An alternative diagnosis is persistent depressive disorder with anxious distress, given her continuous need to manage her symptoms with antidepressants since 2014. [JNT.001.001.0078 [2.2.5]]
907 For those reasons, Dr Samuels disagrees with Dr Parmegiani that her depressive and anxiety symptoms can be regarded as a distinct new condition and not an exacerbation of a pre-existing condition. Dr Samuels nevertheless agrees that Mrs Karpik’s adjustment disorder was well-controlled prior to the voyage, but that between the period March-June 2020 she experienced a relapse of clinically significant depressive and anxiety symptoms. When her husband became ill, she suffered a recurrence of depressive and anxiety symptoms as a consequence of her pre-existing vulnerability to psychiatric disorder. [JNT.001.001.0078 [2.6]-[2.7]]
908 Dr Parmegiani, in turn, acknowledged that in the past Mrs Karpik had experienced episodes of depression and anxiety diagnosable as adjustment disorders, in response to previous stressful events. He also noted that Mrs Karpik demonstrated features of high trait anxiety in her personality, which would make her vulnerable to such episodes. [JNT.001.001.0078 [2.3]] He, however, believes that the absence of documented symptoms of adjustment disorder in 2019 in the clinical records, and Mrs Karpik’s own assertion at his assessment that prior to the cruise she had been clinically well and had experienced no functional impairment, suggest that by then the condition of adjustment disorder was no longer diagnosable. [JNT.001.001.0078 [2.5]]
909 Dr Parmegiani consequently believes that the episode of adjustment disorder that Mrs Karpik experienced after the cruise and its aftermath was a new episode of adjustment disorder, which would not have occurred but for the stressful events that followed the cruise. He says that the episode was not a relapse of a previous condition, as that condition had resolved. [JNT.001.001.0078 [2.6]]
910 Although Dr Samuels acknowledged that Mrs Karpik’s clinical records and self-report suggest that her depressive and anxiety symptoms were controlled during 2019 and prior to the voyage, his view is that her recurrent adjustment symptoms or persistent depressive symptoms were controlled by the antidepressant she was prescribed. For that reason, he says she was not necessarily in complete remission and her future risk of becoming depressed and anxious in the face of new stressors like the events on the cruise and following was heightened by this underlying vulnerability. [JNT.001.001.0078 [2.7]]
911 The result is that the difference between the psychiatrists is that Dr Parmegiani takes the view that Mrs Karpik’s previous adjustment disorder had resolved by the time of the voyage, although she has high trait anxiety in her personality which make her more vulnerable to experiencing episodes of depression and anxiety diagnosable as adjustment disorders, and Dr Samuels says that her previous adjustment disorder had not resolved but was under control of medication, meaning that she was not in complete remission and retained a future risk of becoming depressed and anxious in the face of new stressors. That difference between the psychiatrists is not particularly significant.
912 I am mindful that Mrs Karpik was on antidepressant medication continuously from 2014, and was still on that medication at the time of the voyage. I acknowledge that in 2019 she had discussions with her doctors in which she was considering going off the antidepressant, but she had not reached that point prior to the voyage and the reason for her visit to her doctor in February 2020 being recorded as “depression” is troubling. Insofar as her explanation for continuing on the antidepressant at that time, namely that it helped her sleep, is concerned, I note that none of the records reflect any support for the idea that she was at any time on an antidepressant specifically for that purpose. Although, as Dr Parmegiani explained in cross-examination, I accept that poor sleep can be a symptom of depression (T382:10). Mrs Karpik had numerous prescriptions over time for Temazepam expressly to help her sleep, including in September 2019. [RESsub_CFM.003.001.0001 pp 32, 46, 309, 312, 313, etc] She also told Dr McMahon in April 2020 that she had been taking Valium in the past to help her sleep (although I expect that she was thinking of Temazepam), and that she had a history of depression and had been taking Valdoxan. [RESsub_DDM.001.001.0001 p 3] I am therefore sceptical of her explanation for staying on the antidepressant. I infer that she stayed on the antidepressant in order to manage depression.
913 That said, during cross-examination, Dr Samuels accepted that Mrs Karpik was “obviously better by the end of ‘19”, and that when she went on the cruise she was “functioning quite well and not depressed or anxious” and “her mental state was well controlled” (T416:26-416:30). Although the February 2020 prescription was provided only a month before the cruise, Dr Parmegiani’s evidence is that it is not uncommon for patients to remain on antidepressant medication prescribed by a GP, even at times when the medication may no longer be clinically indicated, for example, by the presence of acute anxiety or depressive symptoms (T400:31-401:14). Also, Dr Samuels explained that antidepressants can have a quite serious withdrawal effect so ceasing to take them needs to be done thoughtfully and carefully (T405:5). Those observations support the conclusion that just because Mrs Karpik was still on an antidepressant at the time of the voyage does not mean that she was still actually suffering from depression in the form of an adjustment disorder.
914 It is not possible for me to say with particular confidence whether Mrs Karpik’s recurring adjustment disorder symptoms were resolved prior to the cruise because of her antidepressant medication, or whether her symptoms would have been present in the absence of the medication. However, I do accept Dr Parmegiani’s evidence that it is not uncommon for patients to remain on antidepressant medication, even at times when that medication may no longer be clinically indicated. Individuals may continue to take antidepressant medication as a precautionary or preventative measure in the context of a recurring vulnerability to anxious and depressive symptoms.
915 A distinction is required to be drawn between a pre-existing vulnerability to causal life stressors and a pre-existing recognised psychiatry injury. In Mrs Karpik’s case, I do not consider that the routine but variable prescription of antidepressant medication is necessarily an indication of a pre-existing adjustment disorder in the period immediately prior to the cruise. Ultimately, Dr Samuels expressed the position well as follows, which I accept (T416:30-417:4):
… in the face of stress, she decompensated again.
… it is hard to know when an adjustment disorder ends because often the stressor doesn’t actually disappear and these are chronic enduring sort of stressors.
… I think she’s always vulnerable. I mean, by her history, when something goes wrong in her life, she tends to develop depressed and anxiety symptoms. So I think she was quite stable on her 25 mg of Valdoxan, which she may or may not have been taking. She was stable at that point. But the vulnerability to becoming depressed and anxious is always there, and it will still be there into the future, because that is one thing we can glean about the history, and the best predictor of future risk is the past.
916 As the applicant submits, and I accept, although there was mention of “depression” in the clinical notes for February 2020, there were no clinical notes regarding any particular stressors, such as family concerns, after 2019 and prior to the voyage. It is in this context that Dr Samuels stated that what happened in 2019 was “a bit speculative” (T416:33).
917 Taking into account the review of Mrs Karpik’s GP clinical records and expert evidence, I consider that despite her having a pre-existing vulnerability to anxiety and depressive symptoms, Mrs Karpik’s pre-existing adjustment disorder was likely in remission by the time of the Ruby Princess cruise and that her post-cruise adjustment disorder constituted a fresh diagnosis. Although Dr Parmegiani’s original opinion was hampered by the fact that he had not been given access to the GP clinical records, once he was given access to those records, and even following his engagement in conclave with Dr Samuels and detailed cross-examination, he maintained his opinion with adequate explanation.
918 Thus, insofar as Mrs Karpik’s claim for damages arising out of her diagnosed personal injury of adjustment disorder following the voyage is concerned, the critical issue is to assess how severely she was affected by the relevant events of and following the voyage. In that regard, it is to be noted that prior to the voyage Mrs Karpik and her GPs had not found it necessary for her to consult a psychologist or a psychiatrist, but that changed with the event of and following the voyage. I accept Dr McMahon’s opinion expressed in his first report that his treatment of her would not have been necessary if her husband had not become unwell with COVID-19 and required ICU admission with a near death experience – those events were a substantial contributing factor to Mrs Karpik’s adjustment disorder. [LAY_SKA.003.001.0018 p 11]
J.4.3 Effects of adjustment disorder
919 Mrs Karpik described the period of time when Mr Karpik was hospitalised and she was required to stay at home isolating as “terribly distressing as [she] knew that it could be the beginning of the end for Henry, and that [she] was not able to be with him.” [LAY_SKA.001.001.0083 [172]] Mrs Karpik described the day of the conference with hospital staff on 27 March 2020 when she was informed that Mr Karpik only had a 10% chance of survival as “the worst day of [her] life” as she grappled “with the idea of never seeing Henry again.” [LAY_SKA.001.001.0083 [185]] She described the period from when Mr Karpik was admitted to hospital on 21 March to about 4 April 2020 as “extremely difficult” and a period during which she “was in a heightened state of distress.” [LAY_SKA.001.001.0083 [251]] The process of observing Mr Karpik regaining consciousness after she was allowed to visit him in hospital from 12 April 2020 was confronting, and she described his circumstances as “tragic.” [LAY_SKA.001.001.0083 [196]] I accept all that evidence. It is compelling and consistent with human experience and the probabilities.
920 After consulting her GP on 16 April 2020, Mrs Karpik was referred to a psychiatrist, Dr McMahon, for trauma counselling. On 23 April 2020, Mrs Karpik consulted Dr McMahon and described the events she had experienced on the Ruby Princess and afterwards as an “emotional rollercoaster” and that “[s]he feels at times that the situation is hopeless” [LAY_SKA.001.001.0083 [253]; RESsub_DDM.001.001.0001 p 3] On 24 April 2020, Dr McMahon reported to Mrs Karpik’s GP that “[d]iagnostically I believe [Mrs Karpik] has trauma related anxiety symptoms” in the context of “her husband contracting Covid 19 on the ill-fated Ruby Princess cruise.” [RESsub_DDM.001.001.0001 p 9]
921 On 8 May 2020, Mrs Karpik had her second consultation with Dr McMahon during which she told him that Mr Karpik had made “good progress” but that she was having “sleep problems.” On 15 May 2020, during her third consultation, Mrs Karpik informed Dr McMahon that Mr Karpik would be discharged home soon and that her sleep was “a bit better.” [RESsub_DDM.001.001.0001 p 4] During a consultation on 1 June 2020, Mrs Karpik told Dr McMahon that Mr Karpik’s rehabilitation was going well, that she was occasionally struggling with sleep, and that she was talking to friends again and had returned to work.
922 On 15 June 2020, Mrs Karpik informed Dr McMahon that her husband was frustrated by his weakness and that her own breathing had not improved. [RESsub_DDM.001.001.0001 p 4] During a consultation on 29 June 2020, Mrs Karpik informed Dr McMahon of the various medical investigations being conducted into her shortness of breath and that Valdoxan was helping to calm her.
923 On 20 July 2020, Mrs Karpik informed Dr McMahon that her medical investigations were coming back “normal” and that she was “[o]therwise gradually getting back to normal”, and that she and Mr Karpik had been on a holiday to Coffs Harbour and had “had a good time.” At this time, her Valdoxan dose remained 50mg (2 tablets) per day.
924 Mrs Karpik gave evidence that during that holiday to Coffs Harbour she had done lots of walking (T227:20). That arose from the record of a consultation she had with her GP on 14 July 2020 which recorded that she had done “OK” on holiday with lots of walking, “long walks but not strenuous”, with no chest pain or shortness of breath. [RESsub_CFM.003.001.0001 p 70]
925 On 3 September 2020, Mrs Karpik told Dr McMahon she was “[d]oing well mostly”, walking, back to part time work and was continuing Valdoxan 50mg per night. Mrs Karpik informed Dr McMahon on 3 December 2020 that she was pleased with her progress but that her breathing was still impaired, and in January 2021 informed him that she was still short of breath on exertion and was “having some name finding difficulties at times and word finding when under pressure and stress.” At that consultation Dr McMahon noted that Mrs Karpik “[f]eels she is not as confident as she was before Covid.” [RESsub_DDM.001.001.0001 p 5]
926 Dr Parmegiani reports that Mrs Karpik told him that over time her mood symptoms fluctuated, and that she began to feel better by December 2020. She said that by this time, she had stopped ruminating on the situation and the worst possible potential outcomes. However, in December 2020, Mrs Karpik’s then 95-year-old mother-in-law came to visit them during which time she was admitted to the COVID-19 ward of Wollongong Hospital, which brought back memories of Mr Karpik’s illness and caused Mrs Karpik to become more tired, anxious and emotionally labile. However, she reported that following her mother-in-law’s recovery, her symptoms improved again. [EXP_SKA.003.003.0276 pp 18, 22]
927 In February 2021, Dr McMahon also noted that Mrs Karpik had reported a rekindling of emotions and anxieties surrounding her mother-in-law being admitted to Wollongong Hospital (where Mr Karpik had been hospitalised). In May 2021, Dr McMahon reported that Mrs Karpik was going “pretty well” and that she was “busy and coping well with things, still taking Valdoxan 50mg nocte.” [RESsub_DDM.001.001.0001 p 5]
928 At the time of Dr Parmegiani’s assessment in February 2021, Mrs Karpik reported that she continued to experience intrusive memories of and flashbacks to Mr Karpik’s hospitalisation. She stated that she was tense, easily startled and irritable, and was triggered by the hospital’s “hold” music on the telephone. She reported that when triggered by the memories of Mr Karpik’s hospitalisation, she also experienced panic attacks characterised by tachycardia, tremors, sweating and shortness of breath. She described her mood as “mostly down” and described decreased reactivity and lack of enjoyment. She stated that she sometimes felt overwhelmed by her situation, and sometimes blamed herself for her predicament, reflecting that “we should not have gone on that ship.” [EXP_SKA.003.003.0276 pp 18-19]
929 Mrs Karpik reported to Dr Parmegiani in February 2021 that she was able to fall asleep and rise quickly, but still felt tired. She described her appetite as “not bad” and noted that she was now exercising and ate three meals per day, although she had recently lost some interest in cooking. She reported that her energy and motivation levels remained low and that her libido was probably reasonable. [EXP_SKA.003.003.0276 p 19]
930 As at the time of Dr Parmegiani’s assessment, she was able to perform household duties, enjoyed company and caught up with her friends regularly, enjoyed watching television, followed the news, experienced no difficulties with respect to travel or mobilisation, and was able to get on well with her friends and family. She reported that her memory and concentration were reasonably good, although she sometimes experienced trouble remembering names. [EXP_SKA.003.003.0276 p 20]
931 Dr Parmegiani concluded that Mrs Karpik’s prognosis should be regarded favourably provided her situation remains stable with respect to her husband’s and mother-in-law’s health. [EXP_SKA.003.003.0276 p 22]
932 During Dr Samuels’s assessment of Mrs Karpik in May 2022, she reported to him that her mood was “good”, that she was pleased with herself, and she was able to cope with the recent death of her mother-in-law although it had been very triggering for her when her mother-in-law was in a COVID-19 care area when she was hospitalised. Mrs Karpik reported that her sleep varied and that she was “not a great sleeper” in the past. She said that she had dreams but did not describe nightmares, did not experience intrusive recollections of what happened, and that she “was quite good at distracting herself and focussing on other issues.” She reported that she was attempting to de-sensitise herself and that she had been able to take her grandson on a trip to the Rocks area in Sydney, where she thought she would never go back to. She told Dr Samuels that she only feels anxious when she reflects on what has happened, and feels distressed if she reads materials related to the Ruby Princess cruise. She reported that she and her friends had been able to make light of the events surrounding the Ruby Princess cruise through use of humour. At the time of the assessment, Mrs Karpik was still taking two Valdoxan per day.
933 Mrs Karpik reported to Dr Samuels that working “has been very good for her” and that her mental health improved when she was able to return to work in June 2020. Initially she experienced some “brain fog”, was not coping all that well, and limited her hours, but things improved within a period of months. Mrs Karpik reported to Dr Samuels that she did not return to her “normal role function” until the end of 2020, and that as at the time of assessment in May 2022, she was still not quite working at her previous level. [EXP_RES.001.001.0001 [30]]
934 Dr Samuels concluded that by the time of his assessment of Mrs Karpik on 4 May 2022, the majority of her psychological symptoms had resolved, she was back to her previous level of psychological functioning, and that her adjustment disorder was in remission on her medication regime at that time. Dr Samuels opines that her prognosis is very favourable, but given her medical history, it is likely that she will need to continue to take anti-depressant/anti-anxiety medication into the future. [EXP_RES.001.001.0001 [55]-[56], [67]-[68], [71], [80]]
935 Mrs Karpik reported to Dr Samuels in May 2022 that she was “trying to keep very busy” and that she was back to her “normal function” at work although no longer travels to Bowral or Nowra for work. She reported that she was socialising, had hobbies, exercises, was getting on well with her husband and family, and that her concentration was “okay.” [EXP_RES.001.001.0001 [58]]
936 Dr Samuels opined in July 2022 that he would regard Mrs Karpik as being back to her psychological baseline, that is “having a propensity to anxiety but with her symptoms controlled on medication which is likely to be reduced to its prior dosage level” and currently having no specific requirement for psychological treatment. He did not believe that Mrs Karpik requires any specific psychiatric or psychological treatment in relation to the Ruby Princess cruise. [EXP_RES.001.001.0001 [91]]
937 In her third affidavit, dated 2 October 2022, Mrs Karpik reported that she had found the period from June 2020 to the end of that year very difficult, in part because of the time that she had to spend caring for Mr Karpik and in part because of having to do most of her work as a Visitor online via Zoom. Thereafter, things started to settle down a bit. She gradually built up the amount of work that she was doing as Mr Karpik became more independent. Thus, by October 2022, Mrs Karpik’s workload was similar to what it had been before the voyage. [LAY_SKA.003.001.0039 [36]]
938 In summary, I have found that Mrs Karpik, a person vulnerable to experiencing depressive and anxiety symptoms, suffered from a new adjustment disorder as a consequence of the voyage and its aftermath. From March to June 2020, Mrs Karpik was very distressed and depressed and required professional psychiatric treatment, which she received from Dr McMahon. Her trauma-related symptoms were medically significant, although Mrs Karpik did not report ever experiencing thoughts of self-harm or suicidal ideation. [EXP_SKA.003.001.0604 p 9; EXP_SKA.003.003.0276 p 18] Fortunately, Mrs Karpik’s depressive and anxiety symptoms did not remain at an acute level for an extended period. Mrs Karpik’s mental health improved from June 2020 when her social functioning returned to normal and she has returned to her baseline state of psychological health and appears to be working and socialising at the level that she was prior to the cruise. By early 2021, the adjustment disorder had essentially resolved with only minor symptoms thereafter. Without any intention of minimising the trauma that Mrs Karpik suffered, particularly during the time of Mr Karpik’s hospitalisation, I find that, overall, the psychiatric illness experienced by Mrs Karpik in the form of her adjustment disorder was of moderate severity and relatively short duration.
939 Mrs Karpik claims that as a consequence of being infected with COVID-19, she developed a condition known as Long COVID, but which is also referred to by other names including Post-COVID. This condition was diagnosed by the US-based rehabilitation physician, Dr Herrera, as an expert witness. Dr Herrera’s diagnosis is in dispute, and the respondents contend that it should be rejected. Dr Herrera undertook a two-hour long consultation with Mrs Karpik on 7 December 2021. That interview was conducted remotely by video, which is to say that Dr Herrera did not conduct a physical examination of Mrs Karpik. Dr Herrera and one of his colleagues also administered multiple patient-reported outcomes questionnaires. Dr Herrera produced three reports, dated 4 March 2022, about 29 August 2022 (it is undated but is an annexure to his affidavit of that date) and 23 October 2022. [EXP_SKA.003.003.0315; EXP_SKA.003.003.0370; EXP_SKA.004.001.0001; EXP_SKA.003.003.0315 p 8]
940 The respondents rely on the expert evidence of Dr Chen, a US-based pulmonary and critical care physician. Dr Chen interviewed Mrs Karpik, also remotely, on 27 June 2022. That was nearly seven months after Dr Herrera’s interview of Mrs Karpik, which may account, at least to some extent, for the differences in their conclusions. Dr Chen’s opinion is that it is not possible to say that Long COVID is the cause of Mrs Karpik’s symptoms which Dr Herrera identified as likely constituting Long COVID. Dr Chen produced a report dated 28 July 2022. [EXP_RES.001.001.0055]
941 The principal issues for determination are the following:
(1) Should Dr Herrera’s reports be rejected (ie, not admitted as evidence or otherwise simply rejected as unreliable) on the basis that Dr Herrera does not possess the relevant “specialised knowledge” required by s 79 of the Evidence Act 1995 (Cth) with the result that his opinion is not admissible on account of being excluded by s 76 of the Evidence Act?
(2) If Dr Herrera’s reports are not rejected, is the evidence of Dr Chen nevertheless preferable, including because the assumptions on which Dr Herrera’s reports are based, namely Mrs Karpik’s symptoms, were not (adequately) established and Dr Herrera’s reports do not reveal the detailed analysis that he accepted is required in order to exclude alternative diagnoses before concluding that someone has Long COVID, or, they do not contain an adequate explanation or exposition of the basis for his opinion?
942 Before turning to those questions, it is helpful to identify the areas of agreement and disagreement between Drs Herrera and Chen as expressed in their joint report.
943 Drs Herrera and Chen met in conclave and produced a joint report dated 13 September 2022 in which they recorded their areas of agreement and disagreement. [JNT.001.001.0086]
944 As at the date of their joint report, there were two relevant, although different, definitions of Long COVID.
945 The CDC definition was as follows:
Post-COVID Conditions: Some people who have been infected with the virus that causes COVID-19 can experience long-term effects from their infection, known as post-COVID conditions (PCC) or long COVID. … Post-COVID conditions are a wide range of new, returning, or ongoing health problems that people experience after being infected with the virus that causes COVID-19. Most people with COVID-19 get better within a few days to a few weeks after infection, so at least four weeks after infection is the start of when post-COVID conditions could first be identified. Anyone who was infected can experience post-COVID conditions. Most people with post-COVID conditions experienced symptoms days after first learning they had COVID-19, but some people who later experienced post-COVID conditions did not know when they got infected.
946 The WHO definition was as follows:
Post COVID-19 condition occurs in individuals with a history of probable or confirmed SARS CoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms and that last for at least 2 months and cannot be explained by an alternative diagnosis. Common symptoms include fatigue, shortness of breath, cognitive dysfunction but also others and generally have an impact on everyday functioning. Symptoms may be new onset following initial recovery from an acute COVID-19 episode or persist from the initial illness. Symptoms may also fluctuate or relapse over time.
947 There are two main differences between the CDC and WHO definitions. First, the CDC states that Long COVID should be considered in those with symptoms that continue for at least four weeks after infection, whereas the WHO states that symptoms should be present at least three months after the onset of COVID-19 and be present for at least two months. Secondly, the CDC does not state that alternative diagnoses need to be ruled out, whereas the WHO definition states that they do. Neither of these differences is material in the present case because the experts agreed that ruling out alternative diagnoses is necessary when evaluating someone for Long COVID, and Mrs Karpik’s relevant symptoms had lasted for more than three months. [JNT.001.001.0086 [3]-[5]]
948 Although Dr Herrera accepted in the joint report that ruling out alternative diagnoses for presenting symptoms was necessary when evaluating for Long COVID, he was cross-examined further in relation to that and accepted that “the exploration and exclusion of alternative diagnoses is an important part of the task of robustly diagnosing Long COVID” and that another important part of the task “is conducting a granular review of a patient or a person’s medical history” (T633:38-42). That is at least in part because there is currently no diagnostic test for Long COVID (T634:14).
949 The WHO definition refers to common symptoms including fatigue, shortness of breath (also referred to as dyspnoea), cognitive dysfunction (or impairment), “but also others.” Dr Herrera identified other symptoms including, relevantly, light-headedness (also referred to as dysautonomia), post-exertional malaise, insomnia and other sleep difficulties, and pain. [EXP_SKA.003.003.0315 p 11]
950 I turn now to the question of Dr Herrera’s specialised knowledge.
J.5.3 Dr Herrera’s specialised knowledge
951 It is not in dispute that s 79 of the Evidence Act requires, for the admissibility of opinion evidence, that the expert’s evidence explains how their field of “specialised knowledge” in which they are an expert by reason of “training, study or experience”, and on which the opinion is “wholly or substantially based”, applies to the facts assumed or observed so as to produce the opinion propounded. It is also the case that those requirements might, in any particular case, be very quickly and easily met – in the case of a specialist medical practitioner expressing a diagnostic opinion in their relevant field of specialisation, little explicit articulation or amplification may be required once the witness has described their qualifications and experience and has identified the subject matter about which the opinion is proffered: Dasreef Pty Ltd v Hawchar [2011] HCA 21; 243 CLR 588 at [37] per French CJ, Gummow, Hayne, Crennan, Kiefel and Bell JJ.
952 The respondents’ principal contention is that Dr Herrera lacks relevant specialist knowledge in diagnosing Long COVID, as opposed to treating and rehabilitating someone who has Long COVID.
953 As was mentioned in section B.3, but worth repeating here, Dr Herrera is a physician in the field of Physical Medicine and Rehabilitation and at the time of trial was the System Chair of Physical Medicine and Rehabilitation within the Department of Rehabilitation and Human Performance for the Mount Sinai Health System in New York. He was also a physician in the Mount Sinai Center for Post Covid Care and a Professor at the Icahn School of Medicine at Mount Sinai, New York. Dr Herrera’s role includes the care of patients with musculoskeletal injuries and concussions, education of residents and fellows, and administrative duties as chair for all eight hospitals in the Mount Sinai Health System. [EXP_SKA.003.003.0315 pp 3, 7]
954 At the Mount Sinai Center for Post Covid Care, he cared for hundreds of patients with Long COVID. His team created treatment protocols for patients who experience fatigue, shortness of breath, dysautonomia (ie, dizziness and fainting) and cognitive impairment. Dr Herrera’s curriculum vitae and his professional webpage show him to have a long history of specialisation in rehabilitative and sports medicine. [EXP_SKA.003.003.0315 p 7, 38ff; MSC.020.142.0001] He explained that he has a certified speciality in physical medicine and rehabilitation, and a sub- specialisation in primary sports care medicine. [EXP_SKA.004.001.0001 p 6]
955 Dr Herrera worked on the frontline caring for patients who had been admitted to the Mount Sinai hospital with COVID-19 starting at the end of March 2020. The hospital’s rehabilitation units were converted into acute COVID units. Dr Herrera led the first team to care for severely ill patients. He tended to the medical needs of the patients, including monitoring and treating the patients’ acute symptoms. He followed daily vitals and bloodwork which required the appropriate adjustment of medications, vent settings and other patient needs that required attention. His duties included resuscitating patients who required emergency attention, doing chest compressions, communicating with families, and doing admissions. [EXP_SKA.004.001.0001 p 6] His practice consists mainly of treating patients with Long COVID. [EXP_SKA.004.001.0001 p 7]
956 Dr Herrera’s list of publications included in his CV shows that he has published principally on concussive injury, shoulder injury and back and spinal problems, with the only peer-reviewed original contribution relating to COVID-19 being an article in the American Journal of Physical Medicine & Rehabilitation in June 2020 entitled “Adapting to the Coronavirus Disease 2019 Pandemic in New York City.” By its title, it does not appear that that article deals with the diagnosis of Long COVID, and in any event Long COVID is not likely to have been known as a phenomenon in June 2020. [EXP_SKA.003.003.0315 p 44]
957 I note, however, that in his second and third reports, Dr Herrera references (and annexes to his third report) an article by him and others submitted in June and published in September 2021 in PM&R, the journal of the American Academy of Physical Medicine and Rehabilitation, entitled “Multidisciplinary collaborative consensus guidance statement on the assessment and treatment of fatigue in postacute sequelae of SARS-CoV-2 infection (PASC) patients.” As its title suggests, the article deals with questions of assessment for and treatment of Long COVID – referred to at that time as PASC. [EXP_SKA.003.003.0315 p 15 [3]; EXP_SKA.004.001.0001 p 14] The article includes a discussion of common symptoms of patients who reported having Long COVID, and a review of studies on the identification of Long COVID. [EXP_SKA.004.001.0001 p 15]
958 Although Dr Herrera accepted in cross-examination that his reports do not explain that he has experience in diagnosing Long COVID (T649-650), he explained that in the Long COVID clinic in which he works “on the frontline” he both diagnoses and treats Long COVID (T649:45, 650:38, 651:36, 654:24, 664:20). He explained that there is a long waitlist of patients for the clinic. Typically, when they come in they have been symptomatic for a long period of time. They are given diagnostic tests, an extensive history is taken and a physical examination is undertaken to come to a diagnosis. Dr Herrera is involved in that process (T652:36-653:9). Dr Herrera explained that at the clinic a multidisciplinary team involving multiple specialities is involved in Long COVID diagnosis (T674:4-14). That is an approach that counsel for the respondents endorsed, and which Dr Herrera accepted (T637:11).
959 It is also to be borne in mind that the evidence is that Long COVID is a developing discipline – the medical understanding of the syndrome that constitutes Long COVID continues to evolve with ongoing studies. There are presently no diagnostic tests for Long COVID. The state of knowledge is in flux, and learning in the area is nascent (T638:15).
960 In the circumstances, I am satisfied that Dr Herrera has the necessary specialised knowledge based on his training, study and, in particular, his experience, to diagnose Long COVID and consequently to express an opinion on a Long COVID diagnosis for Mrs Karpik. As indicated, he has published in the area, and he has been on the frontline in diagnosing (as a member of a multidisciplinary team) Long COVID in people presenting to the Mount Sinai Center for Post Covid Care with constellations of symptoms consistent with Long COVID.
961 I therefore reject the first basis advanced for the rejection of Dr Herrera’s reports.
J.5.4 Did Mrs Karpik have Long COVID?
962 Dr Herrera acknowledged that the diagnosis of Long COVID is reliant on the use of tools that involve the subjective reporting of symptoms. That is to say, Dr Herrera’s identification of symptoms relied almost entirely on what Mrs Karpik reported to him in the video interview on 7 December 2021. Those symptoms were the following: [EXP_SKA.003.003.0315 p 8ff]
(1) shortness of breath on exertion, in respect of which Mrs Karpik reported that her breathlessness made it more difficult to engage in social activities such as walking with her family as she becomes breathless and has to stop, and work because becoming breathless while talking over the phone leads to difficulties in having work conversations;
(2) fatigue;
(3) post-exertional symptom exacerbation or post-exertional malaise, which is distinct from fatigue and relates to a significant worsening of symptoms following exertion;
(4) a general aching pain in both of her legs;
(5) dysautonomia, presenting as dizziness and feelings of pre-syncope (ie, feeling as though she is going to faint) when moving from sitting to standing, especially after prolonged sitting;
(6) cognitive impairment, primarily affecting her speech and language abilities – difficulty with naming objects, places and people and difficulty with communicating verbally;
(7) hair feeling fine in texture; and
(8) difficulty with sleeping throughout the night, although Mrs Karpik acknowledged that her sleep disturbances may be related to the stressful experiences and trauma of the preceding 18-24 months.
963 Based on Mrs Karpik reporting those symptoms, Dr Herrera formed the opinion that Mrs Karpik met the diagnostic criteria for Long COVID. [EXP_SKA.003.003.0315 p 10; EXP_SKA.003.003.0370 [3]]
964 Dr Herrera expressed the view in relation to pre-existing conditions that “[i]t is also not clear that there are any pre-existing injuries or conditions that pre-disposes (sic) Mrs Karpik to Long COVID.” [EXP_SKA.003.003.0315 p 13] In cross-examination, he accepted that that statement with regard to predisposition is a very different thing to whether or not pre-existing injuries or conditions caused Mrs Karpik to suffer from particular symptoms (T662:11).
965 Dr Herrera also accepted that it is a critical part of Long COVID diagnosis to explore not only the possibility of pre-existing conditions that may contribute to the constellation of presenting symptoms, but also to identify any new conditions that may be playing the same role (T638:41-639:3).
966 In Dr Herrera’s first report, there is no reasoning justifying any exclusion of other possible causes for the symptoms that Mrs Karpik complained of. Indeed, Dr Herrera accepted that his first report does not specifically address any of the pre-existing conditions of Mrs Karpik and the role that they might have played in causing any of her symptomology (T662:28).
967 That deficit was sought to be fixed in Dr Herrera’s second report. In response to Dr Chen stating in his report that it is not described by Dr Herrera how he excluded potential alternative diagnoses, Dr Herrera said the following: [EXP_SKA.003.003.0370 [32]]
My process for ruling out potential alternative diagnoses, both diagnosed and undiagnosed, was through a combination of my examination of Mrs. Karpik, as well as a rigorous review and contrasting of Mrs. Karpik’s past medical history prior to the cruise, and in the period after the cruise. Prior to the cruise, Mrs. Karpik had specific, diagnosed comorbidities that I systematically ruled out:
(a) Depression: I ruled out depression because a psychiatrist report from Dr Parmegiani ruled out the possibility that Mrs. Karpik’s depression was causing any level of functional impairment in her daily life. In addition, Mrs. Karpik was also screened for depression using the PHQ-2 instrument, and she screened negative which is consistent with someone who has well-controlled depression. Most likely this is due to the fact that Mrs. Karpik has received medical management of her depression and as such it can be ruled out as a potential cause of her Long COVID symptoms.
(b) Obesity: Mrs. Karpik has steadily gained weight over the years. I ruled out obesity as a cause of Mrs. Karpik’s symptoms because her gradual weight gain over time is not correlated with the severity of her symptoms. For instance, prior to the cruise, Mrs. Karpik had no specific symptoms that were related to her obesity. Immediately following the cruise and her acute COVID-19 infection, Mrs. Karpik developed symptoms consistent with Long COVID. Over one year after her COVID-19 infection, though Mrs. Karpik experienced continued weight gain, her Long COVID symptoms have eased. Thus, I see no meaningful connection between her clinical presentation and her obesity.
(c) Restless Leg Syndrome (RLS): Mrs. Karpik was diagnosed with RLS in 2016 but experienced a significant remission in symptoms in 2018 with medication changes. Since 2018, there are no records of Mrs. Karpik experiencing symptoms that are specifically associated with RLS. In my examination of Mrs. Karpik, she did not mention any return of her RLS symptoms, so it is unlikely that her symptoms that emerged immediately after her SARS-CoV-2 infection would be related to a diagnosis of RLS that had been asymptomatic since 2018.
968 After Mrs Karpik was diagnosed with Long COVID, a colleague of his administered a battery of patient-reported outcome (PRO) scales to assess the severity of her symptoms. Dr Herrera said that PROs are not used to establish the diagnosis of Long COVID. [EXP_SKA.003.003.0370 [4]] He explained that the PROs completed by Mrs Karpik were refined by a team of Long COVID specialists at the Mount Sinai Health System to characterise the presence and severity of common Long COVID symptoms. As a result of Mrs Karpik completing the PROs, she was said to have scored as follows: [EXP_SKA.003.003.0315 pp 11-12]
(1) positive for dysautonomia;
(2) experiencing severe fatigue, scoring 39 on a scale of 0-100 where a higher score indicates less fatigue;
(3) positive for post-exertional malaise;
(4) having mild cognitive impairment, scoring 43.9 on a scale of 8-64.2 where a higher score indicates less cognitive impairment;
(5) having slight functional impairment with an overall score of 80 on a disability scale of 0-100 where a higher score indicates less disability;
(6) experiencing pain of unknown origin that is unlikely to be caused by neuropathic mechanisms.
969 Dr Herrera made it clear in his second report that the PROs were not used for the purpose of diagnosis of Long COVID. They therefore play no part in answering that question. There is in any event a real difficulty with the PROs because they can only be meaningful as reflecting the intensity of Mrs Karpik’s symptoms if they are compared to some norm, and what that norm was is not established. There was to have been evidence of median scores in a cohort of patients reporting Long COVID symptoms against which Mrs Karpik’s scores could be compared, but I ruled that evidence inadmissible (T421:3-9). The result is that the PROs are essentially meaningless.
970 Dr Herrera accepted in cross-examination, in the face of Mrs Karpik “severe” score for RLS in March 2022 that he had not seen previously, that his statement in the joint report that “Mrs Karpik no longer suffers from restless leg syndrome” is incorrect (T661:20).
971 As mentioned, Dr Chen is the Director of the Division of Pulmonary and Critical Care Medicine at Cedars-Sinai Medical Center in Los Angeles, California. Clinically, he has an outpatient practice focused on interstitial lung disease but also spends time attending in the medical ICU. Regarding COVID-19, he oversaw the entire ICU response to manage the surge of patients at the hospital and worked as a frontline provider caring for patients in the ICU. His division started a Post-COVID clinic in partnership with the multidisciplinary COVID-recovery clinics at Cedars-Sinai Medical Center. [EXP_RES.001.001.0055 [2]-[3]]
972 Dr Chen has also conducted translational, epidemiological and treatment studies on COVID-19 with publications in a number of top journals. He has written a book chapter on therapies for COVID-19 and served on the California COVID-19 Academic Advisory Board which was formed by the California Governor to discuss COVID-19-related treatments. He also has an ongoing research project investigating mechanisms that cause pulmonary dysfunction after COVID-19 infection. Further, he is the site principal investigator of a study to investigate mechanisms of Long COVID. [EXP_RES.001.001.0055 [4]]
973 As mentioned, Dr Chen video-interviewed Mrs Karpik on 27 June 2022. That was for approximately one and a half hours. His report sets out in detail the past and present medical history that he took from Mrs Karpik. In summary, she reported shortness of breath on exertion, cognitive deficits and fatigue as ongoing issues. Her shortness of breath had improved and, at the time of interview, typically occurred when carrying heavy items or ascending stairs. [EXP_RES.001.001.0055 [12]-[13]]
974 Dr Chen explained that the potential symptoms associated with Long COVID are wide-ranging and undoubtedly will evolve as the scientific understanding of the disease develops. However, the most common symptoms are fatigue, shortness of breath and cognitive dysfunction. [EXP_RES.001.001.0055 [30]] Determining the causality of symptoms from the COVID virus can be extremely difficult. Many of the symptoms that are associated with Long COVID are non-specific for a particular disease and overlap with many illnesses. For those reasons, teasing out the cause of symptoms after a COVID infection requires a thorough evaluation. Also, the psychological effects of social distancing and quarantine measures associated with the ongoing pandemic on mental health are well-documented and result in symptoms that overlap with those of Long COVID. [EXP_RES.001.001.0055 [31]]
975 Dr Chen explained that medical knowledge continues to evolve in understanding Long COVID. Medical science is still at the beginning stages of unravelling the mechanisms driving Long COVID, and the lack of biomarkers or diagnostic tests for the syndrome complicates the establishment of the diagnosis. One of the main challenges in diagnosing Long COVID is that the symptoms are non-specific and can overlap with many other medical conditions. [EXP_RES.001.001.0055 [43]]
976 Dr Chen identified that the CDC and WHO have provided guidance as to best practice in evaluating patients for Long COVID, which ideally should be conducted with a multidisciplinary approach involving multiple specialities. It would include a thorough history and physical examination being obtained to understand the extent of symptoms. Bloodwork and other diagnostic testing are usually guided by the symptoms. [EXP_RES.001.001.0055 [44]] Dr Herrera agreed with this evidence (T633:41, 637:11).
977 The main goal of extensive clinical evaluation is to identify and accordingly treat potential causes that may explain the symptoms. Thus, Long COVID should be considered only after identifying and treating alternative medical issues that also cause similar symptoms. The difficulty is that Long COVID is a syndrome that spans multiple organs and presents with a constellation of symptoms that often have no identifiable abnormalities on physical examination and diagnostic testing. Thus, clinicians must be attentive and comprehensive in their approach in trying to identify Long COVID, which is currently relegated to being a diagnosis of exclusion. [EXP_RES.001.001.0055 [45]]
978 With reference to Dr Herrera’s report, Dr Chen expressed the opinion that the statement that “Mrs Karpik’s symptoms and clinical history are consistent with a diagnosis of Long COVID” is technically correct, but Dr Herrera has not described how he excluded potential alternative diagnoses. [EXP_RES.001.001.0055 [49]] Dr Chen disagrees with Dr Herrera’s conclusion that “It is also not clear that there are any pre-existing injuries or conditions that predisposes Mrs Karpik to Long COVID”, because Dr Herrera did not elaborate on how he reached the conclusion. Dr Chen says that Mrs Karpik’s medical records clearly demonstrate pre-existing mental illness and restless leg disorder that can manifest as many of the symptoms described in the report (eg, fatigue, shortness of breath, malaise, cognitive impairment, leg pain, sleep issues). Moreover, obesity and age are also risk factors for many of the symptoms. Therefore, several pre-existing conditions do exist that can manifest with symptoms that overlap with Long COVID. [EXP_RES.001.001.0055 [50]]
979 In cross-examination, Dr Chen explained that his view is that the symptoms that were described to him by Mrs Karpik fall within Long COVID, so Long COVID is a condition that could possibly be causing her symptoms. However, there are other likely conditions that could be causing the symptoms, and until they can be ruled out he cannot make a diagnosis of Long COVID (T710:20-30).
980 Having reviewed Mrs Karpik’s medical records, Dr Chen says that several key details in her past medical history and her current symptomology need to be considered. There is no evidence of an ischemic heart disease or abnormal pulmonary physiological changes. Her thyroid function appears to be well treated so is likely not contributing. However, Mrs Karpik is obese and based on the medical records appears to have had significant weight gain over the years. This weight change and any associated deconditioning, in addition to age-related effects, also manifest with symptoms such as shortness of breath on exertion and fatigue. [EXP_RES.001.001.0055 [51]]
981 Dr Chen explained that obesity and advanced age are also risk factors for sleep disorders. Notably, Mrs Karpik reported difficulty sleeping throughout the night, and various disorders can manifest with fatigue and cognitive issues. Obstructive sleep apnoea can manifest with many of the symptoms described by Dr Herrera. RLS is another sleep disorder that is associated with obesity. Leg pain can be a symptom of RLS. Notably, Mrs Karpik has a history of RLS going back to 2016. [EXP_RES.001.001.0055 [52]]
982 Ultimately, Dr Chen says that he cannot conclude that Mrs Karpik has Long COVID. His reasoning is that Mrs Karpik has clear documentation in her medical records of pre-existing conditions such as RLS, depression and anxiety that manifest with symptoms similar to what she described in the report of Dr Herrera. Also, her age and weight gain cannot be excluded as contributing factors. [EXP_RES.001.001.0055 [56]]
983 Dr Chen noted that RLS can cause disturbances to sleep that can manifest with cognitive impairment, leg pain, fatigue and depression. Age and obesity also increase the risk of having sleep disorders. Depression can also present with many of the symptoms that Mrs Karpik describes. Many of Mrs Karpik’s issues (eg, age, obesity, sleep disorders, anxiety, depression) can manifest as breathlessness, making it difficult to disentangle the cause in the absence of any objective findings in her examination and diagnostic workup. That conundrum highlights the difficulty in making a Long COVID diagnosis and the need to treat, or exclude, all potential alternative diagnoses. [EXP_RES.001.001.0055 [57]-[59]]
984 There are a number of considerations that lead me to not be persuaded by the evidence of Dr Herrera and to not be satisfied that Mrs Karpik developed Long COVID following her mild COVID-19 infection in March 2020.
985 First, Dr Herrera did not undertake a physical examination of Mrs Karpik which is a significant shortcoming in his work (through no fault of his own, of course) and casts doubt on his diagnosis. In that regard, he accepted in cross-examination that to undertake a physical examination “may be important” (T633:45). He and Dr Chen wrote in their joint report that a thorough history and physical should be undertaken when evaluating someone for Long COVID, which would include evaluating their past medical history and pre-existing conditions prior to a COVID infection. [JNT.001.001.0086 [7]] Dr Herrera also agreed in his second report with Dr Chen’s opinion that “[a] thorough history and physical examination should be obtained to understand the extent of the symptoms.” [EXP_RES.001.001.0055 [44]; EXP_SKA.003.003.0370 [16]]
986 Secondly, Dr Herrera relied almost entirely on what Mrs Karpik subjectively reported to him, which is itself unreliable and in many instances was not independently proved – leaving Dr Herrera’s diagnosis to rest on unproved assumptions. In that regard, I have already explained that Mrs Karpik’s evidence as to her ailments has to be treated with caution. That is particularly so when it comes to what she reported to an expert witness who was specifically engaged for the purpose of diagnosing whether or not she suffers from Long COVID, and a positive diagnosis would potentially significantly boost her damages claim.
987 For example, Dr Herrera recorded that Mrs Karpik reported a shortness of breath on exertion, both during exercise and talking on the phone. He observed that that was a consistent problem that had been reported in her medical records throughout multiple clinical assessments. She told him that her breathlessness made it more difficult to engage in social activities such as walking with her family. However, her breathlessness is better understood as occasional or episodic, and dependent on the extent of exertion. That is hardly surprising in someone who is 70 years of age and obese.
988 Consistent with that understanding, Mrs Karpik told Dr McMahon on 23 April 2020 that she was walking nearly every day and “gets a little bit puffed.” [RESsub_DDM.001.001.0001 p 3] In July 2020, Mrs Karpik took a holiday to Coffs Harbour with her husband during which she went for long walks. On seeing Dr Croker shortly thereafter she reported “lots of walking, long walks” and “No chest pain or SOB” (ie, no shortness of breath). [RESsub_CFM.003.001.0001 p 70] Mrs Karpik explained that absence of shortness of breath on the basis that she calibrated her exertion so as to avoid becoming breathless (T227:42-228:5). That does not suggest that her breathlessness was exceptional or particularly problematic. Indeed, Dr Chen’s evidence was that the shortness of breath that Mrs Karpik reported, namely when carrying heavy items or going upstairs, was not an abnormal symptom at her age and condition (T712:26).
989 As a further example, there is no evidence from Mrs Karpik to back-up the symptom of “fatigue” that Dr Herrera relied on. Also, Dr Herrera relied on Mrs Karpik having reported cognitive impairment, including difficulty with communicating verbally and sometimes finding it hard to initiate speech. However, there is no mention of this in her first affidavit sworn in February 2021, and in her second affidavit in July 2021 she said that for about six months after she returned to work in June 2020 she would “sometimes forget words mid-sentence” but that she no longer had that problem. [LAY_SKA.001.001.0021 [13]] That is to say, from the end of 2020 she no longer had the problem, yet she reported the problem to Dr Herrera in December 2021. Then, for the first time, in her third affidavit in October 2022, Mrs Karpik complained of “brain fog.” [LAY_SKA.003.001.0039 [28]-[29]]
990 Thirdly, although he accepted that it was necessary to exclude other causes for the symptoms that she complained of, in his first report Dr Herrera did not conduct such an analysis at all and in his second report he purported to do it only in respect of pre-existing conditions of depression, obesity and RLS (see [967] above), and there are problems with his analysis.
991 With regard to other prior ailments that could explain the symptoms, Mrs Karpik had suffered from arthritis, a cervical radiculopathy (pinched nerve) in her neck and back resulting in radiating pain, pins and needles and weakness in her left arm, serious pain in her feet, and insomnia for 20-30 years. She had undergone the total removal of her thyroid and had been taking hormone medication since then, and had suffered bowel problems including intermittent bleeding. She was also 69 years old at the time of the cruise. There is no explanation by Dr Herrera of how these prior ailments were excluded. [SBM.020.007.0001 [56]-[57]]
992 To the extent that Dr Herrera relied on Mrs Karpik having difficulty with sleeping throughout the night (as identified in his first report), it is noteworthy that he nevertheless noted that Mrs Karpik acknowledged that her sleep disturbances may be related to the stressful experiences and trauma of the past 18-24 months (ie, not Long COVID). [EXP_SKA.003.003.0315 p 10] It is in any event to be observed that Mrs Karpik had suffered from sleep issues related to RLS for many years, and she reported to Dr McMahon on 23 April 2020 that “[s]he is usually not a good sleeper” and that she was struggling with sleep then. [RESsub_DDM.001.001.0001 p 4] There is therefore no foundation to a Long COVID diagnosis based on sleep issues.
993 Dr Herrera said that he ruled out depression because a psychiatrist report from Dr Parmegiani ruled out the possibility that Mrs Karpik’s depression was causing any level of functional impairment in her daily life. However, Dr Parmegiani had said that it was most likely that Mrs Karpik’s reported shortness of breath was related to residual symptoms of anxiety but that further investigations should be undertaken. [EXP_SKA.003.003.0276 p 22]
994 Dr Herrera said that he ruled out RLS because there were no records of Mrs Karpik experiencing symptoms that are specifically associated with RLS since 2018, and she did not mention any return of her RLS symptoms to him. However, Mrs Karpik had reported “restless legs” to Dr McMahon on 16 June 2020, and Dr Chen’s report (which predates Dr Herrera’s statement which was in his reply report) recorded that Mrs Karpik reported that her RLS had worsened. [RESsub_DDM.001.001.0001 p 4; EXP_RES.001.001.0055 [66]] Dr Herrera had also been briefed with Mrs Karpik’s RLS rating scale, dated 8 March 2022, which showed her RLS symptoms as being severe. [RESsub_CFM.003.001.0001 p 283ff]
995 It is to be noted that Dr Chen’s unchallenged evidence was that RLS can be the cause of fatigue, concentration issues, and depression. [EXP_RES.001.001.0055 [66]] Also, Dr Herrera accepted that RLS can cause “serious leg pain”, play “havoc with a person’s sleep patterns”, “cause fatigue”, “result in a person feeling extremely tired, lethargic or fatigued the next day” and “take a real toll on a person’s mental health” (T656:13-27). There is therefore the very real possibility, which was not excluded, that several of the symptoms that Dr Herrera relied on in his diagnosis in fact arose from RLS rather than Long COVID.
996 In the face of those errors in Dr Herrera’s evidence in relation to depression/anxiety and RLS, and Dr Chen’s clear evidence that Mrs Karpik’s relevant symptoms could derive from causes other than Long COVID which causes had not been ruled out, I am not persuaded by Dr Herrera’s diagnosis.
997 Fourthly, there is a difficulty with the timing of Dr Herrera’s diagnosis. He conducted his video-interview of Mrs Karpik more than 18 months after her COVID infection. It is very difficult to link the symptoms that she reported back to her COVID infection such a long time previously. Dr Herrera’s focus was on Mrs Karpik’s reported current symptoms, without an explanation of how they related back in time to her COVID infection, and how they were reported or may have developed in the intervening period.
998 Fifthly, in his first report Dr Herrera said that Mrs Karpik reported symptoms consistent with dysautonomia, saying that they presented as “dizziness and feelings of pre-syncope (feeling as though she is going to faint) when moving from sitting to standing, especially after prolonged sitting.” [EXP_SKA.003.003.0315 p 9] However, on 26 June 2020, Mrs Karpik’s cardiologist, Dr Shetty, reported that Mrs Karpik had “denied history of chest pain, palpitation, dizziness or loss of consciousness.” [RESsub_CFM.003.001.0001 p 225] Also, on 9 December 2021, which was only two days after the interview with Dr Herrera, Mrs Karpik reported “Nil issues with dizziness” to her GP Dr Verdon. [RESsub_CFM.003.001.0001 p 108] Thus, to the extent that Dr Herrera’s diagnosis depends on Mrs Karpik presenting with symptoms of dizziness, that presentation cannot be relied on. I reject it.
999 If I am wrong and Mrs Karpik did suffer from Long COVID, the symptoms that she suffered were in any event relatively mild and of short duration. They essential boil down to some breathlessness and limited brain fog in the 24-month period from late 2020 (when she had essentially recovered from the adjustment disorder) to June 2022 (when she presented to Dr Chen as essentially recovered from her Long COVID symptoms). On that basis, a Long COVID diagnosis would not add much to Mrs Karpik’s damages claim.
J.6 Conclusion on personal injury damages
1000 In summary, relevant to personal injury damages, I have found that:
(1) Mrs Karpik contracted COVID-19 as a result of Mr Karpik contracting COVID-19 on the Ruby Princess, although her symptoms were mild;
(2) Mrs Karpik suffered an adjustment disorder in the aftermath of the voyage of moderate severity and relatively short duration; and
(3) I am not satisfied that Mrs Karpik suffered from Long COVID.
1001 It now falls to be considered what an appropriate quantification of damages is in Mrs Karpik’s case.
1002 It will be recalled that in respect of her personal injuries, Mrs Karpik claims damages for past and future medical expenses and for non-economic loss per CLA s 16. “Non-economic loss” is defined in CLA s 3 to mean any one or more of:
(1) pain and suffering,
(2) loss of amenities of life,
(3) loss of expectation of life,
(4) disfigurement.
1003 Mrs Karpik’s claim for non-economic loss calls for an assessment of the overall severity of Mrs Karpik’s loss expressed as a percentage of an MEC. The concept of an MEC is not defined by the CLA, but was described as follows in Kurrie v Azouri (1998) 28 MVR 406 at 413 by Sheppard AJA (with whom Beazley JA agreed):
The expression “a most extreme case” requires some discussion. It enables one to provide oneself with a yardstick as to what the legislature had in mind. A court considering the question will need to contemplate what in practical terms is embraced by “a most extreme case”. Immediately one considers such a case, one thinks of cases of quadriplegia, perhaps some serious cases of paraplegia, cases of serious brain damage and, perhaps, some cases of extremely serious scarring and disfigurement caused, especially to young children, by scalding or burning. No doubt there are others. But even some cases falling within the categories I have instanced would not necessarily justify the description of a most extreme case. There would no doubt be many serious cases which would fall below the maximum although they might yield 80% or 90% of the amount to be awarded in respect of a most extreme case.
1004 Where the degree of severity is less than 15% of an MEC, no damages may be awarded for non-economic loss.
1005 I have already expressed my view that even if Mrs Karpik had suffered all three of the personal injuries claimed by her (COVID-19 infection, adjustment disorder and Long COVID) she would fall short of 15% of an MEC. In respect of the two injuries I have found that she suffered, Mrs Karpik’s COVID-19 symptoms were mild and Mrs Karpik made good progress in her recovery from her adjustment disorder. As I have concluded (see [938] above), although from March to June 2020 her distress was undoubtedly profound, from June 2020 she has functioned reasonably well in her day-to-day life for someone of her age and condition. Her professional workload is similar to what it was before the voyage and she is able to enjoy socialising with friends and family. Mrs Karpik is not disfigured, nor does it appear that she has suffered a loss of enjoyment or loss of expectation of life, at least not for a prolonged period, as a result of her injuries.
1006 When determining damages for non-economic loss, a court may refer to decisions of other courts for the purpose of establishing the appropriate award: CLA s 17A(1). The parties drew my attention to and relied on a large number of cases for comparative purposes. I have found most of them to be unhelpful because the injuries dealt with in them are too far removed from the circumstances of the present case. I have found the following cases to be of some assistance:
(1) Carangelo v State of New South Wales [2015] NSWSC 655 in which the plaintiff, a former police officer, suffered an adjustment disorder which resulted in him experiencing persistent intrusive images of traumatic crimes scenes and having to cease working as a police officer. Although a finding of negligence on the part of his employer was not ultimately made, the Court would have assessed damages at 35% of an MEC.
(2) Mason v Demasi [2012] NSWCA 210 in which the plaintiff suffered permanent physical scarring and a post-traumatic stress disorder from being attacked by a dog while walking with her young son. Her post-traumatic stress disorder symptoms had reduced with time but remained likely to continue indefinitely at a mild level. The Court of Appeal accepted the primary judge’s assessment of damages at 25% of an MEC.
(3) Hall v State of New South Wales [2014] NSWCA 154 in which a plaintiff suffered post-traumatic stress disorder after being locked in a room during a fight between two students under her care at a correctional facility, the psychiatric injury significantly altering the plaintiff’s life and rendering her unable to work. The Court of Appeal found no error in an assessment of damages at 25% of an MEC.
(4) Sutherland Shire Council v Major [2015] NSWCA 243 in which a plaintiff suffered ongoing pain in his lower back, backside, left leg and sciatic discomfort and had to avoid lifting more than five kilograms and repetitive lifting or bending after a railing gave way causing the plaintiff to fall heavily. The injuries interfered with the plaintiff’s capacity to conduct his business and with his enjoyment of life as he needed regular painkilling medication and physiotherapy. The Court of Appeal assessed damages at 20% of an MEC.
(5) Sneddon v Speaker of the Legislative Assembly [2011] NSWSC 508; 208 IR 255 in which a plaintiff suffered for over five years from major depression, panic disorder, agoraphobia and generalised anxiety disorder as a result of workplace bullying and which had required hospitalisation for a month, although by the time of trial the plaintiff had substantially recovered. The Court assessed damages at 16% of an MEC.
(6) Coles Supermarkets Australia Pty Ltd v Meneghello [2013] NSWCA 264 in which a plaintiff suffered tissue damage from a fall and had continuing pain (partly as a result of deconditioning following the injury) but which was controllable with medication. In view of the fact that there was no disfigurement, no loss of expectation of life, very minor pain and suffering and loss of amenities of life and inconvenience and every prospect of a complete recovery when at present the plaintiff was functioning satisfactorily, the Court, on appeal, assessed damages at 10% of an MEC.
(7) Zreika v New South Wales [2009] NSWCA 99 in which the plaintiff suffered injury to his right shoulder causing permanent pain and an injury to the head resulting in laceration with subsequent scarring, headaches, periodic benign vertigo and post-traumatic stress disorder, depression and anxiety. The Court of Appeal was “unable to discern any error” in the primary judge’s assessment of damages at 10% of an MEC.
1007 In the light of the above authorities, and having regard to all of the circumstances, I assess Mrs Karpik’s case as being 8% of an MEC. In view of that assessment, Mrs Karpik cannot be awarded damages for non-economic loss: CLA s 16(1).
1008 In the event that I am wrong on my conclusion that Mrs Karpik did not suffer from Long COVID, I consider that the Long COVID symptoms were in any event so mild and of such short duration that they would not contribute more than 4% to the assessment of her non-economic loss as a percentage of an MEC. Her total assessment would then be 12% of an MEC, still below the 15% threshold.
1009 Mrs Karpik also claims damages for past and future medical expenses. I address this aspect of her damages claim in the course of dealing with her out of pocket expenses in section J.8 below.
J.7 Distress and disappointment
1010 In Baltic Shipping Co v Dillon, every member of the Court accepted that disappointment and distress “caused by the breach of a contract … the object of the contract being to provide pleasure or relaxation” (at 363) is a compensable head of loss separate and distinct from injured feelings compensable under the rubric of pain and suffering and loss of amenities of life associated with personal injury. See Scenic HCA at [43].
1011 In Scenic HCA¸ it was explained that disappointment at a breach of a promise to provide recreation, relaxation and peace of mind is not an “impairment” of the mind or a “deterioration” or “injurious lessening or weakening” of the mind (at [41]). This is accordingly a separate head of damage which is not “non-economic loss” within the meaning of the CLA, and is therefore not subject to the limitations on recovery imposed by CLA s 16 (at [46]). This head of loss is conveniently referred to as Dillon damages.
1012 The Court nevertheless recognised that Dillon damages are not restricted to breach of contract, but are also available under ACL s 267(4) for breach of a consumer guarantee. Mrs Karpik also seeks Dillon damages on her ACL s 18 claim. The assessment proceeds in accordance with principles developed for breach of contract cases: Moore v Scenic Tours Pty Ltd (No 4) [2022] NSWSC 270; 409 ALR 259 at [84] per Garling J. The approach taken by Garling J in that case was upheld on appeal: Scenic Tours Pty Ltd v Moore [2023] NSWCA 74 (Scenic CA No 2) per Griffiths AJA, Ward P and Kirk JA agreeing.
1013 Additional relevant principles extracted from the judgment of Garling J, which in the absence of any criticism from the parties I gratefully adopt, include the following:
(1) The damages awarded in “holiday cases” such as this compensate a plaintiff for what they were promised when the expectation of a happy, joyous, peaceful and contented holiday has been unfulfilled. That involves a comparison between the expectations of the individual traveller and the reality of what the traveller was provided. (At [85], citing Scenic HCA at [46].)
(2) Although, in a shorthand way, these damages are described as being for “distress and disappointment”, a survey of the authorities shows that what is assessed ranges across all kinds of mental distress, inconvenience, anxiety, disappointment, frustration or vexation arising because the services to be provided were not provided, or else the purpose of the acquisition of the services failed (at [86]-[93]).
(3) Whilst each group member is entitled to have their damages assessed on an individual basis to reflect their particular experience, distress and disappointment, it is nevertheless appropriate to have regard to the objectively determined facts about the extent to which the respondents failed to achieve the purpose and result guarantees (at [94]).
(4) The commencement point of the analysis is to identify the services which the respondents promised to supply (at [95]).
(5) The assessment of damages for distress and disappointment in all of the circumstances is a very fact-rich and individual assessment (at [111]). See also Scenic CA No 2 at [188].
(6) Each claim is assessed individually by reference to that individual’s expectation, their particular circumstances, and the experience which they individually had. What was a disappointment for one traveller to miss out on a particular experience may have been a blessing for another traveller who felt relief when the experience was not available. Some passengers are more robust and resilient than others when coping with adversity, and some may have had much lower expectations. Hence, the extent of distress and disappointment may be quite different. (At [115].)
(7) An award for Dillon damages should not only be made in a token or nominal sum. The assessment of the sum for this head of damages is undertaken in the individual case by an evaluative process applying a sense of fairness and justice to the circumstances proved (at [117]). See also Scenic CA No 2 at [195].
(8) As a general proposition, the distress and disappointment occurs during the cruise and then continues after the cruise has ended for varying periods depending on the individual, and the impact which the breach of the consumer guarantees have had on that person (at [118]).
1014 The applicant submits that cases on false imprisonment are useful for comparative purposes for assessing Dillon damages. It relies on the reference to such cases in Scenic HCA at [41] in support of that proposition. There it was said that the claim for damages for disappointment and distress resulting from breach of contract “can be seen as no more a claim relating to personal injury than would be a claim for damages for the indignation occasioned by false imprisonment or defamation.” The references to false imprisonment and defamation were to illustrate the point that the Court was making, namely that disappointment at a breach of a promise to provide recreation, relaxation and peace of mind is not a claim for an “impairment of a person’s physical or mental condition” or otherwise a form of injury within s 11 of the CLA. The Court was not otherwise saying that the distress and disappointment of a failed holiday is comparable to damages for false imprisonment.
1015 Indeed, in Lewis v Australian Capital Territory [2020] HCA 26; 271 CLR 192 at [45] it was explained that the tort of false imprisonment is a form of trespass to the person; it is actionable per se, regardless of whether the victim suffers any harm. It does not require proof of special damage. The tort protects and vindicates a person’s right to freedom from interference with personal liberty as a fundamental legal right.
1016 On any view, damages for distress and disappointment suffered as a consequence of a failed holiday are thus incomparable to compensable damages for false imprisonment. In the circumstances, I do not see any value in having regard to false imprisonment cases in assessing damages in the present case.
1017 Mrs Karpik submits that she should be awarded Dillon damages in the range of $50,000 to $60,000 on the basis of her distress and disappointment, distinct from the personal injuries she suffered. Those damages are said to encompass the distress felt by Mrs Karpik during the voyage when her husband became unwell and her anxiety in the immediate aftermath of the voyage at Mr Karpik’s deteriorating state of health to the point of his hospitalisation, as well as Mrs Karpik’s frustration at the respondents’ conduct of the cruise and her sense of loss for the relaxing and pleasurable holiday that she expected to enjoy.
1018 Mrs Karpik also submits that if I do not find that her Long COVID injury is established, the damages awarded for distress and disappointment should be increased in the amount of $50,000 to reflect the struggles and difficulty that Mrs Karpik has had to endure arising from the symptoms of breathlessness on exertion, fatigue and brain fog. This is said to be on the basis that Mrs Karpik was not suffering from these symptoms before the voyage and so it should be inferred that the respondents’ contraventions of the ACL caused or contributed to these symptoms.
1019 The applicant recognises that Dillon damages are not consequential upon a physical or psychiatric injury, but says that they are for non-economic loss or “pain and suffering” (relying on the concurring judgment of Edelman J in Scenic HCA at [69]). The applicant therefore submits that it is necessary to “distinguish distress and disappointment that was a consequence of her injuries from that which was not.” She submits that that requires drawing conclusions about when Mrs Karpik commenced to suffer from each of the injuries (COVID-19 infection and adjustment disorder) and whether distress felt after this occurred was related to an injury. She submits that distress and disappointment felt by her after she commenced to suffer from her injuries will be compensable as part of an award of distress and disappointment damages if it is not pain and suffering consequential upon an injury.
1020 As mentioned, the applicant also submits that if I find that she did not suffer from Long COVID, as I have now found, then many of the symptoms that she relies on for the Long COVID diagnosis should be taken into account as giving rise to Dillon damages. However, if those matters do not arise from Mrs Karpik’s COVID infection such as to amount to Long COVID, as I have found, then they may arise from her adjustment disorder, which is compensated separately, or from some other cause or ailment. They all manifest physically and are not compensable as Dillon damages.
1021 The applicant is correct in the submission that distress, disappointment, anxiety, frustration, and so on, that arises from personal injury is not compensable as Dillon damages. The result of that, however, and contrary to the applicant’s submission, is that there is very little left to compensate her for as Dillon damages. That is because almost all of those feelings, or experiences of hers – referred to by Edelman J in Scenic HCA as “mental harm” (at [69]) but by the plurality as not being “impairment of a person’s … mental condition” (at [41]) – arise out of personal injury to her (COVID infection and adjustment disorder) or to her husband (COVID infection). There is in any event a question whether Dillon damages would be available in respect of a failure of the purpose or result guarantee in respect of another person, rather than the person claiming. That was not raised by the parties and need not be considered any further.
1022 Commencing the analysis with the services that were promised, I identified the services in section E.2 above. The complaint about the respondents having failed to provide what was promised is a narrow one, relating only to precautions against COVID infection. There is otherwise no complaint about the panoply of cruising, hotel and vacation-type services that were provided. That marks the present case as very different from the Moore v Scenic cases. There, a completely different experience was provided in substitution for the promised experience. In the present case, the cruise went ahead essentially as planned. I deal with these matters in section B.8.3 above. It was cut short by a few days, with a few port visits cancelled, on account of Government decree, but any recovery in respect of that shortcoming is prevented by ACL s 267(1)(c)(i), ie, it occurred only because of an act by a person other than the supplier.
1023 On Mrs Karpik’s evidence, she and her travel companions participated in a range of activities (trivia, bingo, art auctions), went to restaurants, cafes and bars, engaged in shopping, went to the theatre, and undertook excursions to several destinations in New Zealand. To the extent that Mrs Karpik did not participate in other activities, she explained in her first affidavit that she did not attend many of the activities because her intention was to relax and enjoy time with her travel companions.
1024 In her evidence, Mrs Karpik made various references to her concerns about precautions to protect passengers from infection. To the extent that she had such concerns from time to time on the cruise, they did not prevent her from participating in activities or spending time with her friends as planned. Her stated concern did not make her consider using the face masks that she had brought with her, even after Mr Karpik became ill (T167:11-19, 178:21-22, 188:15-31). Also, any generalised fear or concern that Mrs Karpik may have had about getting infected with COVID on board, disconnected from any particular way in which the purpose or result guarantee was not complied with, cannot give rise to any Dillon damages. I accept that she had some level of concern or anxiety about Mr Karpik, her friend Lucy or herself getting COVID while on the cruise, but she would have had that anyway – none of it was caused by the failure to comply with the statutory guarantees. It was caused by the growing epidemic and her knowledge of its risks, including what had occurred on the Diamond Princess.
1025 Contrary to the respondents’ submissions, I accept that Mrs Karpik suffered some distress, disappointment and frustration as a consequence of the respondents’ failure to comply with the purpose and result guarantees. This arises from the ways in which her cruise experience was detrimentally impacted by Mr Karpik becoming ill. Those include that she had to care for her husband which to some degree restricted what she could do, she lost the benefit of his company from time to time when, for example, he cut an excursion short or was isolating so could not join her in the restaurant or for other activities, and because she worried about his health. However, with regard to the latter, it will be recalled that she thought that he likely had influenza A which is not normally life threatening – she said she was “rather pleased that he had influenza A” and that she was “almost celebrating that he had been diagnosed with influenza A” (T169:3, 30, 36, 171:5). The extent of her worry at that stage should therefore not be overstated.
1026 I also accept that Mrs Karpik suffered some Dillon damages in the period from disembarkation on 19 March 2020 until Mr Karpik was admitted to hospital on the morning of 21 March 2020, ie, for a period of approximately one day (dealt with in some detail in section B.8.4 above). I consider that thereafter, which is to say after Mr Karpik became seriously ill, the experiences of distress and the like that Mrs Karpik felt are tied up in her adjustment disorder, contributing to the cause of it and being compensable as personal injury damages.
1027 Mrs Karpik gave evidence that she felt stigmatised by being a Ruby Princess passenger, and she claims that that is compensable as Dillon damages. She gives examples of people shunning her in one way or another on learning that she was a passenger on the Ruby Princess. [LAY_SKA.001.001.0083 [254]] This does not seem to me to be a particularly significant matter, but in any event I do not consider that it is compensable as Dillon damages – it is an injury to dignity or reputation rather than being distress and so on caused by a failure to comply with a guarantee.
1028 Mr and Mrs Karpik each paid approximately $4,400 for their cruise. [LAY_SKA.001.001.0273 p 9; CAU.001.141.0049] They received a total refund from the respondents after the cruise. I do not consider that Mrs Karpik’s Dillon damages exceed that amount – I would assess them at about the costs of the cruise at the most. To a substantial extent she lost the benefit of the cruise in the sense that she was worried, distressed, disappointed and so on thereafter rather than feeling refreshed and reinvigorated, but when on the cruise she essentially enjoyed the experience that she had purchased and paid for. On balance, she suffered no more than $4,400 worth of Dillon damages.
1029 The applicant does not dispute that the refund can properly be taken as credit against the Dillon damages. She does not submit, for example, that the refund should be taken as credit against any reduction in value damages claimable under ACL s 267(3), which damages she does not otherwise claim, or that the refund should be characterised as an ex gratia payment that cannot be credited against any of her damages. Rather, she submits that her Dillon damages substantially exceed the refund that she received. For the reasons I have given, I disagree. Because of the refund, she should receive nil Dillon damages.
1030 Mrs Karpik claims past out of pocket expenses that she incurred in connection with treatment of the three injuries that she allegedly sustained as a consequence of the respondents’ conduct, namely, COVID-19 infection, Long COVID, and an adjustment disorder. Mrs Karpik submits that the combined cost of past medical expenses in relation to all three injuries is $7,866.28. Mrs Karpik also submits that due to her Long COVID injury, an allowance in the sum of $2,500 (in addition to the total figure given for all three injuries) should be made for the possibility of future medical expenses associated with relapse of her symptoms.
1031 Given that I am not satisfied that Mrs Karpik suffered from Long COVID, I reject her claim for out of pocket expenses related to Long COVID, including the allowance for future medical expenses. When her Long COVID expenses are excluded, the total amount of out of pocket expenses claimed by Mrs Karpik is $4,423.48. That figure is based on an itemised list of expenses comprising GP consultations, psychiatrist consultations, specialist consultations and investigations, pathology services and the cost of her Valdoxan medication. The bulk of the total amount claimed is attributable to Mrs Karpik’s adjustment disorder ($4,249.54) with only a small amount claimed in respect of her COVID-19 infection ($173.94).
1032 Mrs Karpik submits that the amount claimed in respect of her adjustment disorder is reasonable when compared against the health benefit of the treatment obtained, citing Lumley v Sainsbury [2017] ACTSC 40 at [69] (Murrell CJ) and Sharman v Evans [1977] HCA 8; 138 CLR 563 at 573 (Gibbs and Stephen JJ). She submits that the amount claimed is relatively modest and the expenses incurred were obviously beneficial as she recovered from her adjustment disorder. Mrs Karpik does not claim for the costs of her Valdoxan medication after December 2021.
J.8.2 The respondents’ position
1033 The respondents accept that if liability is established, the applicant should be entitled to past out of pocket expenses connected with her adjustment disorder. However, the respondents submit that the applicant’s claim in full should be limited to the period between March and June 2020 and claimable only at a reduced rate between July 2020 and February 2021. They say that expenses incurred after February 2021 should be excluded. They submit that the psychiatric expert evidence concerning the applicant’s adjustment disorder confirms that from June 2020, Mrs Karpik’s injury was much less severe and that there is no basis for treatment costs after February 2021. Consequently, the respondents say that the Court should only allow 50% of the treatment costs between July 2020 and February 2021.
1034 The respondents oppose Mrs Karpik’s claims for out of pocket expenses associated with her COVID-19 infection and Long COVID consistent with their position that Mrs Karpik did not contract COVID-19 or suffer Long COVID.
1035 As I have said, I am satisfied on the balance of probabilities that Mrs Karpik did contract COVID-19 (see section C.2.6 above). The out of pocket expenses claimed in connection with the applicant’s COVID injury relate principally to the costs of GP consultations and pathology services. The amount claimed is very small and apparently reasonable. I accept it as properly claimable.
1036 As I have explained why the Long COVID out of pocket expenses are not claimable, the only remaining difference between the parties concerns the proper amount claimable in respect of Mrs Karpik’s adjustment disorder from July 2020.
1037 Once causation is established, the question for a court is whether the expenses incurred in the treatment of an injury were reasonable: State Rail Authority of New South Wales v Brown [2006] NSWCA 220 at [84] per Basten JA (Giles and Santow JJ agreeing). Reasonableness is assessed taking into account the claimed cost, and the health benefit, of the treatment. If the cost is very great and the health benefit only slight or speculative, the cost of treatment will be unreasonable, especially where inexpensive alternatives are available. Where the costs and benefits are more evenly balanced, the weighing of the factors presents a more difficult task: Sharman at 573.
1038 It will be recalled that I have found that Mrs Karpik suffered an adjustment disorder of moderate severity. Her symptoms were acute between March and June 2020, but she subsequently began to improve. Dr Samuels and Dr Parmegiani agree that it is highly likely that Mrs Karpik suffered a recognised psychiatric illness from the period of March 2020 “at least up until the time of Dr Parmegiani’s assessment on 19 February 2021.” Between June 2020 and July 2021, Mrs Karpik continued to see her treating psychiatrist, Dr McMahon. Dr Samuels concluded that by the time of his consultation with Mrs Karpik in May 2022 her adjustment disorder had resolved, although she was still taking the anti-depressant medication, Valdoxan.
1039 The amounts claimed by Mrs Karpik for the treatment of her adjustment disorder encompass the period from 27 March 2020 to 17 December 2021 and relate primarily to GP consultations, consultations with Dr McMahon, and the cost of Valdoxan.
1040 I reject the respondents’ submission that Mrs Karpik’s claim for out of pocket expenses should be reduced from July 2020 merely because her symptoms were less severe from that time as she commenced her recovery. The fact that treatment for an injury is effective is not a proper basis to reduce a claim for the cost of that treatment where such treatment remains medically reasonably necessary. It is to be expected that recovery from an illness will be gradual.
1041 Moreover, except for the costs of her Valdoxan medication which remain stable from the time of her prescription, the costs of Mrs Karpik’s treatment for her adjustment disorder decreased in tandem with the decrease in the severity of her symptoms. As one would expect, Mrs Karpik’s non-Valdoxan treatment expenses were highest in the period March to June 2020 when she consulted with Dr McMahon every week or two, totalling $1,093.75. Between July 2020 and February 2021 the costs of her non-Valdoxan treatment expenses totalled $458.14, whereas between February 2021 and December 2021 those same expenses were only $133.60. Mrs Karpik does not claim any treatment expenses, Valdoxan or otherwise, from December 2021. Given that it is difficult to pinpoint with precision when Mrs Karpik’s adjustment disorder went into remission, on the whole I am satisfied that the costs claimed by her are reasonable.
1042 Mrs Karpik should be awarded the full $4,423.48 claimed for out of pocket expenses in respect of her COVID-19 infection and adjustment disorder injuries. She is entitled to interest on that sum.
1043 In the result, Mrs Karpik should be awarded the following damages:
(1) On her ACL ss 61(1) and 61(2) purpose and result guarantee claims: nil for non-economic loss, but $4,423.48 plus interest for her out of pocket expenses.
(2) On her ACL s 60 care guarantee and common law negligence claims: nil for non-economic loss, but $4,423.48 plus interest for her out of pocket expenses.
(3) On her ACL s 18 claim: nil.
1044 On 20 December 2021, I made Merck Orders (see Merck Sharp & Dohme (Australia) Pty Ltd v Peterson [2009] FCAFC 26, 355 ALR 20) provisionally identifying the common questions to be determined at the initial trial. Some debate arose during the trial with regard to the process for identifying which questions are truly common questions, and giving the parties the opportunity to make submissions on the proper answers.
1045 It was then clarified by me, which the parties accepted, that I would decide all factual and legal issues necessary for the purpose of deciding Mrs Karpik’s claim, including with regard to the provisionally identified common questions annexed to the orders of 20 December 2021. However, I would not make any orders as to the resolution of any of the provisionally identified common questions until I had heard further from the parties (by way of written and/or oral submissions) on which of those questions truly are common and, in the light of the findings made, precisely how those questions should be framed and answered. (See T705-706.)
1046 The matter will accordingly require further listing for the determination of what truly are common questions and what their answers are.
1047 For ease of reference, it is worth taking stock of what I have decided, noting that I do not intend by the summary that follows to say anything different from what I have recorded as having decided above. Also, the summary mostly omits various findings that I have made in the respondents’ favour, focussing instead on the respects in which Mrs Karpik’s claims succeed.
1048 On the critical factual issues, I have found that Mr Karpik most likely contracted COVID-19 on board the Ruby Princess (at [294]), and that Mrs Karpik contracted COVID-19 from Mr Karpik on the voyage (at [397]). Mrs Karpik suffered a recognised psychiatric illness in the form of an adjustment disorder as a consequence of Mr Karpik’s illness and hospitalisation (at [938]), but she did not suffer from Long COVID (at [984]).
1049 With regard to the application of the CLA to Mrs Karpik’s various claims, I have held as follows:
(1) It is common ground that the various provisions of the CLA to which the parties refer (and which are identified in the following sub-paragraphs) all apply to the negligence claim (at [399]), save for CLA s 5D(3)(b) which deals with the admissibility of a statement by an injured person of what they would have done had the negligence not occurred (at [782]).
(2) CLA s 16, which limits liability for damages for non-economic loss for personal injuries unless the severity of the non-economic loss is at least 15% of a most extreme case, and which sets a maximum amount of such liability and an indexed sliding scale for its determination, applies to and limits the consumer guarantee claims (ie, ACL ss 60, 61(1) and 61(2)) (at [419]).
(3) CLA s 5R and s 9(1) of the LRMP Act, which provide for the reduction of recoverable damages to the extent of the claimant’s contributory negligence, apply to the consumer guarantee claims (at [420]).
(4) CLA s 5H, which provides that a person does not owe a duty to another person to warn of an obvious risk, is not picked up and applied to the consumer guarantee claims (at [430]).
(5) CLA s 5I, which provides that a person is not liable in negligence for harm suffered by another person as a result of the materialisation of an inherent risk, is not picked up and applied to the consumer guarantee claims (at [438]).
(6) CLA s 32(1), which applies a standard of “normal fortitude” to claims for mental harm, does not apply to the consumer guarantee claims (at [443]).
(7) It is not contended by either side of the case that any of the CLA provisions apply to the ACL s 18 claim for misleading and deceptive conduct.
1050 With regard to Mrs Karpik’s ACL ss 61(1) and 61(2) claims, the purpose and result consumer guarantees, I have found as follows:
(1) Mrs Karpik made known to the respondents that her purpose in booking the cruise, and the result that she wished the cruise to achieve, was that she would have a safe, relaxing and pleasurable cruise holiday substantially in accordance with the advertised and booked itinerary (at [469]).
(2) The effect of s 61(1) is therefore that the respondents guaranteed that the cruise services to be supplied by them would be reasonably fit for that purpose, and the effect of s 61(2) is that the respondents guaranteed that the cruise services to be supplied by them would be of such a nature, and quality, state or condition, that they might reasonably be expected to achieve that result.
(3) As a result of Mr and Mrs Karpik contracting COVID-19 on the cruise, Mrs Karpik did not have a safe, relaxing and pleasurable cruise holiday. The particular purpose for which the services were acquired and the result that was desired to be achieved accordingly failed. The reason for that failure was because the services were not reasonably fit to achieve that purpose and they were not of such a nature and quality that they might reasonably have been expected to achieve that result.
(4) The purpose and result guarantees were accordingly not complied with.
(See section E.6 above.)
1051 With regard to Mrs Karpik’s negligence and ACL s 60 claims, I have found as follows:
(1) The respondents owed Mrs Karpik a duty to take reasonable care for her health and safety, including with regard to the risk of harm caused by coronavirus infection (at [546]).
(2) The respondents also owed Mrs Karpik a duty of care with respect to a recognised psychiatric illness arising from Mr Karpik contracting COVID-19 on the voyage. In respect of the claim in negligence, the “normal fortitude” test or requirement in CLA s 32(1) is satisfied (at [579]).
(3) The respondents breached their duty of care in various respects, namely by failing to:
(a) cancel the cruise (at [609]);
(b) warn of the heightened risk of the virus being on board RU2007 compared to cruise ships generally (at [625]), but not the heightened risk of infection from the virus on a cruise ship compared to the community generally because that was an obvious risk (at [618]);
(c) implement better pre-embarkation screening, namely temperature screening for passengers and crew and requiring all passengers and crew to record whether they were suffering from any symptoms of COVID-19 and to deny them boarding if they were (at [649]);
(d) implement a system of physical distancing on board (ie, in accordance with the 1.5m rule) (at [665]);
(e) from 11 March 2020, isolate passengers who presented with ARI and ILI on the cruise and failing to provide roommates of those passengers with face masks, alcohol hand rub and information on how they could protect themselves from disease (at [681]).
1052 With regard to Mrs Karpik’s ACL s 18 misleading and deceptive conduct claim, the respondents made the following misleading representations:
(1) A Safe to Board Representation, namely that it was reasonably safe for passengers to embark on the cruise (at [738]);
(2) A Reasonable Care Representation, namely that the respondents would take reasonable care for the safety of passengers during the cruise (at [742]);
(3) A Best Practices Representation, namely that the respondents had implemented, and would continue to implement, increased monitoring, screening and sanitation protocols to protect the health of passengers which measures were designed to be flexible to adapt to changing conditions and recommended best practice (at [752]); and
(4) A Pleasurable Cruise Representation, namely that the respondents would supply the promised cruising services as set out in their advertising brochures and passenger contracts and in doing so would do all things reasonably within their ability to enable the passengers to have a safe, relaxing and pleasurable cruise (at [765]).
1053 I have found that causation and loss is established on each of the causes of action (at [772], [837] and [846]-[847]).
1054 I have found that Mrs Karpik’s COVID-19 infection gave rise to very mild symptoms, and did not result in Long COVID, with the result that it contributes very little to any non-economic loss (at [893]). The non-economic loss for the adjustment disorder is assessed at 8% of a most extreme case (at [1007]), and if Mrs Karpik had Long COVID that would be assessed at 4% of a most extreme case (at [1008]). In the result, no personal injury damages are awarded on the ACL ss 60, 61(1) and 61(2) claims or the negligence claim as the non-economic loss is less than the threshold of 15%.
1055 Out of pocket expenses on the personal injury damages are recoverable on the ACL ss 60, 61(1) and 61(2) and the negligence claim in the sum of $4,423.48 plus interest (at [1042]).
1056 Distress and disappointment damages, which would be available on all the causes of action, do not exceed the sum of the refund paid to Mrs Karpik with the result that no such damages are payable (at [1028]-[1029]).
1057 I have not found it a fruitful exercise to calculate the pre-judgment interest that Mrs Karpik is entitled to on her out of pocket expenses. I expect the parties to agree that.
1058 It is also going to be necessary to make final decisions on the common questions.
1059 I will therefore list the matter for further case management, and direct the parties to bring in agreed or competing orders to give effect to these reasons and for the determination of the common questions.
I certify that the preceding one thousand and fifty-nine (1059) numbered paragraphs are a true copy of the Reasons for Judgment of the Honourable Justice Stewart. |
Associate:

