
FEDERAL COURT OF AUSTRALIA
Reckitt Benckiser (Australia) Pty Limited v AFT Pharmaceuticals (AU) Pty Limited [2018] FCA 1552
Table of Corrections | |
On the Orders Page, the date of order of “10 October 2018” has been replaced with “18 October 2018”. | |
9 May 2019 | In [15], the list numbers have been replaced with “(1)” and “(2)”. |
9 May 2019 | In [118], the list numbers have been replaced with “(1)” and “(2)”. |
ORDERS
DATE OF ORDER: |
THE COURT ORDERS THAT:
1. Within 14 days of the date of this order, the parties file and serve short minutes of orders to give effect to these reasons and for the further conduct of the proceeding.
Note: Entry of orders is dealt with in Rule 39.32 of the Federal Court Rules 2011.
GLEESON J:
Introduction
1 The applicant (“Reckitt”) and the respondent (“AFT”) market and sell over-the-counter (“OTC”) analgesics in Australia. AFT markets and sells Maxigesic and Reckitt markets and sells Nuromol. Ibuprofen and paracetamol (or acetaminophen) are also available OTC as “monotherapies”, that is, products containing a single active ingredient.
2 Maxigesic contains 500mg of paracetamol and 150mg of ibuprofen in a single tablet. The maximum recommended daily dosage of Maxigesic, published by AFT, is eight tablets (being a total dosage of 4000mg of paracetamol and 1200mg of ibuprofen).
3 Nuromol contains 500mg of paracetamol and 200mg of ibuprofen in a single capsule. The maximum recommended daily dosage of Nuromol, published by Reckitt, is three tablets (being a total dosage of 1500mg of paracetamol and 600mg of ibuprofen).
4 Thus, taken at their maximum daily dosages, Maxigesic delivers 2500mg more paracetamol and 600mg more ibuprofen than Nuromol.
5 Until 1 February 2018, codeine and codeine-based analgesics were available OTC in Australia. From that date, they became prescription-only medicines by reason of their listing in Sch 4 to the Therapeutic Goods Regulations 1990 (Cth). In anticipation of that regulatory change, AFT conducted an advertising campaign which promoted Maxigesic as a codeine-free analgesic, suitable for use by consumers of OTC codeine and codeine-based analgesics. Reckitt also marketed Nuromol as an alternative to codeine. The respective advertising campaigns made a variety of claims about the comparative benefits of Maxigesic and Nuromol over other products, including paracetamol and ibuprofen as monotherapies and in comparison with “other paracetamol/ibuprofen combinations”. The Nuromol campaign included explicit comparison of Nuromol and Maxigesic.
6 Each party alleges that the other has breached ss 18, 29(1)(a) and (g) and 33 of the Australian Consumer Law (“ACL”), being Sch 2 to the Competition and Consumer Act 2010 (Cth), by their advertising of Nuromol or Maxigesic respectively. That is, each alleges that the other has engaged in conduct that was misleading or deceptive, or likely to mislead or deceive in contravention of s 18 of the ACL, made false representations in contravention of ss 29(1)(a) and 29(1)(g) of the ACL and engaged in conduct that was misleading or liable to mislead in contravention of s 33 of the ACL.
7 Each party alleges that there is no adequate foundation in scientific knowledge for representations made by the other party in their respective advertising campaigns.
8 Each party claims declaratory and permanent injunctive relief and an order for the publication of corrective material. AFT claims damages or compensation from Reckitt. Reckitt did not pursue its claim for damages.
9 On 3 November 2017, Jagot J granted an interlocutory injunction, on Reckitt’s application, restraining AFT from broadcasting advertisements containing words to the effect of, or substantially similar to “Maxigesic delivers stronger pain relief than other paracetamol/ibuprofen combinations”, except in limited circumstances. On 28 November 2017, the interlocutory injunction was amended to cover words to the effect of, or substantially similar to “At maximum dosage, Maxigesic delivers better pain relief than other paracetamol/ibuprofen combinations”.
10 At the commencement of the hearing, I made an order pursuant to r 30.01 of the Federal Court Rules 2011 that, in relation to the cross-claim, all questions of whether there has been any contravention of the ACL and the nature and form of any declaratory and injunctive relief to be granted to AFT including relief by way of corrective advertising be determined separately from and prior to all other issues.
Summary of conclusions
11 In summary, my conclusions are as follows.
12 By publishing various of the advertisements the subject of the proceeding, AFT made representations that:
(1) Maxigesic provides stronger and more effective relief from all pain than Nuromol when taken at their respective maximum recommended daily doses;
(2) When taken at their respective maximum recommended daily doses, Maxigesic provides stronger and more effective relief from pain than any other paracetamol/ibuprofen combination.
13 Those representations were misleading or deceptive, or likely to mislead or deceive in contravention of s 18 of the ACL; they were misleading representations that the Maxigesic goods were of a particular quality, namely, able to provide the stronger and more effective pain relief referred to in the representations, in contravention of s 29(1)(a) of the ACL; and they were made in contravention of s 29(1)(g) of the ACL because they were misleading representations that the Maxigesic goods had the performance characteristics of providing stronger and more effective pain relief referred to in the representations. In the absence of an adequate scientific foundation, I also conclude that, by making the representations, AFT engaged in conduct that was liable to mislead the public as to the characteristics of the Maxigesic goods, in contravention of s 33 of the ACL.
14 AFT also engaged in conduct that was misleading or deceptive, or likely to mislead or deceive in contravention of s 18 of the ACL by making the further false representations that there was a current adequate foundation in scientific knowledge for the two representations set out above.
15 By publishing various of the advertisements the subject of the proceeding, AFT made representations that:
(1) when taken at their respective maximum recommended daily doses, Maxigesic provides stronger and more effective relief from pain than OTC doses of either paracetamol or ibuprofen alone; and
(2) Maxigesic reduces pain by at least 32% more than a full daily OTC dose of either paracetamol or ibuprofen alone throughout the period of administration of either drug.
16 Those representations were also misleading or deceptive, or likely to mislead or deceive in contravention of s 18 of the ACL and, by making the representations, AFT also contravened ss 29(1)(a) and (g) and 33 of the ACL.
17 Further, by making representations (3) and (4), AFT also engaged in conduct that was misleading or deceptive, or likely to mislead or deceive in contravention of s 18 of the ACL by making the further false representations that there was a current adequate foundation in scientific knowledge for those representations and that those representations were supported by the Merry study and the Mehlisch No. 1 study.
Legal framework
18 Section 18(1) of the ACL provides that a person must not, in trade or commerce, engage in conduct that is misleading or deceptive or is likely to mislead or deceive.
19 Section 29(1) provides relevantly:
A person must not, in trade or commerce, in connection with the supply or possible supply of goods or services or in connection with the promotion by any means of the supply or use of goods or services:
(a) make a false or misleading representation that goods are of a particular standard, quality, value, grade, composition, style or model or have had a particular history or particular previous use; or
…
(g) make a false or misleading representation that goods or services have sponsorship, approval, performance characteristics, accessories, uses or benefits; ...
20 Section 33 provides:
A person must not, in trade or commerce, engage in conduct that is liable to mislead the public as to the nature, the manufacturing process, the characteristics, the suitability for their purpose or the quantity of any goods.
Misleading or deceptive advertising
21 The principles applicable to determining whether conduct contravenes ss 18 or 29 of the ACL are not in dispute.
22 It is necessary first to determine whether each or any of the pleaded representations is conveyed by the various advertisements. The advertisements must be judged by their effect or likely effect on the ordinary or reasonable members of the relevant class of recipients of the advertising. Extreme or fanciful reactions should not be attributed to ordinary or reasonable members of the relevant class: Campomar Sociedad Limited v Nike International Limited [2000] HCA 12; (2000) 202 CLR 45 at [105].
23 In this case, the various advertisements (apart from the Nuromol television advertisements) were directed to health professionals, especially pharmacists, who advise or may advise consumers about OTC analgesics. In the case of the Maxigesic card and the Maxigesic pamphlet (which were distributed to pharmacies), the class of readers probably extends to pharmacists’ support staff who may also advise consumers about the use OTC analgesics to relieve pain. I would expect readers of the various print advertisements to be reasonably familiar with the different kinds of analgesics available to treat pain, including paracetamol, ibuprofen, codeine and codeine based products.
24 Second, it is necessary to ask whether the representations conveyed are false, misleading or deceptive or likely to mislead or deceive. This is a “quintessential question of fact”: Australian Competition and Consumer Commission v Telstra Corporation Limited [2004] FCA 987; (2004) 208 ALR 459 at [49].
25 An advertiser can lawfully compare a particular aspect of its product favourably with the same aspect of a competitor’s product provided the factual assertion is not untrue or a misleading half-truth: Gillette Australia Pty Ltd v Energiser Australia Pty Ltd [2002] FCAFC 223; (2002) 193 ALR 629 (“Gillette”) at [22] per Heerey J; at [43] per Lindgren J; at [91]-[93] per Merkel J.
26 A comparative, as distinct from a unilateral, promotion of a product necessarily indicates that the advertisement is not mere advertising puff, but involves representations of fact which are either true or false: Gillette at [44] per Lindgren J; Novartis Pharmaceuticals Australia Pty Ltd Bayer Australia Ltd [2015] FCA 35; (2015) 322 ALR 621 (“Novartis”) at [177] per Robertson J.
27 Particular care needs to be taken by an advertiser when they not only seek to boost their own product but also seeks to compare its competitor’s products unfavourably: Novartis at [177]. There are greater dangers in the “half-truth” or the unqualified literal truth in comparative advertising: Hoover (Aust) Pty Ltd v Email Ltd [1991] FCA 646; (1991) 104 ALR 369 at 375 per Gummow J; Telstra Corporation Ltd v Optus Communications Pty Ltd & Anor [1996] FCA 1035; (1996) 36 IPR 515 at 524 per Merkel J. Particular care to ensure that the advertisement is accurate is needed because errors made in comparative advertising may have a greater potential to mislead consumers than statements made in unilateral advertisements.
28 The phrase “liable to mislead” in s 33 of the ACL applies to a narrower range of conduct than that comprehended by the phrase “likely to mislead or deceive” appearing in s 18. A contravention of s 33 will not be made out unless “there was an actual probability that the public would be misled” by the impugned conduct: see Australian Competition and Consumer Commission v Coles Supermarkets [2014] FCA 634; (2014) 317 ALR 73 at [44] per Allsop CJ.
Adequate foundation in science for representations
29 Where claims are made of a scientific nature, proof that there is no scientific foundation for those claims may sufficiently establish that the claims are misleading: GlaxoSmithKline Australia Pty Ltd v Reckitt Benckiser (Australia) Pty Limited (No 2) [2018] FCA 1 at [49] (“GlaxoSmithKline”).
30 In Janssen Pharmaceutical Pty Limited v Pfizer Pty Ltd (1985) 6 IPR 227 at 234, Burchett J stated:
Of course it is correct that the onus is on the applicant, but it seems to me that proof that there is no scientific foundation for a statement in the realm of a science may be sufficient proof that the statement is misleading.
This will be so where in its context the statement must be, or is likely to be, taken as implying that there is adequate foundation in scientific knowledge to enable it to be made; cf Colgate Palmolive Pty Ltd v Rexona Pty Ltd (1981) 37 ALR 391.
31 In Janssen, the Court concluded that there was no scientific foundation for a suggestion that a particular chemical, mebendazole, may engender migration of roundworm.
32 In Sterling Winthrop Pty Ltd v Boots Co (Australia) Pty Ltd [1995] FCA 664; (1995) 32 IPR 361 at 365, in the context of an application for an interlocutory injunction, Tamberlin J stated at 365:
It can also, in my view, be misleading to make a statement which implies that there is an adequate foundation in scientific knowledge to justify it when taken in its context the scientific statement quoted does not provide a proper foundation; cf Colgate-Palmolive Pty Ltd v Rexona Pty Ltd [1981] FCA 146; (1981) 37 ALR 391; ATPR 40-242; [1981] FCA 146; 58 FLR 391; Duracell Australia Pty Ltd v Union CaReckittide Australia Ltd (1988) 14 ALR 293; ATPR 40-918; Janssen Pharmaceutical Pty Ltd v Pfizer Pty Ltd (1986) ATPR 40-654.
33 In Johnson & Johnson Pacific Pty Ltd v Unilever Australia Ltd (No 2) [2006] FCA 1646; (2006) 70 IPR 574 at [105], Bennett J said:
The onus is on Johnson to establish that the representation was misleading and deceptive but, following Burchett J’s observations in Janssen Pharmaceutical Pty Ltd v Pfizer Pty Ltd (1986) 6 IPR 227 at 234, if Johnson establishes that there is no foundation in the study for a statement in the advertisements, that may be sufficient proof that the statement is misleading. As his Honour recognised, the question is whether the context in which the representation is made implies that adequate foundation exists for making it.
34 In GlaxoSmithKline, Foster J held that, while there was a clinical study (the “Schachtel study”) that supported representations made as to the superiority of the analgesic Nurofen over Panadol, that single study did not form an adequate foundation in scientific knowledge for the representations of superiority due to subsequent Cochrane reviews which included data from the Schachtel study, but did not come to the same conclusion.. At [209], Foster J concluded that it was “too simplistic a view of the relevant body of scientific knowledge” to say that the Schachtel study had the “full force and effect that its authors claimed” in the light of the subsequent studies and meta-analysis, which concluded that “[n]o authoritative comparisons between active treatments is possible in the present state of knowledge”.
35 An appeal from Foster J’s decision was dismissed after the final hearing in this proceeding: Reckitt Benckiser (Australia) Pty Ltd v GlaxoSmithKline Australia Pty Ltd [2018] FCAFC 138. On the appeal, at [41], the Full Court concluded:
When evaluating whether there was an adequate foundation in the body of scientific knowledge to support the representations that were made, the primary judge did not err by taking into account the totality of the scientific evidence available at the relevant time. Further, the primary judge did not err by concluding that it would be misleading or deceptive, or likely to mislead or deceive, to make the impugned representations on the basis of the Schachtel Study alone, when the balance of the scientific evidence demonstrated no clear-cut superiority of ibuprofen over paracetamol in terms of faster and more effective relief from pain caused by common headaches including TTH. The body of scientific evidence, which took into account the findings of the Schachtel Study, but balanced them against the findings of other studies, did not support the making of simplistic comparisons of the kind found in Reckitt’s comparative advertising material. It was misleading for Reckitt to make the representations it did—which carried with them an unqualified and definitive statement of scientific fact—when the overall conclusion to be drawn from the scientific evidence was that no authoritative comparisons between active treatments were possible in the then state of scientific knowledge.
36 In Tobacco Institute of Australia Ltd v Australian Federation of Consumer Organisations Inc (1992) 38 FCR 1, the Full Court considered a representation that “there is little evidence and nothing which proves scientifically that cigarette smoke causes disease in non-smokers”. At 56, Hill J stated:
For the purposes of determining the falsity of the first part of the statement, it is unnecessary to embark upon a detailed study of the evidence criticising the studies which form the basis of the primary articles. I am, for the purposes of this part of the case, prepared to accept that many of the underlying studies suffer from defects, produce results which are not statistically significant and would not be accepted by all, or perhaps by even a majority of scientists, as rigorous proof in accordance with scientific method. But that does not mean that, looked at as a body of “evidence”, there is such a paucity that it could be dismissed as insignificant. A number of the studies show trends which, even if not statistically significant, point to an association and thus the possibility of a causal relationship between exposure to environmental tobacco smoke and cancer. A number of the Reviews accept these conclusions. That such an apparently authoritative body as the Surgeon General should, in its 1986 report, (albeit published after the date of the advertisement but based on studies available at that time) conclude the existence of causality is, even on its own, evidence of causality which is more than insignificant. Its existence, as even the existence of flawed (although not discredited in the major reviews) studies, makes the statement that there is little evidence that passive smoking causes disease in non-smokers misleading, or renders it likely to mislead.
37 In final submissions, senior counsel for AFT, Mr Crutchfield QC expressly disavowed a submission that the scientific evidence in this case is all one way.
38 AFT submitted that if it is shown that there is a legitimate body of scientific evidence to support an impugned statement, the allegations in relation to that statement should be rejected. AFT argued that a mere conflict in scientific views and/or the existence of conflicting scientific studies is not sufficient; it is, of course, unsurprising that scientists might hold different views on an issue. AFT contended that the very fact that two eminently qualified scientists hold different views on issues like those being considered in this case itself strongly suggests that there is an adequate scientific foundation for both views. Similarly, AFT said, the existence of conflicting clinical studies does not demonstrate that there is no scientific foundation for the conclusions reached in the conflicting studies. Rather, it illustrates that, even where clinical studies are conducted with rigour, there may be variability in the outcomes. Ultimately, AFT submitted that the Court should only uphold allegations of this nature where the scientific evidence is such that the impugned position cannot legitimately be maintained.
39 This submission does not adequately distinguish between statements of fact and statements of opinion. Of course, two eminently qualified scientists may reasonably hold contrary opinions about a matter of fact. However, where that is the case, their disagreement necessarily casts doubt on whether the fact is true or false.
40 It may be possible to extrapolate from the results of one or more clinical studies to reach a conclusion or conclusions that, in turn, may form an adequate foundation in science for a claim. Relevantly, Professor Christie, a professor of pharmacology who was called to give evidence by Reckitt, said:
The results from a single clinical trial can be tentatively extrapolated on the basis of that trial alone to what the behaviour of the trial agent will be in practice. The – those – that interpretation or that extrapolation is necessarily tentative if the trial is not very large or if there are other clinical trials on the same topic that have reliable evidence as well. In that case then all of the clinical trials should be taken together in the meta-analysis to determine whether the potential effect from one clinical trial is substantiated by other clinical trials. And if not, then the notion of the clinical effect of that one trial should be rejected. I hope that’s not too convoluted, but that – that’s the understood and gold standard process for evaluating clinical trials.
41 Again, where a claim of a scientific nature is not based on a scientific study that demonstrates the claim and eminently qualified scientists reasonably hold contrary opinions about the potential for extrapolation from other studies to make the claim, their disagreement necessarily casts doubt on whether the claim is true or false.
Reckitt’s case against AFT
42 Reckitt’s case concerns three publications, referred to as the Maxigesic print advertisement, the Maxigesic card (referred to by the parties variously as a “point of sale advertisement”, a “switch card” and a “dose information card”) and the Maxigesic pamphlet.
Maxigesic print advertisement
43 The Maxigesic print advertisement was developed in about July 2017. It has been published in the trade publications Australian Journal of Pharmacy, Australian Family Physician and Bite.
44 The following is the main text of the advertisement:
GO CODEINE FREE MAKE THE SWITCH TO MAXIGESIC®
MAXIGESIC® DELIVERS STRONGER PAIN RELIEF THAN OTHER PARACETAMOL/IBUPROFEN COMBINATIONS*
˃ The only Paracetamol/ibuprofen combination analgesic clinically proven to reduce pain levels by at least 32% more than a full daily OTC dose of either Paracetamol or Ibuprofen alone.1, 2
˃ The only combination analgesic that provides the maximum daily OTC dosage of paracetamol 4000mg and Ibuprofen 1200mg, if required **
˃ Provides a maximum daily dose of 8 tablets (1-2 tablets every 6 hours), if required, compared to 3 tablets daily (1 tablet every 8 hours) for other Paracetamol/Ibuprofen combinations.
˃ A unique patented combination of Paracetamol 500mg and Ibuprofen 150mg with no generic alternatives.
˃ GET BETTER PAIN RELIEF than Paracetamol or Ibuprofen alone1
45 The single asterisk at the end of the third line refers to the following statement in small font towards the bottom of the advertisement:
*Based on the maximum approved daily OTC dose of 8 tablets (Maxigesic®) vs. 3 tablets 500mg Paracetamol/200mg Ibuprofen combinations, with Maxigesic® being the only Paracetamol/Ibuprofen combination analgesic clinically proven to provide more effective pain relief than a full daily dose of Paracetamol or Ibuprofen alone.
46 Footnote 1 in the main text refers to a reference at the bottom of the advertisement, which states:
Merry, A.F., Gibbs, R.D. Edwards, J., Ting, G.S., Frompton, C., Davies, E. and Anderson, B.LJ. (2010), “Combined acetaminophen and ibuprofen for pain relief after oral surgery in adults: a randomized controlled trial” British Journal of Anaesthesia 104(1): 80-88 (“Merry study”)
47 Footnote 2 in the main text also refers to a reference at the bottom of the advertisement. That reference states:
Mehlisch, D.R., Aspley, S, Daniels, S.E., & Bandy, D.P. (2010. Comparison of the analgesic efficacy of concurrent ibuprofen and paracetamol with ibuprofen modified factorial study. Clinical Therapeutics, 32(5), 882-895. doi:10:1016/j.clinthera.2010.04.022 (“Mehlisch Study”)
48 For present purposes, it is unnecessary to set out the other text of the advertisement, or describe its features in more detail.
Maxigesic card
49 The Maxigesic card was distributed to pharmacies in 2017. The following is the main text of the card:
Maxigesic®
DELIVERS STRONGER PAIN RELIEF THAN OTHER PARACETAMOL/IBUPROFEN COMBINATIONS*
*Based on the maximum approved daily OTC dose of 8 tablets (Maxigesic®) vs. 3 tablets 500mg Paracetamol/200mg Ibuprofen combinations, with Maxigesic® being the only Paracetamol/Ibuprofen combination analgesic clinically proven to provide more effective pain relief than a full daily dose of Paracetamol or Ibuprofen alone 1, 2.
DOUBLE ACTION PAIN RELIEF WITHOUT CODEINE
50 At the bottom of the case are two references: the first is the citation for the Merry study which appeared in the Maxigesic print advertisement; the second is the citation for the Mehlisch (No. 1) study, which also appeared in the Maxigesic print advertisement.
51 AFT says that the card was intended to be placed behind the dispensary areas of pharmacies as a prompt for pharmacists. Based on its format, which gives prominence to the references in support of the advertisement’s asterisked claim and to AFT’s phone and facsimile numbers, I accept that the card is not directed to the public at large. Rather, it is directed to pharmacists and pharmacy assistants.
Maxigesic pamphlet
52 The Maxigesic pamphlet was distributed to pharmacists from March 2017, primarily by sales representatives on sales visits to pharmacists. It was also distributed on other occasions for promotional and informative purposes, for example, at conferences.
53 The pamphlet can be unfolded into a double sided page. Prominently stated, on three occasions, are the words:
GO CODEINE FREE MAKE THE SWITCH TO MAXIGESIC®.
54 In a prominent bright blue box, amongst other things, the pamphlet states:
Lead the change today and recommend your customers make the switch to MAXIGESIC:
The only paracetamol/ibuprofen combination proven to provide more effective pain relief than a full daily OTC dose of paracetamol or ibuprofen.
55 Under the heading “MAXIGESIC IS DIFFERENT”, the pamphlet states:
The only paracetamol/ibuprofen combination analgesic clinically proven to reduce pain levels by at least 32% more than a full daily OTC dose of either paracetamol or ibuprofen alone. 1, 2
56 Again, footnote 1 refers to a reference which cites the Merry study and footnote 2 refers to a citation of the Mehlisch (No. 1) study.
Issues for determination
57 Reckitt alleged that the Maxigesic advertising materials convey the following eight misrepresentations, itemised in accordance with Reckitt’s Fast Track Statement:
(a) Maxigesic provides stronger and more effective pain relief than Nuromol (print advertisement and card);
(b) Maxigesic is better than any other paracetamol/ibuprofen combinations (print advertisement and card);
(c) Maxigesic provides stronger and more effective pain relief than any other paracetamol/ibuprofen combination (print advertisement and card);
(d) A higher single and daily dosage of paracetamol/ibuprofen combination products provides for stronger and more effective pain relief compared to a lower dose of a paracetamol/ibuprofen product (all Maxigesic advertising materials);
(e) Maxigesic is stronger and more effective than OTC doses of either paracetamol or ibuprofen alone (all Maxigesic advertising materials);
(f) Maxigesic reduces pain by at least 32% more than a full daily OTC dose of either paracetamol or ibuprofen alone throughout the period of administration of either drug (all Maxigesic advertising materials);
…
(g) Maxigesic provides equivalent to or superior efficacy to codeine (all Maxigesic advertising materials);Maxigesic provides the same benefits to consumers as codeine (all Maxigesic advertising materials).
(“Maxigesic representations”).
58 Representation (g) in the Fast Track Statement was not pressed.
59 Reckitt also alleges that, in relation to each of the Maxigesic representations, there is a further representation that there is a current adequate foundation in scientific knowledge for that misrepresentation. AFT denies this allegation.
60 Reckitt further alleges that, in relation to each of the Maxigesic representations, there is a representation that the representation is supported by each of the Merry study and the Mehlisch (No. 1) study.
61 Reckitt alleges that there is no current adequate foundation in scientific knowledge for the Maxigesic representations; that the Merry study and the Mehlisch No. 1 study do not support those representations; and that, accordingly, the representations made by the Maxigesic advertisements are false and/or misleading or deceptive or likely to mislead or deceive.
62 AFT admits that the Maxigesic print advertisement and the Maxigesic card each convey representation (c) , except to the extent that (c) refers to “any” other paracetamol/ibuprofen combination. Otherwise, AFT otherwise denies that the alleged representations are conveyed by the Maxigesic advertising materials. In particular, AFT contended that the alleged representations did not correspond to, and placed a gloss on, the actual words used in the advertisements.
63 AFT says that the following three statements which appear in the Maxigesic advertisements are supported by the Merry study and the Mehlisch No. 1 study:
(1) Maxigesic print advertisement: “The only Paracetamol/ibuprofen combination analgesic clinically proven to reduce pain levels by at least 32% more than a full daily OTC dose of either Paracetamol or Ibuprofen alone”.
(2) Maxigesic card: “DELIVERS STRONGER PAIN RELIEF THAN OTHER PARACETAMOL/IBUPROFEN COMBINATIONS*”.
(3) Maxigesic pamphlet: “The only paracetamol/ibuprofen combination analgesic clinically proven to reduce pain levels by at least 32% more than a full daily OTC dose of either paracetamol or ibuprofen alone” and “The only paracetamol/ibuprofen combination proven to provide more effective pain relief than a full daily OTC dose of paracetamol or ibuprofen”.
64 Accordingly, AFT denies that representation (c) is false and denies that it has engaged in any conduct in contravention of the ACL.
65 Thus, the following issues arise for determination:
(1) Whether AFT made any of the Maxigesic representations by publishing the Maxigesic advertisements?
(2) Whether, in relation to each of the Maxigesic representations, AFT made a further representation that there is a current adequate foundation in scientific knowledge for that misrepresentation?
(3) Whether, in relation to each of the Maxigesic representations, AFT made a further representation that the representation was supported by the Merry study and the Mehlisch No 1 study?
(4) Whether Reckitt has established that there was no current adequate foundation in scientific knowledge for the Maxigesic representations?
(5) In the event that Reckitt has established one or more contraventions of the ACL, what relief, if any, should be granted?
66 Reckitt did not plead a case that any of the pleaded representations is a representation with respect to a future matter. Accordingly, it is not necessary to consider the operation of s 4 of the ACL in this case.
Alleged Maxigesic representations
67 Each party adduced evidence of the interpretation of the advertising materials by members of the class of persons to whom the materials were published.
68 I accepted that evidence of health professionals, as members of the class, may be relevant to determining whether the alleged representations were made.
Representation (a): Maxigesic provides stronger and more effective pain relief than Nuromol
69 Reckitt contended that this representation is conveyed by the words “MAXIGESIC® DELIVERS STRONGER PAIN RELIEF THAN OTHER PARACETAMOL/IBUPROFEN COMBINATIONS” in the print advertisement and the card, in the context of Nuromol being the leading competitor of Maxigesic.
70 AFT did not dispute that Maxigesic and Nuromol are competitors. In its written submissions, AFT contended that Maxigesic and Nuromol are the leading paracetamol/ibuprofen combination analgesics in Australia.
71 AFT argued that the word “stronger” in the Maxigesic advertisements referred to a higher dosage. In support of that contention, AFT relied on the following evidence:
(1) Dr Segal, a general practitioner, understood the phrase “stronger pain relief” to indicate that the levels of the active pharmaceutical ingredients (“APIs”) in the patient’s blood will be more consistent over a longer period of time, thereby producing a greater therapeutic benefit.
(2) Dr Foltyn, a dentist, understood the reference to “stronger” in the impugned statements to indicate that Maxigesic provides more of the APIs in question.
72 While I accept that many readers of the Maxigesic advertisements would read the word “stronger” to convey that Maxigesic had more APIs than the comparator product(s), in my view, “stronger pain relief” could also be understood by a reasonable member of the relevant class of readers to mean “stronger and more effective”, as the quality of strength in a product for pain relief may be understood to entail greater efficacy to reduce pain. As Dr Hay, an experienced general practitioner, put it: “My take of ‘stronger’ is more effective”. Thus, Dr Hay agreed, generally speaking, that he would expect to get increased efficacy from a drug the closer you get to the maximum dosage. Dr Hay also agreed that the strength of a medication can be assessed by looking at reductions in pain over time. In cross-examination, Dr Howe, an experienced dentist, also accepted that the “pain relief ability” of an analgesic could be called “strength”.
73 Mr McMaugh, an experienced pharmacist, understood the impugned statements to mean that “Maxigesic is able to achieve a greater reduction in pain than other paracetamol/ibuprofen combinations.” He understood “strength” in this context to refer to the “… magnitude of the effect of a product”. For Mr McMaugh, this referred to a patient’s subjective perception of pain and the duration over which the pain is reduced. Mr McMaugh understood the words “effective” and “efficacy” to have a similar meaning to “stronger”.
74 Taking this evidence into account, I accept that the print advertisement and the card convey representation (a).
75 Reckitt submitted that the representation should be understood to relate to all quantities of the products for all pain.
76 AFT did not argue that its language should be understood to be restricted to any particular type of pain such as, for example, dental pain. However, AFT contended that the Maxigesic print advertisement and the Maxigesic card are to be understood as referring to the daily dosing regimen of Maxigesic and, to the extent that it is relevant, the daily dosing regimen of other paracetamol/ibuprofen combinations. AFT contended that both of these advertisements make clear and prominent references to daily doses. I accept this submission in relation to the card. The position is less clear in the case of the print advertisement, to the extent that the asterisked words are in such small font that they may not be legible for many readers, however, in the context of the asterisk and the other references to maximum daily doses on that advertisement, I accept that a reasonable reader would not understand the representation to be entirely unqualified. Rather, it is to be understood to relate to the maximum approved daily OTC doses of Maxigesic and Nuromol and other paracetamol/ibuprofen combinations.
Representation (b): Maxigesic is better than any other paracetamol/ibuprofen combinations
77 Reckitt contended that this representation is conveyed by the words “MAXIGESIC® DELIVERS STRONGER PAIN RELIEF THAN OTHER PARACETAMOL/IBUPROFEN COMBINATIONS” in the print advertisement and the card. I do not accept that representation is conveyed where the words are followed by an asterisk which explains the meaning of the claim by reference to maximum approved daily doses. In that context, I do not accept that a reasonable reader of the relevant class would understand the advertisements to convey such a general representation of superiority.
Representation (c): Maxigesic provides stronger and more effective pain relief than any other paracetamol/ibuprofen combination
78 As noted above, AFT admits that the Maxigesic print advertisement and the Maxigesic card each convey the representation that Maxigesic provides stronger and more effective pain relief than other paracetamol/ibuprofen combinations. In my view, a reasonable reader may interpret the text “MAXIGESIC® DELIVERS STRONGER PAIN RELIEF THAN OTHER PARACETAMOL/IBUPROFEN COMBINATIONS” to imply that the comparison is being made with all available paracetamol/ibuprofen combinations and would not necessarily understand the comparison to be with a sub-set of the available paracetamol/ibuprofen combinations.
79 Accordingly, I find that representation (c) is conveyed by the Maxigesic print advertisement and the Maxigesic card.
Representation (d): A higher single and daily dosage of paracetamol/ibuprofen combination products provides for stronger and more effective pain relief compared to a lower dose of a paracetamol/ibuprofen combination product.
80 Reckitt contended that this representation is conveyed by the text “MAXIGESIC® DELIVERS STRONGER PAIN RELIEF THAN OTHER PARACETAMOL/IBUPROFEN COMBINATIONS” followed by the following two sub-headings:
˃ The only combination analgesic that provides the maximum daily OTC dosage of Paracetamol 4000mg and Ibuprofen 1200mg, if required **
˃ Provides a maximum daily dose of 8 tablets (1-2 tablets every 6 hours), if required, compared to 3 tablets daily (1 tablet every 8 hours) for other Paracetamol/Ibuprofen combinations.
81 Reckitt submitted that the representation being made is that Maxigesic is stronger than other paracetamol/ibuprofen combinations including because of the factors listed in the sub-paragraphs. Those factors include that you can take the maximum OTC dosage of paracetamol and ibuprofen and you can take more tablets of Maxigesic compared to other combinations.
82 In its Fast Track Statement, Reckitt noted that the pamphlet emphasises that the maximum dose of Maxigesic delivers 2.7 times more and 167% more paracetamol and two times more and 100% more ibuprofen than Nuromol (described as “other paracetamol/ibuprofen combination analgesics”).
83 I am not satisfied that representation (d) is conveyed by any of the Maxigesic advertising materials. For the print advertisement, in my view, an ordinary or reasonable member of the relevant class would be sufficiently astute to appreciate that the claim “MAXIGESIC® DELIVERS STRONGER PAIN RELIEF THAN OTHER PARACETAMOL/IBUPROFEN COMBINATIONS” is followed by an asterisk, referring them to additional information about the claim. The asterisk refers to a statement that the claim is based on maximum approved daily OTC doses. On this basis, an ordinary or reasonable member of the relevant class would not understand the claim to convey anything about single dosages of paracetamol/ibuprofen combination products.
84 For similar reasons, the other advertisements do not convey representations about the comparative efficacy of single dosages of combination paracetamol/ibuprofen products.
Representation (e): Maxigesic is stronger and more effective than OTC doses of either paracetamol or ibuprofen alone
85 Reckitt contended that this representation is conveyed by the express text of the banner at the bottom of the print advertisements, which states:
˃ GET BETTER PAIN RELIEF than Paracetamol or Ibuprofen alone
86 Similar language appears on the pamphlet.
87 In each case, the text is footnoted by a reference to the Merry study.
88 AFT’s written submissions noted that it did not appear to be in contest that a combination of ibuprofen and paracetamol is more effective than the monotherapies alone.
89 In my view, representation (e) is conveyed by print advertisement and the pamphlet. In my view, “better pain relief” could be understood by a reasonable member of the relevant class of readers to mean superior strength and efficacy, as the qualities of strength and effectiveness are qualities that are likely to make one form of pain relief better than another. In the absence of any qualifications, in my view, such a reasonable person could reasonably understand that this representation applies without any qualification. Similarly to representation (a), a reasonable member of the class would understand that representation (e) relates to the maximum approved daily OTC doses of Maxigesic and the monotherapies.
Representation (f): Maxigesic reduces pain by at least 32% more than a full daily OTC dose of either paracetamol or ibuprofen alone throughout the period of administration of either drug
90 Reckitt contended that this representation was conveyed by the following text of the print advertisement:
˃ The only Paracetamol/ibuprofen combination analgesic clinically proven to reduce pain levels by at least 32% more than a full daily OTC does of either Paracetamol or Ibuprofen alone.
91 Similar language appears on the pamphlet.
92 In each case, the text is footnoted by references to the Merry study and the Mehlisch No. 1 study.
93 Reckitt did not point to any relevant language in the card. In the absence of such language, representation (f) is not conveyed by that advertisement.
94 I did not understand AFT to seriously dispute that representation (f) is conveyed by the print advertisement and the pamphlet. In particular, AFT did not put an argument that the words “throughout the period of administration of either drug” were not conveyed to a reasonable member of the relevant class of readers. AFT’s submissions instead noted that the real issue which arises in the case relating to representation (f) is whether it is supported by the Merry Study.
95 Dr Segal, Dr Foltyn and Mr McMaugh understand the statement “The only Paracetamol/ibuprofen combination analgesic clinically proven to reduce pain levels by at least 32% more than a full daily OTC dose of either Paracetamol or Ibuprofen alone” to indicate that there is a study (comparing Maxigesic with the monotherapies) which supports this conclusion.
96 Taking these matters into account, I accept that representation (f) is conveyed by the print advertisement and the pamphlet.
Representations (h) and (i): equivalent or superior efficacy to codeine/same benefits as codeine
97 Reckitt relied on:
(1) The main banner in the print advertisements, which states:
“GO CODEINE FREE MAKE THE SWITCH TO MAXIGESIC”.
(2) The following words in the pamphlet:
GO CODEINE FREE MAKE THE SWITCH TO MAXIGESIC®
And
You don’t want to lose your codeine customers to the GP from February 2018, and GPs don’t want their waiting rooms filled with pain sufferers who can access suitable alternatives from their pharmacy – right now.
And
CHANGE IS COMING
CODEINE – PRESCRIPTION ONLY FROM 1st FEBRUARY 2018
Rescheduling provides an opportunity to lead the change with your customers by proactively recommending alternative pharmacy OTC analgesics before the implementation date.
Retain your codeine customer base by switching them to MAXIGESIC®, the only paracetamol/ibuprofen combination proved to provide superior analgesic efficacy than either a full OTC does paracetamol or ibuprofen alone.1, 2
98 Reckitt’s written submissions did not identify how the representations were said to have been made by the Maxigesic card. The card refers to codeine in the statement:
DOUBLE ACTION PAIN RELIEF WITHOUT CODEINE
99 Reckitt relied on the evidence of Dr Howe in support of these representations. Dr Howe said that he understood the statements “Go Codeine Free” and “Codeine Free” to mean:
(1) Maxigesic does not contain codeine;
(2) Maxigesic is a suitable alternative to analgesics that contain codeine; and
(3) Maxigesic gives equal to or better pain relief than analgesics that contain codeine.
100 In cross-examination about the Maxigesic print advertisement, Dr Howe said:
The ad is conveying that it gives the same pain relief as a codeine containing – over-the-counter codeine containing drug.
101 Dr Howe agreed that the advertisement was conveying that Maxigesic will give “comparable” pain relief to OTC codeine.
102 Mr McMaugh gave evidence that the statements “Go Codeine Free” and “Codeine Free” indicated that “Maxigesic is suitable for the treatment of pain for some patients that are taking analgesics which contain codeine. … Maxigesic can be considered as a treatment option for particularly severe cases of acute pain, acute pain being pain less than chronic pain and chronic pain being the type of pain that should be referred to a general practitioner for assessment and diagnosis”.
103 In cross-examination, Mr McMaugh did not accept that, for a codeine user to switch to Maxigesic, Maxigesic would need to offer the “same benefits” as codeine, saying “comparable benefits” would be sufficient.
104 Mr McMaugh rejected suggestions that a user of Maxigesic would get “equivalent benefits” or the “same benefits” as from a codeine product, preferring the words “comparable” and “similar”.
105 Despite Dr Howe’s affidavit evidence, I do not accept that any of the three Maxigesic advertisements conveys a representation that Maxigesic provides superior efficacy to codeine. Dr Howe did not identify the basis for his evidence that the relevant words convey a representation of “better” pain relief, and ultimately agreed that the representation was one of “comparable” pain relief to OTC codeine.
106 Further, the exhortation to “make the switch” (“switching” your codeine customer base, in the case of the pamphlet) conveys that Maxigesic is likely be a suitable alternative to codeine for consumers. The advertisements represent that Maxigesic can be recommended to consumers, who are currently using codeine or who would otherwise use codeine, as a product of equivalent efficacy for them in the sense that they will obtain the comparable pain relief from Maxigesic as they have obtained or would obtain from codeine. In my view, that representation falls short of representation (h) which includes a representation of superior efficacy.
107 I do not accept that any of the Maxigesic advertisements conveys representation (i) in the absence of any reference to benefits of either product apart from “pain relief”. As reflected in Mr McMaugh’s evidence, the language of the “same benefits” has a degree of specificity that is not conveyed by the more general language of the advertisements.
Conclusions as to representations made
108 Taking into account issues of dosing and the generality with which the pleaded representations are expressed, in my view, the relevant representations made by the Maxigesic advertisements are as follows:
(1) Maxigesic provides stronger and more effective relief from all pain than Nuromol when taken at their respective maximum recommended daily doses (print advertisement and card)).
(2) When taken at their respective maximum recommended daily doses, Maxigesic provides stronger and more effective relief from pain than any other paracetamol/ibuprofen combination (print advertisement and card));=.
(3) When taken at their respective maximum recommended daily doses, Maxigesic provides stronger and more effective relief from pain than OTC doses of either paracetamol or ibuprofen alone (all Maxigesic advertisements)).
(4) Maxigesic reduces pain by at least 32% more than a full daily OTC dose of either paracetamol or ibuprofen alone throughout the period of administration of either drug (print advertisement and pamphlet)).
Alleged implied representations
109 Each of the Maxigesic advertisements conveys the representation that the representations conveyed by the advertisement are grounded in scientific fact. That representation is made variously by the fact that the representations are statements in the realm of science, by the references to the Merry study and the Mehlisch No. 1 study, the use of percentages and, in the case of the pamphlet, the use of charts. Thus, I accept that in relation to each of representations (1) to (4) above, there is a further representation that there is a current adequate foundation in scientific knowledge for that misrepresentation.
110 In relation to representations (3) and (4), there is a representation that the representation is supported by the Merry study and the Mehlisch No. 1 study. That representation is conveyed by the use of a footnote referring to those studies adjacent to the words which convey representations (3) and (4).
111 I do not accept that, in relation to representations (1) and (2), there is a representation that the representation is supported by the Merry study and the Mehlisch No. 1 study because the words conveying those representations are not linked to the footnotes in which the Merry study and the Mehlisch No. 1 study are mentioned.
Foundation for superiority claims over Nuromol/any other paracetamol/ibuprofen combination (representations (1) and (2))
Reckitt’s case
112 To prove the absence of an adequate scientific foundation for the claims of Maxigesic’s superiority over other combination analgesics, Reckitt relied on the following matters:
(1) The absence of a clinical study that supports any representation of comparative superiority of Maxigesic over Nuromol either after single or multiple dosing.
(2) The absence of any meta-analysis that compares the efficacy of Maxigesic and Nuromol.
(3) The absence of any clinical study or meta-analysis that compares combination formulations of doses of ibuprofen and paracetamol in the quantities present in the commercial formulations of Maxigesic and Nuromol (at any dose).
(4) The existence of only a single study to show any significant difference between 500mg paracetamol/200mg ibuprofen and 1000mg paracetamol/400mg ibuprofen, being the Mehlisch No. 1 study, which showed a difference only between 4 to 8 hours (single dose). That significance of that study is affected by the subsequent full study (Mehlisch No. 2 study), which found no statistically significant difference between 500mg paracetamol/200mg ibuprofen compared to 1000mg paracetamol/400mg ibuprofen as a single dose.
(5) The Mehlisch No. 2 study and the Doherty study which, Reckitt submitted, permit no inference to be drawn as to the superiority of Maxigesic over Nuromol.
(6) The relevant available meta-analyses (the Moore review and the Derry review), which disclose that there is no significant difference in efficacy between 500mg paracetamol/200mg ibuprofen and 1000mg paracetamol/400mg ibuprofen. Accordingly, Reckitt argued, no inference can possibly be drawn that two tablets of Maxigesic would be superior to one tablet of Nuromol.
113 Matters (1) to (3) are not disputed. Matters (4) to (6) are addressed below.
AFT’s case
114 AFT argued that the absence of a scientific study of the relative efficacy of Maxigesic and another combination analgesic does not demonstrate the falsity of the representations in the face of the following matters:
The dosing regimen for Maxigesic was approved by the Therapeutic Goods Administration (“TGA”) at the maximum approved daily dose for paracetamol and ibuprofen as monotherapies. It is inherently improbable that the TGA approved a higher dosing regimen for Maxigesic than other paracetamol/ibuprofen combinations if the higher dosing regimen has no additional effect.
Reckitt has sought and obtained regulatory approval in other countries for a dosing regimen of Nuromol at twice the approved levels in Australia. Further, its recommended single dose for Nurofen (ibuprofen) in Australia is 400mg. Reckitt’s own conduct is entirely inconsistent with the position it advances in this case. In effect, it admits the absurdity of that case.
Reckitt’s evidence does not establish a ceiling in the effectiveness of paracetamol and ibuprofen at the dosage of Nuromol (i.e., 500mg paracetamol/200mg ibuprofen single dose and 1500mg paracetamol/600mg ibuprofen daily dose).
There is adequate scientific evidence for the following propositions:
(a) A combination of 1000mg paracetamol/400mg ibuprofen is a more effective dose than 500mg paracetamol/200mg ibuprofen.
(b) A dose of 1000mg of paracetamol is more effective than a dose of 500mg of paracetamol.
(c) A dose of 400mg of ibuprofen is more effective than lower doses of ibuprofen.
Scientific studies
115 The following studies were relied upon by the parties in support of their respective cases. I have considered them broadly in reverse chronological order, from most recent to oldest.
Daniels study (2011)
116 The Daniels study assessed the efficacy of single doses of 1000mg paracetamol/400mg ibuprofen and 500mg paracetamol/200mg ibuprofen against 400mg ibuprofen/25.6mg codeine, 1000mg paracetamol/30mg codeine and placebo in a dental pain model of removal of at least three impacted teeth.
117 Under the heading “Discussion”, the authors concluded:
In conclusion, 1 or 2 tablets of a single-tablet combination of ibuprofen 200mg/paracetamol 500mg provided highly effective analgesia that was comparable with, or superior to, other combination analgesics marketed for strong pain. Paracetamol combined with ibuprofen, at the dose range studied, is a more effective analgesic than codeine combined with ibuprofen. The novel single-tablet combination of ibuprofen/paracetamol would provide a useful alternative analgesic option for people not wishing to take codeine.
118 As AFT contended, the Daniels Study concluded that:
(1) 1000mg paracetamol/400mg ibuprofen was significantly more efficacious than 500mg paracetamol/200mg ibuprofen. The precise finding was that “[t]wo tablets of the single-tablet combination of ibuprofen 200mg/paracetamol 500mg were statistically significantly more efficacious than 1 tablet of the single-tablet combination”.
(2) “The pain relief scores over time curves … illustrate that the peak pain relief was higher and sustained for longer with 2 tablets of the single tablet combination of ibuprofen/paracetamol compared with all other treatments”.
119 Reckitt contended that the Daniels study made no comparative finding as to a statistically significant difference between 500mg paracetamol/200mg ibuprofen and 1000mg paracetamol/400mg ibuprofen over a single 8 hour dose. Under the heading “primary efficacy endpoint’, the authors states:
The results of all 5 planned primary comparisons were positive for both 1 and 2 tablets of the single-tablet combination of ibuprofen 200mg/paracetamol 500mg compared with the other treatments.
120 However, the statements identified by AFT do appear to me to be comparative findings. There is also a finding that “2 tablets of the single-tablet combination of ibuprofen 200mg/paracetamol 500mg provided significantly more pain relief than 1 tablet from 5 hours onwards”.
121 Thus, in my view, the Daniels study provides scientific evidence that a combination of 1000mg paracetamol/400mg ibuprofen is a more effective dose than 500mg paracetamol/200mg ibuprofen. It does not provide scientific evidence that a combination of 1000mg paracetamol/300mg ibuprofen (that is, a combination containing less ibuprofen) is a more effective dose than 500mg paracetamol/200mg ibuprofen, because it did not test that comparison.
Doherty study (2011)
122 The Doherty study examined the efficacy of three daily doses of 400mg ibuprofen, 1000mg paracetamol, 500mg paracetamol/200mg ibuprofen and 1000mg paracetamol/400mg ibuprofen in treating knee pain over both a 10 day and a 13 week period. The study used a range of metrics including a visual-analogue pain scale, an arthritis pain scale and a patient assessment.
123 The relevant conclusion stated in the abstract was:
Ibuprofen/paracetamol combination analgesia, at non-prescription doses, confers modest short-term benefits for knee pain/osteoarthritis.
124 Reckitt noted that the Doherty study, on a multi dose, multi day trial, found that 1000mg paracetamol/400mg ibuprofen was not statistically significantly more effective than 500mg paracetamol/200mg ibuprofen.
125 AFT contended that the Doherty Study found that:
(1) 1000mg paracetamol/400mg ibuprofen was more effective than 500mg paracetamol/200mg ibuprofen but that comparison was “just shy” of statistical significance;
(2) patient assessments rated the 1000mg paracetamol/400mg ibuprofen dose higher on every metric than the 500mg paracetamol/200mg ibuprofen dose;
(3) 1000mg paracetamol/400mg ibuprofen is more effective than 1000mg paracetamol, while 500mg paracetamol/200mg ibuprofen is not; and
(4) 1000mg paracetamol/400mg ibuprofen was associated with a higher rate of adverse events, including haemoglobin loss likely as a result of gastrointestinal bleeding.
126 AFT argued that, in considering whether conduct is misleading or deceptive or likely to mislead or deceive, it is inappropriate to disregard findings on the basis that they lack statistical significance. Rather, the Court should consider the results identified by AFT as supportive of the superiority of 1000mg paracetamol/400mg ibuprofen over 500mg paracetamol/200mg ibuprofen, and as counting against a conclusion that Reckitt has discharged its burden of proof. In support of this argument, AFT relied on the evidence of Professor Rolan, a pain management physician, that the Doherty study’s conclusions are consistent with 1000mg paracetamol/400mg ibuprofen being more effective than 500mg paracetamol/200mg ibuprofen. Professor Rolan also stated that the Doherty study provides further support for his view that there is no plateau effect at 500mg paracetamol/200mg ibuprofen and therefore that Maxigesic is likely more effective than Nuromol at maximum doses.
127 I accept Reckitt’s contention that the Doherty study provides scientific evidence that a combination of 1000mg paracetamol/400mg ibuprofen is not a more effective dose than 500mg paracetamol/200mg ibuprofen where the difference in efficacy of those doses was found not to be of statistical significance. On the other hand, I also accept AFT’s contention that the Doherty study provides scientific evidence of the superiority of 1000mg paracetamol/400mg ibuprofen over 500mg paracetamol/200mg ibuprofen, albeit evidence lacking statistical significance. As with the Daniels study, the results of the Doherty study do not address the comparative efficacy of 1000mg paracetamol/300mg ibuprofen and 500mg paracetamol/200mg ibuprofen.
Mehlisch No. 1 study (2010)
128 The Mehlisch No. 1 study compared the pain relief provided to patients undergoing the removal of three to four impacted molars by a single dose of paracetamol (1000mg and 500mg), a single dose of ibuprofen (400mg and 200mg) and combinations of the two monotherapies (1000mg paracetamol/400mg ibuprofen and 500mg paracetamol/200mg ibuprofen).
129 The authors noted:
One of the main objectives of this proof-of concept study was to test the hypothesis that combination therapy with ibuprofen and paracetamol would be more effective than either agent alone when used at their maximum licensed over-the-counter doses, as stipulated by regulatory authorities in the United States.
130 The authors also referred to the study as a “pilot study”. There were 234 patients in the intent-to-treat population.
131 The authors noted that “doses of ibuprofen and paracetamol were selected to be at or near their analgesic ceiling in relation to their respective dose-response curves”.
132 The study’s conclusions included that:
(1) 1000mg paracetamol/400mg ibuprofen provided significantly better mean pain relief than 500mg paracetamol/200mg ibuprofen, with the authors noting that “[a] dose-response effect for SPRID8 [Sum of Pain Relief and pain Intensity Differences from base line (0 hour) to 8 hours after dosing] was observed with combination therapy;
(2) ibuprofen 400mg/paracetamol 1000mg was ~30% more effective than ibuprofen 200mg/paracetamol 500mg”;
(3) 1000mg paracetamol/400mg ibuprofen provided a higher peak mean pain relief score than 500mg paracetamol/200mg ibuprofen, which was significant at 4 hours;“[at] most time points, patients in the ibuprofen 400mg/paracetamol 1000mg group achieved significantly better mean PID [Pain Intensity Difference] scores than ibuprofen alone, paracetamol alone, and ibuprofen 200mg/paracetamol 500mg”; and
(4) 1000mg paracetamol/400mg ibuprofen provided superior pain relief to 400mg ibuprofen whereas 500mg paracetamol/200mg ibuprofen did not.
133 Reckitt noted that 1000mg paracetamol/400mg ibuprofen was found to be no different in efficacy between zero and four hours, compared to the 200mg/500mg combination. Accordingly, Reckitt submitted, there was no better pain relief, at all, over that four hours, between 500mg paracetamol/200mg ibuprofen and 1000mg paracetamol/400mg ibuprofen. As such, Reckitt argued, the Mehlisch No. 1 study provides no basis for any comparison between Maxigesic and any other combination analgesic and furthermore provides no basis for any assertion of superiority of Maxigesic (single dose duration six hours) over one tablet of Nuromol (single dose duration eight hours) in circumstances where there was no difference in efficacy between 500mg paracetamol/200mg ibuprofen and 1000mg paracetamol/400mg ibuprofen over the first four hours.
134 Accepting Reckitt’s qualifications set out above, the Mehlisch No. 1 study provides scientific evidence that a combination of 1000mg paracetamol/400mg ibuprofen is a more effective dose than 500mg paracetamol/200mg ibuprofen.
Mehlisch No. 2 study (2010)
135 The Mehlisch No. 2 study was two stage clinical trial that was designed to confirm and extend the findings of the Mehlisch No. 1 study and to generate data for regulatory purposes. A total of 735 patients were randomly assigned in stage one and 715 entered and 678 completed stage two.
136 The report of the study described its objectives as follows:
This study was a 2-stage clinical trial that was designed to confirm and extend the findings of the earlier study in the same dental plain model and to generate data for regulatory purposes. The objective of stage 1 was to compare the efficacy and tolerability of 3 doses of a single-tablet fixed-dose combination (FDC) of ibuprofen and paracetamol (ibuprofen 100 mg/paracetamol 250 mg, ibuprofen 200 mg/paracetamol 500 mg, and ibuprofen 400 mg/paracetamol 10000 mg) with comparable doses of ibuprofen monotherapy, paracetamol monotherapy, and placebo. In addition, and from a clinical dosing standpoint, it was of interest to compare results for the FDC ibuprofen 200 mg/paracetamol 500 mg with ibuprofen 400 mg alone and paracetamol 1000 mg alone. The objective of stage 2 was to compare the efficacy and tolerability of the same 3 doses of the FDC with each other and with placebo over the 72 hour postoperative period following stage 1.
137 The stated conclusion of the report was:
FDC ibuprofen 200 mg/paracetamol 500 mg and ibuprofen 400 mg/paracetamol 1000 mg were significantly more effective in this population than were comparable doses of ibuprofen or paracetamol alone in moderate to severe acute dental pain and were significantly more effective than placebo in providing sustained pain relief.
138 The Mehlisch No. 2 study (a) did not find a statistically significant difference between 1000mg paracetamol/400mg ibuprofen and 500mg paracetamol/200mg ibuprofen, and (b) found that 1000mg paracetamol/400mg ibuprofen was superior to 400mg ibuprofen but that 500mg paracetamol/200mg ibuprofen was not.
139 AFT noted the following observations of the report’s authors:
The dental pain model is widely used to evaluate the efficacy of analgesic agents such as NSAIDs [Nonsteroidal Anti-inflammatory Drugs] and paracetamol … The dental pain model has a proven record of assay sensitivity in separating active drugs from each other and from placebo and has the potential to demonstrate additional pain relief with combination therapy (ie, upside model sensitivity).
140 Professor Rolan gave the following affidavit evidence concerning the Mehlisch No. 2 study:
While the Mehlisch Study No 2 did not find the 1000 mg paracetamol/400 mg ibuprofen to be more effective than the 500 mg paracetamol/200 mg ibuprofen dose, I do not consider that this single study conclusively determines that there is a plateau at 500 mg paracetamol/200 mg ibuprofen. It is common in clinical research for trials comparing treatments not to produce the same result. Whether a difference exists between treatments needs to be determined on the overall balance of trials, hence the value of meta-analysis. There is substantial scientific evidence to the contrary as identified in my first affidavit and in this affidavit.
141 Having regard to Professor Rolan’s evidence, the Mehlisch No. 2 study is:
(1) scientific evidence that a combination of 1000mg paracetamol/400mg ibuprofen is not a more effective dose than 500mg paracetamol/200mg ibuprofen; and
(2) scientific evidence of a ceiling in the effectiveness of paracetamol and ibuprofen at the dosage of Nuromol (i.e., 500mg paracetamol/200mg ibuprofen single dose).
Steiner study (2003)
142 The Steiner study compared the pain relief provided to sufferers of tension type headache by a single dose of 500mg and 1000mg of aspirin or paracetamol or a placebo.
143 The Steiner study found that:
(1) Patients who took 1000 mg of paracetamol experienced statistically significant pain relief two hours after dosing compared to those who took a placebo, whereas those patients who took a 500mg dose did not record statistically significant pain relief compared to those who took a placebo. This was reported by the authors of the study as “evidence of a dose-response relationship”.
(2) 1000mg paracetamol achieved statistically significantly superior results for pain intensity scores and pain intensity differences when compared to placebo, while 500mg paracetamol did not.
144 Reckitt did not dispute that the Steiner study provides scientific evidence that a dose of 1000mg paracetamol is more effective than a dose of 500mg paracetamol.
145 Under the heading “Efficacy”, the authors of the study noted:
Most analyses for efficacy were made over the first 4h. Because rescue medication was allowed from 2h onwards, no inferences were drawn for time points beyond this.
Schou study (1998)
146 The Schou study compared the pain relief provided by a single dose of 50mg, 100mg, 200mg or 400mg of ibuprofen to patients having an impacted molar removed.
147 The study’s abstract states relevantly:
A positive analgesic dose-response relationship of 50-mg, 100-mg, 200-mg and 400-mg doses of ibuprofen was observed when evaluated by pain intensity difference, sum of pain intensity difference, pain relief, total pain relief and survival distribution of patients not taking rescue medication. Although significant pain relief was seen after a dose of 50 mg ibuprofen, ibuprofen 400mg provided maximum pain relief and the longest duration of analgesic effect.
148 Under the heading “Discussion”, the authors stated, relevantly:
Although low doses of ibuprofen seem to provide analgesic after surgical removal of third molars in many patients, the apparently rapid need for remedication and the limited analgesic effect indicate that the use of ibuprofen in low doses cannot be advocated for controlling pain after surgical removal of third molars or other types of minor surgery. The 400-mg dose of ibuprofen would be preferable due to its higher and longer duration of analgesic effect.
149 The Schou study concluded that:
… evaluation by SPID [Sum of Pain Intensity Difference], TOTPAR [Total Pain Relief] and survival distribution of patients not taking rescue medication demonstrated a positive analgesic dose-response relationship of 50-mg, 100-mg, 200-mg, and 400-mg doses of ibuprofen in this study.
Cochrane reviews
150 Cochrane reviews are systematic reviews of primary research in health care and health policy. Cochrane is well regarded as one of the “gold standards” that is used for the translation of clinical practice in trials for evidence-based health care resources.
151 Cochrane reviews are meta-analyses. They compare results from multiple clinical trials and may increase power in statistics and results of the individual clinical trials. Professor Rolan accepted that Cochrane reviews are independent, high quality reliable sources of information comparing treatments.
Moore review (2015)
152 The Moore review examined the results of Cochrane reviews looking at the efficacy of different oral analgesics in the treatment of acute postoperative pain. The authors concluded:
There is a wealth of reliable evidence on the analgesic efficacy of single dose oral analgesics. Fast acting formulations and fixed dose combinations of analgesics can produce good and often long-lasting analgesia at relatively low doses.
153 Reckitt submitted that the Moore review found that 1000mg paracetamol/400mg ibuprofen and 500mg paracetamol/200mg ibuprofen had almost the same NNT (1.5 versus 1.6) and “their confidence intervals nearly completely overlapped so that they did not significantly differ (or really differ at all in reality) – which evidences that their efficacy is not different – that is, they have the same efficacy on that metric, noting that is the usual metric for Cochrane meta-analysis and the only metric consistently used in all Cochrane reviews before the Court”.
154 Reckitt also contended that the Moore review provided:
(a) Evidence of a ceiling at or around one tablet of Nuromol as the NNTs are not significantly improving for the double dose of Nuromol.
(b) Evidence of no significant difference in the NNT of 3.5 of paracetamol compared to 3.6 for 975 to 100mg of paracetamol, that is, no difference in efficacy on the NNT metric between 500mg and 1000mg paracetamol.
(c) No basis for any inference of superiority of a larger dose of the combination analgesic or the monotherapy of paracetamol.
155 AFT contended that the Moore review noted that:
(a) Single doses of 1000mg paracetamol/400mg ibuprofen have a slightly better NNT and longer duration of effect than single doses of 500mg paracetamol/200mg ibuprofen.
(b) 60mg of codeine was a relatively ineffective analgesic: “NNTs varied from as low as 1.5 for the combination of ibuprofen 400mg plus paracetamol 1000mg to as high as 12 for codeine 60mg”.
(c) Dose responses of analgesics have “been shown in more detailed direct comparison of doses across a range of analgesics in acute postoperative pain”.
156 As to (c), the relevant passage of the Moore review states:
One further point is that of dose-response. In these studies there may be examples where higher doses do not show greater effect. For example, ibuprofen acid 600mg had a point estimate NNT of 2.7 while for 400mg it was 2.5. The reason may be in case mix … Dose response has been shown in more detailed direct comparison of doses across a range of analgesics in acute postoperative pain (McQuay 2007).
157 Accepting Professor Rolan’s evidence concerning the limitations of the NNT metric, the Moore review forms part of the body of scientific knowledge concerning paracetamol/ibuprofen analgesics and is inconclusive as to whether 1000mg paracetamol/400mg ibuprofen is more efficacious than 500mg paracetamol/200mg ibuprofen.
Rabbie review (2013)
158 The Rabbie review examined the results of studies assessing the efficacy of 200mg and 400mg doses (amongst others) of ibuprofen in the treatment of migraine.
159 The Rabbie review concluded that “NNTs for all efficacy outcomes were better with 400mg than 200mg in comparisons with placebo”. The “NNT”, or number needed to treat, is the number of patients one needs to treat to prevent one additional bad outcome. The authors concluded relevantly:
Ibuprofen is an effective treatment for acute migraine headaches in adults at doses of 200mg and 400mg, providing complete headache relief within two hours to 1 in 5 and 1 in 4 individuals taking those doses, respectively;…the 400mg dose was numerically superior to 200mg for all efficacy outcomes, but achieved statistical significance only for headache relief at two hours….Ibuprofen 400mg would seem to be a good first-line therapy for acute migraine headaches in this population.
160 Reckitt did not dispute that the Rabbie review provides scientific evidence that 400mg of ibuprofen is more effective than 200mg of ibuprofen.
Derry review (2013)
161 The Derry review was a meta-analysis conducted to assess analgesic efficacy of ibuprofen in single oral doses for moderate and severe post-operative pain in adults.
162 The Derry review found that there was no significant difference in the NNT of 2.7 for 200mg of ibuprofen compared to the NNT of 2.5 for 400mg of ibuprofen.
163 Professor Rolan discounted the significance of the review, saying:
It measured one insensitive metric, and this is a common problem with meta-analysis, is they have to find the lowest common denominator across a whole range of studies. So it did aim to look at the efficacy, but it used a metric that – that take – that took a sophisticated response into either a yes or no.
… And hence it is insensitive.
164 Reckitt contended that the Derry review evidenced no difference in efficacy on the NNT metric between 200mg and 400mg ibuprofen, and provides no basis for an inference of superiority of a larger dose of the monotherapy of ibuprofen.
165 AFT submitted that the Derry review concluded there was a trend (not at the level of significance) to increasing efficacy over the range of 100mg to 400mg doses. For dental studies the dose response was more marked and with a significant difference between 200mg and 400mg ibuprofen, although with limited data. The authors of the review acknowledged that the review was an “indirect” measure of dose response, and concluded that 400mg ibuprofen had a longer duration than 200mg.
166 Again accepting Professor Rolan’s evidence on this point, the review forms part of the body of scientific knowledge concerning the efficacy of ibuprofen, and is inconclusive as to whether 400mg ibuprofen is more effective than 200mg ibuprofen.
Toms review (2008)
167 The Toms review was a meta-analysis conducted to assess the efficacy of single dose paracetamol for the treatment of acute post-operative pain.
168 The Toms review found that there was no significant difference in the NNT of 3.5 for 500mg of paracetamol compared to the NNT of 3.6 for 975 to 1000mg of paracetamol.
169 As AFT’s submissions put it, the Toms review did not find that there was a difference between doses of paracetamol but stated that “[d]ose response may be more sensitively determined using trials that directly compare two doses, as has been done for paracetamol 100mg compared with 500mg”.
TGA approved dosing regimen for Maxigesic
170 There is no dispute that the standard Maxigesic single dose of 1000mg paracetamol/300mg ibuprofen was approved by the TGA. There was also no dispute that TGA would not have approved Maxigesic unless it was effective and safe when used in accordance with AFT’s recommended maximum daily dose.
171 AFT submitted that the gravamen of Reckitt’s position is that the standard single and daily doses approved by the TGA offers no benefit over the lower dose approved for other paracetamol/ ibuprofen combinations such as Nuromol. In effect, AFT argued, Reckitt asserts that the TGA has approved a therapeutically inefficacious dosing regimen for AFT. Having regard to the rigour involved in obtaining TGA approval, AFT contended, Reckitt’s position is inherently improbable.
172 In support of this argument, AFT referred to s 25 of the Therapeutic Goods Act 1989 (Cth) (“TG Act”) which provides relevantly that the process of evaluation of goods for registration must have regard to whether the quality, safety and efficacy of the goods for the purposes for which they are to be used have been satisfactorily established.
173 In effect, AFT’s submission asked the Court to assume that the TGA’s approval of Maxigesic is based on matters including an adequate scientific foundation for the representations. As a matter of common sense, it seems plausible that the TGA’s approval of Maxigesic may have involved an acceptance of scientific evidence of the comparative efficacy of dosing regimens of paracetamol/ibuprofen. However, AFT agrees that there is no clinical study of the kind that Reckitt contends is necessary to justify the relevant representations. Further, AFT could readily have adduced any scientific evidence provided to, or procured by, the TGA which provides an adequate scientific foundation for the representations. In the absence of such evidence, or evidence of TGA’s processes of evaluation of Maxigesic and Nuromol or other paracetamol/ibuprofen combinations, and despite Professor Rolan’s opinion to the contrary, I do not accept that the TGA approval provides an answer, whether alone or in combination with other matters, to Reckitt’s case that there is no adequate scientific foundation for the representations in the absence of evidence of the scientific foundation for the approval.
Reckitt’s dosing regimen for Nuromol in other countries and Nurofen in Australia
174 Reckitt did not dispute that it has obtained approval for and markets Nuromol in other countries for a single dose of 1000mg paracetamol/400mg ibuprofen (that is, twice its Australian approved dose).
175 Further, in Australia the standard single dose of Nurofen is 400mg of ibuprofen.
176 AFT argued that Reckitt’s case is incompatible with its own conduct overseas, and its recommended doses of Nurofen. Professor Rolan gave evidence that these matters were relevant to his opinion that 1000mg paracetamol/400mg ibuprofen is likely to be more effective than 500mg paracetamol/200mg ibuprofen (or at least his disagreement that the former is no more effective than the latter).
177 AFT relied on the following passage of Professor Rolan’s evidence, in his first affidavit:
… I do not agree that 400mg ibuprofen/1000mg paracetamol is no more effective than 200mg ibuprofen/500mg paracetamol …
[R]egulatory bodies around the world have accepted the claims that a 400mg dose of ibuprofen provides meaningfully better pain relief than a 200mg dose of ibuprofen … The Applicant’s Nurofen tablets contain 200mg of ibuprofen, and the Applicant’s product information recommends consumers take one or two tablet doses to obtain pain relief.
178 In his second affidavit, Professor Rolan made the following further observations on this subject:
In my first affidavit I explained that regulatory bodies around the world accept the proposition that there is not a ceiling on the effectiveness of ibuprofen at 200mg. I note further that countries including Singapore and New Zealand have approved the sale of a two tablet dose of Nuromol. The suggestion that there is a ceiling at 500mg paracetamol/200mg ibuprofen is inconsistent with the Applicant’s international approach to the marketing and regulatory approval of Nuromol.
179 However, putting aside the scientific studies considered above, AFT did not identify the scientific foundation for the conduct of Reckitt that is said to be incompatible. As explained above, in my view, Reckitt’s dosing regimens for Nuromol overseas and Nurofen elsewhere could only justify the representations to the extent of the scientific foundation for those dosing regimens.
180 In particular, I do not accept that facts concerning overseas regulatory approval demonstrate the superiority of a higher dose paracetamol/ibuprofen combination over a lower dose of the same combination in the absence of evidence that the relative benefits of the different doses are the subject of scientific evidence that was accepted by the regulatory authorities as a part of those processes.
181 Therefore, I do not accept that Reckitt’s other dosing regimens assist AFT in the absence of evidence of the scientific foundation for those dosing regimens.
Analgesic ceiling
182 The authors of the Mehlisch No. 1 study referred to a “ceiling effect” observed for non-opioid analgesics, whereby increases in drug dosage produce little or no increase in analgesic benefit but increase the risk of adverse effects. They raise the prospect that:
[c]ombining 2 or more drugs with different mechanisms of action, such as NSAIDS and paracetamol, may enhance analgesic efficacy without increasing adverse effects.
183 The significance of the existence or otherwise of a relevant analgesic ceiling is that it affects the extent to which extrapolations can be made from studies comparing different doses of paracetamol and ibuprofen.
184 AFT contended that Reckitt’s case appeared to rest on establishing that there is a ceiling at the level of the Nuromol dosing regimen, that is, at a single dose of 200mg of ibuprofen and 500mg of paracetamol (and a daily dose of 600mg of ibuprofen and 1500mg of paracetamol). I did not understand Reckitt to contend that it was necessary for it to establish such a ceiling in order to discharge its onus, although it did contend that the evidence supports the existence of a relevant ceiling.
185 Reckitt contended that the following matters do establish a ceiling:
(1) The experts agreed that “there are insufficient data to determine whether Nuromol and Maxigesic have different maximal effect after single dose”.
(2) The only two clinical studies to assess multiple doses of a paracetamol/ibuprofen combination were the Mehlisch No. 2 study and the Doherty study. Both of these studies found that there was no difference in efficacy between 500mg paracetamol/200mg ibuprofen and 1000mg paracetamol/400mg ibuprofen over multiple doses. Accordingly, Reckitt argued, no possible inference could be drawn from these studies that Maxigesic (having less APIs than two tablets of Nuromol) could be stronger or longer lasting than one tablet of Nuromol over multiple doses.
(3) Professor Rolan accepted that the Mehlisch No. 2 study shows that there is no significant statistical difference in efficacy in Nuromol for the eight-hour period between 500mg paracetamol/200mg ibuprofen and 1000mg paracetamol/400mg ibuprofen.
(4) The meta-analysis points to there being no difference between 500mg paracetamol/200mg ibuprofen and 1000mg paracetamol/400mg ibuprofen. The available Cochrane reviews provide no basis for any inference that Maxigesic is superior to Nuromol.
186 AFT contended that Professor Christie’s evidence in cross-examination demonstrated that the ceiling contended for by Reckitt does not sit at the dosing levels of Nuromol. Professor Christie’s evidence was that there is a well-known plateau effect when treating pain with ibuprofen “at or extremely close to 200mg”. Professor Christie explained that this plateau is not inconsistent with the prescription of ibuprofen at higher doses to treat an inflammatory condition, giving the following evidence:
Q. But are you saying to her Honour that, in your opinion, the ceiling for ibuprofen, as a monotherapy taken alone, is 200 milligrams?
A. Is close to. It might be a little bit higher, and it’s certainly higher for some pain types, but if you go to the meta-analyses of all post-surgical pain types, for example, I think – I would like to go to those, if you wish – then, if it’s not a ceiling, it’s very close to it.
Q. Are you differentiating between a plateau effect for treating the inflammation and a plateau effect for treating pain?
A. I am distinguishing that, yes.
187 Professor Christie said that in some pain models, particularly dental pain, 400mg ibuprofen is more effective than 200mg. He agreed that, subject to any ceiling, an increase in the amount of API will produce stronger or better pain relief.
188 Concerning analgesic ceilings, in his first affidavit, Professor Rolan said:
First, Professor Christie provides no studies in support of his proposition that the plateau effect is likely to be visible at doses of 200 mg of ibuprofen. … the [Mehlisch No. 1 study] at page 1 notes that “the group treated with ibuprofen 400 mg/paracetamol 1000 mg had significantly better mean [pain] scores compared with … ibuprofen 200 mg/paracetamol 500 mg”, and that the “group taking ibuprofen 200 mg/paracetamol 500 mg achieved significantly better mean SPRID8 scores than paracetamol alone (P=0.03), but not ibuprofen alone”. … 400 mg of ibuprofen has been demonstrated to be superior to 200 mg of ibuprofen in the management of acute migraine in [the Rabbie Review].
189 In my view, the observation that Professor Christie had provided no relevant studies was something of a debating point. It was not suggested to Professor Christie in cross-examination that there were no such studies. The Mehlisch No. 2 study and the Doherty studies are relevant studies in support of the proposition.
190 On the other hand, Reckitt did not dispute that the Mehlisch No. 1 study and the Rabbie review are scientific evidence that there is no analgesic ceiling at 200mg ibuprofen. The Schou study also observed a positive analgesic dose-response relationship for 200mg and 400mg doses of ibuprofen.
191 In his second affidavit, Professor Rolan added relevantly:
… I am of the view that a single dose of two tablets of Maxigesic is very likely to provide larger reductions in pain than a one tablet dose of Nuromol. This is because:
(a) a dose of 1000 mg paracetamol has been demonstrated to be more effective than a dose of 500 mg paracetamol;
(b) there is a dose-response relationship for ibuprofen over the dose range 100-800 mg; and
(c) these dose-response relationships remain present when ibuprofen and paracetamol are given in combination, as a dose of 1000 mg paracetamol/400 mg ibuprofen has been demonstrated to be more effective than a dose of 500 mg paracetamol/200 mg ibuprofen.
[T]he limited data concerning the dose response of paracetamol/ibuprofen combinations on balance favours a finding that a 100mg of paracetamol/400mg ibuprofen dose provides superior analgesia over a 500mg paracetamol/200mg ibuprofen dose – specifically the Mehlisch Study, the Doherty Study and the Daniels Study (the latter of which explicitly noted that the two tablet dose of Nuromol provided a higher peak pain relief score) …
At paragraph 32 of the Second Christie Affidavit, Professor Christie states “I also deny that there is strong evidence that the 500 mg paracetamol/200 mg ibuprofen does not produce a plateau response”. I disagree. Two of the studies which examined Nuromol, the Mehlisch Study and the Daniels Study, considered that the 1000 mg paracetamol/400 mg ibuprofen dose was superior to the 500 mg paracetamol/200 mg ibuprofen dose, with the Daniels Study explicitly referring to the higher peak pain relief provided by the higher dose (and the Doherty Study implicitly supports these results).
Against these studies, and the numerous authorities dealing with the individual dose responses of the monotherapies, Professor Christie resorts to the Mehlisch Study No 2 and to Cochrane Reviews (which for the reasons set out in my first affidavit and in this affidavit are inappropriate sources to use to disprove a dose response relationship). I do not consider this sufficient evidence to establish a ceiling effect at 500 mg paracetamol or 200 mg ibuprofen (whether alone or in combination).
192 In my view, the evidence reveals that there is an unresolved question in the science as to the existence or otherwise of a relevant analgesic ceiling. I accept AFT’s submission that Reckitt has not established a ceiling for the analgesic effect of ibuprofen in combination with paracetamol at 500mg paracetamol/200mg ibuprofen. On the other hand, AFT has not established that there is no relevant ceiling.
Scientific evidence comparing other dosing regimens
193 AFT argued that the scientific evidence before the Court is sufficient to establish the following propositions:
(1) There is adequate scientific support for the proposition that a combination of 1000mg paracetamol/400mg ibuprofen is a more effective dose than 500mg paracetamol/200mg ibuprofen (the Mehlisch No. 1 study and the Daniels study). The outcome of the Moore review and the Doherty study are also consistent with this proposition.
(2) It can be accepted that the Mehlisch No. 2 study did not achieve the same results as the Mehlisch No. 1 study or the Daniels study. However, this does not advance Reckitt’s position in any meaningful way. No criticism is made by either party of the conduct of the Mehlisch No. 1 study or the Daniels study. They are both, notably, studies sponsored by Reckitt – it would be most surprising if Reckitt were heard to dismiss the validity of this study and the reliability of the results it achieved. They provide an adequate scientific foundation for the outcomes they report and that are not negated by the outcome of the Mehlisch No. 2 study.
(3) There is adequate scientific support for the proposition that a dose of 1000mg of paracetamol is more effective than a dose of 500mg of paracetamol (the Steiner study).
(4) There is adequate scientific support for the proposition that a dose of 400mg of ibuprofen is more effective than lower doses of ibuprofen (the Schou study and the Rabbie review).
194 AFT argued that it is appropriate to extrapolate from these propositions to conclude that Reckitt has not demonstrated the falsity of the relevant representations, based on the expert evidence of Professor Rolan, and contrary to the expert evidence of Professor Christie.
195 As to (1), I accept that the Mehlisch No. 1 study and the Daniels study provide scientific support for the proposition that a combination of 1000mg paracetamol/400mg ibuprofen is a more effective dose than 500mg paracetamol/200mg ibuprofen. I also accept that the Doherty study provides some scientific support for the proposition, although not to the level of statistical significance. Similarly, the Moore review offers slight scientific support for the proposition.
196 As to (2), the Mehlisch No. 2 study did not achieve the same results as the Mehlisch No. 1 study or the Daniels study. They provide an adequate scientific foundation for the outcomes they report. However, in considering whether they provide an adequate scientific foundation for the representations, it is not appropriate to ignore the Mehlisch No. 2 study. That study casts doubt on whether the Mehlisch No. 1 study and the Daniels study provide an adequate scientific foundation for the representations because it provides evidence that there is no statistically significant difference between 500mg paracetamol/200mg ibuprofen and 1000mg paracetamol/400mg ibuprofen. To that extent, the Mehlisch No. 2 study does advance Reckitt’s case.
197 As to (3), the Steiner study provides scientific support for the proposition that a dose of 1000mg of paracetamol is more effective than a dose of 500mg of paracetamol. Reckitt did not identify scientific evidence to counter the Steiner study.
198 As to (4), the Schou study and the Rabbie review provide scientific support for the proposition that a dose of 400mg of ibuprofen is more effective than lower doses of ibuprofen.
Other evidence
199 AFT argued that Professor Rolan’s opinion that a single dose of two tablets of Maxigesic is very likely to provide larger reductions in pain than 500mg paracetamol/200mg ibuprofen was not shaken in cross-examination, and was not directly challenged at all.
200 AFT contended that Professor Rolan’s evidence was based on an overview of the available scientific learning. In contrast, AFT argued that Reckitt’s “selective, but heavy, reliance on the findings of Cochrane reviews is of limited assistance”. The Cochrane reviews were said to be “insensitive and not as useful as the results of individual studies which use finer, and more specific, metrics”.
201 AFT also noted the following evidence given by Professor Christie:
Q. Now, in the absence of there being a ceiling at 200 ibuprofen, 500 paracetamol, you accept, don’t you, that you don’t need a head to head comparison; you agree with that?
A. If there were the absence of a ceiling between testing 200 ibuprofen and 500 paracetamol versus 400 ibuprofen, 1000 paracetamol, there would not need to be a head to head comparison between those two doses. If the consensus of evidence was that they’re really not any different, then testing – you could actually make a reasonable inference that any dose in between is not any better. You could also make the reasonable inferences that if you generally did find a ceiling with that combination of 200 – could I just say 200 versus 400?
Q. Yes?
A. The 200 versus 400 combination. If you did find reasonable evidence that there is a ceiling, then you would also make the – you could also make the inference, not yet tested, but you would make the inference that using an even higher dose wouldn’t make any difference.
Consideration and conclusion
202 Professor Christie and Professor Rolan have offered competing scientific opinions relevant to whether there is an adequate foundation in science for representations (1) and (3). It is not necessary to decide which of these opinions is more persuasive, because the issue for determination is whether there is an adequate scientific foundation for the relevant representations of fact.
203 On the evidence above, I am satisfied that there is not an adequate scientific foundation for the representations for the following reasons:
(1) There is no clinical study or meta-analysis which supports the representations by a trial of the comparative pain relief provided by Maxigesic and Nuromol or comparable doses of paracetamol/ibuprofen combinations.
(2) The experts agreed that “there are insufficient data to determine whether Nuromol and Maxigesic have different maximal effect after single dose”.
(3) Although there is evidence that 400mg ibuprofen is more effective than 200mg ibuprofen (Mehlisch No. 1 study, Moore review and Rabbie review), the totality of the scientific evidence concerning the absence of a relevant analgesic ceiling is not so conclusive that the relevant body of scientific knowledge can be taken to include the absence of such a ceiling. Accordingly, I am not persuaded that there is an adequate scientific foundation for the representations based on extrapolation from the studies relied upon by AFT.
(4) In particular, the Mehlisch No. 2 study is a significant part of the body of scientific knowledge concerning the truth or otherwise of the representations. That study, albeit involving a comparison of 1000mg paracetamol/400mg ibuprofen and 500mg paracetamol/200mg ibuprofen doses, tends to suggest that the representations may be false.
(5) The Moore and Derry reviews also cast doubt on the truthfulness of the representations, because they indicate that the science is inconclusive as to the whether 1000mg paracetamol/400mg ibuprofen is more efficacious than 500mg paracetamol/200mg ibuprofen; and whether 400mg ibuprofen is more efficacious than 200mg ibuprofen.
(6) I do not accept that the Mehlisch No. 1 study provides an adequate foundation for the representations in the light of the Mehlisch No. 2 study, and the Moore and Derry reviews.
(7) Contrary to the opinion of Professor Rolan, I do not accept that significant weight can be placed on overseas regulatory approvals in the absence of evidence about the basis for those approvals.
204 Accordingly, I conclude by publishing the Maxigesic print advertisement and the Maxigesic card, AFT made representations (1) and (2) which were misleading or deceptive, or likely to mislead or deceive in contravention of s 18 of the ACL. I also conclude that those representations were misleading representations that the Maxigesic goods were of a particular quality, namely, able to provide the stronger and more effective pain relief referred to in the representations, in contravention of s 29(1)(a) of the ACL. I similarly conclude that the representations were made in contravention of s 29(1)(g) of the ACL because they were misleading representations that the Maxigesic goods had the performance characteristics of providing stronger and more effective pain relief referred to in the representations. In the absence of an adequate scientific foundation, I also conclude that, by making the representations, AFT engaged in conduct that was liable to mislead the public as to the characteristics of the Maxigesic goods, in contravention of s 33 of the ACL.
205 Further I conclude that, by publishing the Maxigesic print advertisement and the Maxigesic card, AFT also engaged in conduct that was misleading or deceptive, or likely to mislead or deceive in contravention of s 18 of the ACL by making the further false representations that there was a current adequate foundation in scientific knowledge for representations (1) and (2).
Foundation for superiority claims over monotherapies (representations (3) and (4))
206 Reckitt argued that no study other than the Merry study has analysed the efficacy of Maxigesic. Accordingly, on Reckitt’s case, there is no support for representations (3) and (4) other than from the Merry study.
207 In relation to representation (4), Reckitt argued that Mehlisch No. 1 study does not provide an adequate foundation in scientific knowledge for that representation because it did not involve an analysis of Maxigesic in any dose.
208 Reckitt then contended that, in the light of its unreliability, the Merry study cannot provide an adequate foundation in scientific knowledge for any representations or statement as to the efficacy of Maxigesic.
209 AFT accepted that Reckitt’s case concerning the comparative efficacy of Maxigesic with ibuprofen and paracetamol as monotherapies turns on the validity and reliability of the Merry Study, and in particular the use of rescue medication and the treatment of the resultant data. However, AFT contended that the weight of the evidence indicates that the use of rescue medication and the treatment of the resultant data in the Merry Study does not result in the Merry Study being invalid and unreliable. Particularly, AFT argued that, as the use of rescue medication was even across treatment groups, it did not distort the comparison of the relative effectiveness of the medicines under comparison.
210 AFT did not rely on the Mehlisch No. 1 study to support representations (3) or (4).
211 As to the expert evidence, AFT made the following contentions:
(1) The expert evidence of Professor Rolan and Dr Solterbeck, a biostatistician who was also called to give evidence by AFT, provides strong support for the validity of the Merry study.
(2) Ultimately, Professor Christie’s evidence was consistent with that of both Professor Rolan and Dr Solterbeck.
(3) Professor Keech, a professor of medicine, cardiology and epidemiology who was called by Reckitt, maintained his concerns about the Merry study but ultimately his evidence rises no higher than saying that further analysis should be done to verify the conclusions reached by the Merry study.
212 On this evidence, AFT argued, Reckitt did not discharge its onus.
Merry study
213 In the study, adults (more than 16 years) having one or more wisdom teeth removed under general or local anaesthesia were instructed to take two tablets before operation, then two tablets approximately every six hours for up to 48 hours of:
(1) a combination of paracetamol 500mg and ibuprofen 150mg per tablet (Maxigesic);
(2) paracetamol 500mg per tablet alone; or
(3) ibuprofen 150mg per tablet alone.
214 The stated conclusion in the abstract of the study is: “Maxigesic® tablets provide superior pain relief after oral surgery to [paracetamol] or ibuprofen alone”.
215 The experts agreed that this conclusion is incorrect because, without a baseline value, pain relief cannot be assessed. The experts agreed that the conclusion would be correct if the word “relief” were replaced with “reduction”.
Effect of rescue medication
216 The Merry study records:
If participants required additional postoperative relief while in hospital, a rescue dose of fentanyl 10 µg was given i.v. as required. After discharge to home, codeine was provided (again, as rescue medication) in 30 mg tablets, one to two to be taken as needed up to 4 hourly.
217 Rescue medication is a medicine used to relieve an acute exacerbation of a condition, such as pain. There was no dispute that rescue medication is a necessary part of any clinical trial relating to pain. The issue was how to use data about pain perceptions which was, or which may have been, affected by the administration of rescue medication.
218 The main basis on which Reckitt disputed the validity of the Merry study was the inclusion of data from participants who used rescue medication in the analysis. In the Merry study, over a 48 hour period, 62% of patients using paracetamol, 58% of patients using ibuprofen and 56% using Maxigesic had used rescue medication.
219 Reckitt identified the following four reasons for focussing on this issue:
(1) In their joint report, the experts agreed that table 4 (entitled “Rescue analgesia by group”) of the Merry study does not provide sufficient information to comfortably conclude the use of rescue medication was the same across treatment groups.
(2) While table 24 (entitled “Summary of dose consumption of rescue analgesia dose during the study”) of the Merry study report (also referred to as the clinical study report) suggests that the Maxigesic group did not use more rescue medication, it is readily apparent from that table that Maxigesic did not perform statistically significantly better than both monotherapies over all periods of the study as concerns the use of rescue medication, as Professor Keech acknowledged. Noting that the majority of patients required rescue medication, Professor Keech observed:
And one might even venture to say that the main finding of this study was that none of the three treatment arms being evaluated turned out to control the pain sufficiently in the majority of patients.
(3) In their joint report, the experts agreed that a high percentage of patients used rescue medication and that “[u]sing the data for codeine in Prof Keech’s affidavit (which are not quite complete), the number of patients using codeine across the entire 48 hours is similar on all three treatments”.
(4) The experts also agreed “that the VAS [visual analogue scale] scores collected soon after rescue are likely to mainly reflect pain perceptions after taking fentanyl or codeine rather than reflecting primarily the study medications”.
220 Despite agreeing on the facts above, in the joint report the experts recorded that they had disagreed on the impact of the high use of rescue medication on the interpretation of the Merry study results.
221 Reckitt contended that the Court should find that the results of the Merry study are unreliable due to contamination by rescue medication for the following reasons:
(1) There is a high percentage of patients using rescue medication;
(2) The rate of use of codeine was also high.
(3) In cross-examination, Professor Rolan wrongly opined that the frequency of use of codeine was low. In re-examination, Professor Rolan described the use of fentanyl as “relatively low” and the use of codeine as “moderate”, but did not explain this change in view.
(4) Professor Rolan suggested that codeine was not a relatively strong analgesic but, as Professor Keech said in reference to the use of codeine-based medications as post-discharge “rescue medication” in during the Merry Study:
[T]he reason it’s called rescue medication is because it’s more powerful than the treatments that are being tested, and it’s deployed when patients are not having satisfactory pain control.
As Professor Keech also said:
[O]nce the patients start rescue therapy and their analgesic strategy has failed, their pain scores are unlikely to reflect the analgesic strategy that they are randomised to, and instead reflect the use of fentanyl or codeine, in this instance, predominantly. And that is part of the agreed wording of the expert report from all four experts.
Expert evidence
Professor Christie
222 Professor Christie accepted that, when assessing relative effectiveness, rescue medication is less of a problem than where the question is the magnitude of a medication’s effect. In the Merry study, the question was the relative efficacy of the relevant treatments.
Professor Rolan
223 In his first affidavit, Professor Rolan expressed the opinion that the designers of the Merry study had adopted “unusual techniques for a study in relation to an analgesic” but that, nevertheless, the conclusions reported in the study are valid.
224 One of the design features that Professor Rolan identified as of concern was that there was no explanation of whether the pain scores of those participants receiving rescue medication were “adjusted” to exclude the effect of that rescue medication. Professor Rolan noted that “if the score are not adjusted, then the reduction in pain reported by participants will be in part due to the rescue medication but will be incorrectly attributed to the experimental medication”. Professor Rolan concluded relevantly:
Whilst a significant percentage of participants in the Merry study required rescue medication, I do not consider this to bias the results reported in the study. This is because the rate of use of rescue medication is either slightly higher or the same in the individual monotherapy groups when compared to the combination therapy group. The only effect that this could have on a conclusion as to the efficacy of the combination therapy would be to understate that efficacy. This is because participants receiving the monotherapy who also receive rescue medication will receive more pain relief. This would mean that their pain scores would be lower than without the rescue medication, which means the extent of the reduction of pain provided by the combination therapy is harder to detect.
225 In his second affidavit, Professor Rolan expressed the view that the analysis of data after use of rescue medication is entirely appropriate and is consistent with the intention-to-treat (“ITT”) analysis which is the preferred approach to be taken for analgesic studies.
226 I did not understand Professor Rolan to express an opinion to the effect that the Merry study supports representation (4).
227 Professor Rolan explained that, in clinical practice, a whole range of information is used to make a conclusion as to the likely efficacy of a higher dosage of a medication, starting with the premise that a higher dose product is likely to have some greater efficacy or greater duration.
228 In cross-examination, consistent with his first affidavit, Professor Rolan agreed that it is clearly desirable to strip out or take account of any rescue medication that has been taken by the study participants to ensure that the study is accurately recording the effects of the drugs that are being tested. However, Professor Rolan said, there is no agreed way to do that.
229 Professor Rolan also gave the following evidence:
And you would accept that more than half of the data is likely to reflect the pain perceived on the rescue therapy – ie, codeine or fentanyl – with or without simultaneous – the study medications? No. I do not, as they are short-acting medications, and certainly codeine is a relatively inefficacious medication in this condition, and there’s – so with short duration, relatively low efficacy and with most patients, I think, only using – the majority of people using rescue have only used a single dose of treatment in a – quite a long observation. I think the confounding effect of rescue medication is minor.
230 When Professor Rolan was challenged that he could not say that people using codeine only took one dose in 24 hours, Professor Rolan maintained that his recollection was that the number of doses was low. This evidence was surprising for two reasons:
(1) it seemed to make a counter-intuitive suggestion that one of the chosen rescue medications was relatively inefficacious; and
(2) the basis for the proposition that the majority of patients who used rescue medication used only a single dose of treatment was not clear.
231 However, as to (1), Professor Rolan’s evidence as to the relative inefficacy of codeine was perhaps later corroborated by Dr Foltyn, who said that 60 milligrams of codeine was required for “decent” pain relief from dental pain.
232 As to (2), I accept Reckitt’s submission that Professor Rolan was incorrect in his recollection as to the incidence of use of codeine in the Merry study. In cross-examination, Dr Solterbeck agreed that an Excel spreadsheet prepared by Professor Keech showed a high rate of use of codeine, as high as eight 30 milligram tablets within the first 24 hour period in some patients.
233 In re-examination, Professor Rolan himself suggested that his recollection of “one dose on average” was in reference to fentanyl (another opioid), rather than codeine. Professor Rolan nevertheless maintained that the use of codeine was “modest”.
234 Ultimately, Professor Rolan maintained that the frequency of use of rescue was comparable across the treatment groups with the exception that, in the first 24 hours, the use of codeine by the Maxigesic group was statistically significantly less than that in the paracetamol group. Professor Rolan stated that this reinforced the robustness of the study rather than detracting from it. Professor Rolan further explained his conclusion that the Merry study’s use of data affected by rescue medication was valid as follows:
There are a number of statistical techniques which try to separate out the effect of rescue from the underlying drug effect. They all have statistical assumptions and there’s extensive debate by regulators and statisticians on what’s – on what’s – what can be done. You can, for example, take a window around the time of the dosing. You say a person had a dose of codeine at 8 o’clock. What I will do for the – I think codeine probably works about four hours, therefore I will just draw a horizontal line across the pain scores over that four hour period and it’s called last observation carried forward. It’s probably wrong, but it’s probably less wrong than taking the patient entirely out of the study. There are other methods, which actually make an estimate of what that pain score can be using the model average. So these are quite sophisticated statistical techniques and I’m fairly confident saying there is not universal agreement on what can be done and probably the individual methods don’t matter enormously. But even leaving the data in is not necessarily a confounder, provided that the frequency of rescue is comparable between the treatment arms. And that’s because it’s relatively easy to demonstrate that if you add an effective treatment on top of other treatments, all that will do is aim – will have an effect on reducing the difference between treatments, not increasing it. And therefore any bias that occurs as a result of leaving rescue in is against finding superiority of a higher treatment, not in favour of it, unless the extraordinary unlikely effect that there was more use of rescue in the patients who had a more effective treatment.
Dr Solterbeck
235 Dr Solterbeck expressed the view that the results reported in the Merry study support the statement that Maxigesic reduces pain by 32% compared to paracetamol and ibuprofen alone. Dr Solterbeck also considered that the Merry study is sufficiently robust to provide a proper basis for this claim.
236 In her report entitled “Analysis of the Merry Study”, Dr Solterbeck also expressed reservations concerning the manner in which the Merry study dealt with rescue medication. Specifically, Dr Solterbeck said:
39 However, some factors which are important to the conduct of pain studies have not been fully explained in the Merry Study. The use of rescue medication is one such factor. Ideally, the patient would be asked to rate their pain and then take the rescue medication.
40 This approach is noted in section IVB1a of the FDA Draft Guidance:
“For example, pain can be assessed just before the administration of rescue medication and these data carried over to the next scheduled assessment time.”
41 In this scenario all pain assessments are included in the analysis. Furthermore, section IVB3a the FDA Draft Guidance around rescue medication in repeat dosing studies notes:
“To avoid interference in efficacy measures at scheduled times because of the use of rescue medication, sponsors can make pain assessments before rescue, asking subjects to report the pain intensity at the current time with no recall period, and imputed to the following scheduled assessment time. The primary efficacy endpoint can be based on a time-weighted analysis over the trial period.”
42 Other commonly used approaches are to ignore all assessments made after the use of rescue medication, or to “impute” a value. One possible method of imputation is to use the last pain score recorded before the use of rescue medication as the pain score for all assessments after the use of rescue medication. This is referred to as the “last observation carried forward” approach.
43 Finally, there are methods to analyse pain and rescue together.
44 The Merry Study does not fully explain which approach was taken for assessments made by patients who required rescue medication. Based on Figure 1 and Table 2 in the Merry Study, it is apparent that all patients were included in the analysis (as the number of patients noted to contribute to the results in Table 2 is the same as the number noted to be included in the study in Figure 1). It is not known whether results recorded after use of rescue are included in the analysis.
45 It would help to know the number of patients with data at each time point presented in Figure 3. This would provide some assurance of the robustness of the results (as if few patients provide data at the later time points this would affect the interpretation), and would provide a way to ascertain whether results after rescue were dropped.
46 It is of note from Table 4 that more than half the patients took rescue medication at some stage in the study.
47 I believe the Merry Study used all pain assessments recorded (with or without rescue). This follows the Intent-To-Treat principle (ITT) (an analysis which includes every subject that is randomised and is intended to receive treatment) as required for assessment of superiority.
48 Given there is little difference (according to Table 4 of the Merry Study) in the use of rescue medication I do not consider that inclusion of pain scores after rescue medication undermines the validity of the study.
237 Concerning the claim of a 32% greater reduction in pain by Maxigesic compared with ibuprofen or paracetamol alone, Dr Solterbeck said:
56 From table 2 we have the following results (at rest).
Acetaminophen | Ibuprofen | Combination | A-C | 1-C | Percentage C vs A | Percentage C vs I |
33 | 34.8 | 22.3 | 10.7 | 12.5 | 32.42% | 35.92% |
57 Therefore, at rest, the claim is consistent with the results of the study.
58 As the study was conducted in an acceptable manner, I am confident that the study may be relied upon to substantiate the finding.
59 For completeness, I note that there is a reference in the abstract of the Merry Study to “pain relief”. I consider that, as there is no baseline pain measurement in the Merry Study, the term pain “relief” is inappropriate, as this term has a technical meaning in the field of clinical trials which measure pain. For the Merry Study to draw a conclusion regarding pain “relief”, it would need to have included either a specific question relating to pain relief, or measured a pain intensity difference from baseline, both of which would need the patient to be experiencing pain prior to starting study treatment. However, I consider that the Merry Study does show that Maxigesic provides a larger reduction in pain intensity as set out in its conclusions.
238 In her report entitled “Review of affidavit of Professor Christie sworn 20 October 2017”, Dr Solterbeck said, relevantly:
47 At paragraph 98, Professor Christie states that patients who required rescue analgesia “should have been deemed a treatment failure and excluded from the study altogether” with the result that their data would not be analysed. I disagree.
48 The appropriate method for dealing with patients in clinical analgesic trials who require additional analgesia is a contentious issue, and is the subject of considerable discussion in the present statistical literature. The ICH is currently preparing an addendum to the E9 Guidelines, the Addendum on Estimands and Sensitivity Analysis in Clinical Trials to the Guideline on Statistical Principles for Clinical Trials (ICH E9 R1).
49 The approach which Professor Christie suggests (excluding all data from patients who require rescue analgesia) introduces an unacceptable risk of bias into a study. This is because it would exclude all patients who require additional analgesia from the study, leaving only those patients for whom the relevant treatments were a success. Consider the use of a placebo – under Professor Christie’s approach, all those patients for whom the placebo was ineffective would be excluded, leaving the appearance of a potentially very effective placebo.
50 The ICH E9 Guidelines state that in superiority trials the appropriate approach to analysing a study’s data set is the “intention to treat (ITT) or “full analysis set (FAS) approach, as it “avoids over-optimistic estimates of efficacy” (page 24). ICH E9 R1 expressly notes (page 7) that it may be appropriate to include results observed after a patient has taken rescue medication. The ITT approach involves analysing all data recorded by patients participating in the trial, regardless of whether these patients complete the trial or experience unusual events. In this way, the ITT approach more closely mirrors the range of events that may happen in the “real world”, and a treatment that is shown to be superior by this approach is likely to demonstrate this result when applied more generally to patients.
51 Indeed, this approach is usually regarded as conservative, as it tends to under-rate the efficacy of the treatment being examined. In this way, it introduces minimal bias into the reported results. This is because patients on the less effective treatment (in this case, reasonably predicted to be paracetamol and ibuprofen) will have greater recourse to rescue medication, and accordingly will experience greater reductions in pain levels than they otherwise would, which will under-estimate the efficacy of the more effective treatment. I note that in the Merry Study potentially more patients in the monotherapy arms required rescue medication than patients in the combination arm (as set out in Table 4), however we can only fully assess the impact of rescue medication if we know the amount of rescue medication taken as well as the number of patients (as only the number of patients is reported In Table 4).
52 The decision in the Merry Study to include results from those patients requiring rescue medication is therefore an acceptable approach.
239 In a report entitled “Review of affidavit of Professor Christie sworn 21 November 2017, at paras 8 to 16, Dr Solterbeck expressed additional views concerning the recording of results after use of rescue medication. In particular, Dr S Solterbeck stated:
(1) The Merry study adopted her preferred approach for dealing with data after the use of rescue medication.
(2) Where all data from patients has been included in the primary analysis, the data concerning the use of rescue medication provides a useful insight into the efficacy of the treatments.
(3) All available data suggests that the use of rescue medication did not bias the results of the Merry study.
240 In re-examination, Dr Solterbeck gave the following evidence:
A. … [W]e’re doing an ITT analysis, as I’ve just described. The ITT analysis is about what answers did I get for the patients, irrespective of whether they took the study medication and, here, whether they took rescue medication. And the things that make me comfortable about that is I don’t just take that on face value, I actually went and looked and asked myself the question is there similar usage of rescue medication across the three groups? Because if there was a lot more use in the Maxigesic group, for argument’s sake, then there would be an issue. But, here, there is similar usage across the three groups, so, therefore, that’s not introducing any particular bias in the answer that I’m getting. I also went and asked, okay, how much information do I have to get the AUC – area under the curve? Because, for some patients, I only had a few pain scores recorded over a short timeframe, and for others I had much more. Then, again, that might be introducing a bias that I’m not comfortable with, so I asked for the data, and that was this data sheet that I’ve just been taken through and looking at the various patients. And on the basis of looking at that data sheet, I, then, was quite comfortable that for most patients, actually, they had done a good job of recording their pain, and there was, certainly, no difference between the three different groups about how many scores went into the AUC and the timeframe over which those values were recorded. So given those two pieces of information, I am comfortable that the study is robust and that, within that study, I can say that Maxigesic was superior to the individual components.
Q. It was put to you, Dr Solterbeck, that the results of the Merry study were unreliable because the high use of rescue medication had contaminated the study; do you recall ---?
A. I do recall that.
Q. You said you disagreed; that’s right, isn’t it?
A. That’s correct.
Q. Can you please explain, as briefly as you can, why you disagree?
A. Yes. All right. So the reason why I disagree – because the use of rescue medication was similar across the three groups, we’ve not introduced any bias in answering the question “was Maxigesic better than ibuprofen or paracetamol alone?” If I wanted to get a pure answer of exactly what could Maxigesic do with nothing else happening for the patient, then I don’t get that answer, but that’s not the question that has been asked. What they’re looking for here is how effective is Maxigesic as a treatment policy – as a strategy – compared with a strategy with paracetamol alone or a strategy with ibuprofen alone, and so given that that’s the question that they asked, accepting that, in clinical practice, patients aren’t perfect and they are going to need to go and do other things, they’re not going to take the doses exactly every six hours but, every way that we’ve looked at these data, we’re not introducing any bias because the use of rescue was similar, so I feel “contamination” is not necessarily the right word. It’s not – we’re not getting the pure answer exactly – what are these treatments doing for pain – but that’s not what we want to know. We want to know, in this treatment policy, is Maxigesic better and the study is telling us, yes, it is.
Q. And this treatment policy which includes the taking of rescue medication as required?
A. That’s correct.
(emphasis added)
241 In my view, this evidence is inconsistent with a conclusion that the Merry study provides a scientific foundation for representation (4), because that representation is not qualified by reference to the treatment policy applied in the Merry study. Accordingly, I understood this evidence to have qualified the evidence that Dr Solterbeck had earlier given, referred to at [237] above.
Professor Keech
242 Professor Keech was highly critical of the Merry study, describing it as “fundamentally compromised”. Professor Keech’s opinion was that its results were unreliable “given the high incidence of rescue medication and the failure to separate the data from patients after requiring rescue medication from their prior data and those who did not require rescue medication”.
243 AFT argued that the following matters demonstrates an “important limitation” on the usefulness of Professor Keech’s evidence:
(1) He was not instructed to consider the validity and reliability of the Merry study itself. Rather, he was instructed to review and comment on Dr Solterbeck’s report on the Merry study.
(2) Professor Keech only received the Merry clinical study report as part of the conclave process.
(3) The form of Professor Keech’s instructions is “puzzling. The part of Dr Solterbeck’s evidence which Professor Keech was asked to consider did not touch on the Merry clinical study report, the Merry Results Summary or the Merry Statistical Analysis Plan. Those documents are the subject of another part of Dr Solterbesck’s evidence.” Professor Keech did not read the Merry clinical study report as part of the process of preparing his affidavit and he was not instructed to review the Merry clinical study report.
(4) Consequently, Professor Keech’s affidavit was prepared primarily on the basis of his review of the published report of the Merry study.
244 AFT criticised the following opinion of Professor Keech, given in oral evidence:
The comparison that has been made in this statistical analysis is no longer a comparison of the three treatments. It’s a comparison of the three treatments muddied heavily by the use of fentanyl and codeine, and so I would suggest to you that, in fact, one can’t really interpret the results as being reliable evidence of the superiority of one of the trial medications over the others. Now, it doesn’t mean that it couldn’t be real – a real benefit of the combination therapy – but to confirm that that was real, you would need to do a time-adjusted analysis of the data excluding the data beyond the use of rescue therapy.
245 AFT argued that this passage reveals a significant problem, namely, that Professor Keech’s evidence raises no more than doubts about the validity and reliability of the Merry study.
246 For example, AFT noted Professor Keech’s evidence that it would be necessary to obtain individual patient data “to really get to the bottom of the claims that are made in” the Merry study. Professor Keech continued:
A. One needs to see the impact of rescue medication and for how long it seemed to impact on individual patients to get some sense of – a better sense of how much it has contaminated the conclusion. And, as I said to you before, intention-to-treat analyses of this patient population in the Merry study could take one of two courses.
Q. Okay?
A. The analysis that has been done using all this stuff – I would call it “rubbish”, really – where pain scores are being measured whilst patients are taking fentanyl or codeine, or the other intention-to-treat analysis where, in fact, the data is truncated, or censored, as we use the term, at the point where the analgesic strategy, or policy, has failed, and rescue medication has ensued.
Q. And?
A. And that is the preferred method of analysis that we use in all other models with exactly the same sort of problem as I described with cancer therapy.
Q. Thank you, Professor Keech?
A. ---where the chemotherapy fails and one has to deploy an alternative therapy to save the patient’s life, we don’t use that and attribute it to the previous chemotherapy.
Q. And, as I understand, what you’re saying to her Honour is, if you had that extra information, you would then be able to form a view on whether or not one could rely on this study, or not?
A. Well, I would then be able to perform the analysis that I’ve described to you.
247 I did not understand this evidence to amount to a concession on Professor Keech’s part that the Merry study might be demonstrated to be reliable. I understood Professor Keech to be acknowledging that the data collected by the Merry study could be reviewed and, depending on its contents, analysed in a different way to see whether it supported the conclusion of the Merry study.
248 AFT also sought to rely on the following passage of cross-examination:
Q. Professor Keech, have you heard of the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use?
A. Yes.
Q. Now, they say, for example:
When specifying how to account for rescue medication as in intercurrent event, occurrence of the intercurrent event is ignored and the observations on the variable of interest are used. If applied across all types of intercurrent event, this reflects the comparison described in the ICH glossary as the effect of a treatment policy.
Q. Are you aware of that ---?
A. Yes.
Q. I mean, that ---guideline?
A. Yes. I – I’m familiar with that sort of determination.
Q. Yes?
A. The problem is, you – as I said to you before, you’ve got to decide what you’re actually – what your interpretation is that you can make on the data should you choose to go down that route.
249 I understood Professor Keech to be making the same point as Dr Solterbeck had in her re-examination, referred to above. That is, that the study may permit an interpretation about the efficacy of the treatment policies studied (in the case of the Merry study, the different medications plus certain rescue medication). Later, Professor Keech gave the following evidence to that effect:
If you’re doing an intention to treat analysis you include those patients. But, again, I – I point out to you that the issue is how do you interpret what you find in doing such an analysis. Are you drawing a conclusion that there’s a real difference between the study medications, or are you drawing – drawing a conclusion the difference could be due to rescue medications or other prohibited medication use?
250 Professor Keech did not agree with the evidence of Professor Christie, referred to at [222] above. In explanation, Professor Keech said:
My central tenet is … that once the patients start rescue therapy and their analgesic strategy has failed, their pain scores are unlikely to reflect the analgesic strategy that they are randomised to, and instead reflect the use of fentanyl or codeine, in this instance, predominantly. And that is part of the agreed wording of the expert report from all four experts.
251 I found Professor Keech’s evidence to be persuasively reasoned. In contrast, the criticisms sought to be made by AFT about the terms of his instructions and the circumstances in which he obtained the Merry clinical study report was unpersuasive: ultimately, they did not have any significant impact on Professor Keech’s opinion or reasoning. Similarly, I do not accept that the value of Professor Keech’s evidence is reduced because he is not a pain expert or because he has not been involved in the conduct of clinical trials in relation to analgesics of the type relevant to this dispute: neither of these matters detracts from the fundamental logic of his opinion, which was not effectively challenged.
Conclusion
252 Ultimately, I find the evidence of Professor Keech to be the most persuasive of the four experts, and I therefore prefer his evidence to the evidence of the others to the extent of any inconsistency.
253 In particular, to the extent that it was suggested by Professor Rolan (and perhaps Dr Solterbeck), I do not accept that the stated conclusion of the Merry study, which took account of data affected by the use of rescue medication, provides an adequate foundation for a similar conclusion in relation to the use of Maxigesic, paracetamol and ibuprofen in the relevant doses more generally and apart from the treatment policy of the Merry study.
254 Even if it could be accepted that the use of rescue medication was roughly the same across the different treatment groups, I accept Professor Keech’s opinion that there is insufficient evidence to justify an extrapolation to a conclusion about the relative efficacy of the three medicines in the relevant doses that ignores the use of the rescue medication in the study altogether.
255 In my view, this conclusion does not cast doubt on the publication of the study, which sets out clearly the relevant treatment policy.
256 However, I conclude that the Merry study does not provide an adequate foundation in scientific knowledge for either representation (3) or representation (4).
Other “confounds”
257 Reckitt argued that the following other matters render the conclusions of the Merry study unreliable:
(1) The use of pre-emptive analgesia. While it was agreed that this was not an issue for comparison of Maxigesic with the monotherapies alone in the study, it did mean that that there was no baseline value. As noted earlier, the experts agreed that, where there is no baseline value, “pain relief” cannot be assessed. Reckitt submitted that this constitutes an agreement between all four experts that the Merry study cannot be relied upon to support any representation of pain relief.
(2) The use of pre-emptive analgesia and the inclusion of data from participants who used rescue medication renders the magnitude of any outcome on the effect of pain relief meaningless. Again, the result is that “pain relief” cannot be assessed.
(3) The Merry study is “not sufficiently powered for the primary endpoint”.
(4) The Merry study was “underpowered to detect outcomes on any of the secondary endpoints”. Few of the tests were demonstrated to be significant. Only the AUC (area under the curve) measure, which is confounded by the use of rescue medication was consistently significant. Either there was little real effect or the Merry study was underpowered.
258 It is not necessary to address these issues, having regard to my conclusion above. However, as to (1) and (2), I again note the experts’ agreement that the conclusion in the abstract to the Merry study is incorrect.
Consideration and conclusion
259 I have concluded that the Merry study does not provide an adequate foundation in scientific knowledge for either representation (3) or representation (4).
260 It follows that there is no adequate foundation in scientific knowledge for those representations. Accordingly, I conclude that by publishing each of the Maxigesic advertisements, AFT made representation (3) which was misleading or deceptive, or likely to mislead or deceive in contravention of s 18 of the ACL.
261 I also conclude that representation (3) was a misleading representation that the Maxigesic goods were of a particular quality, namely, able to provide the stronger and more effective pain relief referred to in the representation, in contravention of s 29(1)(a) of the ACL. I similarly conclude that representation (3) was made in contravention of s 29(1)(g) of the ACL because it was a misleading representation that the Maxigesic goods had the performance characteristics of providing stronger and more effective pain relief referred to in representation (3). In the absence of an adequate scientific foundation, I also conclude that, by making representation (3), AFT engaged in conduct that was liable to mislead the public as to the characteristics of the Maxigesic goods, in contravention of s 33 of the ACL.
262 Further I conclude that, by publishing each of the Maxigesic advertisements, AFT also engaged in conduct that was misleading or deceptive, or likely to mislead or deceive in contravention of s 18 of the ACL by making the further false representations that there was a current adequate foundation in scientific knowledge for representation (3) and that representation (3) was supported by the Merry study and the Mehlisch No. 1 study.
263 I also conclude that by publishing the Maxigesic print advertisement and the Maxigesic pamphlet, AFT made representation (4) which was misleading or deceptive, or likely to mislead or deceive in contravention of s 18 of the ACL.
264 I also conclude that representation (4) was a misleading representation that the Maxigesic goods were of a particular quality, namely, able to provide the degree of pain relief referred to in the representation, in contravention of s 29(1)(a) of the ACL. I similarly conclude that representation (4) was made in contravention of s 29(1)(g) of the ACL because it was a misleading representation that the Maxigesic goods had the performance characteristics of providing the degree of pain relief referred to in the representation. In the absence of an adequate scientific foundation, I also conclude that, by making representation (4), AFT engaged in conduct that was liable to mislead the public as to the characteristics of the Maxigesic goods, in contravention of s 33 of the ACL.
265 Further I conclude that, by publishing the Maxigesic print advertisement and the Maxigesic pamphlet, AFT also engaged in conduct that was misleading or deceptive, or likely to mislead or deceive in contravention of s 18 of the ACL by making the further false representations that there was a current adequate foundation in scientific knowledge for representation (4) and that representation (4) was supported by the Merry study and the Mehlisch No. 1 study.
AFT’s case against Reckitt
266 AFT’s cross-claim against Reckitt relates to:
(1) Four print advertisements directed at pharmacists and pharmacy assistants, with the following titles:
(a) “Nuromol – Stronger for Longer than Paracetamol” (“Nuromol advertisement 1”);
(b) “Why take 2 when you can take 1?” (“Nuromol advertisement 2”);
(c) “Switch to hit pain” (“Nuromol advertisement 3”);
(d) “Nuromol provides up to 8 hours of relief from strong pain in a single tablet” (“Nuromol advertisement 4)
(together “Nuromol print advertisements”).
(2) Two television advertisements presenting case studies relating to the use of Nuromol (“Nuromol TV advertisements”);
(collectively “Nuromol advertisements”).
267 A case based on alleged representations made orally by Reckitt sales representatives to at least one pharmacist in relation to the dosing regimen for Nuromol was not pressed.
Nuromol print advertisements
Nuromol advertisement 1
268 Nuromol advertisement 1 contains the following statement:
Nuromol provides up to 8 hours of pain relief in a single tablet, while some other paracetamol/ibuprofen combinations like Maxigesic may require up to 2 tablets for optimal relief, and require 6 hourly dosing.1, 2, 4
269 Footnotes 1, 2 and 4 to Nuromol advertisement 1 state:
1. Mehlisch DR et al. Clin Ther 2010;32:1033-49 (RB sponsored).
2. Daniels SE et al. Pain 2011; 152:632-42 (RB sponsored).
…
4. Maxigesic Product Information.
270 The study referred to in the first footnote is the Mehlisch No. 2 study discussed above at [135] and following. The study referred to in the second footnote is the Daniels study discussed above at [116] and following.
Nuromol advertisement 2
271 Nuromol advertisement 2 contains the following statement:
WHY TAKE 2 WHEN YOU CAN TAKE 1?
Nuromol provides up to 8 HOURS OF STRONG RELIEF FROM PAIN in a single tablet1,2 VS Some other paracetamol/ibuprofen combinations, like Maxigesic®, may require up to 2 tablets 6 hourly dosing3
272 The footnotes to the statement say:
*Based on the recommended dose of Nuromol versus Maxigesic
1. Nuromol Product Information
2. Mehlisch DR et al. Clin Ther 2010;32:1033–49.
3. Maxigesic Product Information.
Nuromol advertisement 3
273 Nuromol advertisement 3 comprises the following advertisement:
Switch to hit pain
Nuromol is the alternative to codeine you’ve been waiting for. Clinical trials show Nuromol is 38% more effective, longer lasting, and better tolerated than paracetamol/codeine 1000/30mg.
Plus, Nuromol provides up to 8 hours of relief from strong pain in a single tablet, while other paracetamol/ibuprofen combinations, like Maxigesic, may require up to 2 tablets and 6-hourly dosing.
So make the switch to Nuromol – a clinically proven alternative to paracetamol/codeine for your customers needing relief from strong pain.
Nuromol advertisement 4
274 Nuromol advertisement 4 contains the following statement:
Nuromol provides up to 8 HOURS OF STRONG RELIEF FROM PAIN in a single tablet1,2 VS Some other paracetamol/ibuprofen combinations, like Maxigesic, may require up to 2 tablets 6 hourly dosing3
275 The footnotes to the statement say:
1. Nuromol Product Information
2. Mehlisch DR et al. Clin Ther 2010; 32:1033–49
3. Maxigesic Product Information
276 Nuromol print advertisement 1 was published in the Australian Journal of Pharmacy. Nuromol print advertisement 2 was published in Post Script, a trade publication directed at pharmacy assistants. Nuromol print advertisement 3 was published in the “Product News” section of the Australian Journal of Pharmacy. Nuromol print advertisement 4 was published in Retail Pharmacy. Accordingly, each of the Nuromol print advertisements is directed at a specialist audience (pharmacists or pharmacy assistants) who can be expected to understand the content of the Nuromol print advertisements in light of their professional qualifications and experience and trade knowledge.
Nuromol TV advertisements
277 The Nuromol TV advertisements are addressed to consumers at large and have been broadcast on national television networks, including Channel 9. There are two advertisements: one features “Trent” who was suffering from a toothache (“toothache advertisement”); the other features “Anthea” who suffers from back pain (“back pain advertisement”).
278 The toothache advertisement includes the following statement by “Trent”:
Paracetamol just didn’t work for my strong pain, so I was recommended Nuromol.
279 The back pain advertisement includes the following statement by “Anthea”:
For strong pain, paracetamol just didn’t last long enough for me, so I tried Nuromol.
280 Both advertisements display the following words on screen:
“Relief from strong pain* that lasts up to 8 hours”
*Daniels SE et al, Pain 2011 152: 632-42
281 Both advertisements display the following graphic material between the statements made by “Trent” and “Anthea”, respectively, and the display of the words set out immediately above: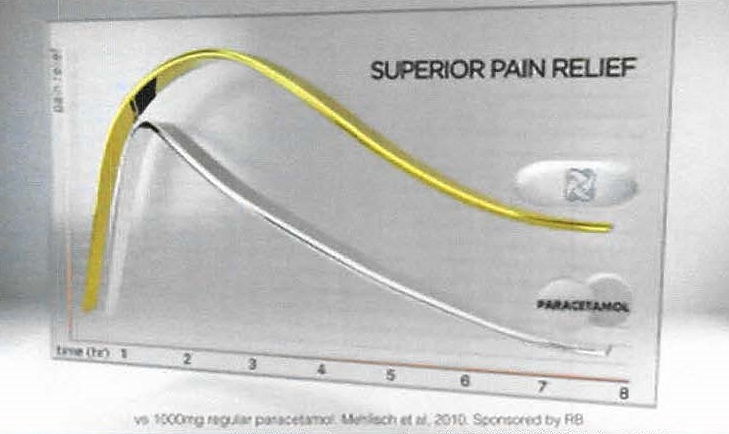
Issues for determination
282 AFT’s case can be considered under the following three headings:
(1) Complaints concerning comparisons of Nuromol and Maxigesic in the Nuromol print advertisements.
(2) Complaints concerning the allegedly represented dosing regimen for Nuromol in Nuromol print advertisement 1.
(3) Complaints concerning alleged representation in the Nuromol TV advertisements that Nuromol is listed on the Australian Register of Therapeutic Goods (“ARTG”) for the treatment of strong pain.
Comparisons of Nuromol and Maxigesic
283 AFT contends that Nuromol advertisement 1 conveys to pharmacists that:
(1) one tablet of Nuromol provides equivalent or superior pain relief to two tablets of Maxigesic; and
(2) over an 8-hour period, one tablet of Nuromol provides equivalent or superior pain relief to two tablets of Maxigesic.
284 Further, AFT alleges that the Nuromol advertisement 1 carries a representation that each of the representations above is supported by the Mehlisch No. 2 study or by the Daniels study.
285 Reckitt does not accept that its print advertisements convey the representations alleged by AFT. Reckitt contends that the Nuromol advertisements make statements of fact about the duration of pain relief and the number of tablets that may be taken of each of Nuromol and Maxigesic to obtain pain relief and the dosing times of each of the combination analgesics.
286 Further, Reckitt asserts that no claim of superiority is made in the advertisements and no comparison of efficacy is expressly made at all.
Nuromol dosing regimen
287 AFT contends that Nuromol advertisement 1 conveys the representation that Maxigesic requires 6-hourly dosing to provide pain relief.
288 Reckitt denied that the alleged representation is conveyed, and asserted that there is a factual basis for repetition of material from Maxigesic product information. For example, the dosage instructions on the Maxigesic box state relevantly:
Repeat dose every six hours as required, up to a maximum of 8 tablets every 24 hours.
Nuromol listing on ARTG
289 AFT alleges that the Nuromol TV advertisements falsely convey that Nuromol is listed on the ARTG for the treatment of strong pain.
290 Reckitt denies that this representation is conveyed by the advertisements. In addition, Reckitt admits that the ARTG does not presently indicate that Nuromol provides relief from strong pain but says that, at all material times, the TGA has accepted that a claim for the relief of strong pain can be made for Nuromol.
291 Accordingly, the following issues arise for determination on AFT’s cross-claim:
(1) whether Reckitt made any of the alleged representations by publishing or causing to be broadcast the Nuromol advertisements; and
(2) whether AFT has established that any of the representations made were false, misleading or deceptive, or likely to mislead or deceive.
Alleged Nuromol representations
292 The Nuromol print advertisement should also be understood by reference to its effect or likely effect on ordinary or reasonable members of the class of pharmacists and pharmacy assistants: see [22] above.
Comparisons of Nuromol and Maxigesic
293 Mr McMaugh gave evidence that Nuromol advertisement 1 conveys to him that one tablet of Nuromol (taken every 8 hours) provides pain relief which is at least as good as that provided by two tablets of Maxigesic (taken every 6 hours).
294 I do not accept Reckitt’s contention that no claim of superiority is made by the advertisements. In my view, a reasonable member of the relevant class of readers, being primarily pharmacists and pharmacy assistants, would understand the comparisons made between Nuromol and Maxigesic to convey a representation of Nuromol’s superiority. This representation is particularly made by the use of the word “while” in drawing the comparison between the products. In the context of the promotion of Nuromol, a reasonable reader would understand the drawing of the comparison “Nuromol x, while Maxigesic not x” to convey that Nuromol is superior to Maxigesic by reason of the fact that it has the characteristic “x”.
295 Thus, considering the Nuromol print advertisements by reference to position of an ordinary or reasonable member of the class of pharmacists and pharmacy assistants, I find that each of the four Nuromol print advertisements convey a representation that one tablet of Nuromol provides equivalent or superior pain relief to two tablets of Maxigesic (“Nuromol superiority representation”). This is because they suggest one tablet of Nuromol will provide up to eight hours of pain relief, while two tablets of Maxigesic may only provide up to six hours of pain relief. By making this comparison, the advertisements imply a comparison of products able to provide the same optimal pain relief. In the case of Nuromol advertisement 2, the implication that the compared products are able to provide the same optimal pain relief is reinforced by the line “Why take 2 when you can take 1”.
296 I am not satisfied that the Nuromol print advertisements convey a representation that over an 8-hour period, one tablet of Nuromol provides equivalent or superior pain relief to two tablets of Maxigesic. As I have said, the advertisements suggest that the products provide comparable pain relief. In my view, the references to “up to 8 hours of pain relief” for Nuromol and “6-hourly dosing” suggest that a more frequent dosing regime is required to achieve the same pain relief from Maxigesic as Nuromol. However, that suggestion is not a representation of equivalent or superior pain relief.
297 I also find that, in Nuromol advertisement 1, the footnoted references to the Mehlisch and Daniels studies at the end of the sentence ending “require 6-hourly dosing” convey the representation that the superiority representation is supported by those two studies.
Nuromol dosing regime
298 AFT relied on the statement set out at [268] above to support its claim as to the representation made by Nuromol advertisement 1.
299 I do not accept that the Nuromol advertisement 1 conveys the representation that Maxigesic requires 6 hourly dosing to provide pain relief. In my view, it conveys no more than that Maxigesic may require 6 hourly dosing to provide optimal pain relief, having regard to the reference to “optimal pain” relief in connection with the possible dose of up to two tablets. In my view, no reasonable consumer would read the advertisement to suggest that Maxigesic will provide no pain relief except with 6 hourly dosing (the logical obverse of the alleged representation) because the extent of the pain relief that may be experienced is not certain and the duration over which pain relief may be required will depend upon the circumstances of the individual consumer.
300 Accordingly, AFT’s case fails on this alleged representation.
Nuromol listing on ARTG
301 AFT relied on the evidence of Mr De Meyer, Reckitt’s Category Manager, Analgesics. Mr De Meyer agreed that the Nuromol TV advertisements suggest that Nuromol could be used to treat strong pain and that this was an important message in the advertisements. Mr De Meyer also accepted that consumers of OTC medicines would understand the Nuromol TV advertisements to represent that Nuromol is suitable for treating strong pain; that many consumers would be aware that the government plays a role in assessing whether medicines are suitable for the conditions for which they will be marketed; and some consumers might be aware that this regulatory role is performed by the TGA.
302 By reference to this evidence, AFT contended that many consumers viewing the Nuromol TV advertisements would understand that the government (and perhaps the TGA) had approved Nuromol for the treatment of strong pain.
303 AFT’s submissions also noted that the TG Act prohibits a person from advertising a therapeutic good for an indication where the therapeutic good is included in the ARTG, but not for the advertised indication. Consistent with this, Mr McMaugh’s evidence was that he expects a medicine advertised for a particular indication will have that indication on the ARTG.
304 I do not accept that the advertisements convey the alleged representation, in the absence of any reference to the ARTG or to regulatory or government approval and where I do not accept that a reasonable consumer would be likely to think that the government’s role includes assessing the suitability of a product for the treatment of “strong pain”. Professor Rolan’s evidence was that the expression “strong pain” is not one typically used by patients, who use a range of metaphors and adjectives to describe their pain including, for example, “terrible” and “incapacitating”. Accepting that the advertisements convey the suitability of Nuromol for the treatment of “strong pain”, in my view, the evidence does not suggest that the adjective “strong” as a descriptor of pain has a sufficiently clear meaning to convey that it is likely to be the subject of regulatory approval.
305 Accordingly, AFT’s case must also fail in relation to the Nuromol TV advertisements.
Foundation in science for Nuromol superiority representation
306 Reckitt made the following submissions concerning the foundations for the Nuromol print advertisements:
(1) The Daniels study provides an adequate foundation in scientific knowledge for a statement about Nuromol providing strong relief from pain or relief from strong pain.
(2) The Mehlisch No. 2 study found, amongst other matters, that the fixed-dose combination ibuprofen 200mg/paracetamol 500mg was significantly more effective than either drug alone in the treatment of moderate to severe acute dental pain in the immediate post-operative period. In terms of pain relief and intensity difference superiority of the fixed-dose combination ibuprofen 200mg/paracetamol 500mg versus placebo was significant at all time points; as against paracetamol 1000mg, one tablet of Nuromol was significant at 15 minutes and from 60 to 480 minutes; and versus ibuprofen 400mg it was significant at 15 to 120 minutes.
(3) The Mehlisch No. 2 study also finds that one tablet of Nuromol is not statistically significantly different in efficacy to two tablets of Nuromol. Hence there is an adequate foundation in science to state that Nuromol at one tablet is as efficacious as Maxigesic.
307 Even assuming in Reckitt’s favour that each of these propositions is true, none of them provides an adequate foundation for the Nuromol superiority representation, which is that one tablet of Nuromol provides equivalent or superior pain relief to two tablets of Maxigesic (“Nuromol superiority representation”). None of the studies is directed to a comparison of Nuromol and Maxigesic or the equivalent APIs.
308 Thus, Reckitt has not identified an adequate foundation in science for the Nuromol superiority representation and accordingly, I find that it is a misleading representation.
Conclusion
309 I will direct the parties file and serve short minutes of orders to give effect to these reasons and for the further conduct of the matter.
310 I note that, consistent with the order separating out the determination of all questions of whether there has been any contravention of the ACL in relation to the cross-claim, I have not made any contravention finding in relation to the Nuromol superiority representation. It will be necessary to make additional findings as to the character of the Nuromol superiority representation, in the event that AFT seeks findings that Reckitt has contravened any of ss 29(1)(a) and (g) and s 33 of the ACL.
I certify that the preceding three hundred and ten (310) numbered paragraphs are a true copy of the Reasons for Judgment herein of the Honourable Justice Gleeson. |
Associate:

