FEDERAL COURT OF AUSTRALIA
Unilever Australia Ltd v Beiersdorf Australia Ltd [2018] FCA 2076
|
Table of Corrections |
|
|
27 February 2019 |
Paragraph 227 has been changed from ‘…between a product with an absolute efficacy of 20% and a product with an absolute efficacy of 10%’ to ‘…between a product with an absolute efficacy of 20% and a product with an absolute efficacy of 30%’. |
|
|
Paragraph 330 has been changed from ‘test #3 may nonetheless have been relatively significant’ to ‘test #3 may nonetheless have been relatively insignificant’. |
ORDERS
Applicant | ||
AND: | Respondent | |
DATE OF ORDER: |
THE COURT ORDERS THAT:
1. The applicant’s amended originating application filed 9 June 2016 be dismissed.
2. The applicant pay the respondent’s costs.
3. Pursuant to r 1.39 of the Federal Court Rules 2011 (Cth), the time within which the applicant must file and serve any notice of appeal pursuant to rr 36.02 and 36.03 of the Rules is to commence to run from 4 February 2019.
Note: Entry of orders is dealt with in Rule 39.32 of the Federal Court Rules 2011.
WIGNEY J:
1 The applicant, Unilever Australia Ltd, is a consumer goods company which, amongst other things, markets, distributes and sells antiperspirant deodorants in Australia under the well-known brands, Rexona and Dove. In July 2009, Unilever began to market, distribute and sell a “Clinical Protection” range of Rexona and Dove antiperspirant deodorants. The key features of the products in that range were that they were “soft-solid” creams contained in canisters from which they were applied; were offered for sale in boxes which contained an instructional leaflet; and prominently featured the words “Clinical Protection” on both the canister and box. The Clinical Protection range was marketed as being particularly suitable for persons who sweated heavily and was generally sold at significantly higher prices than other antiperspirant deodorants.
2 By December 2013, another major distributor of antiperspirant deodorants, Revlon Australia Pty Ltd, began selling a range of antiperspirant deodorants named “Mitchum Clinical”. Products in that range were also soft-solid creams contained in a canister; were sold in a box containing an instructional leaflet; prominently featured the word “clinical” on the canister and box; were marketed as being particularly suitable for persons who sweated heavily; and were generally sold at a higher price than other antiperspirant deodorants, other than products within the Rexona and Dove Clinical Protection range.
3 Like Unilever and Revlon, the respondent, Beiersdorf Australia Ltd, also markets, distributes and sells antiperspirant deodorants in Australia. It does so under the well-known brand, Nivea. In about July 2014, Beiersdorf began to market, distribute and sell a “Nivea Stress Protect Clinical Strength” range of antiperspirant deodorants. The key features of the products within that range were that they were deodorant “sticks” located in a canister from which the stick could be applied; were sold in a box which contained an instructional leaflet; prominently featured the words “Clinical Strength”, albeit along with the equally prominent words “Stress Protect”; and were generally sold at a higher price than other antiperspirant deodorants, other than the Rexona and Dove Clinical Protection range and the Mitchum Clinical range.
4 In this proceeding, Unilever alleged that, in marketing, distributing and selling the Nivea Stress Protect Clinical Strength range of antiperspirant deodorants in the way it did, Beiersdorf engaged in misleading or deceptive conduct, or made false or misleading representations, contrary to, respectively, ss 18 and 29(1)(a) and (g) of the Australian Consumer Law (ACL), which is Schedule 2 to the Competition and Consumer Act 2010 (Cth). Unilever contended, in short, that Beiersdorf’s conduct was misleading or deceptive because, in marketing, distributing and selling the Nivea Stress Protect Clinical Strength range in the way it did, Beiersdorf made a number of representations to consumers concerning the antiperspirant efficacy of that range. Those alleged representations included representations about the efficacy of the range as compared to the antiperspirant efficacy of the Rexona and Dove Clinical Protection range and the Mitchum Clinical range, and the antiperspirant efficacy of the range as compared to all other so-called “non-clinical” antiperspirant deodorants. Some of the representations said to have been made by Beiersdorf related to future matters. Unilever alleged that the representations made by Beiersdorf were false or misleading.
5 Beiersdorf disputed Unilever’s claims and defended the proceedings. There was, of course, no dispute that, at all relevant times, Beiersdorf marketed, distributed and sold antiperspirant deodorants as part of the Nivea Stress Protect Clinical Strength range. Beiersdorf disputed, however, that its conduct in so doing was in any sense misleading or deceptive. In particular, it disputed that its conduct gave rise to any of the representations alleged by Unilever, other than two that related to the efficacy of its product for consumers who suffer from stress sweat. Beiersdorf characterised Unilever’s claim as an allegation of “comparative advertising by stealth”. It contended, amongst other things, that its marketing and distribution of the product, including use of the words “clinical strength”, the packaging in a box, the inclusion of a leaflet and the higher price, said nothing to consumers about the antiperspirant efficacy of the Nivea Stress Protect Clinical Strength range as compared to either the Rexona and Dove Clinical Protection range, or any other antiperspirant deodorants. Beiersdorf also contended that, even if the Court found that any of the alleged representations had been conveyed to consumers, Unilever had not discharged its burden of proving that they were false or misleading as alleged by Unilever. As for the representations that related to future matters, Beiersdorf’s case was that, if they were made, it had reasonable grounds to make them.
6 The principal questions thrown up by the rival claims and contentions are, at least on one level, relatively easy to frame: did Beiersdorf, by its marketing, distribution and sale of the Nivea Stress Protect Clinical Strength range, make representations to consumers about the antiperspirant efficacy of that range as compared to the Rexona and Dove Clinical Protection range and all other “non-clinical” antiperspirant deodorants; if so, were any of those representations false or misleading; and, in respect of the representations as to future matters, did Beiersdorf have reasonable grounds to make those representations?
7 While the principal questions may be easy to frame, they are by no means easy to answer.
8 The question whether Beiersdorf made any of the alleged representations hinges, to a large extent, on whether there was a “clinical” subcategory or segment in the market for antiperspirant deodorants in Australia at the relevant time and, if so, what ordinary consumers perceived, or were likely to perceive, about the characteristics or qualities of products within that subcategory or segment. If, by its conduct in marketing, distributing and selling the Nivea Stress Protect Clinical Strength range, Beiersdorf effectively represented to ordinary reasonable consumers of antiperspirant deodorants in Australia that those products properly belonged in any existing “clinical” subcategory or segment, did it follow that it thereby represented that those products had similar antiperspirant efficacy and characteristics to the existing products in that subcategory or segment, the Rexona, Dove and Mitchum “clinical” products? And did it also follow that Beiersdorf thereby represented that its products had greater antiperspirant efficacy than all other “non-clinical” antiperspirant deodorants in the Australian market for antiperspirant deodorants?
9 The question whether the representations, if found to have been made by Beiersdorf, were false or misleading, turns to a large extent on the nature and reliability of various laboratory tests which measured the relative effectiveness of the products in reducing the amount of perspiration excreted in various conditions or circumstances. Unilever relied on the results of a number of so-called “head-to-head” tests which tended to show that its products generally reduced perspiration by some percentage more than Beiersdorf’s products. It also relied on comparisons between various “absolute” tests which recorded the overall sweat reduction qualities of various products. There was, however, considerable dispute and debate about the tests, and the test results and their interpretation, including about the reliability or ability of the test results to gauge the relative significance of the differences between the tested products.
10 Before turning to address the facts and evidence in more detail, it is necessary to say something about the relevant provisions of the ACL and the legal principles that apply to them in cases like this.
Relevant Statutory Provisions and Applicable Principles
11 Section 18 of the ACL provides as follows:
(1) A person must not, in trade or commerce, engage in conduct that is misleading or deceptive or is likely to mislead or deceive.
(2) nothing in Part 3-1 (which is about unfair practices) limits by implication subsection (1).
12 Section 29(1)(a) and (g) of the ACL are in the following terms:
(1) A person must not, in trade or commerce, in connection with the supply or possible supply of goods or services or in connection with the promotion by any means of the supply or use of goods or services:
(a) make a false or misleading representation that goods are of a particular standard, quality, value, grade, composition, style or model or have had a particular history or particular previous use; or
…
(g) make a false or misleading representation that goods or services have sponsorship, approval, performance characteristics, accessories, uses or benefits;
…
13 Section 4 of the ACL, which relates to misleading representations with respect to future matters, provides as follows:
(1) If:
(a) a person makes a representation with respect to any future matter (including the doing of, or the refusing to do, any act); and
(b) the person does not have reasonable grounds for making the representation;
the representation is taken, for the purposes of this Schedule, to be misleading.
(2) For the purposes of applying subsection (1) in relation to a proceeding concerning a representation made with respect to a future matter by:
(a) a party to the proceeding; or
(b) any other person;
the party or other person is taken not to have had reasonable grounds for making the representation, unless evidence is adduced to the contrary.
(3) To avoid doubt, subsection (2) does not:
(a) have the effect that, merely because such evidence to the contrary is adduced, the person who made the representation is taken to have had reasonable grounds for making the representation; or
(b) have the effect of placing on any person an onus of proving that the person who made the representation had reasonable grounds for making the representation.
(4) Subsection (1) does not limit by implication the meaning of a reference in this Schedule to:
(a) a misleading representation; or
(b) a representation that is misleading in a material particular; or
(c) conduct that is misleading or is likely or liable to mislead
and, in particular, does not imply that a representation that a person makes with respect to any future matter is not misleading merely because the person has reasonable grounds for making the representation.
14 The applicable principles in relation to actions for misleading or deceptive conduct under s 18 of the ACL and false or misleading representations under s 29 of the ACL are relatively well settled. There was ultimately no significant or material dispute about those principles. The real issue in this matter is the application of those principles to the facts and circumstances of this case. It is accordingly unnecessary to discuss the relevant principles in any great detail. It should also be noted that many of the principles concerning misleading or deceptive conduct that are discussed in the authorities are really just common sense or logical guides to the approach that should be taken in deciding what is, at the end of the day, a question of fact.
15 Section 18 of the ACL is not limited to misleading or deceptive representations. The question is whether the respondent’s conduct, which may include acts, omissions, statements or silence, is misleading or deceptive, or likely to mislead or deceive: Australian Competition and Consumer Commission v TPG Internet Pty Ltd (2013) 250 CLR 640 at 655 [49] (per French CJ, Crennan, Bell and Keane JJ).
16 For the enquiry under s 18, it is necessary to identify the impugned conduct and then to consider whether that conduct, considered as a whole and in context, is misleading or deceptive, or likely to mislead or deceive: Google Inc v Australian Competition and Consumer Commission (2013) 249 CLR 435 at [89], [102] and [118]. The same applies to the enquiry as to false or misleading representations under s 29 of the ACL: Australian Competition and Consumer Commission v Coles Supermarkets Australia Pty Ltd (2014) 317 ALR 73; FCA 634 at [38].
17 There is no meaningful difference between the words and phrases “misleading or deceptive” and “mislead or deceive” in s 18 and “false or misleading” in s 29(1): Australian Competition and Consumer Commission v Dukemaster Pty Ltd [2009] FCA 682 at [14]; Coles Supermarkets at [40].
18 Conduct is misleading or deceptive if it has a tendency to lead a person into error, or lead them to believe what is, in fact, false. There must be a sufficient causal link between the conduct and the error on the part of persons exposed to it: TPG Internet at 651 [39].
19 Conduct is likely to mislead or deceive if there is a real or not remote chance or possibility that it will have that effect: Global Sportsman Pty Ltd v Mirror Newspapers Pty Ltd (1984) 2 FCR 82 at 87. It is insufficient for the impugned conduct to only cause confusion or wonderment: Campomar Sociedad, Limitada v Nike International Ltd (2000) 202 CLR 45 at 87 [106] citing the judgment of a majority of the Full Court in Taco Company of Australia Inc v Taco Bell Pty Ltd (1982) 42 ALR 177 at 201; 2 TPR 48 (per Deane and Fitzgerald JJ).
20 The question whether conduct is misleading or deceptive, or is likely to mislead or deceive, is an objective question of fact that is to be determined on the basis of the conduct of the respondent as a whole viewed in the context of all relevant surrounding facts and circumstances. Viewing isolated parts of the conduct of a party “invites error”: Butcher v Lachlan Elder Realty Pty Ltd (2004) 218 CLR 592 at 625 [109] (per McHugh J); Campbell v Backoffice Investments Pty Ltd (2009) 238 CLR 304 at 341-342 [102] (per Gummow, Hayne, Heydon and Kiefel JJ).
21 Where the conduct or representation is in the form of words, it would be wrong to fix on some words and ignore others which may provide relevant context and give meaning to the impugned words. It is necessary to have regard to the whole context: Butcher at 638-639 [152] (per McHugh J).
22 The relevant context may include consideration of the type of market in which the goods are sold, the manner in which such goods are sold and the habits and characteristics of purchasers in such a market: see, generally, TPG Internet at 656 [52]; Parkdale Custom Built Furniture Pty Ltd v Puxu Pty Ltd (1982) 149 CLR 191 at 199; Reckitt & Colman Products Ltd v Borden Inc (1990) 17 IPR 1 at 16-17; 1 WLR 491 at 509; Coles Supermarkets at [41].
23 The question involves the characterisation of the relevant conduct. Evidence that persons have in fact been misled or deceived by the conduct is not an essential element, however, it can in some cases be relevant and material: Parkdale at 198-199 (per Gibbs CJ): Coles Supermarkets at [45].
24 The tendency of the conduct or representation to mislead or deceive is to be considered or tested against the ordinary or reasonable members of the class to whom the representation was made or the conduct directed. In Campomar, the High Court said (at 87 [105]):
The initial question which must be determined is whether the misconceptions, or deceptions, alleged to arise or to be likely to arise are properly to be attributed to the ordinary or reasonable members of the classes of prospective purchasers.
25 The question is whether a substantial, or at least a reasonably significant, number of that class is likely to be misled or deceived: see Optical 88 Ltd v Optical 88 Pty Ltd (No 2) (2010) 275 ALR 526; FCA 1380 at [336]-[342]. The focus on ordinary or reasonable members of the relevant class of consumers means, in effect, that possible extreme, unreasonable or illogical reactions can be put to one side.
26 It is not necessary to prove that the respondent intended to mislead or deceive, however, evidence of such an intention may constitute evidence that the conduct was likely to succeed in misleading or deceiving, and may make a finding of contravention more likely: Yorke v Lucas (1985) 158 CLR 661 at 666 (per Mason ACJ, Wilson, Deane and Dawson JJ); Verrocchi v Direct Chemist Outlet Pty Ltd (2016) 247 FCR 570 at [103]; Australian Woollen Mills Ltd v FS Walton & Co Ltd (1937) 58 CLR 641 at 657 (per Dixon and McTiernan JJ).
27 Where the conduct or representation is in the form of an advertisement, the “dominant message” or “general thrust” of the advertisement is important: TPG Internet at [47]. It is nevertheless important to have regard to the whole advertisement because context is or may be important. It may also be relevant to have regard to the external context in which a consumer is likely to view an advertisement: TPG Internet at 653-655 [45]-[52] (per French CJ, Crennan, Bell and Keane JJ).
28 Where an advertisement is capable of more than one meaning, the question of whether the advertisement is misleading or deceptive must be tested against each meaning that is reasonably open: Tobacco Institute of Australia Ltd v Australian Federation of Consumer Organisations Inc (1992) 38 FCR 1 at 50. If one or more of the reasonably available different meanings is misleading, the conduct may well be misleading or deceptive, or false or misleading: Coles Supermarkets at [47].
29 The question whether Beiersdorf made any of the alleged representations turns on a close consideration of the facts and evidence relating to the market for antiperspirant deodorants in Australia, including Unilever’s Rexona and Dove Clinical Protection range of antiperspirant deodorants, and Beiersdorf’s marketing, distribution and sale of the Nivea Stress Protect Clinical Strength range. The facts and evidence concerning the testing of the antiperspirant efficacy and effectiveness of the rival products will be considered separately in the context of the question whether the representations, if found to have been conveyed, were false or misleading.
30 The market for deodorants in Australia accounts for over $300 million by retail sales value. The market includes deodorants, which impact odour by imparting a perfume, and antiperspirant deodorants which, in addition to imparting a perfume, also operate by reducing the amount of perspiration released by the apocrine and eccrine sweat glands under the arms.
31 In very general terms, an antiperspirant deodorant reduces perspiration by “plugging” the eccrine glands. The active ingredients which are responsible for that action are aluminium salts or actives. Different types of aluminium actives are better able to operate to plug the eccrine glands than others. It appears to be generally accepted that Activated Aluminium Zirconium Tetrachlorohydrex Glycine (AZAG) is the most effective aluminium active at plugging the eccrine glands. The amount and type of aluminium active in an antiperspirant deodorant is an important characteristic in any assessment of antiperspirant efficacy, though there is no precise or linear relationship between efficacy and the amount or type of aluminium active. Other things that may impact on the efficacy of an antiperspirant deodorant include the nature of the delivery mechanism and the nature or type of formulation of the antiperspirant deodorant.
32 Various different types and formulations of antiperspirant deodorants are sold in Australia. They include: stick antiperspirant deodorants, which are a solid or waxy formulation dispensed by a winder mechanism; pump antiperspirant deodorants, which are liquid, pumped out of a container by a pump mechanism; aerosol antiperspirant deodorants, which operate by expelling a gas from a container under pressure; roll-on antiperspirant deodorants, which operate by dispensing a liquid from a container using a rolling ball at the top of the container; and soft-solid antiperspirant deodorants, which are a soft-solid or cream formulation which is applied from a container with a winder mechanism which pushes the formulation through a grate at the top of the container.
33 It is possible to generalise or theorise about the comparative efficacy of the various different formulations, though ultimately the antiperspirant efficacy of any particular antiperspirant deodorant can only be definitively determined by laboratory testing. In very general terms, however, aerosols are usually less efficacious than roll-ons, sticks and soft-solids. That is because the higher efficacy aluminium actives cannot be used in aerosols, the amount of active in aerosols is generally limited and the delivery mechanism is not as efficient. Roll-ons are generally more efficacious than aerosols because they can contain the higher efficacy aluminium salts. They cannot, however, contain AZAG. Both sticks and soft-solids can contain AZAG and are therefore generally more efficacious than other formulations. Though theories and opinions may be expressed concerning the comparative efficacy of sticks and soft-solids, ultimately, the antiperspirant efficacy of any particular stick or soft-solid would be likely to depend on a number of considerations, not just the amount and type of the aluminium actives, including AZAG, in the particular product.
Unilever’s Rexona and Dove Clinical Protection range
34 In July 2009, Unilever commenced marketing, distributing and selling what it referred to as its “Clinical Protection” antiperspirant deodorant range. That range included the following products: “Rexona Clinical Protection”, “Rexona Men Clinical Protection” and “Dove Clinical Protection”. Those products all had the following characteristics.
35 First, they were offered for sale in a box which was approximately 11cm high, 7cm long and 4.5cm wide.
36 Second, the product itself was an antiperspirant deodorant soft-solid cream within a canister from which the soft-solid cream could be applied.
37 Third, also located in the box was an instructional leaflet. The Rexona Clinical Protection leaflet relevantly included the following statements or claims: “Rexona Clinical Protection provides our most advanced, long-lasting protection against wetness and odour”; “clinical strength wetness protection”; and “motion activated odour control technology”. The Dove Clinical Protection leaflet relevantly included the following statements or claims: “[p]rovides clinical strength protection against wetness”; “[d]elivers all-day freshness through odour-fighting technology”; and “[f]eatures a signature fragrance”. Both the Rexona and Dove Clinical Protection leaflets also provided directions for use and answers to questions such as “[w]hat is the difference between deodorants and anti-perspirant deodorants?” and “[a]re anti-perspirants safe?”. The leaflets do not contain any specific quantified or quantifiable claims concerning perspiration reduction.
38 Fourth, both the box and the canister in which the product was located prominently featured, along with the brand name “Rexona” or “Dove”, as the case may be, the words “clinical protection” above the words “antiperspirant deodorant”. While there were some variations between different boxes and canisters, they almost invariably included the words “[c]linical strength wetness” protection. Some of the boxes and canisters also included, after those words, the words “& odour protection” or “for heavy sweating”. Some included the words “Dermatologist Tested” or, in one case, “Doctor Recommended”. From about 2014, some included the words “[m]otion activated odour protection”.
39 Fifth, the products within the Clinical Protection range were sold in supermarkets at prices substantially higher than other antiperspirant deodorants; often as much as two to three times higher. That was the case until, as will be seen, Revlon introduced into the market its Mitchum Clinical range and Beiersdorf later introduced its Stress Protect Clinical Strength range.
40 The products within the Clinical Protection range were sold with different types of fragrances and other apparently distinguishing features. For example, some of the boxes and canisters included labels or descriptions such as “sport”, “adventure”, “stress control” and “summer strength”.
41 Appendix 1 contains images of various boxes used in the range.
42 From 2009, Unilever marketed its “Clinical Protection” range in Australia as being particularly suitable for persons who sweat heavily, or who were concerned about heavy sweating.
43 Unilever’s Clinical Protection range was the subject of fairly extensive advertising and publicity from the time of its launch. The focus of that advertising and publicity was that the Clinical Protection range was designed, tested and proven to be effective for people who were heavy sweaters. In a segment on a current affairs program broadcast on television in August 2012, for example, it was said, amongst other things, that “[a]fter ongoing testing and development for five years, it [Rexona Clinical Protection] claims to be the only antiperspirant deodorant that works for heavy sweaters who don’t have a medical problem”. A television advertisement that was broadcast from about 2011 to early 2014 said that people who sweat more than normal should try Rexona Clinical Protection deodorant because “it’s the most effective antiperspirant deodorant in Australia that protects you twice as much”. An advertisement relating to Dove Clinical Protection stated that it was “clinically proven to give twice the protection of a basic antiperspirant”. A Rexona Clinical Protection advertisement broadcast throughout 2014 and into the first quarter of 2015 emphasised that “[n]othing is stronger”.
Other “clinical” products before July 2014
44 In about December 2013, Revlon commenced marketing, distributing and selling a range of antiperspirant deodorants using the name “Mitchum” or “Mitchum Clinical”. Those products included the following features.
45 First, they were offered for sale in a box which was approximately 12.5cm high, 7cm long and 3cm wide.
46 Second, the product itself was an antiperspirant deodorant soft-solid cream within a canister from which the soft-solid cream could be applied.
47 Third, also located in the box was an instructional leaflet. There was no evidence concerning the contents of the Mitchum Clinical leaflet.
48 Fourth, both the box and the canister in which the product was located prominently featured the word “clinical”, either as part of, or along with, the brand name “Mitchum”. While there were some variations between different boxes and canisters, they generally also included the words “Oxygen odour control technology”, “maximum strength formula harnesses the power of pure oxygen” and “48 hr protection”.
49 Fifth, the product was sold in supermarkets at prices substantially higher than other antiperspirant deodorants, other than Unilever’s Rexona and Dove Clinical Protection range and, subsequently, Beiersdorf’s Nivea Stress Protect Clinical Strength range.
50 The products within the Mitchum Clinical range were sold with different types of fragrances and other apparently distinguishing features. For example, some of the boxes and canisters included labels such as “sport”, “clean control” and “powder fresh”.
51 Appendix 2 contains images of various boxes used in the “Mitchum Clinical” range.
52 In 2011 and early 2012, antiperspirant deodorants using the brand name “Brut V8 Clinical Protection” and “Norsca Clinical Protection” were sold in Australia. Between 2011 and early 2013, an antiperspirant deodorant called “Lady Speed Stick Clinical Proof” was also sold in Australia. There was very little evidence concerning those products, though it was common ground that, like Unilever’s Rexona and Dove Clinical Protection range and Revlon’s Mitchum Clinical range, they were sold in a rectangular box, prominently featured the word “clinical” as part of their name or otherwise, and were generally sold at prices substantially higher than all other antiperspirant deodorants. It was also common ground that, in the period 2011 to 2013, those products had a combined market share of antiperspirant deodorants which used “clinical” as part of their name by units sold of less than 6%.
The Australian antiperspirant deodorant market as at July 2014
53 As at July 2014, the deodorant and antiperspirant deodorant market in Australia, measured by units sold from August 2013, was divided as follows: 53.6% aerosol antiperspirant deodorants; 21.16% roll-on antiperspirant deodorants; 19.81% body spray deodorants; 2.58% stick antiperspirant deodorants; 1.95% soft-solid antiperspirant deodorants, being essentially the Rexona and Dove Clinical Protection range and the Mitchum Clinical; and 0.90% pump, creams and other deodorants. The Rexona and Dove Clinical Protection range accounted for 90.8% of the sales of soft-solid antiperspirant deodorants, and the Mitchum Clinical range accounted for 9.2%.
54 The Rexona and Dove Clinical Protection range and the Mitchum Clinical range were the only antiperspirant deodorants sold in Australian supermarkets as at July 2014 which: were packaged in a rectangular box; were supplied with an instructional leaflet inside the box; prominently featured the word “clinical” as part of the product name or otherwise; and were sold at a price which was substantially higher than all other antiperspirant deodorants.
Beiersdorf’s launch of the Nivea Stress Protect Clinical Strength range
55 In July 2014, Beiersdorf commenced marketing, distributing and selling in Australia a new Nivea range of antiperspirant deodorants called Nivea Stress Protect Clinical Strength. Before considering the particular features of that range, and the marketing and advertising that accompanied its launch, it is relevant to have regard to the circumstances in which that range came to be launched in Australia.
56 In June 2012, Beiersdorf decided to introduce a new range of antiperspirant deodorants in Australia called the “Stress Protect” range developed by its parent company, Beiersdorf AG, which was based in Hamburg, Germany. That range included a roll-on, an aerosol spray and an antiperspirant stick. Beiersdorf initially decided to only launch the Stress Protect roll-on and aerosol in Australia. That was in part due to the fact that antiperspirant sticks were only a small segment of the Australian market. In September 2012, however, Beiersdorf decided to investigate the possibility of also introducing the Nivea Stress Protect Clinical Strength stick into Australia. The intention was to market that product as having a high efficacy against stress sweat in particular.
57 Ms Julia Braun was the General Manager of Marketing at Beiersdorf. Her evidence was that a number of considerations were taken into account in deciding to launch the Nivea Stress Protect Clinical Strength stick in Australia as a high-efficacy product. Those considerations included that, unlike its competitors at that time, Beiersdorf did not have any products which were specifically marketed as having high efficacy. In addition, Beiersdorf AG had advised that, as compared to the roll-on and aerosol formats of the Stress Protect range, the Nivea Stress Protect Clinical Strength stick had the highest concentration and the most scientifically advanced form of antiperspirant active. It was the most efficacious of the three products.
58 According to Ms Braun, Beiersdorf AG had also advised Beiersdorf that each of the roll-on, aerosol and stick formats of the Nivea Stress Protect range had been proven, in scientific testing conducted by Beiersdorf AG, to have a high level of efficacy against stress sweat. Nevertheless, Beiersdorf did not wish to launch the roll-on or aerosol formats as high-efficacy products against stress sweat at the time because the “high efficacy segment” represented only a small segment of the Australian market, whereas the general roll-on and aerosol segments were much larger. Beiersdorf did not wish to limit the marketing of the roll-on and aerosol formats to the high efficacy segment at the expense of capturing market share in the general roll-on and aerosol segments. Since the stick segment of the market in Australia was small, it was considered that marketing the stick format as high efficacy would not limit, but, rather, would assist with the sale of the product.
59 In cross-examination, Ms Braun agreed that she believed or was aware that there was a “clinical protection” or “highly efficacious clinical protection” segment of the antiperspirant deodorant market in Australia. She also agreed that that segment was established by Rexona and Dove in 2009. Ms Braun also knew, in September 2012, that Rexona, Dove and Lady Speed Stick had products which were specifically marketed as having high efficacy. Those products were marketed as being “clinical” or “clinical protection” products, which she understood as meaning high efficacy.
60 In September 2012, Ms Braun and Mr Paul Croci, who was the Marketing Services Manager at Beiersdorf, decided to engage a consumer research agency, Lonergan Research, to conduct a blind home user test to assess whether the female variant of the Nivea Stress Protect Clinical Strength stick would perform as well, or better than, Rexona and Dove Clinical Protection and the Lady Speed Stick antiperspirant deodorants, each of which was marketed as having high efficacy. The results of that testing were to be used by Beiersdorf to assess whether it would be desirable to introduce the Nivea Stress Protect Clinical Strength stick into Australia as a high-efficacy product against stress sweat.
61 The research brief prepared by Mr Croci and another Senior Brand Manager noted:
1.1 What is the situation, and why are we doing this research?
The ANZ Deodorant Category is traditionally an Aerosol and Roll On format market, and consumers are highly format loyal (dislike other formats). Three years ago, our key competitor Rexona introduced a new product called ‘Clinical Protect’ x 2 to the mass market in a creamy stick format. Since then Rexona have launched 4 further Clinical Protect variants, now contributing 11% of their sales; this range is by far the largest contributor to the overall growth of the deodorant category, which otherwise is commoditized and competes highly on price. More recently, Dove have also launched 2 Clinical Protection variants.
The NIVEA Deodorant brand has enjoyed significant growth over the past two years with true market innovations in form of added benefit or formulation innovations like NIVEA & NIVEA MEN INVISIBLE FOR BLACK & WHITE, NIVEA MEN SILVER PROTECT, which are driving the brand forward. At the same time, it is the brands challenge to overcome its poor efficacy perception in the mind of the consumer; efficacy is the No 1 Purchase Driver in the ANZ market.
2013 will see the brand launch another true market innovation with the launch of NIVEA & NIVEA Men Stress Protect in the traditional Aerosol & Roll on Format. Following the establishment of this new range & benefits, we are considering extending this line into Clinical Strength Stress Protect Sticks x 2 (launch in June).
62 The report also stated, under the subheading “What do we already know?”:
The Clinical Protection Range is marketed & formulated for people that perceive themselves to be ‘heavy sweaters’ or sweat excessively (highly efficacious against underarm wetness & odour). These consumers are prepared to pay a premium for a product that finally helps with their underarm sweat problems, which emotionally provides them with a huge amount of confidence.
63 Under the subheading “Crux”, the following was recorded:
Our stick format would be intended to compete against the Dove and Rexona Cream Sticks; however, we still face the perception of lower efficacy in the minds of consumers. Our stick format would be branded as Clinical Strength Stress Protect, but to be successful it would have to work at least as well as the competitors. This research is intended to determine whether our Stress Protect stick does perform as well as (or better than) our key competitors – because if it doesn’t, we won’t launch it.
64 When taken to this passage in cross-examination, Ms Braun gave the following evidence:
Yes?---Because, you know, for us at Nivea it was of utmost importance, you know, that when we launch in a segment which is high efficacy that then we also fulfil the needs of the consumers, in this case heavy sweaters, that it is highly efficacious. And as this high efficacy segment was formed by Rexona and Dove you know, then it is to have one – yes, you know, you want to be – to offer to the consumer something which is similar, you know, to their offering in terms of satisfying them against heavy sweat and, in our specific case, stress sweat.
(Emphasis added.)
65 As will be seen, Unilever relied heavily on Ms Braun’s use of the word “similar” when giving that evidence. It would appear from Ms Braun’s evidence as a whole, however, that her concern in launching the Nivea Stress Protect Clinical Strength stick in Australia was not so much with the comparative efficacy of the Nivea product in a purely quantitative sense. Nor was she referring to what Beiersdorf’s proposed marketing of the Nivea Stress Protect Clinical Strength stick in the “high efficacy” segment would convey, or would be likely to convey, to Australian consumers of antiperspirant deodorants. Rather, her concern was that, before deciding to launch the product, Beiersdorf wanted to be satisfied that its product would be able to effectively compete with the Rexona and Dove Clinical Protection range as a high-efficacy product. That was likely to depend on consumer perceptions concerning the overall efficacy of the product as compared to the existing high-efficacy products. It did not necessarily depend on specific quantitative measures or levels of efficacy. Ms Braun did not believe that consumers thought in terms of “levels” of efficacy.
66 Ms Braun gave the following evidence in that regard:
Yes. I want to suggest to you that you, as marketing general manager of Beiersdorf Australia, reading this document had in your mind that users of Dove and Rexona cream sticks had formed a certain expectation of a level of efficacy?---I think consumers, they don’t think in level of efficacy. It has to – it’s very simple. It has to work for them or not and especially heavy sweaters. You know, they go trial and error. When something works [for] them, then it’s an efficacious product and they stick with them.
Do you accept that the notion of determining whether the Stress Protect stick “performs as well as or better than” starts with an assumption of a level of efficacy which the new product wants to either equal or exceed?---That was to be competitive in the market, you know. I mean, and for – in order to be so, you know, to be competitive you have to perform compared to the market leader at least on a similar level.
Yes. And on a similar level means with a similar level of efficacy or a better level than efficacy?---As perceived by the consumer.
Thank you. And it doesn’t – that includes, does it not, the idea that the consumer being the Dove or Rexona consumer has a present level of perception of the level of efficacy?---When they have used the products and they are happy with and they say it works for them, then it works for them. They don’t think in levels.
67 The results of the blind testing survey conducted by Beiersdorf are considered in some detail later in the context of the issue concerning whether the representations, if found to have been made, were false or misleading. Suffice it to say at this stage that Ms Braun’s evidence concerning the results was that the Nivea Stress Protect Clinical Strength stick generally performed on par with or close to the Rexona, Dove and Lady Speed Stick products in terms of perceived antiperspirant efficacy and deodorant efficacy. Nevertheless, Beiersdorf decided not to proceed with the launch at that time on the basis that the results could be further improved. In February 2013, Beiersdorf decided to ask Beiersdorf AG to reformulate the Nivea Stress Protect Clinical Strength stick “to further improve the product’s perceived deodorant efficacy”. Beiersdorf AG subsequently substantially increased the amount of fragrance in the formulation.
68 Beiersdorf commissioned further blind home user tests in 2013. The results of those tests are also considered later. Suffice it to say at this stage that, so far as Ms Braun was concerned, the results showed that the reformulated Nivea products generally performed on par with or close to the Rexona products, in terms of both perceived antiperspirant and deodorant efficacy.
69 In November 2013, Beiersdorf decided to launch “a Nivea high efficacy product for stress sweat” in Australia. Ms Braun’s evidence was that Beiersdorf decided to adopt the name “Nivea Stress Protect Clinical Strength” for its “high efficacy product for stress sweat” in Australia for essentially five reasons.
70 The first reason was that Beiersdorf wanted to capitalise on the success of the “‘Stress Protect’ sub-brand”. Ms Braun’s evidence in cross-examination was that “Stress Protect was first and foremost, you know, because we were building the sub-segment and this launch could further enhance and positive[ly] build the sub-segment”.
71 The second reason was that “[e]ach of the Rexona, Mitchum, Dove and Lady Speed Stick products sold in the Australian market which were marketed as having high efficacy … were described as ‘clinical’”.
72 The third reason was that there was no legal or regulatory definition of “clinical” or “clinical strength” in respect of antiperspirant deodorants in Australia. In those circumstances, Beiersdorf “considered ‘clinical’ to be a descriptor which different suppliers were using to identify a product which falls within the high efficacy subcategory”.
73 The fourth reason was that Beiersdorf was satisfied that the Nivea product was a high-efficacy product with respect to stress sweat.
74 The fifth reason, which Ms Braun referred to during cross-examination, was that “clinical strength is the subcategory in the market” which included products with “extra efficacy”.
75 A campaign brief prepared by Ms Kate Hensley, a Senior Brand Manager at Beiersdorf, in January 2014 provided some further insight into Beiersdorf’s perceptions concerning the launch and marketing of the Nivea Stress Protect Clinical Strength stick at the time. It stated, amongst other things, that Nivea “will launch into the highly efficacious ‘clinical protection’ antiperspirant segment” which was “established by Rexona & Dove in 2009”. It also noted that the “Clinical Protection segment” had been used by Unilever to “imply superior product efficacy of their products in treating excessive sweating”.
76 The campaign brief included the following questions and answers:
What makes a product Clinical Strength?
1. No legal or regulatory definition for ‘Clinical Strength’
2. Efficacy vs. standard anti-perspirant deodorants (ingredients & concentration)
3. Clinically proven
…
What makes NIVEA Stress Protect Clinical Strength?
1. TSST study conduc[t]ed by BDF research Efficient sweat reduction of three different antiperspirant application forms during stress-induced sweating. International Journal of Cosmetic Science 35, 622-631, 2013
2. Concentration & type of Anti-perspirant ingredients
3. Results from local BHUT (superior to market leader for female and on par with market leader for male).
77 The reference in this document to “TSST study” was reference to a “Trier Social Stress Test” study which was discussed in a paper co-authored by a biochemist employed by Beiersdorf AG, Dr Thomas Schmidt-Rose. That paper was published in the December 2013 edition of the International Journal of Cosmetic Science. That study will be referred to in detail later in the context of the relevant test results and the alleged falsity of the representations. It is sufficient to note at this stage that Ms Braun’s evidence was that, at the time of the launch of the Nivea Stress Protect range, she understood that scientific testing conducted by or on behalf of Beiersdorf AG had established that the products within that range, including the Nivea Stress Protect Clinical Strength stick, had a high level of antiperspirant efficacy against stress sweat.
Marketing, distribution and sale of Nivea Stress Protect Clinical Strength
78 From July 2014, Nivea Stress Protect Clinical Strength antiperspirant deodorants were offered for sale in two variants. Both variants had the following key features.
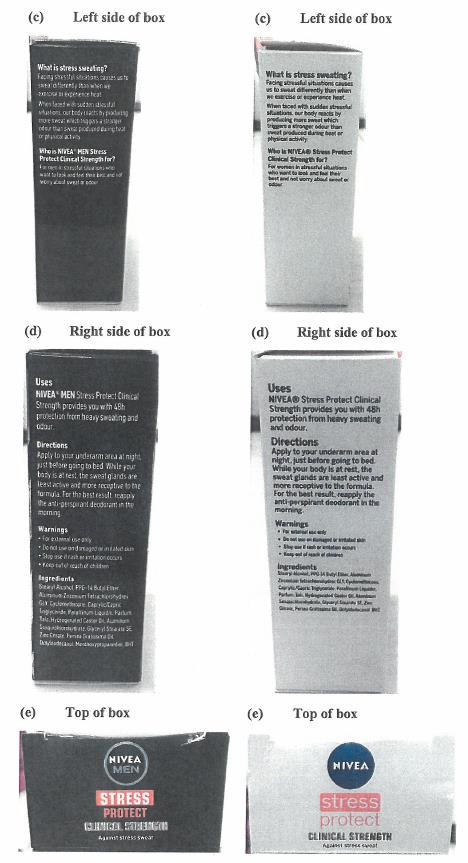
79 First, the product was sold in a box which was approximately 13cm high, 7cm long and 4cm wide.
80 Second, the product itself was an antiperspirant deodorant stick, as opposed to a soft-solid cream, located in a canister from which the stick could be applied.
81 Third, the product was sold with an instructional leaflet inside the box. The leaflet posed and answered three questions, each directed in one way or another at “stress sweating”. The first question was: What is stress sweating? The answer provided was that there are two types of sweating: thermal sweating, produced by the eccrine glands as the body’s reaction to temperature and physical exertion; and stress sweating, which is produced by activation of the apocrine gland as the body’s reaction when facing a heightened emotionally stressful situation. The second question was: Do I need protection from stress sweating? The answer provided was, in essence, “yes”. The third question was: How does Nivea Stress Protect Clinical Strength work? The answer referred to the “latest generation anti-perspirant actives”, a “Zinc complex which prevents the production of odour-causing bacteria” and a “fresh and subtle scent”.
82 Fourth, the box and canister prominently featured the words “Stress Protect” and “Clinical Strength”. The words “Stress Protect” were in a different and perhaps even more prominent typeface than the words “Clinical Strength”. The words “against stress sweat” appear below the words “Clinical Strength” in smaller typeface.
83 Appendix 3 contains an image of the box.
84 The price recommended by Beiersdorf as a retail price for the Nivea Stress Protect Clinical Strength antiperspirant deodorants was a price which was similar to the Rexona and Dove Clinical Protection antiperspirant deodorants and was substantially higher than all other antiperspirant deodorants.
85 Ms Braun’s evidence was that Beiersdorf decided to sell the product in a box with a leaflet “to align with the [cues] of the segment and to say clearly, ‘[h]ere is a special stress sweat solution for heavy sweaters which is highly efficient’”. She regarded the box “as an important part of the clinical category” and as “[r]einforcing that these are specific products for heavy sweaters … which are highly efficient”. Ms Braun was aware that Rexona and Dove Clinical Protection, Mitchum Clinical and Nivea Stress Protect Clinical Strength were the only antiperspirant deodorants in supermarkets that were sold in a box.
86 Ms Braun’s evidence was that the addition of the words “Clinical Strength” to the stick product differentiated it from the Stress Protect roll-on and aerosol and was intended to signal to the market that the product was “above those two [the roll-on and aerosol] in efficacy”, was “especially for heavy sweaters” and “was a product with a specially high efficacy”. Nevertheless, the “get-up” of the Nivea Stress Protect Clinical Strength stick was designed to indicate that it was still part of the same range as the Stress Protect roll-on and aerosol, which was why it carried the words “Stress Protect” so prominently on the pack.
87 Ms Braun’s evidence in relation to pricing was similar. The price recommended by Beiersdorf as the retail price for the Nivea Stress Protect Clinical Strength stick was similar to Unilever’s recommended price for the Rexona and Dove Clinical Protection range. As has already been noted, that price was substantially higher than most other antiperspirant deodorants. Ms Braun’s evidence was that the recommended pricing of the Nivea Stress Protect Clinical Strength stick was “a [cue] of the sub-category” and that she expected that it would be a strong cue that the Nivea Stress Protect Clinical Strength stick would be more effective than its Stress Protect “siblings”. Beiersdorf’s intention in relation to the pricing was to “adapt to” or to be “aligned with” the segment because the Nivea Stress Protect Clinical Strength stick was Beiersdorf’s strongest antiperspirant deodorant.
Advertising of Beiersdorf’s product
88 During the period 14 August 2014 to 2 April 2015, two Beiersdorf television commercials were broadcast throughout Australia. The common theme of those advertisements was fighting stress sweat and associated body odour. The advertisements included the following visual or audio cues or messages: “Nivea’s strongest protection against heavy stress sweat”; “[p]ut an end to extra heavy stress sweating or your money back”; “Nivea’s strongest stress sweat solution”; and “with the highest concentration and most advanced stress sweat fighting anti-perspirant ingredients”.
89 As can be seen, the claims concerning the properties of the Nivea Stress Protect Clinical Strength product that were made in the advertisements related almost exclusively to protection against stress sweat. Little or nothing was made of any property or properties relating to the word “clinical”. Perhaps more significantly, to the extent that the advertisements contained any comparative claims, the comparisons related to other Nivea products. There was certainly no express comparisons with, or even mention of, the Rexona and Dove Clinical Protection products or Mitchum Clinical.
90 The Nielsen Company is a company which, amongst other things, provides market data including sales, distribution, market share and market pricing covering major Australian retailers including Woolworths, Coles and IGA. Nielsen’s data concerning antiperspirant deodorants included information about the type or category of each product. That information was provided by the suppliers, including Unilever and Beiersdorf. The vast majority of the products in Nielsen’s database were simply described as being “anti-perspirants”. The exception was that each of the products in Unilever’s Clinical Protection range, the Mitchum Clinical range and Beiersdorf’s Nivea Stress Protect Clinical Strength range were described in the Nielsen data as being “clinical” products. The effect of Ms Braun’s evidence was that Beiersdorf supplied information to Nielsen concerning the Nivea Stress Protect Clinical Strength range on the basis that the products within the range were in the “clinical category” because Beiersdorf was “launching [the range] into the clinical category”.
Nivea Stress Protect range in the United Kingdom
91 Beiersdorf also marketed, distributed and sold a Nivea Stress Protect range in the United Kingdom. That range included a Nivea Stress Protect stick. That product was essentially the same as the Nivea Stress Protect Clinical Strength stick sold in Australia, save for the fact that the Australian product had a different and stronger fragrance. As noted earlier, Beiersdorf arranged for the formulation of the Stress Protect stick which was to be launched in Australia to have a stronger fragrance following the 2012 blind home user tests.
92 The Nivea Stress Protect stick which was sold in the United Kingdom was not called “Clinical Strength”, was not sold in a box and was not sold at a significantly higher price than the Nivea Stress Protect roll-on or aerosol. It should be noted, however, that there was no “clinical” subcategory or segment of antiperspirant deodorants in the United Kingdom. Ms Braun’s evidence was that the “clinical” segment was specific to Australia.
Expert marketing evidence concerning antiperspirant deodorants
93 Unilever adduced expert evidence from Professor Jill Klein, Professor of Marketing at the Melbourne Business School, University of Melbourne. There was no issue concerning Prof. Klein’s experience, qualifications or expertise. Nor was there any dispute that the opinions she expressed were based wholly or substantially on specialised knowledge derived from her training, study or experience.
94 In preparing her expert report, Prof. Klein was asked to assume a number of facts, including facts relating to the market for antiperspirant deodorants in Australia as at July 2014. It is unnecessary to set out the facts that Prof. Klein was asked to assume. It should, however, be observed that Prof. Klein was in effect asked to assume that there was a “clinical” segment of the Australian market which was occupied by the Rexona and Dove Clinical Protection products and Mitchum Clinical. She was also asked to assume that those “clinical” products provided a greater level of protection against excessive sweating. As will be seen, some of Prof. Klein’s key opinions did not travel much beyond those assumptions.
95 Prof. Klein was asked to report on how consumers, or different types of consumers, form opinions about the strength of an antiperspirant deodorant in combatting perspiration amongst products ordinarily available in supermarkets in Australia. She was asked to answer that question in relation to both products ordinarily available in supermarkets in Australia and the Nivea Stress Protect Clinical Strength products. Prof. Klein was asked to address those questions by reference to any relevant statements of accepted marketing principle, research or characteristics of consumer behaviour.
96 Prof. Klein’s evidence was that the answer to the key question asked of her “very much related to the issue of how consumers learn about and categorise products and the cues consumers use to assign a particular product to a category or subcategory”. According to Prof. Klein, as consumers are exposed to information about different products, they develop “schemas”, organised around taxonomic categories or divisions that classify similar objects into the same category. She gave, as an example, the schema for soft drinks, which would include Coke, Pepsi, Diet Pepsi, Sprite, Coke Zero, Fanta Orange and, no doubt, a number of other carbonated drinks. Prof. Klein’s evidence was that schemas can contain category and object associations, and are hierarchical and organised into subcategories. The soft drink schema, for example, could be organised into subcategories, such as diet and non-diet soft drinks. Advertising, pricing, packaging and shelving placement can all contribute to consumers developing subcategories.
97 Prof. Klein’s opinion, based on the facts she was asked to assume and her knowledge of consumer behaviour, was that there was a “clinical subcategory” of antiperspirant deodorants in the minds of consumers in Australia. That view was supported by the following factors: the advertising of “clinical products” that emphasised the word “clinical” and that the products were for heavy sweaters or people who needed a very strong deodorant; the pricing of products in the subcategory, which was two to three times higher than regular antiperspirants; the packaging of the “clinical” products, which was distinct in the use of a box and the prominent display of the word “clinical”; and the fact that supermarkets typically shelved the clinical products together, often in the top or second from the top shelf.
98 In cross-examination, Prof. Klein explained the development of the subcategory for clinical deodorants in the following terms:
Did you study that …..?---So it’s hierarchical. So people – people in Australia would probably have an antiperspirant schema. And it may have subcategories or – you know, there’s the general category – and above that is toiletries and healthcare products and all kinds of things. So it’s – it’s a very broad category. Within that we have antiperspirants, deodorants. And growing up, learning about these things, seeing our parents use them, seeing advertisements, seeing the products, we would then get a more complicated schema. And it wouldn’t just be the one mum uses but we would start to get more and more information populated. And we might – you know, perhaps someone would have the roll-on subcategory or the not-roll-on subcategory. There might be different kinds of – the very smelly, perfume-y ones. The not so perfume-y one. Women’s ones. Men’s ones. You know, depending on how much someone has paid attention, they might have more or less complex schemas. So what I’m suggesting in – in my statement is that over time as these clinical products started to become known, people saw them on the shelves, people talked about them, people started using them, people saw advertisings for them – they would start creating a subcategory of clinical antiperspirant deodorants. And then there would be associations they would make with those: that they’re very strong or that they solve a special person’s problem or something like that.
99 Importantly, in Prof. Klein’s opinion, consumers were very likely to classify the Nivea Stress Protect Clinical Strength stick as a “clinical product” due to: the similarities between the advertising of that Nivea product and the advertising for the other “clinical protection products” (principally the Rexona and Dove Clinical Protection range); the price, which was roughly two to three times higher than normal antiperspirant deodorants; the packaging, which was in a box with the prominent display of the word “clinical”; the shelving of the products in supermarkets, which was typically together with other so-called clinical products; the fact that the “point [was] clearly made that these products [were for] people who sweat a great deal and/or need a very strong deodorant”; and the fact that the “clinical product advertised is different from regular antiperspirants”.
100 As will be discussed in more detail shortly, however, Prof. Klein’s opinions did not directly address what were perhaps the most critical questions. Those questions relate to what the ordinary reasonable consumer perceived, or was likely to perceive, that “membership” of the clinical subcategory entailed. What did a particular product’s membership, or claimed membership, of the clinical subcategory represent to consumers? What did consumers perceive to be the common qualities or characteristics of the products within the clinical subcategory?
101 Consumers presumably did not buy, or consider buying, products in the clinical subcategory simply because they were sold in a box, or included a leaflet, or were described by reference to the word “clinical”, or (almost self-evidently) because they were more expensive. They presumably bought them because they associated those features with certain characteristics or qualities of the products in the subcategory. Prof. Klein did not indicate, from a marketing or consumer behaviour perspective, exactly what those characteristics or qualities were. To the extent that her evidence did touch on that issue, it tended to suggest that consumers simply perceived that the products in the clinical subcategory were high-strength or high-efficacy products for use, or intended use, by heavy sweaters.
Supermarket shelves and planograms
102 The major supermarkets determine how particular products, including antiperspirant deodorants, are to be placed on their shelves. They prepare “planograms” which depict how the various brands and product ranges are to be shelved.
103 Planograms prepared by Woolworths and Coles during the relevant period tended to reveal that the supermarkets generally grouped the Nivea Stress Protect Clinical Strength range together with the Rexona and Dove Clinical Protection range and the Mitchum Clinical range. Those products tended to be grouped together towards the middle of either the top or second top shelf of the shelving that housed antiperspirant deodorants. Photographs taken at various supermarkets also showed that the planograms were generally implemented.
104 Unilever tendered summaries of various consumer complaints received and recorded by Beiersdorf in relation to the Nivea Stress Protect Clinical Strength stick. The nature of some of those complaints is dealt with in more detail later in the context of the question whether the alleged representations, if made, were false or misleading. Some of the complaints, however, are also potentially relevant in considering whether the alleged representations were made.
105 The content of some of the consumer complaints tended to suggest that consumers did associate the Nivea Stress Protect Clinical Strength stick with the Rexona and Dove Clinical Protection range and the Mitchum Clinical range. One consumer, for example, said “I have previously used the same style deodorant Rexona and Mitchum”. Others reported that they had used Rexona Clinical Protection but thought they would “give Nivea a go” or “try the Nivea version”. One consumer reported that he or she had “changed from a similar deodorant from Rexona”.
106 Beiersdorf ceased supplying the Nivea Stress Protect Clinical Strength products in Australia on and from 31 December 2016.
107 The representations allegedly made by Beiersdorf, as pleaded in Unilever’s Further Amended Statement of Claim (FASOC), were as follows:
1. Nivea Stress Protect Clinical Strength is a product with similar antiperspirant efficacy and characteristics to the Clinical Products [FASOC 28(a)].
2. Nivea Stress Protect Clinical Strength is a product which will, if used, provide similar antiperspirant protection to the Clinical Products [FASOC 28(b)].
3. Nivea Stress Protect Clinical Strength is a product with greater antiperspirant efficacy than all other non-clinical antiperspirant deodorants ordinarily available from supermarkets in Australia [FASOC 28(c)].
4. Nivea Stress Protect Clinical Strength is a product which will, if used, provide a greater level of antiperspirant protection than all other non-clinical antiperspirants ordinarily available from supermarkets in Australia [FASOC 28(d)].
5. Nivea Stress Protect Clinical Strength is a product which has a similar efficacy in preventing stress sweat to the Clinical Products [FASOC 28(e)].
6. Nivea Stress Protect Clinical Strength is a product which will, if used, provide similar antiperspirant protection to the Clinical Products against stress sweat [FASOC 28(f)].
7. Nivea Stress Protect Clinical Strength is a product with greater antiperspirant efficacy in protecting against stress sweat than all other non-clinical antiperspirant deodorants ordinarily available from supermarkets in Australia [FASOC 28(g)].
8. Nivea Stress Protect Clinical Strength is a product which will, if used, provide a higher level of protection from stress sweat than all other non-clinical antiperspirant deodorants ordinarily available from supermarkets in Australia [FASOC 28(h)].
9. Nivea Stress Protect Clinical Strength has a particularly strong efficacy for consumers who suffer from stress sweat [FASOC 35(a)].
10. Nivea Stress Protect Clinical Strength will provide particularly strong protection against stress sweat [FASOC 35(b)].
11. Nivea Stress Protect Clinical Strength will, if used, provide a higher level of protection from stress sweat than all other non-clinical antiperspirant deodorants ordinarily available from supermarkets in Australia [FASOC 35(c)].
108 The term “Clinical Products” is defined in the pleading as comprising, essentially, the Rexona and Dove Clinical Protection range and the Mitchum Clinical range. While not specifically defined in the pleading, the expression “non-clinical [a]ntiperspirant [d]eodorants” would appear to include all antiperspirant deodorants other than the “Clinical Products”. The term “[a]ntiperspirant [d]eodorants” is defined as products which combine antiperspirant and deodorant characteristics.
109 Beiersdorf admitted that it made representations 9 and 10. It denied making any of the other representations.
110 It was common ground that representations 2, 4, 6, 8, 10 and 11 were representations as to future matters within the meaning of s 4 of the ACL.
111 It should perhaps be noted that representations 8 and 11 are in almost identical terms. Unilever did not explain why that was the case or whether anything turned on the different context in which those particular representations were pleaded.
112 While there are various differences between the representations, some of them fairly minor, it is possible and useful to group the representations into three groups: first, those that involve a representation that Nivea Stress Protect Clinical Strength was a product which had, or would if used have, similar antiperspirant efficacy and characteristics to the Clinical Products, or similar efficacy in preventing stress sweat to the Clinical Products (representations 1, 2, 5 and 6); second, those that involve a representation that Nivea Stress Protect Clinical Strength was a product which had, or would if used have, greater antiperspirant efficacy, or greater antiperspirant efficacy in protecting against stress sweat, than all other non-clinical antiperspirant deodorants ordinarily available from supermarkets in Australia (representations 3, 4, 7, 8 and 11); and third, those that involve a representation that Nivea Stress Protect Clinical Strength was a product which had a particularly strong efficacy or would provide particularly strong protection in relation to stress sweat (representations 9 and 10).
113 The first group will be referred to generally as the Similarity Representations; the second group will be referred to as the Superiority Representations; and the third group will be referred to as the Stress Sweat Representations. As has already been noted, Beiersdorf admitted that it made the Stress Sweat Representations.
114 It can be seen that each of the pleaded representations refer, in one way or another, to either “antiperspirant efficacy” or “antiperspirant protection”. At Beiersdorf’s request, Unilever provided further particulars of those expressions in the context in which they were used in the representations. Unilever’s further particulars stated, perhaps unhelpfully, that the expressions “similar antiperspirant efficacy” and “similar antiperspirant protection” were to be given their “ordinary English meaning”. More significantly, Unilever’s case as further particularised was said to be that the “criterion for efficacy and protection is a comparison of perspiration reduction, following use of antiperspirants by a consumer”. Similarly, it was said that the “criterion for efficacy in preventing stress sweat, acting against stress sweat and protecting against stress sweat is a comparison of stress sweat reduction following use of antiperspirants by a consumer”.
115 The pleaded representations must be read and construed having regard to the further particulars provided by Unilever. The criterion for the efficacy and protection of antiperspirant deodorants, on Unilever’s case, was strictly quantitative and limited to the amount by which the respective products reduced the amount of sweat that would otherwise have been excreted. The efficacy that the relevant products might have had in terms of preventing or masking odour associated with perspiration – the efficacy of the products as deodorants – was, on Unilever’s case, essentially irrelevant. As will be seen, there was a significant issue concerning whether the ordinary reasonable consumer of antiperspirant deodorants in Australia would have seen or perceived efficacy, or representations or claims about efficacy, in such narrow terms.
116 There are four principal issues.
117 The first issue is whether, in marketing, distributing and selling the Nivea Stress Protect Clinical Strength product in the way it did, Beiersdorf made any of the Similarity or Superiority Representations.
118 The second issue is whether the Similarity and Superiority Representations which did not involve representations as to future matters (representations 1, 3, 5 and 7), if found to have been made by Beiersdorf, were false. It should be noted in this context that, while Unilever pleaded that the Similarity and Superiority Representations were false, misleading or deceptive, it ultimately put its case solely in terms of the representations being false.
119 The third issue is whether the Stress Sweat Representation which did not involve a representation as to future matters (representation 9) was false.
120 The fourth issue is whether Beiersdorf had reasonable grounds to make such of the Similarity, Superiority and Stress Sweat Representations which involved representations as to future matters (representation 10, which Beiersdorf admitted to making, and representations 2, 4, 6, 8 and 11, if it is found to have made them).
Issue 1: Did Beiersdorf make the Similarity and Superiority Representations?
121 The first issue is whether, in marketing, distributing and selling the Nivea Stress Protect Clinical Strength product in the way it did, Beiersdorf made any of the Similarity or Superiority Representations.
122 The first point that should be made in respect of this issue is a rather obvious one. The point is that this is not a passing-off case, or at least not the usual type of passing-off case, where a trader who has established a reputation in a particular or distinctive name, “get-up”, or other trade indicia, alleges that a competitor had effectively appropriated that name or get-up and was thereby misleading consumers by representing that there was some association between the two rival traders or their products. Unilever did not allege that, by using the name “clinical”, or by selling its products in a box with a leaflet, or by selling its products at a price which was higher than other “non-clinical” antiperspirant deodorants, Beiersdorf misled, or was likely to have misled, consumers into believing that the Nivea Stress Protect Clinical Strength products were somehow associated or affiliated with Unilever or its Rexona and Dove Clinical Protection range. There was also no allegation that consumers were, or were likely to be, misled as to the source or origin of the Nivea Stress Protect Clinical Strength range. There could be little doubt that consumers were aware, or were likely to be aware, that Unilever’s Rexona and Dove Clinical Protection products and Beiersdorf’s Nivea Stress Protect Clinical Strength products were rival products that were marketed, distributed and sold by rival traders.
123 As Beiersdorf pointed out, it was not in any way prevented from using the word “clinical” in its product name or in its marketing, unless in doing so it misled or deceived consumers in some way. Nor was it prevented from selling its product in a box with a leaflet, again unless in some way it misled or deceived consumers. Beiersdorf argued that that was unlikely to be the case, at least in the conventional passing-off sense, in circumstances where it had clearly marked its product to distinguish it from Unilever’s products. In that regard, the following observations of Gibbs CJ in Parkdale were apposite (at 199-200):
Speaking generally, the sale by one manufacturer of goods which closely resemble those of another manufacturer is not a breach of s. 52 if the goods are properly labelled. There are hundreds of ordinary articles of consumption which, although made by different manufacturers and of different quality, closely resemble one another. In some cases this is because the design of a particular article has traditionally, or over a considerable period of time, been accepted as the most suitable for the purpose which the article serves. In some cases indeed no other design would be practicable. In other cases, although the article in question is the product of the invention of a person who is currently trading, the suitability of the design or appearance of the article is such that a market has become established which other manufacturers endeavour to satisfy, as they are entitled to do if no property exists in the design or appearance of the article. In all of these cases, the normal and reasonable way to distinguish one product from another is by marks, brands or labels. If an article is properly labelled so as to show the name of the manufacturer or the source of the article its close resemblance to another article will not mislead an ordinary reasonable member of the public.
124 The second point is perhaps equally obvious. With the possible exception of the Stress Sweat Representations, which were in any event admitted, Beiersdorf did not expressly make any of the representations. Neither the Nivea Stress Protect Clinical Strength advertisements, nor the get-up or other trade or marketing indicia or material, expressly stated that the Nivea product was or would be similarly efficacious, or would provide similar antiperspirant protection, to the products in the Rexona and Dove Clinical Protection range and the Mitchum Clinical range. No such statement was made on the relevant Nivea canisters, or the box in which they were sold, or in the leaflet that was included in the box. The marketing material did not contain or include any express comparison of any sort between the antiperspirant efficacy of the Nivea Stress Protect Clinical Strength products and the Rexona or Dove Clinical Protection and Mitchum Clinical products.
125 The Nivea Stress Protect Clinical Strength advertisements and other marketing material also did not expressly state that the products had greater antiperspirant efficacy than all other “non-clinical” antiperspirant deodorants. Nor was such a representation expressly made on the relevant Nivea canisters, or the box in which they were sold, or in the leaflet included in the box.
126 In those circumstances, Unilever’s case was, in substance, that the Similarity and Superiority Representations were to be implied or inferred from Beiersdorf’s conduct in marketing, distributing and selling the Nivea Stress Protect Clinical Strength range; that Beiersdorf’s conduct in that regard impliedly or implicitly conveyed the representations. Unilever contended, in short, that Beiersdorf had not employed the “primitive club of direct misrepresentation”, but had instead employed the “more sophisticated rapier of suggestion”: cf. Pacific Dunlop Ltd v Hogan (1989) 23 FCR 553 at 586.
127 It should be emphasised, in this context, that the question whether the representations were conveyed as alleged must be approached from the perspective of the relevant class of people who were, or were likely to be, misled or deceived by the representations if they were false as alleged. The relevant class of persons, having regard to the way Unilever pleaded its case, was the class of ordinary or reasonable consumers of antiperspirant deodorants in Australia. Unilever alleged that the relevant market was the Australian market for antiperspirant deodorants. While Unilever contended that there was a clinical subcategory or segment within the Australian market for antiperspirant deodorants, it did not go so far as to allege or contend that there was a separate market for so-called clinical antiperspirant deodorants.
128 Unilever’s case, in simple terms, was that the Similarity Representations and the Superiority Representations were implicitly or impliedly conveyed to ordinary reasonable consumers of antiperspirant deodorants by Beiersdorf’s marketing, distribution and selling of the Nivea Stress Protect Clinical Strength range having regard to particular features of the market for antiperspirant deodorants in Australia at the relevant time. In that regard, Unilever pointed, in particular, to evidence that suggested that there was a clearly established “clinical” subcategory or segment of the antiperspirant deodorant market in Australia. Prior to the launch of the Nivea product, the Rexona and Dove Clinical Protection range and the Mitchum Clinical range were essentially the only products in the clinical subcategory. Those products had particular and unique features: use of the word “clinical”; packaging in a box; the inclusion of a leaflet in the box; and a significantly higher price than products that were not within the clinical subcategory or segment.
129 Unilever’s case was that, when Beiersdorf launched its Nivea Stress Protect Clinical Strength range in Australia in July 2014, it consciously and deliberately launched it in the clinical subcategory or segment. It prominently used the word “clinical” on the canisters and packaging; it sold the product in a box; it provided a leaflet in the box; and it recommended that the product be priced at a price similar to the Rexona, Dove and Mitchum products in the clinical segment, being a price significantly higher than most, if not all, other antiperspirant products. Unilever contended that, in those circumstances, Beiersdorf impliedly conveyed to ordinary reasonable consumers of antiperspirant deodorants that, in general terms, the Nivea Stress Protect Clinical Strength product would have similar antiperspirant efficacy, or provide similar antiperspirant protection, as the antiperspirants that were already established in the clinical subcategory: the Rexona and Dove Clinical Protection antiperspirant deodorants and the Mitchum Clinical range.
130 Unilever also contended that, by acting as it did, Beiersdorf impliedly conveyed to ordinary reasonable consumers of antiperspirant deodorants that the Nivea Stress Protect Clinical Strength products had greater antiperspirant efficacy, or provided a greater level of antiperspirant protection, than all other “non-clinical” antiperspirant deodorants. “Non-clinical” antiperspirant deodorants, in that context, comprised all antiperspirant deodorants sold in Australian supermarkets other than the Rexona and Dove Clinical Protection range and the Mitchum Clinical range. The basis of that contention appeared to be that the ordinary reasonable consumer of antiperspirant deodorants would have perceived that “membership” of the clinical subcategory or segment entailed superiority over all other antiperspirant deodorant products.
131 It would be fair to say that the evidence, considered as a whole, did establish a number of the key factual components of Unilever’s case.
132 There could be little or no doubt, for example, that there was, or was at least perceived by consumers to be, a “clinical” subcategory or segment of the Australian market for antiperspirant deodorants. Beiersdorf’s internal marketing documents effectively recognised the existence of that category or segment. So too did Ms Braun in her evidence. The existence of the clinical segment was also consistent with Prof. Klein’s evidence concerning the established clinical “subcategory”. The supermarkets also appeared to recognise the existence of the clinical subcategory or segment; they grouped the members, or perceived members, of the segment together on their shelves.
133 The evidence also established that, as at July 2014, the clinical subcategory or segment was effectively occupied by the Rexona and Dove Clinical Protection range and the Mitchum Clinical range. There could be little doubt that those products were marketed, distributed and sold in a relatively distinctive way: prominent use of the word “clinical” in the product name and on the packaging; sale in a box with an instructional leaflet; a significantly higher price; and marketing and advertising which suggested that the products were suitable for people who were, or perceived themselves to be, heavy sweaters, or people who were concerned about the effects of heavy sweating.
134 There could also be little or no doubt that Beiersdorf launched the Nivea Stress Protect Clinical Strength range in such a way that the product would be perceived by consumers to fall within the existing clinical subcategory or segment. Indeed, according to Ms Braun, Beiersdorf consciously adopted the various “cues” of the existing products within the clinical subcategory: use of the word “clinical”; the box; the leaflet; and the comparatively higher price. By doing so, it may reasonably be inferred that Beiersdorf intended to, and effectively did, impliedly represent to ordinary reasonable consumers of antiperspirant deodorants that its Nivea Stress Protect Clinical Strength product belonged in the clinical subcategory or segment.
135 The critical question, however, is what membership of the clinical subcategory or segment itself conveyed, or was likely to convey, to ordinary reasonable consumers of antiperspirant deodorants? What did Beiersdorf impliedly represent to the ordinary reasonable consumer when it adopted the clinical subcategory “cues” and marketed its product in such a way as to position its product in the clinical subcategory? Did it, as Unilever contended, implicitly or impliedly represent to those consumers that Nivea Stress Protect Clinical Strength had similar antiperspirant efficacy, or provided similar antiperspirant protection, to the existing products in the clinical subcategory or segment, and superior antiperspirant efficacy to all other non-clinical antiperspirant deodorants? Or did it, as Beiersdorf effectively contended, only convey that the Nivea Stress Protect Clinical Strength products were Nivea’s highest strength, or most efficacious antiperspirant deodorant in its Stress Protect range, and were high-strength, or high-efficacy products, particularly in respect of stress sweat?
136 Those questions, while easy to pose, are by no means easy to answer. They raise a number of issues.
137 The first, and perhaps most critical, issue concerns the qualities or characteristics that the ordinary reasonable consumer of antiperspirant products may be taken to have expected of an antiperspirant deodorant which was effectively marketed as being within the clinical subcategory or segment. As was noted earlier, in the context of Prof. Klein’s evidence, it is, at best, doubtful that consumers would have bought an antiperspirant deodorant in the clinical segment or subcategory of the market simply because it included the word “clinical” in its name or get-up, or because it was sold in a box which included a leaflet, or because it was more expensive. They no doubt bought it because of what those features, in combination, conveyed or represented about the product itself; what they understood or believed to be the qualities or characteristics of a so-called “clinical” product.
138 The difficulty for Unilever is that the evidence, considered as a whole, ultimately established that the ordinary reasonable consumer of antiperspirant deodorants in Australia was, in all the circumstances, likely to believe or understand no more than that an antiperspirant deodorant in the clinical segment was one which was, or was said to be, a high-strength product, or a product which was highly efficacious and particularly suitable for people who were, or perceived themselves to be, heavy sweaters. In those circumstances, Beiersdorf’s conduct in marketing, distributing and selling the Nivea Stress Protect Clinical Strength range as belonging in the clinical subcategory or segment amounted to no more than a representation that its product was a product which was a high-strength product, or perhaps a highly efficacious product for heavy sweaters. It did not, as Unilever effectively contended, amount to an implied representation that the product met some specific benchmark of strength or efficacy, by reference to perspiration reduction, which had been established by the existing products in the clinical range.
139 There are a number of considerations that lead to that conclusion. They include: the relatively limited meaning that consumers were likely to give to the use of the word “clinical” in the circumstances; the nature of the so-called clinical subcategory or segment in the market for antiperspirant deodorants in Australia and what consumers were likely to infer from it; and the advertising in respect of the products within the clinical subcategory or segment, which emphasised high strength, but did not advert to any specific clinical benchmark. Questions also arise about how the ordinary reasonable consumer would be likely to understand and approach information or representations concerning the efficacy or strength of antiperspirant deodorants. Are they likely to see efficacy and strength simply in quantitative terms involving the reduction of perspiration, or do they also have regard to the deodorant qualities of an antiperspirant deodorant and perhaps other even more subjective or qualitative features?
140 Each of those considerations or issues will be discussed in turn.
Clinical, Clinical Protection and Clinical Strength
141 At the heart of this issue is the use of the word “clinical” and what it conveyed, or was likely to convey, to the ordinary reasonable consumer of antiperspirant deodorants when used in, or as part of, the name or marketing of an antiperspirant deodorant. That is not to deny the importance of the other cues, including the box, the leaflet and the price point. It was, however, the word “clinical”, in its various collocations, which appeared to define the subcategory or segment. It is difficult to imagine that Unilever would have commenced this action if Beiersdorf had not used the word “clinical” as part of the name for its product, but had simply sold it in a box, with a leaflet and at a comparable price.
142 It should be noted, in this context, that it was common ground that there was no regulatory or other relevant standard that applied to the Australian market for antiperspirant deodorants which prescribed when a product could or could not be called “clinical”. It was simply a word which certain companies who marketed, distributed and sold antiperspirant deodorants had adopted to describe their products.
143 What, then, was, or was likely to be, conveyed to ordinary reasonable consumers of antiperspirant deodorants by the word “clinical” in this context?
144 The ordinary meaning of the word does not greatly assist. Its meanings, according to the Macquarie Dictionary, include “pertaining to a clinic”; “pertaining to or used in a sickroom”; “pertaining to medical training carried out in a hospital”; “concerned with observations and treatment of disease in the patient … ”; and “scientific; involving professional knowledge and not affected by the emotions … ”. The word “clinic” also has various different meanings, including, again according to the Macquarie Dictionary: “a class of medical students which takes place in a hospital ward, where practical instruction in examining and treating patients is given”; “one of a number of out-patient sections of a hospital for the specialised treatment of particular conditions and diseases”; “any medical centre used for such treatments as X-rays, child care, vaccinations, etc.”; and “a hospital for private patients”.
145 It is difficult to see how any of those ordinary meanings of the word “clinical” could shed any relevant light on what would, or would likely be, conveyed to a consumer by use of the word “clinical” in the name or description of an antiperspirant deodorant. Did it connote that the product was suitable for use in or by a clinic; or that its use had been tested in a clinic; or that it was suitable for use in treating a condition akin to a disease, presumably heavy sweating?
146 The position is complicated further by the fact that the word “clinical” is used in different collocations in relation to the various products. In the case of Unilever’s products, it was used as part of the composite expression “Clinical Protection”. That would appear, in context, to describe a type or level of protection against sweat, or heavy sweating. The box and canister also included the words (albeit in considerably smaller letters): “clinical strength wetness protection”, which again would tend to suggest that the product was of a particular strength in terms of preventing wetness or perspiration.
147 The Mitchum product simply used the word “clinical”, either independently or as part of its name. At one stage, however, the box also included the words “maximum strength formula”. To the extent that that statement was linked to the word “clinical”, it again conveyed that the product was a high-strength product.
148 The Beiersdorf product used the word “clinical” as part of the composite expression “Clinical Strength”. That too appeared to convey that the product had a particular strength. The context in which that expression was used – after the name or words “Stress Protect” and before the words (albeit in considerably smaller letters) “against stress sweat” – would appear to suggest that the product had a particular strength in protecting against stress sweat.
149 Two further points should be made concerning the words used on the boxes of the respective products and in the accompanying leaflets.
150 The first point is that, to the extent that the word “clinical” may connote a particular strength, there was no specific statement or representation on any of the boxes, canisters or leaflets, which quantified, or specified, the criterion or reference point by which strength was to be measured. It was not suggested, for example, that the strength of the product was to be measured by reference to the reduction in sweat (or wetness) measured by weight, or volume, or percentage, or any other measure.
151 The second point is that, to the extent that the word “clinical” may have connoted a particular type or level of protection, that connotation appeared to relate to protection against both wetness and odour. Perhaps more importantly, the only suggested criterion or reference point by which protection against both wetness and odour was to be measured was time. The Rexona Clinical Protection box, for example, represented that the product provided “clinical strength wetness protection”, but also “motion activated odour protection”. The Dove Clinical Protection box stated that the product provided “clinical strength wetness protection” and “all-day freshness through odour fighting technology”. The Mitchum Clinical box stated that the product provided “48 hour odor protection and maximum 24 hour wetness protection”. The Nivea Stress Protect Clinical Strength box stated that the product provided “48h protection from heavy sweating and odour”.
152 It will be necessary to return to those two points later. Suffice it to say at this stage that, as noted earlier, Unilever’s case was that the representations conveyed by Beiersdorf involved the comparative efficacy and protection as between the respective products, with the specific criterion for efficacy and protection being perspiration reduction; meaning, presumably, a comparison of the weight or percentage of sweat (wetness) that the respective products stopped or prevented. The representations were not said to relate to the efficacy of the product in preventing or masking odour.
153 The important point to note at this stage is that the wording on the respective boxes and canisters, and in the respective leaflets, does not suggest that such claims or representations as were made concerning strength or protection were so limited and specific.
154 In all the circumstances, the meaning of the word “clinical” itself, as a marketing or descriptive term in the context of antiperspirant deodorants, was, at best, indeterminate and unclear. The evidence, such as it was, tended to suggest that, to the extent that the word had acquired any secondary meaning in the market for antiperspirant deodorant in Australia, that secondary meaning was no more than “strong” or “high strength”, particularly when used in the expression “clinical strength”; or “high efficacy”, in terms of protection against sweat and odour, particularly when used in the expression “clinical protection”. The evidence did not suggest that the word had acquired any secondary meaning amongst consumers of antiperspirant deodorants which involved or included a particular benchmark of antiperspirant strength or efficacy established by the Rexona and Dove Clinical Protection range, or the Mitchum Clinical range. Nor did it suggest that any secondary meaning involved any quantified, or quantifiable, amount of perspiration reduction.
The clinical subcategory or segment
155 As was noted earlier, Unilever’s case, to a large extent, hinged on what membership of the so-called clinical subcategory or segment conveyed, or was likely to convey, to the ordinary reasonable consumer of antiperspirant deodorants. In that regard, Unilever relied heavily on Beiersdorf’s internal marketing documents. Unilever contended that the activities and views of “traders” in the relevant market concerning the way consumers viewed their products and marketing was probative of how consumers were in fact likely to react to marketing. In Unilever’s submission, Beiersdorf’s internal marketing documents supported its case that membership of the clinical subcategory conveyed, or was likely to convey, to consumers that the product met a benchmark of “perspiration reduction” which had effectively been established by the existing products in that subcategory or segment.
156 The difficulty for Unilever, however, is that, while Beiersdorf’s internal documents clearly revealed that Beiersdorf recognised that there was a clinical subcategory or segment of the Australian antiperspirant deodorant market, they did not suggest that Beiersdorf believed or understood that ordinary reasonable consumers perceived, or were likely to perceive, that a product’s membership of that subcategory meant or conveyed anything other than that the product was a high-strength, or highly efficacious product. The documents certainly did not indicate that Beiersdorf believed or understood that, by adopting the “cues” for the clinical sector for its Nivea product, it was representing to consumers that the Nivea product had similar antiperspirant efficacy to the existing products in that segment, or that the Nivea product had greater efficacy than all the other products that were not in the segment.
157 The key passages from Beiersdorf’s internal marketing documents were referred to or extracted earlier in the context of the evidence concerning Beiersdorf’s launch of the Nivea Stress Protect Clinical Strength range. The documents noted that there was no legal or regulatory definition of “clinical strength” and that a product could be said to be clinical strength if it was “clinically proven” or more efficacious than standard antiperspirant deodorants. They also recorded that Beiersdorf recognised that Unilever established the “Clinical Protection” segment and “used this definition to imply superior product efficacy of their products in treating excessive sweating”. The clinical segment was also referred to as the “highly efficacious” segment.
158 Nothing in the documents suggested that Beiersdorf thought that consumers believed or understood that membership of the clinical subcategory or segment conveyed, or was likely to convey, to consumers that clinical products met a specific quantitative benchmark established by the existing members of the subcategory or segment. Nor do the documents suggest that Beiersdorf believed that consumers believed or understood that strength or efficacy in the clinical segment was to be quantified or measured solely in terms of perspiration reduction.
159 One of Beiersdorf’s internal documents recorded that Unilever’s existing products in the clinical subcategory or segment had “the highest loyalty, due to [their] benefit to provide advanced/strong protection against wetness and odour” and that, for the proposed Nivea Stress Protect Clinical Strength product to compete, it would have to “perform as well as (or better than) our key competitors”. That, however, appeared to reflect nothing more than Beiersdorf’s recognition of the commercial reality that the proposed Nivea entrant in the clinical segment was unlikely to be successful if it did not perform as well as, or better than, the competing products. It does not indicate that Beiersdorf believed or understood that, if it launched its product in the clinical segment, consumers were likely to perceive that as a representation that the product met some quantitative benchmark of strength or efficacy established by the existing products in the segment.
160 It should perhaps be noted in this context that Unilever initially appeared to contend that Beiersdorf’s internal documents revealed that it intended to mislead or deceive by making representations along the lines of the Similarity and Superiority Representations. Ultimately, however, that contention was not pursued. Unilever ultimately did not submit that an inference of the sort referred to in Australian Woollen Mills was available.
161 Ms Braun’s evidence, which was discussed earlier, was broadly consistent with the internal documents. She essentially saw that membership of the clinical subcategory or segment conveyed nothing more than that the product was a high-strength or highly efficient product in terms of protection against sweat and odour. Beiersdorf’s intention in adopting the “cues” for the clinical segment was “to say clearly, ‘[h]ere is a special stress sweat solution for heavy sweaters which is highly efficient’” and to reinforce “that these are specific products for heavy sweaters”.
162 Prof. Klein’s opinion evidence also did not assist, or greatly assist, in determining what membership of the clinical subcategory or segment conveyed, or was likely to convey, to the ordinary reasonable consumer of antiperspirant deodorants. As discussed earlier, her evidence was that consumers were very likely to classify Nivea Stress Protect Clinical Strength as being a “clinical product”, or as being part of the clinical “subcategory” of the antiperspirant deodorant “schema”. That opinion was based on, amongst other things, similarities between the advertising of the Nivea product and the advertising for “clinical protection products”: the price, the packaging in a box with the prominent display of the word “clinical”, and the use of the word “clinical” on the canister.
163 Prof. Klein did not, however, express any opinion at all about what membership of the clinical subcategory represented, or was likely to represent, to consumers of antiperspirant deodorants in Australia. Nor did she express any opinion concerning what was or was likely to have been represented to consumers by the fact that the Nivea Stress Protect Clinical Strength product was marketed, distributed and sold in the way it was, other than that the product had entered the clinical subcategory. Indeed, she did not express any opinion about the qualities or characteristics that the ordinary consumer was likely to expect of an antiperspirant deodorant which was marketed as falling within the clinical subcategory or segment, other than perhaps that clinical deodorants were distinct from other deodorants in that they were stronger and more efficacious.
164 Ultimately, such evidence as there was concerning what consumers were likely to perceive from a product’s membership of the clinical subcategory or segment suggested no more than that consumers were likely to think that products that were within that subcategory or segment, or purported to be within it, were high-strength or highly efficacious products which were particularly suitable for heavy sweaters. The evidence did not suggest that a product’s membership, or purported membership, of the clinical subcategory or segment would, or would be likely to, represent to consumers that the product met some quantitative benchmark of strength or efficacy established by the existing products in that subcategory or segment.
165 The limited nature of any representation arising from membership of the clinical subcategory or segment of the Australian market for antiperspirant deodorants may perhaps be illustrated by using an analogy touched on by Prof. Klein in her evidence. As noted earlier, Prof. Klein referred to a schema for soft drinks that would include Coke, Pepsi, Diet Pepsi, Sprite, Coke Zero, Fanta Orange and others. She also suggested that the soft drink schema or category might be organised into subcategories such as diet and non-diet. Prof. Klein also suggested that consumers would associate soft drinks within the diet subcategory, such as Diet Pepsi, as having the quality of low calorie.
166 In that context, let it be assumed that the diet subcategory at a particular point in time was occupied by, at least, Diet Pepsi and Diet Coke. Then let it be assumed that a rival soft drink company began to market and distribute a cola soft drink in such a way that it represented to consumers that the product belonged in the existing diet subcategory of the market for soft drinks. The product, for example, used the word “diet” prominently on its bottle or can. That marketing could readily be said to represent to consumers that the new entrant in the diet subcategory was, like the existing members, a low-calorie cola or soft drink. It is, however, unlikely that it could be said to have represented to consumers that the new entrant met some specific low-calorie benchmark that had been established by the existing members; that it had the same or a similar calorie count to Diet Pepsi and Diet Coke.
167 It must be emphasised that the diet soft drink example is entirely hypothetical. There was no evidence concerning the Australian soft drink market, or the diet subcategory of it, or consumer perceptions in relation to it. And, like all analogies, it is no doubt less than perfect. It does, nevertheless, tend to illustrate the point concerning the clinical subcategory or segment of the Australian market for antiperspirant deodorants and, more importantly, what membership of that subcategory or segment was likely to have conveyed to the ordinary reasonable consumer.
168 The evidence concerning the advertising of the respective products also established little more than that the relevant products were marketed or represented as being high-strength or highly efficacious products.
169 The advertisements relating to the Rexona and Dove Clinical Protection range emphasised that the products in that range were high strength and highly efficacious. The products were said to offer “twice the protection of a basic antiperspirant” and to be the most effective antiperspirant deodorant in Australia that “protects you twice as much”. It was also said that “nothing is stronger”. Beyond the general assertion of twice the protection, however, no express statement or representation was made in the advertising which suggested a particular quantitative benchmark referable specifically to the reduction of sweat.
170 The advertisements relating to the Nivea Stress Protect Clinical Strength range also focussed on strength and efficacy. The product was said to be “Nivea’s strongest protection against heavy stress sweat” and “Nivea’s strongest stress sweat solution”. It was also said to contain “the highest concentration and most advanced stress sweat fighting anti-perspirant ingredients”. Importantly, however, the advertisements said nothing about the Nivea products meeting any specific quantitative benchmark referable specifically to the reduction of sweat, let alone a benchmark established by the existing members of the clinical segment.
171 To the extent that there were any common themes in the respective advertisements, those themes were limited to very general assertions of high strength and high efficacy.
172 The following points may also be noted. First, the Nivea advertisements made no express representations concerning any comparison between the Nivea Stress Protect Clinical Strength products and the Rexona or Dove Clinical Protection products or the Mitchum Clinical products. Second, to the extent that the word “clinical” was used or displayed in the advertisements, it was primarily, if not exclusively, used or displayed in the context of the product name. Third, the representations concerning strength and efficacy in the Nivea advertisements were specifically directed at stress sweat.
“Similar” – The Similarity Representations
173 It may perhaps be accepted that, on a broad and somewhat superficial level, Beiersdorf’s marketing of the Nivea Stress Protect Clinical Strength range was likely to convey to the ordinary reasonable consumer of antiperspirant deodorants that the Nivea product was similar to the existing members of the clinical subcategory or segment: the Rexona and Dove Clinical Protection range and the Mitchum Clinical range. By adopting many of the “cues” or trade or marketing indicia of the pre-existing products in the clinical subcategory or segment (prominent use of the word “clinical”; the box; the leaflet; the higher price), Beiersdorf effectively represented that its Nivea product properly belonged in the clinical subcategory or segment of the Australian antiperspirant deodorant market. As has already been discussed, consumers were likely to perceive that products in that subcategory or segment of the market were, or were likely to be, high-strength or high-efficacy products designed for, or suitable for use by, heavy sweaters. It would follow that, by effectively representing that the Nivea Stress Protect Clinical Strength range properly belonged in the clinical subcategory or segment, Beiersdorf also effectively represented to consumers that the Nivea products were similar to the existing products in that subcategory in terms of them being high-strength or high-efficacy products for heavy sweaters.
174 Unilever’s case in respect of the Similarity Representations, however, depended on the proposition that Beiersdorf’s conduct represented not just that the Nivea Stress Protect Clinical Strength range was similar to the Rexona and Dove Clinical Protection range, and Mitchum Clinical, in that very broad and general sense. Unilever’s case was that Beiersdorf’s conduct also conveyed, or was likely to convey, to consumers that the Nivea product was similar to the Rexona, Dove and Mitchum products in terms of antiperspirant efficacy specifically by reference to a comparison of perspiration reduction, both generally and in relation to stress sweat. Unilever’s case was, in effect, that the existing products in the clinical subcategory or segment had established a quantitative benchmark in terms of sweat reduction and that, by positioning its product in the clinical subcategory or segment, Beiersdorf impliedly represented to consumers that its product met that benchmark.
175 There are, however, a number of difficulties or deficiencies in Unilever’s case in respect of the Similarity Representations. A number of them have already been touched on.
176 First, there was nothing to suggest that ordinary reasonable Australian consumers of antiperspirant deodorants perceived, or were likely to perceive, that membership of the clinical subcategory or segment of the market entailed or required the relevant product to meet a specific quantitative benchmark in terms of antiperspirant efficacy or antiperspirant protection, let alone a benchmark that was fixed, or had been established, by the existing products in that subcategory or segment. Rather, for the reasons largely already given, consumers were likely to simply regard membership of the clinical subcategory or segment to entail or require the product to be a high-strength or high-efficacy product in terms of protection against excessive sweat and the odour associated with it.
177 The evidence did not suggest otherwise. As has already been noted, the evidence did not establish that the word “clinical” had taken on a secondary meaning in the antiperspirant deodorant market in Australia which involved any particular quantitative benchmark in terms of antiperspirant reduction alone. To the extent that there was any secondary meaning in the market, it was a meaning which simply involved high strength or high efficacy in terms of protecting against sweat and odour. The boxes, canisters and leaflets associated with both the Rexona and Dove Clinical Protection range and Mitchum Clinical did not make any specific quantitative claims about antiperspirant efficacy or antiperspirant protection. Nor did the advertisements or marketing associated with the Rexona and Dove Clinical Protection range, beyond the broad statements that the products provided “twice the protection” and that “nothing [was] stronger”. The boxes, canisters and leaflets associated with the Nivea Stress Protect Clinical Strength range also did not contain specific quantitative claims about antiperspirant efficacy or protection. Nor did the advertisements relating to the Nivea product. The general statements that were made concerning the Nivea product were also only made in respect of stress sweat.
178 The evidence concerning the state of the relevant market, the market for antiperspirant deodorants in Australia, and the existence of a clinical subcategory or segment within that market, also did not establish that membership of the clinical subcategory or segment entailed anything more than high strength or high efficacy generally. The evidence did not establish that consumers perceived, or were likely to perceive, that before a product could be said to be within the clinical subcategory or segment, it had to meet any specific quantitative benchmark in terms of antiperspirant efficacy or antiperspirant protection, let alone one established by the existing members of the subcategory or segment.
179 It should also be reiterated in this context that the issue must be approached from the perspective of the ordinary reasonable consumer of antiperspirant deodorants in Australia. That class would include people who may not be heavy sweaters, or who may have never used any so-called “clinical” antiperspirant deodorants before. It cannot be assumed, therefore, that the ordinary reasonable consumer of antiperspirants would have, or would be likely to have had, a clear and detailed knowledge of the sweat reduction efficacy of the existing products in the clinical subcategory or segment in the market. It cannot be assumed that the ordinary reasonable consumer would know or believe that the existing products in the clinical segment had similar efficacies, in terms of sweat reduction, and therefore had established some sort of benchmark for membership of the segment.
180 Second, there was nothing to suggest that the ordinary reasonable consumer of antiperspirant deodorants in Australia would perceive, or would be likely to perceive, representations of high strength and high efficacy as necessarily being limited to the reduction of sweat in a quantitative sense. Rather, consumers were more likely to perceive strength and efficacy in more qualitative terms, which included, not only sweat reduction, but also the protection against, or masking of, unpleasant odour caused by or associated with sweat.
181 The evidence did not establish that the relevant consumers were likely to perceive high strength or high efficacy in terms that related only to a quantified or quantifiable level of sweat reduction. None of the marketing and advertising concerning any of the products, Rexona, Dove, Mitchum or Nivea, made any specific quantifiable claims concerning sweat reduction. As has already been discussed at some length, the claims that were made on the boxes and the canisters, and in the leaflets and advertising, were broad and general claims concerning protection against both wetness and odour. To the extent that any measure was provided, the specified criterion was usually time: the length of time that the product provided protection against wetness and odour.
182 Each of the relevant products was an antiperspirant deodorant. It was common ground that an antiperspirant deodorant is a product which combines both antiperspirant and deodorant characteristics. As has already been noted, the claims and statements on the boxes and the canisters, and in the leaflets, related to both wetness and odour.
183 Prof. Klein acknowledged that the advertisements relating to the relevant products emphasised the deodorant qualities of the products, as well as the antiperspirant qualities. That did not surprise her, as an expert in marketing, because “you want to cover the things that people are worried about, and if they’re worried about both, which they’re likely to be, then you would cover that”.
184 Ms Braun’s evidence was that the claims in the advertisements for the Nivea Stress Protect Clinical Strength product, including that it was Nivea’s “most advanced stress sweat fighting solution”, that it provided “clinical strength protection from stress sweating” and that it provided “[Nivea’s] strongest protection against heavy stress sweat”, related to both “antiperspirant and deodorising efficacy”. The claims did not solely relate to perspiration reduction. It should also be noted that the claims were made specifically in relation to stress sweating.
185 Ms Braun’s evidence was also that consumers do not think in “levels” when it comes to efficacy. When it was put to her in cross-examination that “users of Dove and Rexona cream sticks [the Clinical Protection range] had formed a certain expectation of a level of efficacy”, her answer was:
I think consumers, they don’t think in level of efficacy. It has to – it’s very simple. It has to work for them or not and especially heavy sweaters. You know, they go trial and error. When something works [for] them, then it’s an efficacious product and they stick with them.
186 Some of Unilever’s witnesses also accepted that the deodorant qualities of the Rexona and Dove products were an important part of the way the products were marketed and sold in Australia. Mr Mark McCarthy, who was a Marketing Director at Unilever, did not agree that the deodorant qualities of the Rexona and Dove products were “vital”, but nevertheless agreed that they were important. Dr Vernon Marti, who was a Clinical Manager employed by Unilever PLC in England, agreed that a consumer’s perception of antiperspirant efficacy is affected by the presence of fragrances in an antiperspirant product and that: “when a consumer uses an antiperspirant deodorant in the real world … their perception of efficacy will include perceptions about antiperspirant effect, deodorant effect and fragrance”.
187 The consumer complaint evidence adduced by Unilever also did not support the proposition that consumers saw strength and efficacy only in quantitative perspiration reduction terms. None of the complaints referred specifically to a comparison of sweat reduction in quantitative terms. Some of the complaints referred to efficacy in terms which included “odour control” and the elimination of body odour.
188 While it might perhaps be accepted that many consumers were likely to see the deodorant qualities of the relevant products as perhaps secondary to the antiperspirant or sweat reduction qualities, the elimination or masking of odour was nonetheless likely to be seen by consumers as having some importance in assessing the strength and efficacy of the products. The criterion for assessing efficacy adopted by Unilever in relation to the Similarity Representations effectively ignored the fact that the ordinary and reasonable consumer of antiperspirant deodorants in Australia was likely to view the efficacy and strength of antiperspirant deodorants, not only in terms of sweat reduction, but also in terms of the elimination or masking of odour.
189 There is an additional problem with the use of the word “similar” in the Similarity Representations, though it perhaps is a problem which is exposed more in the context of the question whether the Similarity Representations, if made, were false. The problem is that while Unilever’s case involved the comparison of the relevant products in a quantitative sense – quantified or quantifiable reduction of perspiration – the word “similar” is an indeterminate comparator. While the word “similar” is an ordinary English word which, in general terms, means having likeness or resemblance, it is difficult to know precisely what the measure or mark of similarity is in the context in which it is used in the Similarity Representations. It clearly does not mean that the Nivea product reduced the same amount, or a greater amount, of perspiration than the Rexona, Dove and Mitchum products, as Unilever appeared to contend in its opening submissions.
190 What, then, does “similarity” mean in this context? Is similarity to be measured in terms of the weight or volume of the perspiration that the respective products are able to prevent or reduce? Or is similarity to be measured in terms of the percentage of sweat reduced? Either way, what is the relevant range of disparity of results beyond which the products can be said to be dissimilar? Plainly the results would have to be relatively close if the products are to be regarded as similar, but how close? As will be seen, Unilever contended, in effect, that there only had to be some “statistically significant difference” between the test results for sweat reduction for the products to be dissimilar. It is not immediately apparent why that must be so. Perhaps more significantly, in the context of considering whether the Similarity Representations were conveyed, it is highly doubtful that the ordinary reasonable consumer of antiperspirant deodorants would be likely to think in those terms in assessing whether the products were similar in terms of their efficacy or level of protection.
Points of distinction – Stress sweat
191 Unilever’s case in relation to the Similarity Representations also tended to disregard, or minimise the significance of, some clear points of distinction in the marketing of the Nivea Stress Protect Clinical Strength range. The main point of distinction, of course, was that the Nivea Stress Protect Clinical Strength range was part of the broader “Stress Protect” range, which was marketed specifically at people who were concerned about stress sweat and the accompanying odour caused by stress sweat. That was certainly the focus of the relevant advertisements. The boxes and canisters included the words “Stress Protect” in a large orange font, almost as prominently as the words “Clinical Strength”. The words “Clinical Strength” were also accompanied by the words “against stress sweat”. The instructional leaflet included considerable information concerning the nature and causes of stress sweat.
192 Some of the products in the Rexona Clinical Protection range included, at least at some stage, a specific statement on the box that the product was “proven against stress sweat”. It could not be said, however, that protection against stress sweat was a major feature of the get-up or marketing of the Rexona product. The same could be said in relation to Mitchum Clinical.
193 Ms Braun’s evidence was that the Nivea product was to be “specifically marketed as having high efficacy against stress sweat” which would “distinguish it from other products in the market”.
194 Prof. Klein was cross-examined at some length about whether there might be a “stress” subcategory or segment in the market for antiperspirant deodorants. She appeared unwilling to accept that there was such a subcategory, though she had not actively considered or investigated whether that might be the case. It was not an issue raised in her instructions or the assumptions that she was asked to make for the purposes of her report. In those circumstances, little weight should be given to much of Prof. Klein’s evidence in respect of that issue. In any event, Prof. Klein’s evidence did not significantly detract from the point that, in its marketing of the Nivea Stress Protect Clinical Strength range, Beiersdorf appeared to be attempting to position the product, not only in the clinical segment or subcategory, but also in a perhaps new or emerging subcategory related to stress sweat.
195 While certainly not a major, let alone determinative, point, the fact that there was a relatively clear point of distinction between the Nivea Stress Protect Clinical Strength product, and the existing products in the clinical sector, tended to make it even less likely that Beiersdorf’s marketing of its product conveyed, or was likely to convey, the Similarity Representations to the ordinary reasonable consumer. While the overall effect of the marketing conveyed, or was likely to convey, that the Nivea product properly belonged in the clinical segment or subcategory, it also suggested that it belonged there because of its efficacy specifically in respect of stress sweat, rather than because it had a similar antiperspirant efficacy to the existing products, which were not specifically marketed by reference to their efficacy in dealing with stress sweat.
“Greater” antiperspirant efficacy or protection – the Superiority Representations
196 Unilever’s case in respect of the Superiority Representations was that, by marketing the Nivea Stress Protect Clinical Strength range as falling within the existing clinical subcategory, Beiersdorf thereby represented that its product had a greater antiperspirant efficacy or provided a greater level of antiperspirant protection, both generally and in relation to stress sweat, than all other “non-clinical” antiperspirant deodorants ordinarily available from supermarkets in Australia. “Non-clinical antiperspirant deodorants” in that context effectively meant all other antiperspirant deodorants other than deodorants in the Rexona and Dove Clinical Protection range and the Mitchum Clinical range. The evidence indicated that there were well over 500 different antiperspirant products which were sold in supermarkets in Australia.
197 It is difficult to see how Beiersdorf’s marketing of its Nivea Stress Protect Clinical Strength range could be seen to have conveyed such an absolute comparative proposition to ordinary reasonable consumers of antiperspirant deodorants in Australia.
198 For the reasons effectively already given, it may be accepted that membership of the clinical subcategory or segment, or the adoption of all the “cues” of that segment by Beiersdorf in respect of the Nivea Stress Protect Clinical Strength range, was likely to convey to the ordinary reasonable consumer of antiperspirant deodorants that the Nivea product was a strong or high-efficacy product. It was also likely to convey that the product was Nivea’s strongest and most efficacious product, particularly in respect of stress sweat. It does not follow, however, that in marketing the Nivea Stress Protect Clinical Strength product as being part of the clinical subcategory or segment, Beiersdorf represented to consumers that its product had greater efficacy, or provided greater protection than all other antiperspirant deodorants other than the existing Rexona, Dove and Mitchum products in the clinical subcategory. Nor were consumers likely to perceive the Nivea product’s membership of the clinical subcategory, or its adoption of the cues of that subcategory, in that way. That is particularly so, having regard to the narrow way that Unilever particularised the criterion for efficacy and protection: basically as involving nothing more than a comparison of sweat reduction.
199 Unilever’s case in relation to the Superiority Representations depended, in effect, on the proposition that a product’s membership, or claimed membership, of the clinical subcategory itself conveyed to the ordinary reasonable consumer that the product was more efficacious or provided a greater level of protection against sweat than every other antiperspirant product that was not in the clinical subcategory or segment. That proposition was not made out by the evidence, effectively for the reasons already given in the context of the Similarity Representations.
200 It should perhaps be noted, in this context, that, in one of the Rexona Clinical Protection advertisements, it was stated that the product was “the strongest antiperspirant deodorant in Australia” and that “nothing is stronger”. Another Rexona Clinical Protection advertisement included the claim that the product was “the most effective antiperspirant deodorant in Australia”. Those claims could perhaps be compared with the slightly more modest claim made in other Rexona and Dove Clinical Protection advertisements, which was that those products provided “twice the protection of a basic antiperspirant”. A few points can be made concerning those claims.
201 First, the claim that the products provided twice the protection of “basic” antiperspirants does not necessarily amount to a claim that they provided greater protection than “all” other antiperspirant deodorants.
202 Second, the claims would not necessarily have been perceived by consumers as relating only to antiperspirant efficacy, in terms of sweat reduction, as opposed to strength in terms of reducing sweat and eliminating or masking odour.
203 Third, and most significantly, consumers were unlikely to take from those claims that all products which were in the clinical subcategory or segment of the market therefore had greater antiperspirant efficacy than all other deodorants available in Australian supermarkets. They were claims made only in respect of the Rexona and Dove products.
204 Fourth, those claims were not made in or on any of the other Rexona and Dove Clinical Protection marketing material, including on the canisters, or on the boxes, or in the leaflets.
205 It should also be noted that none of the Nivea advertisements made any such claims.
206 In all the circumstances, the ordinary reasonable consumer would not have understood or believed, or was unlikely to have understood or believed, that a product’s membership of the clinical subcategory meant anything of substance more than that the product was a high-strength, or high-efficacy product that provided strong protection against sweat and associated odour, particularly for heavy sweaters, or people who believed that they were heavy sweaters or had a sweat problem. A product’s membership of the clinical subcategory would not, of itself, connote or represent to the ordinary reasonable consumer that the product was better at reducing perspiration, or was represented as being better at reducing perspiration, than all other antiperspirant deodorants that were not in, or did not claim to be in, the clinical subcategory. To conclude otherwise would be to read far too much into membership, or claimed membership of the clinical segment or subcategory. Consumers were also unlikely to see efficacy, strength or protection solely in terms of capacity to reduce perspiration. That would, amongst other things, ignore the efficacy, strength or protection in terms of reducing or masking odour associated with sweat, which was an important, albeit perhaps not the most important, feature of all antiperspirant deodorants, including those said to be in the clinical subcategory.
Conclusion in relation to the Similarity and Superiority Representations
207 Unilever has not discharged its burden of proving that Beiersdorf made any of the Similarity Representations (representations 1, 2, 5 and 6) or the Superiority Representations (representations 3, 4, 7, 8 and 11). The evidence, considered as a whole, does not support the conclusion that Beiersdorf, by its marketing, distribution and sale of the Nivea Stress Protect Clinical Strength range, made any of those representations. Those representations were not “reasonably open” or “reasonably available” meanings that consumers were likely to imply or infer from Beiersdorf’s conduct: cf. Tobacco Institute at 50; Coles Supermarkets at [47]. While the evidence supported the existence of a clinical subcategory or segment in the market for antiperspirant deodorants in Australia and that, in marketing, distributing and selling the Nivea Stress Protect Clinical Strength range, Beiersdorf adopted the “cues” of that subcategory or segment and positioned the Nivea product within it, that conduct did not convey any of the Similarity or Superiority Representations to the ordinary reasonable consumer of antiperspirant deodorants.
208 At its highest, Beiersdorf’s conduct conveyed, or was likely to convey, to the ordinary reasonable consumer, that the Nivea Stress Protect Clinical Strength range were high-strength or high-efficacy products that provided strong protection against sweat and associated odour, particularly for heavy sweaters, or people who believed that they were heavy sweaters or had a sweat problem. While, at a superficial level, that may have conveyed that the relevant Nivea products were similar to the Rexona, Dove and Mitchum clinical products, in the sense that those products were also said to be high-strength, highly efficacious products, it did not convey similarity in the narrow and specific sense of the Similarity Representations. Nor did it convey that the relevant Nivea products had greater antiperspirant efficacy, or provided a greater level of antiperspirant protection, to the many hundreds of other antiperspirant deodorants which were not, or were not said to be, in the clinical subcategory or segment.
Issue 2: Were the Similarity and Superiority Representations false?
209 Given that it has been found that Beiersdorf did not make any of the Similarity or Superiority Representations, it is strictly unnecessary to consider whether Unilever made out its case that those representations, if made, were false. Findings concerning the alleged falsity of the representations should nevertheless be made, particularly to avoid the necessity of remittal should it be found, on appeal, that the findings that have been made concerning the making of the representations are in some way erroneous.
210 As has already been noted, some of the Similarity and Superiority Representations (representations 2, 4, 6, 8, 10 and 11) are representations with respect to future matters for the purposes of s 4 of the ACL. The question whether Beiersdorf had reasonable grounds for making those representations will be considered separately.
211 There are essentially two critical questions that must be answered in relation to Unilever’s case that the Similarity and Superiority Representations, if made, were demonstrably false.
212 The first question is whether Unilever proved, on the balance of probabilities, that the Nivea Stress Protect Clinical Strength products did not have similar antiperspirant efficacy to the Rexona and Dove Clinical Protection products and the Mitchum Clinical product, either generally or with respect to stress sweating. The criterion in respect of antiperspirant efficacy, in this context, involves a comparison of perspiration reduction following use of an antiperspirant deodorant. This question essentially addresses the alleged falsity of the Similarity Representations.
213 The second question is whether Unilever proved, on the balance of probabilities, that the Nivea Stress Protect Clinical Strength products did not have greater antiperspirant efficacy than all other “non-clinical” antiperspirant deodorants, either generally or with respect to stress sweating. “Non-clinical” antiperspirant deodorants, in this context, means all other antiperspirant deodorants other than the Rexona and Dove Clinical Strength products, and the Mitchum Clinical products. The criterion in respect of antiperspirant efficacy in this context again involves a comparison of perspiration reduction following use of an antiperspirant deodorant. This question essentially addresses the alleged falsity of the Superiority Representations.
214 It should be reiterated that, while Unilever pleaded that the Similarity and Superiority Representations were variously false, misleading or deceptive, or likely to mislead or deceive, its case was ultimately put solely on the basis that the representations were false.
215 Finding the answers to the two critical questions is, once again, by no means easy. It necessarily involves an excursion through numerous different types of laboratory tests relating to the comparative or relative antiperspirant efficacy of the respective products, challenges to aspects of the utility and methodology of those different tests, and the analysis and interpretation of the relevant test results, including some issues concerning statistical analysis. There were differing expert opinions concerning most of those matters. The resolution of the questions was made even more difficult by some ultimately unnecessary or immaterial debates about some scientific background, including sweat gland physiology, sweat production and how antiperspirants work.
216 Before embarking on the required excursion through the evidence and submissions concerning the relevant tests and test results, and more significantly before even attempting to answer the critical questions, it is necessary to address a number of the key issues that divided the parties in relation to the testing and test results.
Similarity, statistical significance and perceptibility
217 The issue concerning the alleged falsity of the Similarity Representations must be considered on the basis of the representations as pleaded and particularised by Unilever. It follows that the criterion for determining whether or not the respective products have “similar antiperspirant efficacy” or provide “similar antiperspirant protection” is a comparison of perspiration reduction following the use of antiperspirants by a consumer. What Unilever’s particulars do not address, however, is exactly what is meant by “similar” in this context. It is no real answer to simply say that the word “similar” bears its ordinary English meaning.
218 Unilever’s case was not that Beiersdorf represented that the antiperspirant efficacy of its Nivea products was identical to, or greater than, the antiperspirant efficacy of the Rexona and Dove Clinical Protection products. If that had been Unilever’s case, the laboratory test results may have been, or at least been capable of being, definitive.
219 Unilever’s case was that Beiersdorf represented that the antiperspirant efficacy of its products was similar to its products. The difficulty, however, is that two things may be said to be “similar” even if they are not the same. Some degree of difference is tolerated before the two things can be said to be dissimilar. It follows that the antiperspirant efficacy of the Nivea Stress Protect Clinical Strength products may be considered to be similar to the antiperspirant efficacy of Rexona and Dove Clinical Protection even if there is a difference between the efficacy of the respective products.
220 The question is: at what point does a difference in the antiperspirant efficacy of the respective products mean that they are not similar?
221 Unilever provided no answer to that question. It certainly did not specify any quantitative measure of difference, either in terms of weight, volume or percentage of sweat reduced, which would make the respective products dissimilar. In its oral submissions, Unilever initially appeared to concede that it would need to prove that any difference in the antiperspirant efficacy of the respective products would need to be significant or even substantial before it could be said that they were not similar. It then appeared to retreat to the position that it would be sufficient for it to prove that there was a “statistically significant” difference between the laboratory test results.
222 If Unilever’s final position was that it was sufficient to prove that there was some “statistically significant” difference between the laboratory test results for it to prove that the products were not similar, that submission is rejected. To say that a test result was “statistically significant” generally says no more than that the result was beyond an accepted margin of error. The representations in issue in this case were alleged to have been made to, or to have misled or deceived, consumers of antiperspirant deodorants in Australia. It is difficult to accept, in that context, that ordinary reasonable consumers of antiperspirant deodorants would see two antiperspirant products as being dissimilar, in terms of their antiperspirant efficacy, simply because laboratory tests revealed that there was some “statistically significant” difference, in terms of a difference beyond an accepted margin of error, between them. What if the difference was “statistically significant”, but nonetheless so small that no consumer would ever be able to perceive that difference?
223 There ultimately could be little doubt that the question of the perceptibility of any proven difference between the relevant products was at least relevant in determining whether the antiperspirant efficacy of two products could be said to be similar or not similar. It is difficult to accept that the antiperspirant efficacy of two products could be said to be not similar simply because laboratory tests showed a “statistically significant” difference, unless it could also be established that the difference was one which was likely to have been perceived by a consumer. There may, of course, be circumstances where perceptibility would be an available or even obvious inference from the test result itself. That would, however, depend on the nature of the test and the nature of the result.
224 The potential relevance of perceptibility is supported, to a certain extent, by some of what was said by the Food and Drug Administration agency of the United States of America (FDA) in a monograph published by it in the Federal Register in 2003. That monograph was entitled “Antiperspirant Drug Products For Over-the-Counter Human Use; Final Monograph” (the FDA Monograph).
225 The FDA Monograph is a long and very dense document. It is not always easy to understand. In it, the FDA considered, amongst other things, the testing and test results which it considered, from a regulatory perspective, would be required to sustain various claims concerning the effectiveness of antiperspirant deodorants. In that context, the FDA considered both objective gravimetric tests, which determined the amount of sweat reduction, and user perception tests, which tested the user’s perception of the effectiveness of the antiperspirant.
226 The FDA appeared to accept the potential relevance of user perception tests. It appeared to conclude, for example, that user perception tests were able to substantiate “emotional sweating, 24-hour protection and extra effective claims”. It also appeared to conclude, however, that if gravimetric testing was able to show a 30% reduction in sweat (for “extra effective” claims) or a 20% reduction in sweat (for “emotional sweating and 24-hour protection” claims), no further user perception testing was required to substantiate those claims. That conclusion appeared to be based, at least in part, on user perception tests which showed that a statistically significant number of subjects were able to perceive that an antiperspirant deodorant which contained 25% of a particular active was more effective than an antiperspirant deodorant which contained only 10% of that active. The FDA’s conclusion was expressed in the following terms:
The agency has determined that the studies indicate that gravimetric testing shows an adequate difference between a standard antiperspirant (with a 20-percent reduction in sweat) and an antiperspirant with at least a 30-percent reduction in sweat, as required by the Panel, to support an “extra effective” claim. The agency stated in the tentative final monograph (47 FR 36492 at 36499) that once the level of activity that is perceivable by users has been established using the Panel’s recommended guidelines, it will not be necessary to perform user perception testing on individual products. Accordingly, the agency concludes that no further user perception testing is necessary for an “extra effective” claim, which is being included in the monograph for those antiperspirant products that reduce underarm perspiration by 30 percent or more using the guidelines for effectiveness testing of antiperspirant drug products referred to in §350.60.
227 Unilever appeared to contend, based on the views of its expert witnesses, that this amounted to a finding by the FDA that a consumer can perceive the difference between a product with an absolute efficacy of 20% and a product with an absolute efficacy of 30%. Whatever the views of the experts may have been, that does not appear to have been what the FDA was saying. The FDA appeared to be simply saying that, for regulatory reasons, a manufacturer or supplier of a product which could show, by gravimetric testing, that the product could reduce sweat by 30% or more, could claim that the product was “extra effective” without having to perform additional user perception tests. That is not to say that user perception is not potentially relevant in assessing claims concerning effectiveness, particularly comparative claims.
228 In any event, and putting to one side what the FDA may or may not have said about user perception tests, or user perception generally, it is difficult to see how it could be concluded that the antiperspirant efficacy of two products could be said to be dissimilar simply on the basis that laboratory testing showed a “statistically significant” difference between the amount of sweat that the products reduced under test conditions. If the difference was very small, or relatively insignificant, having regard to the overall amount of sweat reduced, such that the difference would be unlikely to be perceived by consumers, on what realistic basis could it be said, from a consumer’s perspective, that the efficacy of the products was not similar?
229 As will be seen, the issue concerning the relevance of the perceptibility of differences in sweat reduction detected by laboratory tests is not a merely academic issue.
Head-to-head testing and absolute testing
230 Unilever relied heavily on so-called “head-to-head” tests. Head-to-head testing is the term used to describe clinical tests conducted to compare efficacy between two products: for example, a Rexona Clinical Protection antiperspirant deodorant versus a Nivea Stress Protect Clinical Strength antiperspirant deodorant. In simple terms, the two products that are to be compared are applied to a person (subject) under controlled conditions, one under the right arm and one under the left. The subject is then exposed to either thermal (heat) or stress conditions for a fixed period to induce sweat. The amount of sweat produced by the subject under each arm is then measured by weight and the difference is statistically analysed.
231 Beiersdorf did not rely on any head-to-head testing. Rather, to the extent that it relied on any tests, it relied on so-called “absolute” testing. Unilever also relied on some absolute testing. Absolute testing is the term used to describe clinical tests conducted to provide information about the overall or absolute efficacy of a particular antiperspirant deodorant. The test itself does not involve any direct comparison with another product. In general terms, absolute testing employs the same methodology as head-to-head testing, but with the antiperspirant deodorant applied under one of the subject’s arms, and no product at all, or a placebo, applied under the subject’s other arm. The amount of sweat produced by the subject, under each arm, is then measured by weight. The difference represents the absolute efficacy of the product. While the results of absolute tests of different products can be compared, there was general agreement between the experts that there were risks and shortcomings in such an exercise.
232 The evidence of Unilever’s expert witnesses, Dr Iain Weddell and Dr Marti, tended to indicate that head-to-head tests were the optimal and only definitive way to test the comparative efficacy of two products. That is because two products are tested in different axillae (armpits) in a single test in controlled conditions. A comparison of products using two absolute tests, on the other hand, involves a comparison across tests, which introduces variability into the comparison. For example, the different tests may have involved different protocols, there may have been differences between the subjects involved in the different tests and there may have been differences in the conditions between the tests.
233 Beiersdorf’s expert, Dr Schmidt-Rose, initially expressed the view that it was possible to compare absolute test results of different products as a means of determining comparative product efficacy by utilising a process involving the “statistical normalization” of data to compensate for “intra-individual day-to-day variations”. That evidence was the subject of considerable cross-examination and, ultimately, revision by Dr Schmidt-Rose. He eventually accepted that a comparison of absolute test results had certain limitations. He also indicated that the statistical normalisation process could not be used to compare absolute stress test results without the availability of baseline sweat measurements before application of the product.
234 Ultimately, Beiersdorf accepted that head-to-head tests were the most reliable and useful means to assess whether one product was more efficacious than another. Dr Schmidt-Rose agreed that the best way to determine whether there was a difference between two products would be to do a head-to-head test. His evidence, however, was that a head-to-head test alone would not give any reliable indication of the significance or materiality of the difference between the two products. To obtain an indication of the significance of the difference, it would be necessary to also have a baseline measurement.
235 The general effect of Dr Schmidt-Rose’s evidence on that point was that, if the results of a head-to-head test were only expressed in terms of a relative comparison, in percentage terms, between the two products based on the average amount of sweat excreted, the significance or relative size of the difference could only be ascertained if there was some measure of the absolute reduction of perspiration. If, for example, the absolute amount of sweat reduction was very small, even a large percentage difference between the sweat reduction efficacy of the two rival products might mean that the difference, expressed in terms of sweat reduction by weight, may be fairly insignificant. Indeed, it might be so insignificant that it would not be able to be perceived by a customer. Conversely, if the amount of absolute sweat reduction by both products was large, meaning that the absolute efficacy of the two products was high, even a relatively large percentage difference between the sweat reduction efficacy might mean that the overall sweat reduction of the respective products, expressed in percentage terms, might not be significantly different.
236 The issue concerning the importance of baseline measurements is considered in more detail later in the context of specific tests and test results. In short terms, Beiersdorf maintained that simply proving, by way of a head-to-head test, that one product was more efficacious than another in terms of reducing perspiration does not prove that they are not “similar” in terms of their antiperspirant efficacy. That is because it is necessary to determine the degree or significance of the difference. In Beiersdorf’s submission, that effectively cannot be done in the absence of a baseline measurement of absolute sweat reduction. It followed that Unilever’s head-to-head test results could not alone prove that the antiperspirant efficacy of Nivea Stress Protect Clinical Strength was not similar to the antiperspirant efficacy of Rexona Clinical Protection.
237 Unilever disagreed with that analysis, at least in the context of the relevant test results. It contended that, considered in context, including in the context of the results of some absolute tests that Unilever had conducted, the results of the head-to-head tests expressed in percentage terms could prove that the respective products were not similar.
238 In a sense, this issue highlights the difficulty with the Similarity Representations which was adverted to earlier: the somewhat indeterminate nature of “similarity” as a comparator. Unilever did not nominate or specify what degree of difference was sufficient to establish that the two products were not similar in terms of their antiperspirant efficacy. It simply asserted that the difference revealed by the relevant tests was such that the products were not similar. Had the Similarity Representations been pleaded or particularised in more specific terms, this issue would not have arisen, or at least it may not have been so acute.
Thermal sweat tests and stress sweat tests
239 Thermal sweat is the term used to describe sweat that is produced in response to a thermal (heat) stimulus. Thermal testing is the term used to describe clinical tests conducted to measure the performance of antiperspirants against thermal sweat. In simple terms, those tests generally involve exposing the subjects, to whom the relevant antiperspirant deodorant or deodorants have been applied, to heat in controlled circumstances. The amount of sweat excreted in those circumstances is then measured.
240 Stress sweat, which is sometimes also referred to as “emotional sweat”, is the term used to describe sweat produced in response to an emotional stimulus. Stress testing is the term used to describe clinical tests conducted to measure the performance of antiperspirant deodorants against stress sweat. In general terms, those tests generally involve exposing the subjects to some emotional stimuli under controlled circumstances and measuring the amount of sweat excreted under those circumstances.
241 As has been seen, some of the Similarity and Superiority Representations concern the comparative antiperspirant efficacy of the Nivea Stress Protect Clinical Strength product with respect to stress sweating. In seeking to prove that the representations which related specifically to stress sweat were false, Unilever relied, at least to some extent, on thermal test results to prove the comparative efficacy of the respective products in respect of both stress and thermal sweat. There was, however, an issue between the parties, as to whether thermal tests can provide reliable results in respect of stress sweat. Beiersdorf ultimately submitted that the Court would be “hesitant” to accept that thermal tests accurately predict the efficacy of an antiperspirant deodorant in relation to stress sweat. Unilever submitted that the Court should find that thermal tests accurately predict stress sweat efficacy.
242 Unilever’s position was based on the proposition, supported by its expert, Dr Weddell, that the mechanism by which an antiperspirant blocks thermal sweat and stress sweat is essentially the same. Dr Weddell’s evidence was, in brief terms, that sweat is produced by both the eccrine glands and the apocrine glands. A thermal stimulus triggers production of sweat from the eccrine gland only, whereas an emotional stimulus triggers production of sweat from both the eccrine and apocrine glands. Importantly, however, Dr Weddell’s evidence was that antiperspirants act only on the eccrine glands, not the apocrine glands. Equally importantly, according to Dr Weddell, was the fact that antiperspirants block eccrine glands effectively by the same mechanism and in the same way, irrespective of whether the eccrine gland is stimulated by a thermal stimulus or a stress stimulus. Therefore, in Dr Weddell’s opinion, a formulation which is effective in blocking eccrine sweat will operate with the same efficacy against perspiration from the eccrine gland, whether the perspiration is caused by heat or stress.
243 Beiersdorf’s position was informed by the evidence of its expert, Dr Schmidt-Rose. His evidence, at least initially, was that “efficacy against thermal sweat is no necessary indication of a similar level of efficacy against stress sweat”. He initially went further and still asserted that the results of one of Unilever’s thermal studies of the Nivea product were “irrelevant” to whether the product exhibited high efficacy against stress sweat. In Dr Schmidt-Rose’s opinion, “[t]he kinetics and value of the flow rate (i.e. amount secreted per time) [of sweat] can differ substantially depending on whether the stimulus is an emotional one or a thermal one”. His evidence was that, in the case of a heat stimulus, it takes some time for sweat to flow, and when it does, it does so in small increments. In the case of an emotional stimulus, “the body reacts very quickly and high sweat flow rates can be achieved within minutes if not seconds”. Accordingly:
… a formulation which is effective in blocking sweat which is caused by heat, may not necessarily be equally or similarly effective in blocking sweat which is caused by stress, or vice versa, as the “mechanical challenge” for the antiperspirant plug to block sweat which is caused by stress may be different (i.e., there could be more initial sweat and faster onset of sweat in response to stress but no continuous sweating after the stress stimulation is removed).
244 It would be fair to say, however, that in the course of cross-examination, Dr Schmidt-Rose retreated somewhat from the fairly emphatic position that he initially took in respect of this issue. The cross-examination also exposed some weaknesses in his reasoning. First, Dr Schmidt-Rose conceded that the results of a thermal study would not be irrelevant in determining efficacy in respect of stress sweat, but rather would not provide an “exact indication of what the outcome of a stress test would be”. Second, Dr Schmidt-Rose effectively conceded that a publication which he initially cited as support for his opinion in fact provided no support. Third, the only real support that Dr Schmidt-Rose could point to in respect of his “hypothesis” concerning the different “mechanical challenge” presented by stress sweat was “common sense” and “basic physics” or “hydrodynamics”.
245 While Unilever was critical of Dr Schmidt-Rose’s hypothesis, it should be noted that its expert, Dr Weddell, accepted that it made “sense to him as a scientific hypothesis of how the underarm perspires”. Dr Weddell also appeared to accept that stress sweat involved a faster flow and that, having regard to the different “rates” of sweating as between thermal and stress sweat, “antiperspirants may well block at different efficiencies when you compare one stimulation to the other”. Dr Weddell’s point was that he did not know of any studies that either verified or contradicted that hypothesis.
246 In its final written submissions, Unilever also relied on parts of the FDA Monograph. In one part of the FDA Monograph, the FDA noted that it had “determined that gravimetric sweat tests combined with mental stress tests support an emotionally-induced sweating claim”. The FDA Monograph then explained the nature of the relevant sweat tests and the data obtained therefrom. The passage relied on by Unilever, which appears in the FDA Monograph after that discussion, was as follows:
The products tested under the emotional sweat protocol were also evaluated under a standard thermal sweat protocol at 100 oF with 30 percent relative humidity. The average percent sweat reduction for aerosols was 37.0 percent for emotional sweating and 34.0 percent for thermal sweating, for sticks it was 46.0 percent for emotional sweating and 41.4 percent for thermal sweating, and for roll-ons it was 51.3 percent for emotional sweating and 53.3 percent for thermal sweating. These data show that the same products have similar average percent sweat reduction for both emotional and thermal sweating.
The agency concludes that gravimetric sweat tests combined with mental stress tests are sufficient to show effectiveness for control of emotionally-induced sweating; the data show antiperspirant drug products that are effective for thermal sweating are also effective for emotional sweating. The agency has determined that no additional testing (e.g., user perception tests) is required for an emotionally-induced sweating claim for products containing monograph ingredients that meet the guidelines for effectiveness testing of antiperspirant drug products referred to in §350.60.
247 It is doubtful that this passage provided any real support for Unilever’s broad proposition that thermal tests accurately predict stress sweat efficacy. The FDA simply referred to the results of its testing, which tended to show that the particular products that were tested returned similar average sweat reduction for both emotional and thermal sweat. That is not to say, however, that the particular thermal tests carried out by the FDA accurately predicted stress sweat efficacy, let alone that that would always be the case in respect of any thermal test and any antiperspirant deodorants. Unilever also appeared to interpret this passage from the FDA Monograph as suggesting that the FDA allowed claims to be made about stress sweat efficacy solely on the basis of thermal testing. It is by no means entirely clear that the FDA was saying that. Indeed, the FDA seemed to be saying that, for regulatory purposes, thermal testing “combined with” stress testing could support efficacy claims concerning stress sweat without the need for further user perception tests.
248 Ultimately, Unilever’s emphatic and unqualified claim that thermal tests accurately predict stress sweat was not supported by the evidence and cannot be accepted. Nor, however, can the position initially taken by Dr Schmidt-Rose, which was, in effect, that thermal tests were irrelevant in determining efficacy in respect of stress sweat. The better view would appear to be that, given the different way that the body reacts to heat and emotional stimuli, thermal tests, while perhaps relevant, may not be the best indicator of specific stress sweat efficacy. That perhaps explains why specific stress tests were developed and utilised, including by the FDA.
249 The implications of this finding will be considered later in the context of the relevant tests conducted by Unilever and Beiersdorf.
250 It should also be noted in this context that, in his evidence, Dr Schmidt-Rose referred to another FDA publication, referred to generally as the FDA Guidelines: “Guidelines for effectiveness testing of OTC antiperspirant drug products”. That publication, as its title suggests, contained the FDA’s guidelines for thermal testing of antiperspirant deodorants. While there was much debate about what was said in the FDA Guidelines, ultimately not much turned on it.
251 As was noted earlier in the context of the facts concerning the launch of the Nivea Stress Protect Clinical Strength range, before launching the range, Beiersdorf conducted blind home user tests. In simple terms, those tests involved providing a relatively large number of test participants with unmarked versions of the relevant products. The participants were then given instructions concerning the use of the products and were asked to fill in a daily diary and a post-usage questionnaire which asked a series of questions concerning their experiences and perceptions of the products.
252 Beiersdorf did not contend that it could rely on the blind home user tests as proof of clinical or scientific levels of efficacy. Rather, it relied on the results of the tests as supporting the inference that consumers could not readily perceive any relevant differences in efficacy as between the Nivea Stress Protect Clinical Strength products and the Rexona and Dove Clinical Protection products. That in turn supported the proposition that, while Unilever’s laboratory testing may have shown that there were statistically significant differences between the amounts of sweat reduced by the respective products, those differences were not, or were unlikely to be, such that they were perceived by consumers. It also contended that the tests provided some measure of support for its case that it had reasonable grounds for making the alleged representations concerning future matters.
253 The potential relevance or significance of the blind home user tests conducted by Beiersdorf in the context of the launch are considered separately to the thermal and stress laboratory tests.
Unilever’s head-to-head tests and test results
254 Unilever relied on the results of five head-to-head tests involving some of the relevant products. Three of the head-to-head tests were thermal tests and two were stress tests. Unilever adduced evidence concerning the methodologies or protocols employed in carrying out those tests. It is unnecessary to consider that evidence in detail. To the extent that Beiersdorf mounted any challenge or criticism of the thermal test methodologies or protocols, that challenge or criticism is addressed in the context of the results of test #2. Beiersdorf’s arguments concerning the significance of the absence of any baseline in the tests is also considered in that context. Beiersdorf mounted a significant challenge to, or criticism of, the methodology or protocol utilised by Unilever in its stress tests. That issue is considered later in the context of test #3.
Test #1 – Head-to-head thermal test between Rexona Clinical Protection and Mitchum Clinical
255 Test #1 was a head-to-head study to test the relative sweat weight reduction of Rexona Men Clinical Protection AP Soft-Solid Sport and Mitchum Men Clinical AP Soft-Solid Oxygen Sport. The study was a three application, 24-hour and 48-hour hot room sitting study. There were 32 subjects, all female. The test was conducted in a laboratory in the Philippines in January 2014 by Ms Kathleen Lucas, a Research and Development Assistant Manager employed by Unilever Philippines Inc.
256 The results of the test were, relevantly:
At 24 hours, an average of 0.2201 grams of sweat was excreted from the underarms of those subjects to whom the Rexona product had been applied and 0.2270 grams of sweat was excreted from the underarms of those subjects to whom the Mitchum product had been applied.
At 48 hours, an average of 0.3002 grams of sweat was excreted from the underarms of those subjects to whom the Rexona product had been applied and 0.3064 grams of sweat was excreted from the underarms of those subjects to whom the Mitchum product had been applied.
257 The conclusion drawn by Ms Lucas was that there was no significant difference between the clinical wetness control afforded by the Rexona and Mitchum products after either 24 or 48 hours.
258 The result of test #1 was of some relevance to Unilever’s case because the Similarity Representations involved a comparison between Nivea Stress Protect Clinical Strength and the “Clinical Products”, which included Mitchum Clinical. Since test #1 established that the antiperspirant efficacy of Rexona Clinical Protection and Mitchum Clinical was not significantly different, Unilever contended that it was unnecessary to conduct further tests comparing Mitchum Clinical to Nivea Stress Protect Clinical Strength. As will be seen, however, Unilever did not conduct any head-to-head tests involving Dove Clinical Protection, which was also one of the “Clinical Products”.
Test #2 – Head-to-head thermal test between Rexona Clinical Protection and Nivea Stress Protect Clinical Strength
259 Test #2 was a head-to-head thermal study to test the relative sweat weight reduction of Rexona Clinical Protection Shower Clean Sport and Nivea Stress Protect Clinical Strength. The study was a three application, 24-hour and 48-hour hot room sitting study. There were 32 subjects, all female. The test was conducted in a laboratory in the Philippines in September 2014 by Ms Lucas.
260 The results of the test were:
At 24 hours, an average of 0.1367 grams of sweat was excreted from the underarms of those subjects to whom the Rexona product had been applied and 0.2065 grams of sweat was excreted from the underarms of those subjects to whom the Nivea product had been applied.
At 48 hours, an average of 0.1737 grams of sweat was excreted from the underarms of those subjects to whom the Rexona product had been applied and 0.2295 grams of sweat was excreted from the underarms of those subjects to whom the Nivea product had been applied.
The percentage sweat weight reduction (SWR), being a measure of the relative efficacy of the two products was 36% at 24 hours and 27% at 48 hours.
261 The conclusion drawn by Ms Lucas was that, after 24 hours, the Rexona product provided “significantly better” clinical wetness control compared to the Nivea product (relative efficacy was 36% SWR) and, after 48 hours, the Rexona product provided “significantly better” clinical wetness control compared to the Nivea product (relative efficacy was 27% SWR).
262 The expression “significantly better” in that context referred to statistical significance.
Beiersdorf’s arguments concerning test #2
263 Dr Schmidt-Rose criticised two aspects of the “design” of Unilever’s thermal test studies. He claimed that the methodology applied in the tests departed in some ways from the FDA Guidelines. It is unnecessary to determine the merits of those criticisms. Even if there was some merit in them, Beiersdorf failed to demonstrate that the deficiencies identified had, or were likely to have had, any, or any material, effect on the results of the tests.
264 Beiersdorf’s main argument concerning Unilever’s reliance on the results of test #2, and Unilever’s reliance on its head-to-head test results generally, concerned the fact that the head-to-head test results did not include any baseline measurement. The results, expressed in terms of SWR, provided a comparison between the two products based on the average amount of sweat excreted during the test. There was, however, no measurement of the overall sweat reduction, in either weight or percentage terms, for either product in comparison to a baseline point of the average amount of sweat excreted by the test subjects untreated by any antiperspirant under the same “hot room” conditions. In Dr Schmidt-Rose’s opinion, the baseline point has a significant impact on the interpretation of the figures for the average amount of sweat excreted.
265 Dr Schmidt-Rose illustrated that point by analysing the results of test #2 by reference to two assumed baseline measurements. The first assumed measurement was that the test subjects, untreated by any antiperspirant, excreted an average of 400mg of sweat during exposure to the same hot room conditions. The second assumed measurement was that the test subjects, untreated by any antiperspirant, excreted an average of 600mg of sweat during exposure to the same hot room conditions. Dr Schmidt-Rose noted that, in his experience, both those measurements would be a “realistic” amount of sweat excreted under the relevant conditions.
266 On the first assumption, the results of test #2 would be that the Rexona product would have caused an overall sweat reduction of 65.8% at 24 hours and the Nivea product would have caused an overall sweat reduction of 48.4% at 24 hours: a difference of 17.4%. That compares with a SWR of 36%. At 48 hours, the Rexona product would have caused an overall sweat reduction of 77.2% and the Nivea product would have caused an overall sweat reduction of 65.6%: a difference of 11.6%, as compared to a SWR of 27%. The difference between the products was, in both scenarios, significantly less than the difference suggested by the SWR.
267 Unilever did not dispute these calculations by Dr Schmidt-Rose. It did, however, dispute that 400mg and 600mg would be realistic amounts of sweat excreted under hot room conditions. It pointed, in that regard, to Dr Weddell’s evidence that he considered that the use of 300mg as a standard baseline was “not unreasonable”. It does not necessarily follow, however, that 400mg or 600mg were not reasonable baselines as Dr Schmidt-Rose contended.
268 Unilever also submitted that Dr Schmidt-Rose’s analysis demonstrated, in any event, that “the difference between [the Rexona product] and [the Nivea product] is not ‘similar’”. The precise basis of that assertion was somewhat unclear. It would appear to have been premised on the proposition that a difference in overall sweat reduction of 17.4% at 24 hours, and 11.6% at 48 hours, would be considered as significant based on what was said in the FDA Monograph. The suggestion appeared to be that the FDA Monograph stated that a product that caused an absolute sweat reduction of 20% in 50% of the target population was permitted to be called an antiperspirant, and a product that caused an absolute sweat reduction of 30% in 50% of the target population was permitted to be called an “extra-effective” antiperspirant. It followed, according to Unilever, that the FDA considered that a difference of 10% in terms of absolute efficacy was significant.
269 It is, however, by no means clear that it is open to construe what is said in the FDA Monograph as an indication of what is or is not “similar”. The fact that, for essentially regulatory reasons, the FDA determined that a product which was able to achieve 30% sweat reduction could be called “extra-effective”, whereas one which only achieved 20% reduction was not, does not mean that the FDA had determined that a difference of 10% or more was significant.
270 Unilever also mounted an argument which involved using the absolute efficacy of the Nivea product established by another test (test #6) and calculating the absolute efficacy of the Rexona product using the SWR (relative efficacy) result in test #2. The absolute efficacy of the Nivea product established by test #6 was 32% and the absolute efficacy of the Rexona product calculated in this way was said to be 57%. Those results showed, so Unilever argued, that the products were not so highly efficacious as to render the head-to-head result of 36% SWR incapable of demonstrating that the products were not “similar”.
271 There are, however, significant problems with that argument. It is by no means clear that the results from an absolute test involving different subjects under potentially different conditions can properly be used to calculate the absolute efficacy of the products based on the comparative efficacy results produced by a different head-to-head test. None of the experts provided any real support for that sort of analysis. Indeed, the experts all agreed that comparing the results of different absolute tests was problematic because of potential variances between the conditions of the different tests. Those variances would include, for example, different protocols, different subjects and different climatic conditions. That would also tend to suggest that potential variances between the conditions of an absolute test and a different head-to-head test would mean that using the results of the absolute test to determine the absolute efficacy of the product tested in the head-to-head test would be equally, if not more, problematic.
272 Ultimately, it must be accepted that that, while the results of head-to-head tests are capable of proving that one product is more efficacious, in terms of sweat reduction, than another product, there are some difficulties involved in determining the extent or significance of the differences from head-to-head tests alone in circumstances where the tests do not include a baseline measurement of absolute efficacy. While the percentage difference based on average weight of the sweat excreted during the head-to-head test may suggest a difference, sometimes a relatively large percentage difference, between the efficacies of the respective products, the significance of that difference is difficult to determine without knowing the absolute efficacies of the products in question.
273 The particular difficulties that this issue poses in determining whether the relevant Nivea Stress Protect Clinical Strength products were “similar” to the Rexona and Dove Clinical Strength products are discussed later.
Test #3 – Head-to-head stress test between Rexona Clinical Protection and Nivea Stress Protect Clinical Strength
274 Test #3 was a head-to-head study to test the relative efficacy of Rexona for Women Clinical Protection Shower Clean and Nivea Stress Protect Clinical Strength. The study involved a cohort of 31 subjects who, after a “washout” period, underwent a 10-minute “emotional stress sitting” after the product application. The weight of a pad placed under the armpits of the subjects was taken before and after the sitting to determine the amount of sweat excreted. The test was conducted by an independent testing company, Intertek Clinical Research Services, in the United Kingdom in July 2015.
275 The key results of the study, in simple terms, were:
The mean increase in the pad weight after the sitting was 0.050 grams for the Nivea product and 0.026 grams for the Rexona product.
The difference between the results, excluding outliers, was 0.017 grams
276 The conclusion expressed in the test report was that there was “a statistically significant difference in the amount of perspiration collected (pre-test to post-test) between [the Rexona and Nivea] products” and that “[s]ignificantly less perspiration was collected from the axilla treated with Rexona for Women ‘Shower Clean’ … than the axilla treated with Nivea Clinical ‘Stress Protect’ … when data were analysed”. The mean SWR was recorded as 50%.
Beiersdorf’s arguments in relation to test #3
277 Beiersdorf contended that the stress test methodology employed by Intertek was flawed. In its submission, the flaws were such that the results of test #3 should be given little weight.
278 Beiersdorf’s main criticism of the test was that it was not possible to determine whether the 10-minute emotional stress sweat sitting in fact induced sufficient stress to produce reliable results. That is because, unlike the Trier Social Stress Test (TSST), which was a commonly accepted and rigorous test for inducing psychobiological stress responses in a laboratory setting, the Intertek test did not include any physiological measurement of stress or biomarkers to test whether sufficient stress was induced in the subjects.
279 Dr Schmidt-Rose’s evidence was:
TSST is a psycho-social test where a test subject is asked to give an impromptu-speech in an imagined job application scenario in front a [sic] committee. After that the test subject has to solve a mental arithmetic task during which he or she has to count backwards from 2023 in 17 steps as quickly and correctly as possible and in the case of miscalculation, he or she has to start all over again. The tests last for 15 minutes.
TSST was developed by a group of scientists led by Professor Dirk Hellhammer from the University of Trier … TSST is a widely accepted method of inducing stress in a laboratory environment. According to the Google Scholar search engine, since publication of the Kirschbaum Paper, it has been cited 2788 times by other articles …
Before and after the test, the individual stress levels of the test subject is determined by heart rate and saliva cortisol measurements. The test subject is also asked to assess their feelings of stress perception, anxiety, insecurity, perspiration and body malodour by way of responding to questionnaires shortly before, during and immediately after the test.
280 While Dr Weddell would not agree, in cross-examination, that the Intertek methodology was deficient, he conceded that he did not have enough information to determine whether the test was reliable or not.
281 The evidence of Mr Peter Allen, who was involved in the design and conduct of the test, was that, while there were no biomarkers or biological information to confirm that the subjects were in fact stressed at any time during the 10-minute period, his view was that the test results produced a sufficient difference in the amount of sweat as between the two products to indicate that enough stress and enough sweat was created to produce meaningful results. That view also appeared to have been informed by the use of the protocol in previous tests, though Mr Allen gave no detail whatsoever of those previous tests or the results of them.
282 The evidence of Dr Marti, who ultimately approved the design of the test, was similar to Mr Allen’s evidence. He agreed that, from the information in the test report, it was not possible to be confident that the sweating that was measured was as a result of emotional or stress sweat reaction. He claimed, however, that he had experience of the method which demonstrated that it prompted emotional sweating beyond ambient sweating. Like Mr Allen, however, he gave no detail about that past experience.
283 Beiersdorf also pointed to the fact that the amount of sweat produced during the 10-minute test (0.026g for the Rexona product and 0.050g for the Nivea product) was very small. Dr Marti agreed that he would be very surprised if 0.026g of sweat would be perceptible in a clinical setting. The difference between the two products, in terms of weight (0.017 once outliers were removed) was also extremely small. Dr Marti also agreed that, from the results of test #3 alone, it was not possible to determine whether, on the one hand, a lot of sweat would have been produced by the test, but the products were very efficacious, or on the other hand, that the test simply produced a very small amount of sweat. He agreed that the small difference between the two products could be explained on the basis that they were both highly efficacious.
284 There is merit in Beiersdorf’s criticisms of the methodology employed in test #3. The evidence of Dr Weddell, Mr Allen and Dr Marti concerning the test, including its departures from the TSST, was not persuasive.
285 Perhaps more significantly, the nature and results of the test suggest that considerable caution should be exercised in giving any real weight to the 50% SWR produced by the test. That is particularly the case given that it cannot be excluded that the very small amount of sweat produced by the test, and the small difference between the test results for the respective products in terms of weight (0.017g), could be explained either on the basis that both products were highly efficacious, or that the test did not produce much stress. If the former, while the 50% SWR might appear large, it might nonetheless be fairly insignificant given the high absolute efficacy of both products. If the latter, the result would most likely be unreliable because of deficiencies in the test protocol.
286 It should also be noted in this context that there is no baseline measurement of absolute sweat reduction involved in this test. The experts all effectively agreed that there were difficulties in taking baseline measurements in stress tests. In any event, in those circumstances, and in circumstances where it cannot be excluded that both products were highly efficacious in absolute terms, the 50% SWR may not in fact reflect any significant level of difference between the two products.
Test #4 – Head-to-head thermal test between Rexona stick and Nivea Stress Protect Clinical Strength
287 Test #4 was a three application, 24-hour and 48-hour hot room sitting study to test the relative sweat weight reduction performance of Rexona for Women Shower Fresh antiperspirant deodorant stick and Nivea Stress Protect Clinical Strength. It was conducted in a laboratory in the Philippines in January 2015.
288 The results of the test were:
At 24 hours, an average of 0.1570 grams of sweat was excreted from the underarms of those subjects to whom the Rexona product had been applied and 0.1713 grams of sweat was excreted from the underarms of those subjects to whom the Nivea product had been applied.
At 48 hours, an average of 0.1927 grams of sweat was excreted from the underarms of those subjects to whom the Rexona product had been applied and 0.2018 grams of sweat was excreted from the underarms of those subjects to whom the Nivea product had been applied.
The percentage SWR was 11% at 24 hours and 6% at 48 hours.
289 The conclusions recorded in the report were that, after 24 hours, the Rexona product provided “significantly better” clinical wetness control compared to the Nivea product (relative efficacy was 11% SWR) and, after 48 hours, the Rexona product provided “significantly better” clinical wetness control compared to the Nivea product (relative efficacy was 6% SWR). The expression “significantly better” in that context presumably again referred to statistical significance.
290 Unilever relied on this test in support of its case that the Superiority Representations were false.
291 Beiersdorf noted that this was the only head-to-head thermal test between a Nivea Stress Protect Clinical Strength product and a so-called “non-clinical” product. It emphasised, however, that the one product that Unilever chose to test head-to-head with the Nivea product was its antiperspirant stick which contained AZAG.
Test #5 – Head-to-head stress test between Rexona stick and Nivea Stress Protect Clinical Strength
292 Test #5 was a head-to-head stress test designed to determine the relative efficacy of Rexona for Women Shower Fresh antiperspirant stick and Nivea Stress Protect Clinical Strength. It was an Intertek test conducted at the same time, and pursuant to the same methodology and protocols, as test #3.
293 The key results of the study, in simple terms, were:
The mean increase in the pad weight after the sitting was 0.036 grams for the Nivea product and 0.034 grams for the Rexona product.
The difference between the results, excluding outliers, was 0.004 grams
294 The conclusion expressed in the test report was that there was “a statistically significant difference in the amount of perspiration collected (pre-test to post-test) between [the Rexona and Nivea] products” and that “[s]ignificantly less perspiration was collected from the axilla treated with Rexona for Women ‘Shower Fresh’ … than the axilla treated with Nivea Clinical ‘Stress Protect’ … when data were analysed”. The mean SWR was recorded as 22%.
295 While this test was not the subject of any specific detailed submissions, the criticisms levelled by Beiersdorf at the test #3 methodology and results apply equally to it. The findings made concerning the reliability and relevance of the results of test #3 also apply equally to test #5. Indeed, it may be noted that the amount of sweat generated by the test, and the difference, is considerably smaller than the amount of sweat and difference generated in the case of test #3. The observations made in relation to the test #3 results therefore apply with even more force to results of test #5.
296 Unilever relied on this test in support of its case that the Superiority Representations which involved efficacy in respect of stress sweat were false. Beiersdorf again pointed out that the one product that Unilever chose to test head-to-head with the Nivea Stress Product Clinical Strength product was its antiperspirant stick which contained AZAG.
297 Unilever relied on a number of absolute thermal sweat tests. The first test (test #6) was a test of the Nivea Stress Protect Clinical Strength product. The other tests (test #11 and test #12) concerned various formulation of soft-solid and stick antiperspirant deodorants.
Test #6 – Absolute thermal test of Nivea Stress Protect Clinical Strength versus Impulse body fragrance
298 Test #6 was a hot room study to evaluate the absolute efficacy of the Nivea Stress Protect Clinical Strength product at 24 hours and 48 hours. The Nivea product was tested against another product, Impulse Body Fragrance, which was said to be a “control”, presumably because it had no antiperspirant effect. The test was conducted by Ms Lucas in a laboratory in the Philippines in December 2015.
299 The relevant results of the test were as follows:
At 24 hours, an average of 0.2054 grams of sweat was extracted from the underarms of the subjects treated with the Nivea product and 0.3007 grams was extracted from the underarms of the subject treated with the control. The results at 48 hours were 0.2641 for the Nivea product and 0.3435 for the control.
The SWR was 32% at 24 hours and 24% at 48 hours.
300 Ms Lucas’ conclusion was that the Nivea product provided significant clinical wetness control compared to the “deodorant control” at both 24 hours (32%) and 48 hours (24%).
301 As will be seen, despite the fact that all the experts agreed that there were difficulties comparing absolute test results, Unilever’s case appeared to depend, at least in part, on a comparison of the results of test #6 with the results of another absolute test, test #11.3, which was said to be a test of another Unilever product with the same efficacy as Rexona Clinical Protection.
Test #11 – Four absolute thermal tests of various Unilever soft solid antiperspirant deodorants
302 Test #11 was in fact four separate absolute thermal tests that were performed in various countries in 1999, 2007, 2009, and 2011 in respect of four different Unilever-made soft-solid antiperspirant deodorants. There was no evidence concerning the formulation of the tested soft-solids and no evidence that they were within the Rexona or Dove Clinical Protection range that was sold in Australia. Dr Weddell’s evidence was that they might or might not have been equivalent to any particular variant of Rexona or Dove, that different variants have slightly different lists of ingredients, and that he was unable to say whether the products tested in 1999 and 2007 were still current formulations.
303 Unilever relied, however, on the fact that one of products, the one tested in 2011 (test #11.3), had the same percentage of the active ingredient, AZAG, as the Rexona and Dove Clinical Protection range. It contended on that basis that the product the subject of test #11.3 could be said to have the same efficacy as a Rexona Clinical Protection product.
304 Confidentiality orders were made in respect of the percentage of the active ingredient in the products and the SWR results of the tests. It suffices for present purposes to say that there was a significant difference between the tested soft-solid products and the control.
305 As noted earlier, Unilever sought to compare the results of test #6, the absolute test of the Nivea Stress Protect Clinical Strength product, with the results of test #11.3, and contended that the difference was such that the two products could not be said to be “similar”.
Beiersdorf’s arguments concerning test #11
306 Beiersdorf disputed Unilever’s contention that the product that was the subject of test #11.3 could be taken to have the same efficacy as Rexona Clinical Protection. It pointed out that there was no evidence that the product tested in test #11.3 was a Rexona Clinical Protection product, or had the same formulation as the Rexona Clinical Protection product. It submitted that there was evidence that different formulations can impact upon efficacy of the product, even when the products contained equivalent quantities of AZAG. It also pointed out, in that regard, that the results of the four tests showed that there was no linear relationship between the efficacy of a particular product and the percentage of AZAG in that product. It followed, according to Beiersdorf, that any comparison between the absolute test results of test #6 and test #11.3 was irrelevant and said nothing about the comparative efficacy of Nivea Stress Protect Clinical Strength and Rexona Clinical Protection.
307 Beiersdorf also contended that a direct comparison of absolute tests was, in any event, dangerous because of variances between the tests. Dr Weddell agreed, in the context of the test results of the four tests in test #11, that factors such as different people being involved in the tests, testing in different countries, testing in different seasons and testing in different climates can make direct comparison difficult.
Test #12 – Four absolute thermal tests of various stick antiperspirant deodorants
308 Test #12 was in fact four separate absolute thermal tests that were performed in in 2006, 2007, 2010 and 2012 in respect of four different stick antiperspirant deodorants. There was no evidence concerning the precise formulation of the tested sticks or that they were within the Rexona or Dove range of products that was sold in Australia. There was, however, evidence of the percentage of AZAG in the products. That evidence was the subject of confidentiality orders. Unilever also claimed that the SWR results of the tests were confidential.
309 Unilever sought to compare the results of test #6 with the results of test #12 in support of its case that the Superiority Representations were false.
310 Beiersdorf submitted, however, that such a comparison was irrelevant for essentially the same reasons as those that it relied on in support of the contention that comparing the results of test #6 with the results of test #11 was irrelevant. Beiersdorf pointed out that there was no evidence that the stick deodorants which were the subject of test #12 were the same or similar to the formulations of the Rexona stick products sold in Australia. It submitted that, even if the tested products had the same level of active ingredient, AZAG, as the Rexona sticks, it did not follow that they could be taken to have the same level of efficacy because different formulations can nonetheless affect efficacy. The same problems associated with the comparison of different absolute efficacy tests also applied.
Beiersdorf’s tests – Tests #7, #8, #9 and #10
311 Beiersdorf tendered an article co-authored by Dr Schmidt-Rose and published in the International Journal of Cosmetic Science: Thomas Schmidt-Rose et al., ‘Efficient sweat reduction of three different antiperspirant application forms during stress-induced sweating’ (2013) 35(6) International Journal of Cosmetic Science 1. The synopsis of that article was as follows:
OBJECTIVES: Stress sweating can occur in everyday situations independently of thermally-induced perspiration. It is triggered by emotionally challenging situations and leads to underarm wetness and a characteristic unpleasant malodor. In this study, we aimed to determine the long-term efficacy of three unperfumed antiperspirant (AP) formulas for different application forms (roll-on, stick, aerosol) against stress-induced sweating and malodor formation.
METHODS: We utilized the widely accepted Trier Social Stress Test (TSST) to induce psychosocial stress in female and male volunteers (18 – 40 years) and determined physiological stress parameters. To additionally assess the efficacy of the test AP roll-on against thermally-induced sweating, a hot room study was performed.
RESULTS: Increasing heart rates and an augmentation of saliva cortisol levels during the TSST indicated a substantial stress reaction which was paralleled by a pronounced sweat production in the untreated axillae of both males and females. Forty-eight hours after application, all three test APs significantly decreased the amount of sweat in the treated axillae independent of gender. With respect to AP effects on malodor production, trained sniffers assessed sweat samples collected during the TSST from the untreated axillae as significantly more malodorous than comparable samples from the AP-treated axillae. Also, independent of gender the test AP roll-on significantly decreased the thermally-induced sweat in the AP-treated axilla.
CONCLUSION: We show for the first time a highly effective reduction of emotionally-induced axillary sweating and malodor production for three different application forms 48 h after the last product use. The specially developed roll-on, stick, and aerosol AP provide long-term protection against stress-induced sweat which is of high relevance in everyday life.
312 It was common ground that the three products that were subject to the stress test (roll-on, stick and aerosol) were effectively the same as the products that were ultimately launched as the Nivea Stress Protect range. The stick that was tested, however, was not exactly the same as the Nivea Stress Protect Clinical Strength stick that was launched in Australia. As was noted earlier, there was evidence that the Nivea stick that was launched in Australia had additional fragrance added to it following the first blind home user tests.
313 While the sweat test results were the main focus of the article, a second study involved an absolute thermal test of the roll-on only.
314 The results of the tests (referred to in Unilever’s “tests bundle” material as tests #7, #8, #9 and #10) were as follows:
The stress test of the un-fragranced formulation of the Nivea Stress Protect Clinical Strength stick recorded (as at 48 hours after application of the product) a median sweat reduction (compared to the untreated axilla) of 52.7% for the female test subjects and 67.3% for the male subjects; and a mean percentage sweat reduction of 58%. Dr Schmidt-Rose’s evidence was that the results proved that at least 50% of the subjects obtained a sweat reduction of at least 30%.
The stress test results for the aerosol recorded a mean sweat reduction of 33% for the male subjects and 50% for the female subjects.
The stress test results for the roll-on showed a mean sweat reduction of 51% for the male subjects and 55% for the female subjects.
The absolute thermal test results for the roll-on mean sweat reduction of 26% for the male subjects and 29% for the female subjects.
315 Unilever contended that the test results showed that the Nivea Stress Protect Clinical Strength stick was less efficacious than the Nivea Stress Protect roll-on, and the Nivea Stress Protect aerosol was equally efficacious as the Nivea Stress Protect Clinical Strength stick, based on a comparison of the mean results relating to the female subjects and the female variants of the products.
316 Beiersdorf submitted that Unilever’s reliance on only the female test results indicated that it was simply “cherry-picking” the results. It also relied on the evidence of Dr Schmidt-Rose which, in very general terms, was that, if consideration is given to the data distribution, the median result for the stick was not below that of the roll-on. Dr Schmidt-Rose also referred to a recent statistical examination of the data that had been performed by a statistician in Germany. That statistical analysis was not included in his affidavit and the raw data was not available for examination. Dr Schmidt-Rose himself was not a statistician. It would, perhaps, be fair and not uncharitable to say that Dr Schmidt-Rose’s evidence concerning the statistical analysis was not particularly persuasive.
Conclusions that may be drawn from the laboratory tests and test results
317 Unilever’s case that the Similarity and Superiority Representations were false relied heavily, if not almost exclusively, on the various head-to-head and absolute tests. It submitted that the falsity of the representations was established by its head-to-head testing alone, its absolute testing alone, and its head-to-head testing together with its absolute testing.
318 There are, however, difficulties with Unilever’s reliance on the testing and test results.
319 First, it may be accepted that the tests and test results are capable of establishing that the efficacy of the Rexona Clinical Protection product was different to the efficacy of the Nivea Stress Protect Clinical Strength product, at least in terms of sweat reduction measured by laboratory tests. Indeed, the laboratory results tend to show that the Rexona product was more efficacious, in terms of reducing sweat, than the Nivea product. Unilever’s case, however, was not that Beiersdorf represented to the ordinary reasonable Australian consumer of antiperspirant deodorants that the Nivea product was the same or better than the Rexona product. If it had, subject to some of the following points, the test results may have been capable of proving the falsity of those representations.
320 Second, Unilever’s case in respect of the Similarity Representations appeared to proceed on the premise that the relevant products are dissimilar (or have been proved to be not similar) if the test results show that there is a statistically significant difference between the efficacy of the products in terms of the weight of the sweat reduced by them. That is not, however, the way that Unilever pleaded or particularised its case. In the further particulars of its claim, Unilever stated that the words in expressions such as “similar antiperspirant efficacy” and “similar antiperspirant protection” bore their ordinary English meaning, and that the criterion for efficacy and protection was “perspiration reduction”. Nowhere in its pleading or particulars does Unilever claim that similarity, or dissimilarity, is to be judged solely in terms of statistically significant differences revealed by laboratory test results.
321 More importantly, it is difficult to imagine that the ordinary reasonable consumer of antiperspirant deodorants would necessarily understand or perceive that representations concerning the “similar antiperspirant efficacy” and “similar antiperspirant protection” of different brands of antiperspirant deodorants hinged on whether there were statistically significant differences in laboratory tests concerning the reduction of perspiration. If, contrary to the conclusion reached earlier, the Similarity Representations were conveyed, consumers were unlikely to have viewed “similarity” in such narrow terms. Rather, they would have seen similarity in terms of how the products worked for them. They would be unlikely to consider that two products were dissimilar, in terms of their antiperspirant efficacy, simply on the basis of statistically significant differences between the amounts of sweat reduced in laboratory tests. In that context, consumer perceptions may be as important as, if not more important than, laboratory tests. If consumers were unable to perceive any difference between the products, in terms of their antiperspirant efficacy, they would be likely to consider them to be similar, or at least not dissimilar.
322 Third, and related to the second point, a statistically significant difference between the respective weights of the sweat reduced by the relevant products in laboratory tests would not necessarily be a difference able to be perceived by a consumer in a real world setting. Much would depend on the size of the difference and the overall or absolute amount of sweat that the products reduced. If the difference in the efficacy of the products was not one which would be able or likely to be perceived by a consumer, it is difficult to see how the products could confidently be found to be dissimilar. Moreover, even if the difference was, or was likely to be, perceptible to a consumer in a real world setting, it still does not follow that the products would necessarily be found to be dissimilar. Much would depend on the degree or extent of the perceptible difference. The Similarity Representations do not convey that the respective products were identical. In the context in which the Similarity Representations were said to be conveyed, some minor degree of perceptible difference would have to be able to be tolerated before the products could be said to be dissimilar.
323 Fourth, the tests and test results relied on by Unilever were by no means extensive or complete having regard to the terms of the Similarity and Superiority Representations. Unilever did not adduce evidence of any absolute thermal test results of the Rexona and Dove Clinical Protection products sold in the Australian market. Rather, it only adduced evidence of absolute thermal testing of Unilever soft-solid products which were not established to be formulated in exactly the same way as the Rexona and Dove products sold in Australia. While one of the products tested had the same percentage of the active ingredient, AZAG, as the Rexona Clinical Protection product, it does not necessarily follow that it had the same efficacy. As noted earlier, it was generally accepted by the expert witnesses that different product formulations may have an impact on efficacy, even if the same quantity of AZAG is used, and that there is no linear relationship between the quantity of AZAG and antiperspirant efficacy.
324 Unilever also did not adduce evidence of any absolute stress test results for any of its soft-solid products, or Mitchum Clinical.
325 In relation to the Superiority Representations, the only absolute test results of products other than the Nivea Stress Protect Clinical Strength product were the results of absolute tests conducted on its own antiperspirant stick products which contained relatively high levels of the active ingredient, AZAG. The formulations of those stick products were also not shown to be the same as the formulations of the Rexona or Dove Clinical Protection sticks sold in Australia.
326 Fifth, it was generally accepted by all the relevant experts that there are difficulties involved in comparing absolute test results of competing products, particularly where the tests may have been conducted using different protocols, or in different countries, or in different seasons, or involving different subjects, or at different times. Yet Unilever’s analysis of the test results and what could be concluded from them relied, at times to a considerable extent, on comparing or using the results of different absolute tests.
327 Sixth, as has already been noted, Beiersdorf’s submissions concerning the limited utility of Unilever’s head-to-head tests in determining the significance of the differences between the antiperspirant efficacy of the products have merit and should be accepted. While it may be accepted that head-to-head tests are the most reliable way of determining whether one product is more efficacious than another, there are also demonstrable difficulties involved in reaching firm conclusions about the relative significance of any difference if the demonstrated difference in efficacy cannot be placed in the context of any measurement of the baseline or absolute sweat reduction efficacy of the products in question.
328 While Unilever disputed that proposition, it also sought to account for or remedy the asserted difficulties by selectively employing the results of some of its absolute tests, and some of what was said in the FDA Monograph, in complex calculations designed to establish baseline or absolute efficacy figures to put the head-to-head results in context. There are, however, inherent difficulties involved in selectively using other absolute test results in the way Unilever sought to use them, particularly having regard to variances likely to exist between the different tests. Unilever’s use of parts of the FDA Monograph was also problematic. On the whole, Unilever’s attempt to overcome the deficiencies in its head-to-head testing arising from the absence of any baseline measurements was unpersuasive. Ultimately, the absence of any baseline measurements makes it difficult to reach firm conclusions concerning the relative significance of the differences in sweat reduction as between the respective products revealed by the head-to-head tests.
329 Seventh, for the reasons already given, Beiersdorf’s submissions concerning the methodological flaws in Unilever’s head-to-head stress tests between the Rexona Clinical Protection product and the Nivea Stress Protect Clinical Strength product (test #3), and between the Rexona stick and the Nivea Stress Protect Clinical Strength product (test #5) should also be accepted. Because the test protocol did not involve any physiological measurement of stress or biomarkers, it was not possible to determine whether the 10-minute emotional stress sweat sitting in fact induced sufficient stress to produce reliable results.
330 The amount of sweat produced during the 10-minute test was very small, as was the difference between the amount of sweat reduced by the products in real terms. That indicated either that the emotional stimulus did not produce much stress sweat, or that both products were highly efficacious in reducing stress sweat. In the absence of biomarkers recording the amount of stress generated, it was not possible to determine which of those possibilities was more likely. If the latter was the case, the difference indicated by the 50% SWR result in test #3 may nonetheless have been relatively insignificant.
331 The results of those head-to-head tests also perhaps exemplify the difficulties involved in determining the significance of the difference between the products without a baseline measurement. What may at first blush appear as a large difference, in terms of the SWR, may in fact be a very small difference in real or comparative terms when properly situated in the context of the absolute sweat reduction efficacy of the respective products. The same difficulties would appear to apply to the head-to-head stress test between the Rexona stick and the Nivea Stress Protect Clinical Strength product (test #5).
332 Eighth, in relation to the Superiority Representations, Unilever’s case to a large extent ultimately hinged on the proposition that the test results showed that the Nivea Stress Protect Clinical Strength product did not have greater antiperspirant efficacy than some of its own antiperspirant sticks, being those that included relatively large percentages of the active ingredient, AZAG. To the extent that Unilever’s case relied on test #5, the difficulties with that test have already been referred to. To the extent that it relied on a comparison of test #6 with test #12, that analysis involves the inherent difficulties of comparing different absolute tests, together with the added difficulty that Unilever did not prove that any of the products tested in test #12 had the same formulation as products sold in Australia at the relevant time.
333 That leaves the results of test #4. That test is at least capable of establishing that the Nivea Stress Protect Clinical Strength product did not have greater antiperspirant efficacy than one so called “non-clinical” product that may have been available in the Australian market. To that extent, it is capable of proving the falsity of the Superiority Representations, or at least representation 3, which is the Superiority Representation that does not relate specifically to stress sweat. The Superiority Representations that involve representations as to future matters are addressed separately.
334 The fact that the Superiority Representations, or at least some of them, could be proved to be false by proving that the Nivea product was not superior to one apparently highly efficacious Unilever product (with a high level of AZAG) selected from among the many hundreds of other antiperspirant deodorants on the Australian market rather demonstrates how unrealistic and contrived the Superiority Representations are. In some respects it tends to support the finding that the Superiority Representations were not likely to have been conveyed by Beiersdorf’s conduct.
335 Finally, in relation to the Superiority Representations, Unilever appeared to rely on a highly selective and narrow reading of the paper co-authored by Dr Schmidt-Rose: a comparison of the median sweat reduction result for female subjects who used the un-fragranced Nivea Stress Protect Clinical Strength stick (52.7%) in the stress test compared with the mean sweat reduction result for female subjects who used the roll-on. Such a selective and narrow reading of the paper is unwarranted. Ultimately, Dr Schmidt-Rose did not accept that the median figure for females who used the stick was below that of the roll-on. While his evidence concerning the need for a more detailed statistical comparison involving the data distribution was not very persuasive, it should nonetheless not be rejected out of hand, particularly given the purpose for which the paper was prepared. It was not prepared for the purposes of the detailed comparative exercise required to meet Unilever’s case.
336 Having regard to all of the deficiencies and difficulties with the testing, on balance it cannot be accepted that the test results alone are capable of proving the falsity of the Similarity Representations. While it may be accepted that the evidence is capable of establishing that there are differences between the Nivea Stress Protect Clinical Strength product and the Rexona Clinical Protection product, and that the Rexona product was generally more efficacious in terms of reducing sweat than the Nivea product, the precise scope, significance and perceptibility of the differences are not able to be determined with any degree of certainty or confidence. In those circumstances, it cannot be concluded that the test results prove that the antiperspirant efficacy of Nivea Stress Protect Clinical Strength was not “similar” to the antiperspirant efficacy of Rexona and Dove Clinical Protection and Mitchum Clinical.
337 It should also be reiterated in this context that Unilever’s difficulties in proving the falsity of the Similarity Representations on the basis of the laboratory tests can, at least to a certain extent, be traced back to its forensic decision to couch the representations in terms which used the word “similar” as the relevant comparator. As was noted previously, the word “similar” is an indeterminate comparator, particularly in the context of laboratory or scientific testing of a product like an antiperspirant deodorant. Unilever contended that the laboratory results were so clear that the conclusion that the products were not similar was obvious. It called in aid the observations of Lindgren J in Universal Music Australia Pty Ltd v Sharman Networks Ltd (2006) 150 FCR 110 at [55], where his Honour said, in the context of an argument that the orders which were said to found a contempt charge were uncertain:
If an order restrains a person from doing something “in daylight” and the person does the thing at midday in broad daylight, it is no answer to a charge of contempt that the order might have had an uncertain application requiring a dismissal of the charge if the evidence had shown that the person did the thing at twilight. The facts hypothesised would have suggested that the potential uncertainty of operation could have been avoided if the order had been expressed in terms of hours of the day, rather than in terms of “in daylight”. This does not signify, however, that “the nature and terms” of the order were such that a charge of contempt was always destined to fail.
338 The problem for Unilever, however, is that, to continue with Lindgren J’s analogy or metaphor, its test results were far closer to twilight than midday. The extent, significance and perceptibility of the statistical differences were far from obvious.
339 As for the Superiority Representations, the results of test #4 are at least capable of proving that the Nivea Stress Protect Clinical Strength product does not have a greater antiperspirant efficacy than a particular Rexona antiperspirant stick and, to that extent at least, are capable of proving the falsity of one of the Superiority Representations (representation 3). In a sense, however, that simply serves to demonstrate how unrealistic and contrived the Superiority Representations are.
340 Both Unilever and Beiersdorf pointed to a number of other considerations that were said to be relevant to determining whether or not Unilever had made out its case that the Similarity and Superiority Representations were false. The principal additional consideration was Beiersdorf’s blind home user test results. Other considerations included competing submissions relating to what was said in the FDA Monograph and Guidelines, evidence of the complaints concerning the Nivea product, market performance and the significance of evidence concerning the marketing and distribution of the Nivea Stress Protect stick in the United Kingdom.
Beiersdorf’s blind home user tests
341 It should perhaps first be noted that Unilever objected to Beiersdorf’s tender of the evidence relating to the blind home user tests. The objection was based broadly on the proposition that survey evidence is prima facie inadmissible. Unilever also pointed to what it contended were fundamental flaws in the design and implementation of the blind home user tests. It submitted that the probative value of the evidence was low and outweighed by the prejudicial effect flowing from the fact that no witness from Lonergan Research, the company who conducted the tests, was being called. Therefore, no witness could be cross-examined about the alleged flaws and deficiencies in the design and implementation of the tests. Unilever contended that, in those circumstances, the evidence should be excluded in exercise of the discretion under s 135 of the Evidence Act 1995 (Cth).
342 The evidence was admitted over Unilever’s objection. It is, in all the circumstances, unnecessary to give detailed reasons for the admission of the evidence. Suffice it to say that the blind home user tests were not commissioned for the purposes of this proceeding, or indeed any prospective litigation. Rather, they were commissioned by Beiersdorf to assist it in making commercial decisions in relation to the Australian launch of the Nivea Stress Protect range and the proposed Nivea Stress Protect Clinical Strength stick in particular. In those circumstances, the records relating to the testing were made or maintained for the purposes of Beiersdorf’s business. It follows that the statements in the various documents recording the tests were admissible as business records pursuant to s 69 of the Evidence Act.
343 Unilever ultimately did not dispute that the documents were admissible as business records. It submissions focussed on the alleged flaws in the testing and the proposition that the documents should be excluded pursuant to s 135 of the Evidence Act.
344 While there may have been some issues in relation to the methodology of the tests, those issues went to the weight to be given to the evidence, not its admissibility. The problem for Unilever was that, even if it could be said that the probative value of the evidence was very low having regard to those issues, which was, at best, doubtful, Unilever could nonetheless not point to any unfair prejudice arising from the admission of the evidence. Indeed, the fact that Unilever was able to make extensive submissions concerning the alleged flaws in the methodology of the tests without cross-examining anyone from the company which conducted the tests rather demonstrated that there was no unfair prejudice. There was accordingly no basis upon which to exclude the documents pursuant to s 135 of the Evidence Act. The probative value of the evidence was not outweighed by the danger that the evidence might be unfairly prejudicial to Unilever.
345 Beiersdorf ultimately relied on the evidence relating to the blind home user tests in relation to some fairly narrow issues. It is accordingly unnecessary to consider the evidence in great detail. Following is a brief summary.
346 In about October 2012, Beiersdorf commissioned Lonergan Research to carry out consumer testing to “determine whether our Stress Protect stick does perform as well as (or better than) our key competitors – because if it doesn’t, we won’t launch it”. The testing that Lonergan Research conducted involved the test participants completing and returning a 7-day diary and “post-usage questionnaire” in respect of their experience with the products which they used during the testing. The products used by the participants were the female variants of Rexona and Dove Clinical Protection, Lady Speed Stick and the female variant of Nivea Stress Protect Clinical Strength.
347 Mr Croci’s evidence concerning the results of the 2012 testing included that the Nivea product was performing “similarly, but not better than the deodorants we were compared against” and that a majority of consumers gave “‘top two box’ ratings” to each of the tested products in respect of the following measures: overall antiperspirant efficacy; overall deodorant efficacy; antiperspirant efficacy against stress sweat; deodorant efficacy against stress sweat; and overall performance against stress sweat. “Top two box” rating meant the highest or second highest rating on the survey form. The measure where the proportion of the top two ratings was furthest below the nearest competitor product was the level of satisfaction in terms of “long lasting protection against odour”. That result led Beiersdorf to request Beiersdorf AG to increase the amount of fragrance in the Nivea Stress Protect stick which was to be sold in Australia. Beiersdorf AG did not, however, make any changes to increase the antiperspirant efficacy of the product.
348 Beiersdorf commissioned Lonergan Research to conduct further consumer testing in 2013, after Beiersdorf AG had increased the level of fragrance in the Nivea Stress Protect product. That testing again involved participants using the relevant products as directed and then completing a questionnaire which was in essentially the same terms as the 2012 testing. The tested products included the female and male variants of Rexona Clinical Protection and the female and male variants of Nivea Stress Protect Clinical Strength.
349 Lonergan Research reported to Beiersdorf in respect of the 2013 testing that both the female and male variants of Nivea Stress Protect Clinical Strength performed as well in the questionnaire results as the female and male variants of Rexona Clinical Protection. A majority of consumers again gave top two box ratings to the Nivea product in respect of a number of measures comparing the product to their current antiperspirant deodorant. Lonergan Research recommended that Beiersdorf go ahead and launch the product, which it did in November 2013.
350 Lonergan Research was also commissioned to do some further testing in 2015, mainly because Nivea Stress Protect Clinical Strength was selling below Beiersdorf’s expectations. The 2015 testing included online surveys. The results of that survey were broadly consistent with the earlier test results.
351 As has already been noted, Beiersdorf did not suggest that it could rely on the results of the blind home user tests as clinical or scientific evidence concerning the efficacy of its products in terms of sweat reduction. Nor could it. Rather, Beiersdorf contended that the results of the blind home user tests were capable of demonstrating that, to the extent that Unilever’s laboratory tests established that there were differences between the relevant products in terms of sweat reduction efficacy, those differences were unlikely to have been able to be perceived by consumers. In Beiersdorf’s submission, had the test participants perceived material differences in the antiperspirant efficacy of the Nivea Stress Protect Clinical Strength products as compared to the Rexona and Dove Clinical Protection products, the results of the blind home user tests would have been different. The participants would not have placed the Nivea product in the same top two box as the Rexona and Dove products.
352 Beiersdorf submitted, in that context, that if consumers were not able to perceive the difference between the two products, that would be a good reason for finding that the products were similar, or at least not dissimilar, particularly in the context where the Similarity Representations were essentially said to have misled, or been capable of misleading, consumers.
353 Unilever, however, contended that there were numerous flaws and deficiencies in the design and execution of the blind home user test questionnaires and that, accordingly, the results should be given no weight. It submitted that the flaws were such that the results were meaningless and unreliable. It contended that the situation was made worse by the fact that it was unable to cross-examine anyone from Lonergan Research in relation to the deficiencies. The alleged flaws in the design and execution of the tests included, in summary: the fact that the screening questionnaire which was completed online was no longer available and it was therefore not possible to know what the participants saw or how they navigated through the questionnaire; the questions in the questionnaire which asked the participant to compare the test products with the participant’s current deodorant were flawed; the instructions that were given to participants in relation to their daily routine did not make sense; the questions that the participants were asked to answer about rating the “wetness” and “smell” experienced by them were defective; some of the questions about the participant’s “stress-related ‘sweat situation’” were unrealistic; there were issues about whether the test was truly “blind”; a longer “wash-out” period should have been allowed for; and the number of participants in the tests was too low.
354 It is unnecessary to give detailed attention to all of the alleged flaws in the design of the blind home user tests. It suffices to give a few examples, being the examples highlighted in both Unilever’s and Beiersdorf’s final submissions, to illustrate the general nature of the alleged flaws.
355 Prospective participants were asked to complete a screening questionnaire. Question 7 of the questionnaire asked the prospective participant: “I would describe my perspiration without the use of an anti-perspirant deodorant as …?” The prospective participant could choose one of four answers: a very big problem; a fairly big problem; a very small problem; or not a problem at all. Unilever criticised this question on the basis that some consumers had indicated that they applied an antiperspirant up to five times a day, and the average application rate was 1.6 times per day. Its argument was that such a consumer would not readily be able to answer a question which asked them to describe their perspiration without a deodorant. They were never in that position.
356 When asked in cross-examination about this question, however, Mr Croci said that the prospective participant would “surmise how … much of a problem it actually would be” and would be “fine answering question 7 because they would know whether they’ve got a big problem with perspiring or not”. Mr Croci further explained that “[a]t some point … they must have not used a deodorant, realised they were sweating and chosen to use one. So they can imagine what they would like if they didn’t use a deodorant”.
357 Beiersdorf submitted that question 7 in the screening questionnaire was a common sense question which asked a consumer to describe whether or not they considered themselves to be a heavy sweater. Mr Croci’s responses in cross-examination demonstrated that to be the case.
358 There is perhaps some merit in Unilever’s submissions in relation to question 7. If the intention was to ascertain whether or not the participant considered themselves to be a heavy sweater, there are no doubt better ways that the question could have been framed. Nevertheless, it is doubtful that it could be described as a significant or material flaw in the test design or methodology. It is also difficult to see how any deficiency in this question would necessarily undermine the reliability of the test results generally.
359 Another criticism advanced by Unilever concerned the diary that participants were required to complete each day. The diary included a number of questions. The instructions in relation to the completion of the diary, in respect of day 1, were as follows:
Perform your everyday routine as usual. At night before you apply the anti-perspirant deodorant and go to bed. Please complete Day 1 column on the diary at this time.
360 The instructions in relation to the following days were:
Continue the product trial, applying the anti-perspirant deodorant and completing the diary every evening.
361 Unilever contended that the instructions did not make any sense. Mr Croci’s evidence, however, was that it made sense to him. It simply meant that the participant was to go about his or her everyday routine, apply the antiperspirant, go to bed and complete the diary.
362 Questions 5 and 6 of the diary were: how would you rate the overall wetness in your underarm area; and how would you rate the overall level of smell in your underarm area? Unilever criticised those questions, in light of the general instructions in relation to the completion of the diary, on the basis that the participant’s attention was not directed to any particular part of the day. That perhaps may be accepted. Mr Croci’s evidence, however, was that the question was “designed to try to get a consistent measure across all respondents at roughly the same time every day”, though he did agree that “one doesn’t really know when it’s asking about”. He also appeared to agree, when cross-examined about the questions, that they were about wetness and the level of smell “at the time of completing the diary”, which conceivably meant “when they have a shower and have dried themselves, applied the deodorant and gone to bed”. That, however, would appear to be a rather perverse way of reading or interpreting the questions.
363 It may perhaps again be accepted that the instruction for the completion of the diary could have been expressed more clearly. Equally, diary questions 5 and 6 could perhaps be said to have lacked clarity in relation to the time or times of the day to which the questions were directed. Common sense would, however, tend to suggest that the participants were being asked about the level of wetness and smell at the time they completed the diary, which was in the evening before, rather than after, the participant showered and re-applied the antiperspirant deodorant.
364 It is unnecessary to refer to the balance of Unilever’s criticisms of the blind home user test instructions and questions. Most of them were similar to the criticisms that have just been addressed. It may be accepted that at least some of Unilever’s criticisms were valid criticisms. There were undoubtedly some issues or problems with the some of the instructions and questions contained in the survey diary and questionnaires. Beiersdorf effectively accepted as much, though it submitted that the issues or problems could not be characterised as fundamental flaws, as Unilever sought to characterise them. More significantly, the flaws were not such as to significantly undermine the general reliability of the test results, particularly having regard to the purpose for which they were intended to be utilised by Beiersdorf. That submission should be accepted.
365 As Beiersdorf correctly pointed out, Lonergan Research, an experienced and respectable market research firm, was engaged to conduct the testing for Beiersdorf’s business purposes prior to the potential launch of the relevant Nivea product, not for any actual or expected litigation. In those circumstances, Beiersdorf submitted that Unilever’s minute “nit-picking” and parsing of the test questionnaire and other aspects of the test methodology was unwarranted and unrealistic. The issues and problems were not significant or material when the tests and the test results were considered in the appropriate context; they were not, and were not intended to be, a scientifically rigorous quantitative analysis of the antiperspirant efficacy of the tested products.
366 Unilever went so far as to submit that the test instructions and questionnaire were “slanted in favour of” the Nivea product. There was, however, no proper basis for that submission. As has already been noted, the tests were commissioned for business purposes. According to Ms Braun, the ultimate purpose of the tests was to assist Beiersdorf in deciding whether to introduce the Stress Protect stick into Australia as a high-efficacy product against stress sweat. The tests were not designed to assist Beiersdorf in this or any other litigation. In those circumstances, there would have been no reason or rationale for “slanting” the results of the tests in favour of the Nivea product. Indeed, that would have been counterproductive. It may well have led Beiersdorf to make the wrong business decision.
367 It may be accepted that the issues and problems with some aspects of the methodology of the blind home user tests were such that the results of those tests must be viewed with some degree of caution. Nevertheless, the results of the 2012 and 2013 blind home user tests remain relevant, and should be given some weight, albeit for the relatively limited purpose for which Beiersdorf sought to use them: not as testing which was on par with scientific or laboratory testing, but as some evidence of consumer perceptions about the rival Unilever and Beiersdorf products.
368 The blind home user test results were plainly not capable of establishing the comparative sweat reduction efficacy of the rival products in quantitative terms. They do, however, tend to cast some doubt on whether the quantitative differences between the sweat reduction efficacies of the products which were established by some of Unilever’s laboratory testing were actually able to be perceived by consumers in a non-laboratory real world setting. The point is that if the differences were not able to be perceived by consumers, it is difficult to see that they could support the conclusion that the products were therefore not similar.
369 It must be accepted, however, that even on this limited and narrow point, the blind home user tests were deserving of only fairly limited weight. Were it not for the deficiencies in the laboratory testing, in particular the fact that the head-to-head tests without any baseline measurement were unable to provide any real assistance in determining the relative extent or significance of the differences in sweat reduction efficacy, the blind home user tests would have provided little assistance in determining whether or not the Similarity Representations were false.
370 Unilever relied on Beiersdorf’s internal documents which revealed the number and nature of complaints that had been made to it concerning the Nivea Stress Protect Clinical Strength range. It submitted that those complaints showed “a clear picture of consumer disappointment as to the misrepresentation made for [Nivea Stress Protect Clinical Strength] that it was of a clinical standard”.
371 The complaint evidence, however, must be put in context. The following three points may be made.
372 First, the evidence was that 125 complaints were made between October 2014 and October 2016. Of those complaints, only 59 related to efficacy. Having regard to the evidence concerning the volume of sales during that period, it would be surprising if there were no complaints. The number of complaints was on any view very small.
373 Second, close consideration of the 59 efficacy-related complaints reveals that many of them could not necessarily be said to be complaints about the antiperspirant efficacy of the Nivea product in the narrow terms of sweat reduction. Some of them relate to complaints about the lack of odour control or other matters unrelated to sweat reduction. Many of them simply complain that the product was not as effective as the consumer thought it would be, or that it compared unfavourably with Rexona or Dove Clinical Protection, without identifying the precise reason for the disappointment, or the precise reason why the product did not meet their expectations.
374 Third, and perhaps most significantly, very few of the complaints indicated that the consumer considered that they had been misled by Beiersdorf because of the way the product had been marketed. None suggested in clear terms that the consumer was misled on the basis of a misrepresentation or misrepresentations along the lines of either the Similarity or Superiority Representations, though one referred to the product comparing unfavourably to “deodorants marketed similarly”.
375 Evidence that members of the public have actually been misled may be relevant, but is neither necessary nor conclusive: Parkdale at 198-199. Such evidence, however, may be of limited relevance or utility, particularly in circumstances where it may have no statistical significance, and the Court cannot draw inferences from it that any significant section or fraction of the population, or the relevant part of it, had or would have had similar reactions: Homart Pharmaceuticals Pty Ltd v Careline Australia Pty Ltd (2017) 349 ALR 598; FCA 403 at [32]. If the inference that the impugned conduct was likely to mislead or deceive is open, independently of such evidence, then it may be that the evidence can strengthen the inference: Verrocchi v Direct Chemist Outlet Pty Ltd (2015) 228 FCR 189 at [94]; State Government Insurance Corporation v Government Insurance Office of New South Wales (1991) 28 FCR 511 at 529. That, however, was not the case here.
376 While the complaint evidence was relevant, it was deserving of little, if any, weight in determining whether the Similarity and Superiority Representations were or were not false.
377 Much the same can be said about Unilever’s reliance on the evidence concerning the relatively poor market performance of the Nivea Stress Protect Clinical Strength range.
378 Unilever contended that the evidence of the low repurchase rate of Nivea Stress Protect Clinical Strength, the failure of the product to meet Beiersdorf’s sales expectations, and the removal of the product from the market after only 30 months, amongst other things, provided “an overwhelming basis for a finding that the antiperspirant efficacy of [Nivea Stress Protect Clinical Strength] was not of a ‘clinical standard’”. Unilever’s reference to “clinical standard” in that context may be taken to be a reference to antiperspirant benchmark efficacy, in terms of sweat reduction, which had allegedly been established by Rexona and Dove Clinical Protection and Mitchum Clinical.
379 The difficulty with that submission, however, is that the evidence tended to suggest that the failure of Nivea Stress Protect Clinical Strength to meet Beiersdorf’s sales expectations may have been the product of various factors, not just antiperspirant efficacy. As was noted earlier, the poor sales performance of the Nivea product was one of the main reasons Beiersdorf commissioned further market research from Lonergan Research in 2015. Ms Braun’s evidence was that the further work by Lonergan Research showed, amongst other things, that there was no clear conclusive reason for the sales performance issue and that there was “no unique issue with the antiperspirant and deodorant efficacy of the Nivea product”. The suggestion appeared to be that the issue concerning poor sales performance arose across the range of “clinical” products, or at least some of the other products in that range, not just Nivea’s product.
380 Data obtained by Ms Braun from a commercial data provider, Quantium, also showed that, while there may have been an issue with the repurchase rates of Nivea Stress Protect Clinical Strength, the repurchase rates were higher than the repurchase rates of one particular variant in the Rexona Clinical Protection range which had been introduced into the market at about the same time.
381 Two of Unilever’s witnesses, Mr McCarthy and Mr Mark Whitby, who was a Consumer Markets Insights Manager at Unilever, agreed that product sales or repurchase rates could be influenced by a number of factors. Mr McCarthy said it could be the name, the colour of the pack or the fragrance. Mr Whitby agreed that marketing and advertising may have some impact on repurchase rates.
382 Unilever relied on some passages from the Lonergan Research presentation which suggested that the poor market performance of the Nivea product was due to a combination of factors, including efficacy. The key finding in relation to efficacy was in the following terms:
EFFICACY – Efficacy is an issue, and perceptions of efficacy remain stronger for Rexona than NIVEA. However, data amongst users suggests that it is an issue experienced by other Clinical segment brands. NIVEA’s Clinical deodorant is performing at or close to par with Rexona across all key efficacy measures amongst current users, consistent with the results from the BHUT tests conducted before the product line was launched. We believe that consumers looking for the strongest product on the market are moving to Rexona, primarily driven by brand perceptions and Rexona’s strong brand presence in the segment rather than a unique issue with the efficacy of the NIVEA product line. Where dissatisfaction with efficacy occurs this is often due to performance not meeting the heightened expectations of performance suggested by the price point and the ‘clinical’ positioning – an issue we expect occurs across a range of clinical brands.
383 The following points may be made concerning that finding. First, the issue concerning efficacy was said to be an issue “experienced by other Clinical segment brands”, not just Nivea. Second, it reiterates the conclusion, based on the blind home user tests, that the Nivea product was performing “at or close to par with Rexona across all key efficacy measures”. Third, and critically, the poor market performance appeared to Lonergan Research to be a result of consumers moving to Rexona due to “brand perceptions and Rexona’s strong brand presence”. That is a consideration quite separate to efficacy.
384 These three points just discussed are inconsistent with Unilever’s contention that the overwhelming inference from the poor market performance was that the Nivea product did not meet the so-called “clinical standard” in terms of antiperspirant efficacy. Rather, the poor performance appeared to have more to do with consumer perceptions, including brand perceptions.
385 It should also be noted that the Lonergan Research findings also do not support Unilever’s narrow interpretation of the efficacy of an antiperspirant deodorant as only involving the reduction of sweat. Lonergan Research reported that consumers saw efficacy in terms of a product that “delivers on two key requirements: providing long-lasting protection and preventing smells”. Unilever’s submissions continually ignored the second element of efficacy.
386 It may again be accepted that the evidence concerning the poor market performance of Nivea Stress Protect Clinical Strength had some relevance to the question concerning the alleged falsity of the Similarity Representations, and perhaps the Superiority Representations. On balance, however, it does not carry much weight because the poor market performance may have been due to any number of factors, not just the narrow concept of antiperspirant efficacy involved in the Similarity and Superiority Representations.
The Nivea Stress Protect stick in the United Kingdom
387 Finally, Unilever relied on evidence which suggested that the Nivea Stress Protect stick was sold in the United Kingdom at the same price point as the Stress Protect roll-on and deodorant. That, in Unilever’s submission, was the “normal” price for an “ordinary” antiperspirant deodorant. In Unilever’s submission, that fact supported the inference that the product did not properly belong in the “clinical club” and was not superior to ordinary antiperspirant deodorants.
388 There is, however, no merit in that submission. That is so for a number of reasons.
389 First, the Nivea Stress Protect Clinical Strength stick sold in Australia was not identical to the product sold in the United Kingdom. The product sold in Australia had additional or stronger fragrance.
390 Second, there was no clinical segment or subcategory in the antiperspirant market in the United Kingdom.
391 Third, there was very little evidence concerning the market in the United Kingdom, including the prices of the Nivea Stress Protect products compared with other antiperspirant deodorants.
392 Fourth, and perhaps most significantly, there is no direct relationship between the price of an antiperspirant deodorant and its efficacy. Unilever adduced no evidence to justify the significantly higher prices it charged for its Clinical Protection range. While the apparently large disparity between the price of the Stress Protect stick in the United Kingdom and the price of the Stress Protect Clinical Strength stick in Australia might tend to suggest that Beiersdorf intended to take advantage of the higher prices that consumers might be prepared to pay for products in the clinical segment, that itself is not probative of whether the product in fact was not as efficacious as the Rexona and Dove Clinical Protection products, or was not superior to other antiperspirant deodorants.
Conclusion in relation to the falsity of the Similarity and Superiority Representations
393 For all the reasons given in detail earlier, the evidence concerning laboratory tests and test results alone does not prove, on the balance of probabilities, that the Similarity Representations, if made, were false. The tests were capable of proving that the antiperspirant efficacy of the Nivea Stress Protect Clinical Strength product, in terms of reducing sweat, was not the same as the antiperspirant efficacy of the Rexona Clinical Protection, and perhaps the Mitchum Clinical products. Indeed, the tests tended to prove that the antiperspirant efficacy of the Nivea product was not as good as the antiperspirant efficacy of the Rexona product. The difficulty for Unilever, however, is that the test results were not able to reliably establish that the relative size or significance of the different antiperspirant efficacy of the respective products was such that it could safely be concluded that the Nivea product was not “similar” to the Rexona product.
394 That difficulty was compounded by the indeterminate nature of the word “similar” as a comparator and by the fact that it was not possible to reliably exclude the proposition that some of the differences revealed by the results would not necessarily have been able to be perceived by consumers. There were also other gaps in the testing evidence, including that none of the tests related specifically to the Dove Clinical Protection products, which it was accepted contained different formulations to the Rexona products.
395 For the reasons just given, the evidence concerning the blind home user tests, while not particularly significant, nonetheless make it even more difficult to conclude that the Similarity Representations were false. While those tests were plainly not capable of measuring or determining the antiperspirant efficacy of the respective products, in terms of sweat reduction, the results nonetheless tend to suggest that the differences between the products in terms of sweat reduction efficacy may not have been able to be perceived by consumers in a real world, as opposed to laboratory, setting.
396 The other considerations relied on by Unilever, including the consumer complaints and the evidence concerning the poor market performance of the Nivea product provided some very minor support for the proposition that the efficacy of the Nivea product was not similar to the efficacy of the Rexona product. Ultimately, however, that support did not make up for the relevant deficiencies and gaps in the testing evidence.
397 Considering the evidence as a whole, Unilever did not discharge its burden of proving, on the balance of probabilities, that the Similarity Representations, if made, were false. Nor did it prove that, if made, they were misleading or deceptive.
398 The Superiority Representations are, however, a different matter. If they were made, the evidence concerning Unilever’s head-to-head laboratory thermal test between one of its stick deodorants and the Nivea Stress Protect Clinical Strength stick (test #4) did establish that the Nivea product did not provide “greater antiperspirant efficacy” or “a greater level of antiperspirant protection” than all other antiperspirant deodorants ordinarily available from supermarkets in Australia. That is because that test proved, on balance, that the Nivea Stress Protect Clinical Strength stick did not provide greater antiperspirant efficacy, or greater antiperspirant protection, in terms of sweat reduction, than one of Rexona’s antiperspirant sticks that was a so-called “non-clinical” product. That is sufficient to prove the falsity of at least representation 3. That conclusion would not necessarily apply to representation 7, which concerns stress sweat specifically, given the deficiencies in Unilever’s head-to-head stress test (test #5).
Issue 3: Were the Stress Sweat Representations false?
399 This issue relates primarily to representation 9, which is that “Nivea Stress Protect Clinical Strength has a particularly strong efficacy for consumers who suffer from stress sweat”. Beiersdorf admitted that it made that representation. Representation 10, is in somewhat similar terms, but involves a representation concerning future matters. It is dealt with separately in that context.
400 Unilever’s case concerning the falsity of representation 9 was misconceived. Unilever contended that representation 9 was false because Beiersdorf’s own testing showed that the Nivea Stress Protect Clinical Strength stick was less efficacious than the Stress Protect roll-on and had the same efficacy as the Stress Protect aerosol. The results of Beiersdorf’s tests (tests #7, #8, #9 and #10 in Unilever’s materials) and the limited conclusions that can be drawn from them were referred to earlier and do not need to be repeated. Suffice it to say in this context that Unilever’s contentions in relation to the results of the test are based on a selective and incomplete reading of the results and Dr Schmidt-Rose’s evidence in relation to them.
401 In any event, even if the Nivea Stress Protect Clinical Strength stick was less efficacious than the Stress Protect roll-on, and had the same efficacy as the aerosol, that would not prove that it did not have strong efficacy for consumers who suffer from stress sweat. The conclusion of the paper co-authored by Dr Schmidt-Rose, which included the test results relied on by Unilever, was as follows:
In conclusion, we were able to show, for the first time, a highly effective reduction in emotionally induced axillary sweating for three different topical AP formulas 48 h after product application. The roll-on, the stick and the aerosol substantially reduced both underarm wetness and malodour. Also, as shown exemplarily for the roll-on, thermally induced perspiration was effectively decreased.
402 The substance and effect of that conclusion was that each of the Stress Protect products – the stick, the roll-on and the aerosol – had strong efficacy for consumers who suffer from stress sweat. Dr Schmidt-Rose maintained that opinion in his evidence. Nothing of substance that emerged in the course of cross-examination cast any material doubt on the opinion or its basis. Ms Braun’s evidence was also that, based on what she understood about the testing of the Stress Protect products, each of them showed high efficacy against stress sweat and each of them could have been marketed as high-efficacy products.
403 Unilever did not prove the falsity of the non-future Stress Sweat Representation.
Issue 4: Future matters and reasonable grounds
404 For the reasons already given, the evidence does not support a finding that Beiersdorf made any of the Similarity and Superiority Representations that comprised or included representations as to future matters (representations 2, 4, 6, 8 and 11). There was no dispute that those representations, if made, comprised or included representations as to future matters.
405 If, however, contrary to that conclusion, those representations were made, the question arises whether Beiersdorf had reasonable grounds for making them. The same question arises in relation to the remaining Stress Sweat Representation (representation 10), which also comprised or included a representation as to future matters.
406 It should be noted, in this context, that while s 4(2) of the ACL imposes an evidential burden on Beiersdorf, it does not impose a legal burden of proving that reasonable grounds existed for the making of the representations as to future matters: Fubilan Catering Services Ltd v Compass Group (Australia) Pty Ltd [2007] FCA 1205 at [545], [548]; North East Equity Pty Ltd v Proud Nominees Pty Ltd (2010) 269 ALR 262; FCAFC 60 at [29]-[33]; Crowley v WorleyParsons Limited [2017] FCA 3 at [71].
407 The general operation of s 4 of the ACL would appear to be as follows: first, if the person who made the representation as to a future matter does not adduce any evidence of reasonable grounds for making the representation, the representation will be taken to be misleading; second, the representor will not be taken to have had reasonable grounds merely because some evidence of reasonable grounds is adduced; third, if the representor does adduce evidence of reasonable grounds, the representor does not bear the legal onus of establishing that they had reasonable grounds for making the representation; fourth, even if reasonable grounds are established, the representation may still be found to be misleading on general principles.
Were there reasonable grounds for the future Similarity Representations?
408 This question must be addressed on the hypothetical basis that, contrary to the findings that have been made, by marketing, distributing and selling Nivea Stress Protect Clinical Strength in the way it did, Beiersdorf represented that the product would, if used, provide similar antiperspirant protection, to Rexona and Dove Clinical Protection and Mitchum Clinical (representation 2), or similar antiperspirant protection to Rexona and Dove Clinical Protection and Mitchum Clinical against stress sweat (representation 6). Those representations must also be construed or interpreted in terms of the particulars supplied by Unilever; meaning that the expressions “similar antiperspirant efficacy” and “similar antiperspirant protection” have their ordinary English meaning and the criterion for efficacy and protection is a comparison of perspiration reduction, following application of the antiperspirant by the consumer.
409 The question is whether Beiersdorf had reasonable grounds for making those representations.
410 Beiersdorf faced a practical difficulty in addressing this question which was, at least in some respects, similar to the difficulty adverted to by Sheppard and Neaves JJ in Cummings v Lewis (1993) 41 FCR 559, a case which concerned the predecessor provisions in s 41(2) of the Fair Trading Act 1987 (NSW) and s 52 of the Trade Practices Act 1974 (Cth). Their Honours said (at 565-566):
That raises a practical difficulty about the application of subs (2) of s 41 to some cases. There are many cases, whether under s 52 of the Trade Practices Act or s 42 of the Fair Trading Act, where the principal protagonists are not dishonest or fraudulent. Each gives evidence to the best of his or her ability of conversations which took place before a transaction was entered into or other steps were taken. One party alleges inducement by misleading or deceptive conduct. The other party denies it because he or she says that nothing of that kind was said. That evidence is given honestly and to the best of the witness’s recollection. Yet so often a judge will find that party’s evidence unreliable, but it will be rejected, not because it is dishonest but because it is mistaken. The question arises how, from a practical point of view, can a witness in that situation face up to what is to him or her a false position. Evidence needs to be given to show reasonable grounds for the making of a statement that the witness claims never to have made. That was the position both [the representors] would have been placed in if an attempt had been made to elicit evidence of reasonable grounds from them.
411 This case, of course, was not concerned with a representation said to have been made during a disputed conversation. It concerned Beiersdorf’s conduct in marketing Nivea Stress Protect Clinical Strength and whether it impliedly or implicitly conveyed the Similarity Representations, including those which involved representations as to future matters, to ordinary reasonable consumers of antiperspirant deodorants in Australia. The situation is similar to that considered in Cummings v Lewis, however, in that Beiersdorf denied that it intended to make, or did in fact make, the Similarity Representations. Beiersdorf’s case was that it intended to convey that Nivea Stress Protect Clinical Strength was a high-efficacy product and, in that very limited respect, was similar to Rexona and Dove Clinical Protection. It did not, however, intend to convey, and on its case did not convey, that the Nivea product was similar to the Rexona and Dove products in the specific and narrow sense contended by Unilever. Beiersdorf maintained, however, that if the Court found that it did make the relevant representations, the evidence nonetheless established that it had reasonable grounds for making them.
412 Beiersdorf relied on five categories of evidence which it contended established reasonable grounds for making the Similarity Representations as to future matters.
413 The first category was evidence that established that Nivea Stress Protect Clinical Strength contained the same form of aluminium salt active (AZAG) as the Rexona and Dove Clinical Protection products.
414 The second category was evidence, primarily from Ms Braun and Dr Schmidt-Rose, which was said to establish that Beiersdorf’s internal assessment, based on information provided by Beiersdorf AG, was that Nivea Stress Protect Clinical Strength had a more advanced formulation, a higher level of fragrance and a higher overall antiperspirant and deodorant efficacy against stress sweat than the Nivea Stress Protect roll-on and aerosol variants.
415 The third category was evidence which was said to establish that Beiersdorf’s internal marketing assessment was that Nivea Stress Protect Clinical Strength was a high-efficacy product with respect to stress sweat.
416 The fourth category was evidence concerning Beiersdorf’s internal scientific testing, recorded in the paper co-authored by Dr Schmidt-Rose, which concluded that the Nivea Stress Protect stick, which was the same as the Nivea Stress Protect Clinical Strength stick save for the amount of fragrance, was “highly effective” in reducing “emotionally-induced axillary sweating and malodor production”. As has already been discussed in detail, the test results were that, 48 hours after application, the stick achieved a median sweat reduction (compared to the untreated axilla) of 52.7% for the female test subjects and 67.3% for the male subjects and that at least 50% of the subjects obtained a sweat reduction of at least 30%.
417 The fifth category was evidence concerning the blind home user tests conducted by Lonergan Research.
418 Two questions arise in relation to this evidence: first, whether it was in fact evidence of reasonable grounds such that Beiersdorf discharged its evidential burden pursuant to s 4(2) of the ACL; and second, if so, whether Unilever nonetheless discharged its legal burden of proving that Beiersdorf did not have reasonable grounds.
419 It may be accepted that the five categories of evidence were capable, in combination, of discharging Beiersdorf’s evidential burden under s 4(2) of the ACL. The more difficult question is whether the evidence, considered as a whole, established that Beiersdorf did not have reasonable grounds for making the Similarity Representations which involved representations as to future matters. It is, in that regard, necessary to separately consider each of the five categories of evidence relied on by Beiersdorf.
The Nivea product contained the same aluminium salt active
420 There was evidence that Nivea Stress Protect Clinical Strength contained the same aluminium salt active as the Rexona and Dove Clinical Protection products. However, even if it is accepted that Beiersdorf was aware of that fact at the time the relevant representations were made, that alone would not have provided reasonable grounds for the making of the representations.
421 The mere presence of that ingredient in the Nivea product could not provide a reasonable basis for a representation that the Nivea product had similar antiperspirant efficacy, in terms of sweat reduction, to the rival Rexona and Dove products. There was no evidence that the mere presence of the same relevant aluminium salt in two products, irrespective of the amount of the active ingredient and other features of the product formulation of each product, could provide a reliable guide to the comparative antiperspirant efficacy of those products. Indeed, the evidence tended to suggest quite to the contrary. Even the presence of a comparable amount of that active ingredient in the products would not necessarily have provided a reliable guide to the comparative antiperspirant efficacy of the products. In any event, the evidence did not go so far as to establish that the Nivea product contained the same, or a comparable, amount of that active ingredient as the Rexona and Dove products, let alone that that fact was known to Beiersdorf at the relevant time.
The efficacy of the Nivea Stress Protect Clinical Strength stick as compared to the roll-on and aerosol variants
422 It is difficult to see how Beiersdorf’s knowledge or understanding of the efficacy of the Nivea Stress Protect Clinical Strength stick, as compared to the efficacy of the Stress Protect roll-on and aerosol variants, could provide reasonable grounds for the making of the relevant Similarity Representations. The relevant Similarity Representations concerned the relative antiperspirant efficacy of Nivea Stress Protect Clinical Strength as against the Rexona and Dove Clinical Protection products. Beiersdorf’s understanding about how its own Stress Protect products compared amongst themselves could not bear on the comparative efficacy as against the Rexona and Dove products.
Beiersdorf’s belief that its product was “high efficacy”
423 It may be accepted, for present purposes, that Ms Braun understood and believed that “clinical”, in the context of the clinical segment or subcategory of the market for antiperspirant deodorants in Australia, meant “high efficacy”. It may also be accepted that Ms Braun understood, based on Beiersdorf AG’s scientific testing and the Lonergan Research blind home user tests, that Nivea Stress Protect Clinical Strength could properly be characterised as a high-efficacy product, at least with respect to stress sweat. Even so, it is difficult to see how Ms Braun’s understanding concerning those two matters could provide reasonable grounds for a representation that the Nivea product would, if used, provide similar antiperspirant protection to the rival Rexona, Dove and Mitchum products, either generally or in terms of stress sweat specifically.
424 It should also be noted in this context that, while the general tenor of Ms Braun’s evidence was that she believed that Beiersdorf had reasonable grounds to represent the Nivea product as a high efficacy product, she did not go so far as to say that she believed that Beiersdorf had reasonable grounds to represent that the Nivea product, if used, would provide similar antiperspirant efficacy to the rival Rexona, Dove and Mitchum products. That is because she did not believe that Beiersdorf made any such representation. The absence of such testimonial evidence was perhaps a product of the Cummings v Lewis conundrum referred to earlier.
425 The absence of such evidence from Ms Braun was not, however, fatal to Beiersdorf’s case in relation to reasonable grounds. That point was illustrated in Cummings v Lewis itself, where after referring to the conundrum faced by a person who, despite denying making a future representation, must attempt to adduce evidence of reasonable grounds, Sheppard and Neaves JJ said (at 566):
Evidence of reasonable grounds may be established by evidence other than that of the persons who are alleged to have made particular representations as to a future matter. Indeed, as in so many other areas, a court may find the overall probabilities to which the circumstances of a given case give rise, the background to it and the conduct of parties prior to conversations taking place as providing better guides to whether or not they had particular states of mind or whether particular factors existed which would establish evidence of something such as reasonable grounds. It was the overall circumstances of the case which enabled his Honour to say, in relation to both [the representors], that each genuinely believed the encouraging assertions which his Honour found them to have made. If one changes the exercise to an inquiry, not into genuine or honest belief, but into whether there were reasonable grounds, it is again the overall circumstances of the case which will provide more reliable guidance than would oral evidence on the part of interested parties.
426 The problem for Beiersdorf, however, is that the “overall circumstances” which informed Ms Braun’s belief that Nivea Stress Protect Clinical Strength was a high-efficacy product were essentially limited to her knowledge of Beiersdorf AG’s scientific testing and the blind home user tests. As will be seen, while those two types of testing may have given Beiersdorf reasonable grounds to represent that Nivea Stress Protect Clinical Strength was a high-efficacy product, they did not give it reasonable grounds to make favourable representations comparing the sweat reduction efficacy of the Nivea product with Rexona and Dove Clinical Protection.
427 In any event, the mere fact that Ms Braun believed that the Nivea products were high efficacy products which could legitimately be said to belong in the high efficacy clinical subcategory or segment of the market, does not provide reasonable grounds for specific representations which compared the sweat reduction efficacy or protection of the Nivea Stress Protect Clinical Strength, if used, with the sweat reduction efficacy of the Rexona and Dove Clinical Protection products.
Beiersdorf AG’s scientific testing
428 Beiersdorf AG’s scientific testing has already been discussed in detail. The critical point to note in this context is that Beiersdorf AG’s testing was limited to absolute stress tests of the Nivea Stress Protect Clinical Strength stick and the Stress Protect roll-on and aerosol, and an absolute thermal test of the roll-on. Beiersdorf AG did not conduct any absolute stress or thermal tests of the Nivea Stress Protect Clinical Strength or Dove Clinical Protection products, for the purposes of comparison with its testing of the Nivea products or generally. Nor did it conduct any head-to-head tests of the Nivea Stress Protect Clinical Strength products against the Rexona and Dove Clinical Protection products. In those circumstances, it is difficult to see how Beiersdorf AG’s scientific testing could provide reasonable grounds for representations that effectively compared the Nivea product’s antiperspirant efficacy with the antiperspirant efficacy of the rival Rexona and Dove products.
429 The difficulty inherent in Beiersdorf’s reliance on the scientific testing by Beiersdorf AG as providing reasonable grounds for the making of the relevant future representations are exacerbated by the fact that the evidence relating to its reliance on the testing was relatively thin. Ms Braun’s evidence was that each of the roll-on, aerosol and stick formats of the Stress Protect range had been proven by scientific testing to have a high level of efficacy against stress sweat. She did not, however, read the article co-authored by Dr Schmidt-Rose, or task anyone else at Beiersdorf to read it. Her evidence was that “Hamburg [Beiersdorf AG] informed us about this study … that it was successfully done”. It would appear, however, that all she knew was the “top line marketing information”, which was that “the product was a high efficacy product, meeting the FDS threshold”. There was no evidence that anyone else at Beiersdorf knew anything more than Ms Braun about the scientific testing.
430 In all the circumstances, the scientific testing by Beiersdorf AG, or so much of it as was known by Beiersdorf at the relevant time, was not capable of providing reasonable grounds for the relevant representations. As has already been indicated, at most it provided reasonable grounds for a belief that Nivea Stress Protect Clinical Strength was a high efficacy product.
431 The blind home user tests conducted by Lonergan Research on behalf of Beiersdorf have also already been the subject of considerable discussion. As was noted earlier, Beiersdorf accepted that it could not rely on the blind home user tests as proof of clinical or scientific levels of efficacy of antiperspirant deodorants. It also accepted that “some elements of the test could have been designed differently in some aspects”, though it took issue with Unilever’s contention that the tests suffered from “fundamental flaws”.
432 In its final written submissions, Beiersdorf noted that it did not depend on the blind home user tests to make out reasonable grounds. Rather, the evidence concerning the tests merely served “to bolster Beiersdorf’s pre-existing and reasonable understanding of the efficacy” of Nivea Stress Protect Clinical Strength. The pre-existing understanding was said to be the information provided by Beiersdorf AG. That was essentially the information which was provided concerning the scientific testing, though Ms Braun also indicated that Beiersdorf AG had advised that the Stress Protect stick had the highest concentration and the most scientifically advanced form of antiperspirant active as compared to the roll-on and aerosol formats.
433 The difficulty for Beiersdorf, however, is that, essentially for the reasons already given, the information provided by Beiersdorf AG was not capable of providing reasonable grounds for the Similarity Representations that concerned future matters. That information may have provided reasonable grounds for a representation that Nivea Stress Protect Clinical Strength was a highly efficacious product, and one that met the FDA’s criterion for an “extra-effective claim”. It did not, however, provide reasonable grounds for a representation that, if used, Nivea Stress Protect Clinical Strength would provide similar antiperspirant protection, in terms of a comparison of perspiration reduction, to Rexona and Dove Clinical Protection and Mitchum Clinical. That is because Beiersdorf AG’s scientific testing, and the other information provided by Beiersdorf AG, did not concern or involve any comparison between the Nivea product and the Rexona, Dove and Mitchum products in terms of antiperspirant efficacy.
434 Even putting Beiersdorf’s apparent concession concerning reliance on the blind user tests to one side, it is difficult to see how the blind home user tests could provide reasonable grounds for the Similarity Representations which include representations concerning future matters. That is so for at least three reasons.
435 First, as has already been indicated, there were some issues or problems with some aspects of the design of the tests. It is unnecessary to repeat what has already been said on that topic. For the reasons that have already been given, it would not be fair or accurate to characterise those issues as “fundamental flaws”, or as having “slanted” the tests in favour of the Nivea product. Nevertheless, the methodological problems mean that some of the test results should be approached with some degree of caution.
436 Second, the blind home user tests and test results should be approached having regard to the circumstances and purpose for which tests were commissioned. As has already been noted, they were commissioned for Beiersdorf’s internal business purposes; to assist it to make decisions concerning the possible launch of the Nivea Stress Protect stick as a high-efficacy product. That involved assessing whether the relevant product would perform as well as, or better than, the high efficacy Rexona and Dove products in terms of perceived antiperspirant and deodorant efficacy. The tests were not, and were not intended to be, scientifically rigorous testing of the antiperspirant efficacy of the respective products in quantitative sweat reduction terms. Nor were they commissioned for the purpose of determining whether Beiersdorf would or would not have reasonable grounds to make representations concerning the comparative antiperspirant efficacy, in terms of perspiration reduction, of the Nivea Stress Protect Clinical Strength product and the Rexona and Dove Clinical Protection products.
437 Third, having regard to the way they were particularised, the relevant Similarity Representations involved antiperspirant efficacy in a strictly quantitative sense; the criterion being a comparison of perspiration reduction following use of an antiperspirant by a consumer. Other than perhaps in one respect, the results of the blind home user tests said very little in terms of the actual quantitative antiperspirant efficacy of the respective products. The assessment of antiperspirant efficacy which was involved in the testing was essentially qualitative and based on consumer perceptions. It did not involve any actual measurement of perspiration reduction or any comparison of perspiration reduction in quantitative terms.
438 The one respect in which the results of the blind home user tests were potentially capable of shedding some light on the quantitative antiperspirant efficacy of the respective products was discussed earlier in the context of the issue whether the Similarity and Superiority Representations were false. As was noted in that context, there was an issue as to whether Unilever’s laboratory test results were capable of reliably determining the significance of the differences between the antiperspirant efficacies of the products which the testing detected. If the differences detected by the laboratory tests were such that they were unlikely to be perceived by consumers in the circumstances, it would be difficult to see why the differences meant that the products were relevantly dissimilar. The results of the blind home user tests tended to show, in that context, that the differences detected by the laboratory testing may not have been perceptible to consumers. Even in that context, however, the test results were deserving of only fairly limited weight.
439 The results of the blind home user tests were therefore not capable of providing Beiersdorf with reasonable grounds to make representations concerning the efficacy, in quantitative sweat reduction terms, of the product which it was proposing to launch as a high-efficacy product, as compared with the Rexona and Dove Clinical Protection products. Nor did Beiersdorf intend them to provide reasonable grounds for the making of any such representations. Had it wanted to conduct testing to provide it with reasonable grounds, it could perhaps have conducted laboratory tests, both absolute and head-to-head, which were capable of measuring the reduction of perspiration produced by the respective products. It did not do so. As has been seen, the only scientific tests which were conducted by Beiersdorf AG involved absolute sweat tests of the Nivea products alone.
Conclusion in relation to reasonable grounds for the future Similarity Representations
440 It follows that none of the evidence pointed to by Beiersdorf supported a finding that it had reasonable grounds to make the Similarity Representations which involved representations as to future matters. Nor was there any other basis for finding that Beiersdorf had reasonable grounds. The only available inference in the circumstances is that it did not. If follows that the representations, if made, were, or must be taken to have been, misleading.
Were there reasonable grounds for the future Superiority Representations?
441 This question must be addressed on the hypothetical basis that, contrary to the findings that have been made, by marketing, distributing and selling Nivea Stress Protect Clinical Strength in the way it did, Beiersdorf represented that the product would, if used, provide a greater level of antiperspirant protection than all other “non-clinical” antiperspirants ordinarily available from supermarkets in Australia (representation 4), or a higher level of protection from stress sweat than all other “non-clinical” antiperspirant deodorants ordinarily available in Australia (representations 8 and 11). As has already been noted, “non-clinical” antiperspirant deodorants, for the purposes of those representations, essentially meant all antiperspirant deodorants other than the Rexona and Dove Clinical Protection range and Mitchum Clinical.
442 Beiersdorf conceded that, if it made those representations, it did not adduce any evidence capable of discharging the evidential burden created by s 4(2) of the ACL. It must follow that that if, hypothetically, Beiersdorf did make the representations, they were, or must be taken to have been, misleading.
Were there reasonable grounds for the future Stress Sweat Representation?
443 Beiersdorf admitted that it made representation 10 and that it was a representation as to a future matter.
444 The relevant question is whether Beiersdorf had reasonable grounds for representing that Nivea Stress Protect Clinical Strength will, if used, provide particularly strong protection against stress sweat. According to Unilever’s particulars of this representation, the words “particularly strong protection” in this context are to be given their ordinary English meaning.
445 Neither party advanced any detailed submissions concerning this specific question. Beiersdorf, however, submitted generally that the five categories of evidence summarised earlier in the context of the question whether there were reasonable grounds for making the future Similarity Representations also established that it had reasonable grounds for making this representation. Unilever submitted, in equally general terms, that the five categories of evidence did not provide reasonable grounds.
446 Despite the paucity of submissions on the point, the resolution of this issue is fairly straightforward.
447 As was noted earlier, Beiersdorf AG advised Beiersdorf that it had conducted scientific tests which had established that the Nivea Stress Protect antiperspirant deodorants, including a version of the stick which, with the addition of further fragrance, came to be marketed and distributed in Australia as Nivea Stress Protect Clinical Strength, had a high level of efficacy against stress sweat. While Ms Braun did not read the paper which reported that scientific testing, nor did she have any particular reason to doubt what she had been told about it. She was involved in marketing and was not a scientist. She was entitled to rely on what she had been told by the scientists. The likely high efficacy of the product, including against stress sweat, was also confirmed, at least to an extent, by the results of Beiersdorf’s own blind home user tests.
448 In all the circumstances, the reported results of Beiersdorf AG’s scientific testing, and Beiersdorf’s own blind home use tests, provided reasonable grounds for the relevant Stress Sweat Representation.
449 This conclusion is also consistent with the reasons for finding that Unilever had not proved the falsity of the non-future Stress Sweat Representation (representation 9). The position in relation to this representation is plainly distinguishable from the position in relation to the future Similarity Representations. That is because this representation, like representation 9, does not involve any, or any direct, comparison between the perspiration reduction efficacy of Nivea Stress Protect Clinical Strength and Rexona and Dove Clinical Protection and Mitchum Clinical.
450 Following is a short summary of the findings that have been made.
451 First, Beiersdorf did not, in marketing, distributing and selling Nivea Stress Protect Clinical Strength, represent that Nivea Stress Protect Clinical Strength was a product with similar antiperspirant efficacy and characteristics to the Clinical Products (representation 1; FASOC 28(a)).
452 Second, if, contrary to the first finding, Beiersdorf did make representation 1, Unilever nevertheless did not prove on the balance of probabilities that it was false or misleading, or deceptive, or likely to mislead or deceive.
453 Third, Beiersdorf did not, in marketing, distributing and selling Nivea Stress Protect Clinical Strength, represent that Nivea Stress Protect Clinical Strength was a product which will, if used, provide similar antiperspirant protection to the Clinical Products (representation 2; FASOC 28(b)).
454 Fourth, if, contrary to the third finding, Beiersdorf did make representation 2, it did not have reasonable grounds for making it and it is therefore taken to be misleading.
455 Fifth, Beiersdorf did not, in marketing, distributing and selling Nivea Stress Protect Clinical Strength, represent that Nivea Stress Protect Clinical Strength was a product with greater antiperspirant efficacy than all other non-clinical antiperspirant deodorants ordinarily available in supermarkets in Australia (representation 3; FASOC 28(c)).
456 Sixth, if, contrary to the fifth finding, Beiersdorf did make representation 3, it was false or misleading, or deceptive, or likely to mislead or deceive.
457 Seventh, Beiersdorf did not, in marketing, distributing and selling Nivea Stress Protect Clinical Strength, represent that Nivea Stress Protect Clinical Strength was a product which will, if used, provide a greater level of antiperspirant protection than all other non-clinical antiperspirant deodorants ordinarily available in supermarkets in Australia (representation 4; FASOC 28(d)).
458 Eighth, if, contrary to the seventh finding, Beiersdorf did make representation 4, it did not have reasonable grounds for making it and it is therefore taken to be misleading.
459 Ninth, Beiersdorf did not, in marketing, distributing and selling Nivea Stress Protect Clinical Strength, represent that Nivea Stress Protect Clinical Strength was a product which had similar efficacy in preventing stress sweat to the Clinical Products (representation 5; FASOC 28(e)).
460 Tenth, if, contrary to the ninth finding, Beiersdorf did make representation 5, Unilever nevertheless did not prove on the balance of probabilities that it was false or misleading, or deceptive, or likely to mislead or deceive.
461 Eleventh, Beiersdorf did not, in marketing, distributing and selling Nivea Stress Protect Clinical Strength, represent that Nivea Stress Protect Clinical Strength was a product which will, if used, provide similar antiperspirant protection to the Clinical Products against stress sweat (representation 6; FASOC 28(f)).
462 Twelfth, if, contrary to the eleventh finding, Beiersdorf did make representation 6, it did not have reasonable grounds for making it and it is therefore taken to be misleading.
463 Thirteenth, Beiersdorf did not, in marketing, distributing and selling Nivea Stress Protect Clinical Strength, represent that Nivea Stress Protect Clinical Strength was a product with greater antiperspirant efficacy in protecting against stress sweat than all other non-clinical antiperspirant deodorants ordinarily available in supermarkets in Australia (representation 7; FASOC 28(g)).
464 Fourteenth, if, contrary to the thirteenth finding, Beiersdorf did make representation 7, Unilever nevertheless did not prove on the balance of probabilities that it was false or misleading, or deceptive, or likely to mislead or deceive.
465 Fifteenth, Beiersdorf did not, in marketing, distributing and selling Nivea Stress Protect Clinical Strength, represent that Nivea Stress Protect Clinical Strength was a product which, if used, would provide a higher level of protection from stress sweat than all other non-clinical antiperspirant deodorants ordinarily available in supermarkets in Australia (representation 8; FASOC 28(h)).
466 Sixteenth, if, however, contrary to the fifteenth, Beiersdorf did make representation 8, it did not have reasonable grounds for making it and it is therefore taken to be misleading.
467 Seventeenth, Beiersdorf did, in marketing, distributing and selling Nivea Stress Protect Clinical Strength, represent that Nivea Stress Protect Clinical Strength had a particularly strong efficacy for consumers who suffer from stress sweat (representation 9; FASOC 35(a)).
468 Eighteenth, Unilever did not prove, on the balance of probabilities, that representation 9 was false or misleading, or deceptive, or likely to mislead or deceive.
469 Nineteenth, Beiersdorf did, in marketing, distributing and selling Nivea Stress Protect Clinical Strength, represent that Nivea Stress Protect Clinical Strength will provide particularly strong protection against stress sweat (representation 10; FASOC 35(b)).
470 Twentieth, Beiersdorf had reasonable grounds for making representation 10. Unilever did not prove, on the balance of probabilities, that it was otherwise false or misleading, or deceptive, or likely to mislead or deceive.
471 Twenty-first, Beiersdorf did not, in marketing, distributing and selling Nivea Stress Protect Clinical Strength, represent that Nivea Stress Protect Clinical Strength will, if used, provide a higher level of protection from stress sweat than all other non-clinical antiperspirant deodorants ordinarily available in supermarkets in Australia (representation 11; FASOC 35(c)).
472 Twenty-second, if, contrary to the twenty-first finding, Beiersdorf did make representation 11, it did not have reasonable grounds for making it and it is therefore taken to be misleading.
473 In light of the findings that Beiersdorf did not make any of the Similarity or Superiority Representations, and the findings that the two admitted Stress Sweat Representations were not proved to be false or misleading, Unilever’s application must be dismissed with costs.
I certify that the preceding four hundred and seventy-three (473) numbered paragraphs are a true copy of the Reasons for Judgment herein of the Honourable Justice Wigney. |
Associate:
Dated: 20 December 2018