
FEDERAL COURT OF AUSTRALIA
Sevdalis v Director of Professional Services Review (No 2) [2016] FCA 433
VID 309 of 2015 | |
DATE OF ORDER: |
THE COURT ORDERS THAT:
1. The application for an extension of time to make an application under the Administrative Decisions (Judicial Review) Act 1977 (Cth) is granted.
2. The application for judicial review under sections 5 and 6 of the Administrative Decisions (Judicial Review) Act 1977 (Cth) is dismissed.
3. The application for judicial review under section 39B of the Judiciary Act 1903 (Cth) is dismissed.
4. The applicant pay the costs of the respondents.
Note: Entry of orders is dealt with in Rule 39.32 of the Federal Court Rules 2011.
MORTIMER J:
1 The applicant, Dr Sevdalis, is a medical practitioner who operates a general practice in Fairfield, Victoria. His medical practice is subject to the regulatory regime in the Health Insurance Act 1973 (Cth), which sets out a scheme for professional services review.
2 The second respondent, the Professional Services Review Committee No 855, is a reviewing authority established under the Act. By way of a report dated 18 November 2014, it found that the applicant had engaged in “inappropriate practice” within the meaning of s 82 of the Act. The inappropriate practice related primarily to his attendances on patients outside consulting rooms and his record-keeping of clinical records, including a finding that he had fabricated documents purporting to be contemporaneous clinical notes.
3 On 12 May 2015, the third respondent, the Determining Authority, decided to impose sanctions on the applicant under s 106U of the Act. The sanctions were serious, comprising directions that the applicant be reprimanded and counselled, that he be disqualified from receiving a medicare benefit for a period of two years, and that he repay medicare benefits in the amount of $453,656.75 to the Commonwealth.
4 No appeal lies to this Court from the findings of a Professional Services Review Committee or the determinations of the Determining Authority.
5 The applicant seeks judicial review under ss 5 and 6 of the Administrative Decisions (Judicial Review) Act 1977 (Cth) and s 39B of the Judiciary Act 1903 (Cth) in relation to the report and the determination. He seeks orders setting aside the decision and findings of the Committee and the decision and directions of the Determining Authority imposing sanctions. Alternatively, he seeks orders in the nature of certiorari quashing those decisions and in the nature of mandamus requiring each of the Committee and the Determining Authority to make a fresh decision in accordance with law.
6 For the reasons that follow, his application for judicial review must be dismissed.
BACKGROUND
An overview of the Professional Services Review Scheme
7 Part VAA of the Act makes detailed provision for the Professional Services Review Scheme. The Full Court in Kutlu v Director of Professional Services Review [2011] FCAFC 94; 197 FCR 177 had cause to consider the operation of the Scheme. At [7]-[13] Rares and Katzmann JJ set out an overview of the Scheme, which I respectfully adopt:
Part VAA of the Act provides for the Professional Services Review Scheme. The object of Part VAA is to protect the integrity of the Commonwealth medical and pharmaceutical benefits programs and in doing so to protect, first, patients and the community from risks associated with inappropriate practice (as defined in s 82) and secondly, the Commonwealth from having to meet the cost of services provided as a result of “inappropriate practice” (s 79A). The Part applies to a range of practitioners in professions including medicine, dentistry, chiropracty, physiotherapy and osteopathy (s 81).
A general practitioner engages in inappropriate practice if his or her conduct in connection with rendering or initiating services is such that a Committee could reasonably conclude that the conduct would be unacceptable to the general body of general practitioners (s 82(1)(a)). Similar definitions of “inappropriate practice” apply to practitioners of the other professions regulated by the Professional Services Review Scheme (s 82).
The Minister may appoint a medical practitioner to be the Director of Professional Services Review …
The Chief Executive Officer of Medicare Australia (previously the Health Insurance Commission) may request the Director to review the provision of services by a person during the period of up to two years immediately preceding the request (ss 86, 88A). The Director has one month to decide whether or not to undertake the review. The Director must so decide if it appears to him or her that there is a possibility that the person has engaged in inappropriate practice in providing services during the review period (s 88A(2)). If the Director decides to undertake the review, he or she must set up a Committee in accordance with Div 4 of Pt VAA and make a referral to it to investigate whether the person under review did engage in inappropriate practice in providing the services specified in the referral (s 93(1)).
…
Once a Committee has been set up, it must carry out its functions of investigation under the Act and produce a final report (s 106G(1) and (2)). It must make findings only in respect of the services referred to it for review (s 106H). After the Committee has prepared a draft report it must provide the draft to the person under review for his or her written submissions as to suggested changes (s 106KD). Then, if the person under review has had the opportunity to suggest changes, the Committee must prepare a final report in accordance with s 106L. If that final report contains a finding of inappropriate practice by the person under review, the Committee must give it to the Determining Authority (s 106L(3)(b)). The Determining Authority has functions under Div 5 of Pt VAA to make determinations that, among others, can provide for services by the person under review to cease to be eligible for Medicare benefits or require him or her to repay to the Commonwealth the whole or part of any such benefits that he or she had received (s 106U).
8 It can be seen that there are several stages of decision-making before a final determination can be made imposing sanctions under s 106U. The relevant stages in this proceeding are: first, the decisions, conduct and findings of fact of the Committee in its final report under s 106L of the Act dated 18 November 2014; and, second, the final determination of the Determining Authority pursuant to s 106TA imposing sanctions under s 106U.
Background facts and procedural history
9 The following summary is drawn from the parties’ agreed statement of facts and chronology and from copies of key documents in the decision-making process annexed to affidavits filed in this proceeding.
10 On 12 July 2013, pursuant to s 86 of the Health Insurance Act, a delegate of the Chief Executive Officer of Medicare requested that the first respondent, the Director of Professional Services Review, review the provision of services by the applicant for the period of 1 December 2011 to 20 November 2012. After conducting a review, the Director established the Committee pursuant to s 93 of the Act and made a referral to the Committee to investigate whether the applicant had engaged in inappropriate practice in providing particular services under the Medicare Benefits Schedule (MBS item numbers 37, 597, 5043, and 721) during the review period.
The Committee’s decision
11 Pursuant to s 106, the Committee conducted a hearing over five days in March 2014. The applicant appeared in person at the hearing and gave evidence with legal assistance from a solicitor.
12 Following the hearing, pursuant to s 106KD, the Committee provided the applicant with its draft report dated 22 July 2014. The draft report recorded the Committee’s preliminary finding that the applicant had engaged in inappropriate practice within the meaning of s 82 in connection with all of the MBS item 37, 5043 and 721 services and 89 per cent of the MBS item 597 services in the review period. In making that finding, the Committee applied the Health Insurance (Professional Services Review – Sampling Methodology) Determination 2006 (Cth) made under s 106K(3) of the Act.
13 On 4 September 2014, pursuant to s 106KE(3), the applicant provided written submissions to the Committee in respect of the draft report.
14 On 18 November 2014, the Committee issued its final report pursuant to s 106L recording:
(1) the Committee’s finding that the applicant had engaged in inappropriate practice in the rendering of:
(a) MBS item 37, 597 and 5043 services, including because of inadequate clinical input, because the services did not meet MBS requirements, and because of a failure to keep adequate records; and
(b) MBS item 721 services, including because of inadequate clinical input and because the services did not meet MBS requirements; and
(2) the Committee’s opinion that the applicant’s conduct during the review period had caused, was causing, or was likely to cause, a significant threat to the life or health of the patients under his care and failed to comply with professional standards.
15 Having made those findings, on 11 November 2014 the Committee referred the applicant’s conduct to the Director for appropriate action pursuant to ss 106XA and 106XB.
16 Further, a copy of the Committee’s report was given to the first and third respondents, the Director and the Determining Authority, pursuant to s 106L(3).
The Determining Authority’s decision
17 On 8 January 2015, the applicant was invited pursuant to s 106SA to make submissions about the directions the Determining Authority should make as a result of the Committee’s report. He provided his written submissions on 6 and 9 February 2015.
18 On 6 March 2015, the Determining Authority provided the applicant with its draft determination under s 106T of the Act proposing directions that he be reprimanded and formally counselled, fully disqualified for the purposes of s 19B for a period of two years (so that a medicare benefit would not be payable in respect of services rendered by him during that time), and that he repay $453,656.75 to the Commonwealth. The proposed repayment amount of $453,656.75 corresponds to the figure representing all of the medicare benefits paid for MBS item 37, 5043 and 721 services and 89 per cent of the medicare benefits paid for MBS item 597 services in the review period. The Determining Authority gave the applicant an opportunity to make written submissions as to any amendments to the proposed directions.
19 On 24 March 2015, the applicant provided his written submissions. He accepted that he should be reprimanded and counselled, but opposed the proposed directions in relation to repayment and disqualification. He submitted that those directions should be amended to direct that he be disqualified only from receiving medicare benefits for MBS item 23 services and that he be directed to repay only 50 per cent of the amount proposed.
20 The Determining Authority did not accept those submissions and on 12 May 2015 sent the applicant its final determination, making directions in materially the same terms it had earlier proposed.
21 On 11 June 2015, the applicant commenced the present proceedings for judicial review.
INTERLOCUTORY APPLICATION REGARDING ACCESS AND DISCLOSURE
22 On 22 January 2016, the first respondent filed an interlocutory application seeking orders restricting access to, or publication of, certain documents provided as annexures to an affidavit of Dr Sevdalis sworn 27 August 2014 and as annexures to affidavits of Bruce Neville Topperwien affirmed 15 October 2015 and 20 November 2015 filed on behalf of the respondents. The relevant documents comprised material produced to and by the Committee in the course of its review of services provided by Dr Sevdalis.
23 An affidavit in support of the interlocutory application drew attention to s 106ZR of the Act, which relevantly provides:
(1) A person must not disclose to another person:
(a) any of the deliberations or findings of a Committee; or
(b) any information or evidence given to the Committee in the course of its deliberations;
unless the disclosure is required or permitted under this Act or the Dental Benefits Act 2008 or is necessary in connection with the performance of the first-mentioned person’s functions or duties under this Act or the Dental Benefits Act 2008.
Penalty: Imprisonment for 12 months.
24 The interlocutory application was heard on 28 January 2016 and, on 2 February 2016, the Court made orders restricting access to the documents identified by the first respondent. The Court published reasons in relation to those orders and in relation to the application of s 106ZR to court processes: Sevdalis v Director of Professional Services Review [2016] FCA 32.
APPLICATION FOR AN EXTENSION OF TIME
25 The applicant seeks an extension of time to make an application under the AD(JR) Act in respect of the decision and conduct of the Committee. Neither party addressed the question whether an extension was required or should be granted in written submissions or at the hearing of the matter. Given the applicant could proceed under the Judiciary Act in any event, in my opinion it is appropriate to grant the extension of time.
APPLICATION FOR RELIEF
26 The applicant’s amended originating application (leaving aside three grounds no longer pressed by the applicant) articulates three review grounds impugning the Committee’s final report and five review grounds impugning the Determining Authority’s final determination.
27 It is convenient to follow broadly the grouping of grounds adopted by the parties in their submissions. The applicant contends that:
(1) in making findings in the final report about records kept by the applicant, the Committee misconstrued or misapplied the Health Insurance (Professional Services Review) Regulations 1999 (Cth) by inferring a requirement that such records be accessible to other practitioners (ground 3);
(2) in making findings in the final report about the services rendered by the applicant, the Committee misconstrued MBS items 37 and 5043 by construing those items as requiring a clinical need for the relevant services (grounds 5 and 6);
(3) in making the final determination, the Determining Authority made directions which were punitive rather than protective and therefore failed to take account of relevant considerations, including the risk of the applicant engaging in further inappropriate practice in the future, and acted for the improper purpose of punishing the applicant (grounds 7, 8 and 9); and
(4) in making a direction for the repayment of benefits in the amount of $453,656.75, the Determining Authority failed to take into account mandatory relevant considerations or otherwise acted contrary to law because it did not consider, in respect of each particular service examined by the Committee, whether the benefits paid in respect of that service should be repaid in part or in full (grounds 7.1.2, 10 and 11).
Relevant legislative provisions
28 Sections 9 and 10(1) of the Health Insurance Act provide for the payment of medicare benefits in respect of a range of medical services prescribed in tables set out in regulations made under the Act:
9 Medicare benefits calculated by reference to fees
Medicare benefits under this Part (other than sections 10ACA and 10ADA) shall be calculated by reference to the fees for medical services set out in the table.
10 Entitlement to Medicare benefit
(1) Where, on or after 1 February 1984, medical expenses are incurred in respect of a professional service rendered in Australia to an eligible person, medicare benefit calculated in accordance with subsection (2) is payable, subject to and in accordance with this Act, in respect of that professional service.
Note: For eligible person, medical expenses, medicare benefit and professional service see subsection 3(1).
29 Part VAA of the Act provides for the Professional Services Review Scheme. Section 79A sets out the object of Pt VAA:
The object of this Part is to protect the integrity of the Commonwealth medicare benefits, dental benefits and pharmaceutical benefits programs and, in doing so:
(a) protect patients and the community in general from the risks associated with inappropriate practice; and
(b) protect the Commonwealth from having to meet the cost of services provided as a result of inappropriate practice.
30 Section 80 summarises the main features of the scheme. It is convenient to set out those features in full:
(2) The Professional Services Review Scheme is a scheme for reviewing and investigating the provision of services by a person to determine whether the person has engaged in inappropriate practice.
(3) The Chief Executive Medicare can request the Director to review the provision of services by a person and the Director must decide whether to undertake a review.
(4) Following a review, the Director must:
(a) decide to take no further action in relation to the review; or
(b) enter into an agreement with the person under review; or
(c) make a referral to a Committee.
(5) If the Director enters into an agreement with the person under review, the agreement must be ratified by the Determining Authority before it takes effect. Having an agreement ratified avoids a Committee investigation.
(6) A referral to a Committee initiates an investigation by the Committee into the provision of the services specified in the referral. The Committee can investigate any aspect of the provision of the referred services and its investigation is not limited by any reasons given in a request for review or a Director’s report following a review.
(7) Committee members must belong to professions or specialities relevant to the investigation.
(8) Committees can hold hearings and require the person under review to attend and give evidence. Committees also have the power to require the production of documents (including clinical records).
(9) Committees can base findings on investigations of samples of services.
(10) If a Committee finds that the person under review has engaged in inappropriate practice, the finding will be reported to the Determining Authority. The Determining Authority decides what action to take.
(11) Provision is made throughout the scheme for the person under review to make submissions before key decisions are made or final reports are given.
(12) A Committee cannot make a finding of inappropriate practice unless it has given the person under review:
(a) notice of its intention to do so; and
(b) the reasons for the finding; and
(c) an opportunity to respond.
31 Section 86 provides that the Chief Executive Medicare may, and in certain cases must, request the Director of Professional Services Review to review the provision of services by a practitioner:
(1) Subject to subsection (1A), the Chief Executive Medicare may, in writing, request the Director to review the provision of services by a person during the period specified in the request.
Note: For provides services see subsection 81(2).
(1A) If the Chief Executive Medicare becomes aware that the circumstances in which services were rendered or initiated by a person constitute a prescribed pattern of services, the Chief Executive Medicare must make a request under subsection (1) in relation to the services.
(2) The period specified in the request must fall within the 2 year period immediately preceding the request.
(3) The request must include reasons for the request.
Note: If the request is made because of subsection (1A), it may include reasons other than the prescribed pattern of services.
(4) The content and form of the request must comply with any guidelines made under subsection (5).
(5) The Minister may, by legislative instrument, make guidelines about the content and form of requests for review.
32 Section 93 provides that the Director may refer an investigation concerning whether a practitioner engaged in “inappropriate practice” to a Professional Services Review Committee:
(1) The Director may, by writing, set up a Committee in accordance with Division 4, and make a referral to the Committee to investigate whether the person under review engaged in inappropriate practice in providing the services specified in the referral.
(2) If the referral arises from a request made by a Committee to the Director under subsection 106J(1), the Director may, instead of setting up a Committee under subsection (1), make the referral to the Committee that made the request.
(3) Subject to this section, the content and form of a referral must comply with any guidelines made under subsection (4).
(4) The Minister may, by legislative instrument, make guidelines about the content and form of referrals.
(6) If the Director makes a referral, the Director must:
(a) prepare a written report for the Committee, in respect of the services to which the referral relates, giving reasons why the Director thinks the person under review may have engaged in inappropriate practice in providing the services; and
(b) attach the report to the referral.
Note: The reasons given by the Director may relate solely to the services being rendered or initiated in circumstances that constitute a prescribed pattern of services.
(7) Within 7 days after making the referral, the Director must give a copy of the referral and report to the Chief Executive Medicare and the person under review.
(7A) The copy given to the person under review must be accompanied by a written notice setting out the terms of sections 102, 106H and 106K.
(7B) The services that may be specified in the referral are any or all of the services provided by the person under review during the review period.
(7C) Subsection (7B) is not limited by the terms of the Director’s report under subparagraph 89C(1)(b)(i).
(7D) Failure to comply with subsection (7) or (7A) does not affect the validity of the referral.
(8) If, in the course of the review that gave rise to the referral:
(a) the Director formed an opinion that any conduct by the person under review caused, was causing, or was likely to cause, a significant threat to the life or health of any person and sent a statement of his or her concerns to a person or body under section 106XA; or
(b) the Director formed an opinion that the person under review failed to comply with professional standards and sent a statement of his or her concerns to an appropriate body under section 106XB;
the referral must contain a statement that the Director formed that opinion and set out the terms of the statement sent to the person or body.
(9) The Director must disregard any opinion formed as mentioned in subsection (8) when making the referral.
33 Section 82 defines “inappropriate practice” in the following way:
Unacceptable conduct
(1) A practitioner engages in inappropriate practice if the practitioner’s conduct in connection with rendering or initiating services is such that a Committee could reasonably conclude that:
(a) if the practitioner rendered or initiated the services as a general practitioner—the conduct would be unacceptable to the general body of general practitioners; or
(b) if the practitioner rendered or initiated the services as a specialist (other than a consultant physician) in a particular specialty—the conduct would be unacceptable to the general body of specialists in that specialty; or
(c) if the practitioner rendered or initiated the services as a consultant physician in a particular specialty—the conduct would be unacceptable to the general body of consultant physicians in that specialty; or
(d) if the practitioner rendered or initiated the services as neither a general practitioner nor a specialist but as a member of a particular profession—the conduct would be unacceptable to the general body of the members of that profession.
Prescribed pattern of services
(1A) Subject to subsections (1B) and (1C), a practitioner engages in inappropriate practice in rendering or initiating services during a particular period (the relevant period) if the circumstances in which some or all of the services were rendered or initiated constitute a prescribed pattern of services.
(1B) A practitioner does not, under subsection (1A), engage in inappropriate practice in rendering or initiating services on a particular day during the relevant period if a Committee could reasonably conclude that, on that day, exceptional circumstances existed that affected the rendering or initiating of the services.
(1C) Subsection (1B) does not affect the operation of subsection (1A) in respect of the remaining day or days during the relevant period on which the practitioner rendered or initiated services even if the circumstances in which the services were rendered or initiated on that day or those days would not, if considered alone, have constituted a prescribed pattern of services.
(1D) The circumstances that constitute exceptional circumstances for the purposes of subsection (1B) include, but are not limited to, circumstances that are prescribed by the regulations to be exceptional circumstances.
Causing or permitting inappropriate practice
(2) A person (including a practitioner) engages in inappropriate practice if the person:
(a) knowingly, recklessly or negligently causes, or knowingly, recklessly or negligently permits, a practitioner employed by the person to engage in conduct that constitutes inappropriate practice by the practitioner under subsection (1) or (1A); or
(b) is an officer of a body corporate and knowingly, recklessly or negligently causes, or knowingly, recklessly or negligently permits, a practitioner employed by the body corporate to engage in conduct that constitutes inappropriate practice by the practitioner under subsection (1) or (1A).
34 Pursuant to s 82(3), in determining whether a practitioner engaged in inappropriate practice, a Committee must have regard to whether the practitioner kept adequate and contemporaneous records:
A Committee must, in determining whether a practitioner’s conduct in connection with rendering or initiating services was inappropriate practice, have regard to (as well as to other relevant matters) whether or not the practitioner kept adequate and contemporaneous records of the rendering or initiation of the services.
35 Under s 81, the term “adequate and contemporaneous records” is defined to mean “records that meet the standards prescribed by the regulations for the purposes of this definition”. The relevant regulations are the Professional Services Review Regulations. Regulations 5 and 6 prescribe the following definitions:
5 An adequate record
For the definition of adequate and contemporaneous records in section 81 of the Act, the standard to be met in order that a record of service rendered or initiated be adequate is that:
(a) the record clearly identify the name of the patient; and
(b) the record contain a separate entry for each attendance by the patient for a service and the date on which the service was rendered or initiated; and
(c) each entry provide clinical information adequate to explain the type of service rendered or initiated; and
(d) each entry be sufficiently comprehensible that another practitioner, relying on the record, can effectively undertake the patient’s ongoing care.
6 A contemporaneous record
For the definition of adequate and contemporaneous records in section 81 of the Act, the standard to be met in order that a record of a service rendered or initiated be contemporaneous, is that record must be completed:
(a) at the time the practitioner rendered or initiated the service; or
(b) as soon as practicable after the service was rendered or initiated by the practitioner.
36 Section 106K provides that, in the course of investigating services referred to it, a Committee may have regard to “samples” of the services:
(1) The Committee may, in investigating the provision of services included in a particular class of the referred services, have regard only to a sample of the services included in the class.
(2) If the Committee finds that a person has engaged in inappropriate practice in providing all, or a proportion, of the services included in the sample, then, the person under review is taken, for the purposes of this Part, to have engaged in inappropriate practice in the provision of all, or that proportion, as the case may be, of the services included in the class from which the sample is chosen.
(3) The Minister may, by legislative instrument, make determinations specifying the content and form of sampling methodologies that may be used by Committees for the purposes of subsection (1).
(4) The Committee may use a sampling methodology that is not specified in such a determination if, and only if, the Committee has been advised by a statistician accredited by the Statistical Society of Australia Inc that the sampling methodology is statistically valid.
37 The Health Insurance (Professional Services Review – Sampling Methodology) Determination 2006 (Cth) specifies a sampling methodology for the purpose of s 106K(1). Items 7 and 8 of the Determination provide:
7 Sample
(1) Under this methodology, the Committee must have regard to a sample of no fewer than 25 provided services randomly drawn from a class of referred services being investigated.
(2) The Committee may:
(a) omit a service from the sample; and
(b) include another provided service, randomly drawn from the same class, in its place.
(3) If the Committee omits a service and includes another provided service in its place under subsection (2), the Committee must state its reasons for doing so in the draft report and final report it prepares in respect of the person under review to whom the sample relates.
Note The Committee must prepare a draft report under section 106KD of the Act, and a final report under section 106L of the Act, in relation to its findings.
8 Determining percentage of inappropriate practice in sample
(1) A Committee relying on subsection 106K (1) of the Act must work out, in accordance with subsection (2), the proportion of services in the sample in relation to the provision of which the person under review engaged in inappropriate practice.
(2) For subsection (1), the proportion is to be expressed as a percentage, as follows:
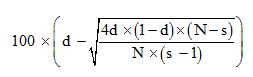
where:
d is the number of services in the sample that the Committee has determined are services in relation to the provision of which the person under review engaged in inappropriate practice, divided by s.
s is the number of services in the sample.
N is the number of services in the class.
(3) The percentage must be expressed as a whole number (if necessary, for that purpose, rounded down to the nearest whole number).
38 The Health Insurance (General Medical Services Table) Regulations 2011 (Cth) (2011 GMS Table Regulations) described the services that are the subject of findings in the Committee’s final report:
37 Professional attendance by a general practitioner (other than attendance at consulting rooms or a residential aged care facility or a service to which another item in the table applies), lasting at least 20 minutes and including any of the following that are clinically relevant:
(a) taking a detailed patient history;
(b) performing a clinical examination;
(c) arranging any necessary investigation;
(d) implementing a management plan;
(e) providing appropriate preventive health care;
for 1 or more health related issues, with appropriate documentation — an attendance on 1 or more patients at 1 place on 1 occasion — each patient
…
597 Professional attendance by a general practitioner on not more than 1 patient on 1 occasion – each attendance (other than an attendance in unsociable hours) in an after hours period if:
(a) the attendance is requested by the patient or a responsible person in, or not more than 2 hours before the start of, the same unbroken after hours period, and the patient’s medical condition requires urgent treatment; and
(b) if the attendance is performed at consulting rooms — it must be necessary for the practitioner to return to, and specially open, the consulting rooms for the attendance
…
721 Attendance by a medical practitioner (including a general practitioner, but not including a specialist or consultant physician), for preparation of a GP management plan for a patient (other than a service associated with a service to which any of items 735 to 758 apply)
…
5043 Professional attendance by a general practitioner (other than attendance at consulting rooms, a hospital or a residential aged care facility or a service to which another item in the table applies), lasting at least 20 minutes and including any of the following that are clinically relevant:
(a) taking a detailed patient history;
(b) performing a clinical examination;
(c) arranging any necessary investigation;
(d) implementing a management plan;
(e) providing appropriate preventive health care;
for 1 or more health related issues, with appropriate documentation — an attendance on 1 or more patients on 1 occasion — each patient
39 The review period examined by the Committee was 1 December 2011 to 30 November 2012. Therefore, the Health Insurance (General Medical Services Table) Regulations 2012 (Cth) (2012 GMS Table Regulations) were the relevant regulations for services provided by Dr Sevdalis after 1 November 2012, being the commencement date of those regulations and the date upon which they superseded the 2011 GMS Table Regulations, which were the relevant regulations before that date. However, apart from the amounts payable for the relevant services, the 2011 and 2012 regulations are materially the same for the purposes of the applicant’s judicial review grounds. I will therefore refer to the 2011 regulations only, unless the context requires specificity as to which of the regulations is relevant.
40 Clause 1.2.3(2) of Schedule 1 of the 2011 GMS Table Regulations provided in respect of the term ‘professional attendance’ in items 37, 597 and 5043:
(2) A professional attendance includes the provision, for a patient, of any of the following services:
(a) evaluating the patient’s condition or conditions including, if applicable, evaluation using a health screening service mentioned in subsection 19 (5) of the Act;
(b) formulating a plan for the management and, if applicable, for the treatment of the patient’s condition or conditions;
(c) giving advice to the patient about the patient’s condition or conditions and, if applicable, about treatment;
(d) if authorised by the patient — giving advice to another person, or other persons, about the patient’s condition or conditions and, if applicable, about treatment;
(e) providing appropriate preventive health care;
(f) recording the clinical details of the service or services provided to the patient.
41 “Clinically relevant service” is defined in s 3(1) of the Act to mean:
a service rendered by a medical or dental practitioner or an optometrist that is generally accepted in the medical, dental or optometrical profession (as the case may be) as being necessary for the appropriate treatment of the patient to whom it is rendered.
42 Clause 2.23.1(2) of Sch 1 of the 2011 GMS Table Regulations provided that item 5043 applied “only to a professional attendance that is provided in an after-hours period”, where “after-hours period” was defined to mean any of the following:
(a) a public holiday;
(b) a Sunday;
(c) before 8 am, or after 12 noon, on a Saturday;
(d) before 8 am, or after 6 pm, on any day other than a Saturday, Sunday or public holiday.
43 Clause 2.15.1 of Sch 1 of the 2011 GMS Table Regulations set out the meaning of “patient’s medical condition requires urgent treatment” in item 597:
(1) For items 597 to 600, a patient’s medical condition requires urgent treatment if:
(a) medical opinion is to the effect that the patient’s medical condition requires treatment within the unbroken after hours period in, or before, which the attendance mentioned in the item was requested; and
(b) treatment could not be delayed until the start of the next in hours period.
(2) For subclause (1), medical opinion is to a particular effect if:
(a) the attending practitioner is of that opinion; and
(b) in the circumstances that existed and on the information available when the opinion was formed, that opinion would be acceptable to the general body of medical practitioners.
44 The prescribed fee for each relevant service under the 2011 GMS Table Regulations, described as the “Schedule fee” in s 8(1A) of the Act, was:
(1) for an item 37 service, $69.00 plus either:
(a) $25 divided by the number of patients if there were not more than six patients in a single attendance; or
(b) $1.90 multiplied by the number of patients if there were more than six patients in a single attendance;
(2) $124.90 for an item 597 service;
(3) for an item 5043 service, $80.75 plus either:
(a) $25 divided by the number of patients if there were not more than six patients in a single attendance; or
(b) $1.90 multiplied by the number of patients if there were more than six patients in a single attendance; and
(4) $138.75 for an item 721 service.
45 The Schedule fee for each relevant service under the 2012 GMS Table Regulations was:
(1) for an item 37 service, $70.30 plus either:
(a) $25.45 divided by the number of patients if there were not more than six patients in a single attendance; or
(b) $1.95 multiplied by the number of patients if there were more than six patients in a single attendance;
(2) $127.25 for an item 597 service;
(3) for an item 5043 service, $82.30 plus either:
(a) $25.45 divided by the number of patients if there were not more than six patients in a single attendance; or
(b) $1.95 multiplied by the number of patients if there were more than six patients in a single attendance; and
(4) $141.40 for an item 721 service.
46 The Schedule fees must be read together with s 10(2) of the Act, which provides:
(2) A benefit in respect of a service is:
(a) in the case of a service provided:
(i) as part of an episode of hospital treatment; or
(ii) as part of an episode of hospital‑substitute treatment in respect of which the person to whom the treatment is provided chooses to receive a benefit from a private health insurer;
an amount equal to 75% of the Schedule fee; or
(aa) in the case of a service to which paragraph (a) does not apply and that is prescribed by the regulations for the purposes of this paragraph—an amount equal to 100% of the Schedule fee; or
(b) in any other case—an amount equal to 85% of the Schedule fee.
47 If a Committee makes a finding of inappropriate practice in its final report, s 106L(3) provides that, subject to an irrelevant exception, the Committee must:
(a) give copies of the final report to the person under review and the Director; and
(b) give the final report to the Determining Authority not earlier than 1 month after the day on which a copy of the report is given to the person under review.
48 Section 106SA(1) provides that the Determining Authority must give the person under review an opportunity to make written submissions regarding the Committee’s final report:
(1) The Determining Authority must give the person under review a written invitation to make written submissions to the Authority, having regard to the Committee’s final report and any information given by the Director under section 106S, about the directions the Authority should make in the draft determination relating to the person.
49 Pursuant to s 106T(1) and (3), the Determining Authority must then produce a draft determination and give it to the person under review, who may make further written submissions in relation to the draft determination:
(1) The Determining Authority must, after taking into account any submissions made by the person under review in accordance with section 106SA:
(a) make a draft determination in accordance with section 106U relating to the person; and
(b) give copies of the draft determination to the person and to the Director.
…
(3) The person under review may, within the 14 day period referred to in subsection (2), make written submissions to the Authority suggesting changes to the directions contained in the draft determination.
50 Section 106TA(1) provides that the Determining Authority must then produce a final determination:
(1) If the Determining Authority has made a draft determination under section 106T, the Authority must, within one month after the end of the 14 day period within which the person under review may make submissions, and after taking into account any submissions made by the person during that 14 day period, make a final determination in accordance with section 106U relating to the person under review.
51 Section 106U prescribes the content of determinations which may be made by the Determining Authority:
(1) A draft determination or a final determination must contain one or more of the following directions:
(a) that the Director, or the Director’s nominee, reprimand the person under review;
(b) that the Director, or the Director’s nominee, counsel the person under review;
(c) that any medicare benefit or dental benefit that would otherwise be payable for a service in the provision of which the person is stated in a report under section 106L to have engaged in inappropriate practice cease to be payable;
(ca) if any medicare benefit or dental benefit for a service:
(i) that was rendered or initiated by the person under review, by an employee of the person under review, or by an employee of a body corporate of which the person under review is an officer; and
(ii) in connection with the rendering or initiation of which the person under review or such an employee is stated in a report under section 106L (other than a report based on a finding made under subsection 106K(2) or 106KB(3)) to have engaged in inappropriate practice;
has been paid (whether or not to the person under review)—that the person under review repay to the Commonwealth the whole or a part of the medicare benefit or dental benefit that was paid for that service;
(cb) if any medicare benefits or dental benefits for a class of services:
(i) that were rendered or initiated by the person under review, by an employee of the person under review, or by an employee of a body corporate of which the person under review is an officer; and
(ii) in connection with the rendering or initiation of which, or of a proportion of which, the person under review or such an employee is stated in a report under section 106L, based on a finding made under subsection 106K(2), to have engaged in inappropriate practice;
have been paid (whether or not to the person under review)—that the person under review repay to the Commonwealth the whole or a part of the medicare benefits or dental benefits that were paid for the services or that proportion of the services, as the case may be;
(e) if the person under review is a participating optometrist—that the Minister’s acceptance of the undertaking by the participating optometrist under section 23B is taken to be revoked, either wholly or in so far as the undertaking covers particular premises;
(ea) if the person under review is a midwife and there is in force in respect of the person an undertaking under section 21B—that the Minister’s acceptance of the undertaking is to be taken to be revoked;
(eb) if the person under review is a nurse practitioner and there is in force in respect of the person an undertaking under section 22A—that the Minister’s acceptance of the undertaking is to be taken to be revoked;
(f) if the person under review is a person in respect of whom a Part VII authority is in force and the service in connection with which the person is stated in a report under section 106L to have engaged in inappropriate practice involves prescribing or dispensing a pharmaceutical benefit—that the Part VII authority be taken, for the purposes of the National Health Act 1953, to be suspended;
(g) if the person under review is a practitioner—that the practitioner be disqualified, for a specified period starting when the determination takes effect, in respect of one or more of the following:
(i) provision of specified services, or provision of services other than specified services;
(ii) provision of services to a specified class of persons, or provision of services to persons other than persons included in a specified class of persons;
(iii) provision of services within a specified location, or provision of services otherwise than in a specified location;
(h) if the person under review is a practitioner—that the practitioner be fully disqualified for a specified period starting when the determination takes effect.
Note: Medicare benefits and dental benefits are not payable in respect of services rendered or initiated by, or on behalf of, disqualified practitioners (see section 19B of this Act in relation to medicare benefits, and section 20A of the Dental Benefits Act 2008 in relation to dental benefits).
(1A) For the purposes of paragraph (1)(cb), it is to be assumed that all the medicare benefits paid for services in the class of services referred to in that paragraph were paid at the lowest rate that was payable for any of the services included in the class.
…
(2A) A direction under paragraph (1)(f) must specify a period of suspension of up to 3 years, to start when the determination takes effect.
(3) For the purposes of paragraphs (1)(g) and (h), the period specified must not be more than:
(a) if the person under review is a practitioner in relation to whom an agreement under section 92, or a final determination under section 106TA, has previously taken effect—5 years; or
(b) in any other case—3 years.
The decision and report of the Committee
52 In its final report, the Committee first set out the review process it followed, including an account of hearings held in March 2014, which the applicant attended with a solicitor, and a description of documents the Committee examined in the course of its review. The Committee then gave a summary of its findings in respect of each relevant service and recorded the sampling process it adopted in respect of those services pursuant to s 106K of the Act. The Committee provided its draft report to the applicant on 22 July 2014 and invited him to make written submissions regarding the draft report pursuant to s 106KD(3) of the Act. In its final report, the Committee summarised those submissions and set out its final findings regarding whether the applicant engaged in inappropriate practice in relation to each of the services it examined. Detailed reasons for the Committee’s findings in respect of each sampled service are contained in appendices to the report.
53 Based on its review of the sampled services, the Committee found that Dr Sevdalis had engaged in inappropriate practice, in particular because:
the conduct of Dr Sevdalis in connection with providing the services referred to below would be unacceptable to the general body of General Practitioners: as defined in section 82(1 )(a) of the Health Insurance Act 1973:
100% of the MBS Item 37 services
89% of the MBS Item 597 services
100% of the MBS item 5043 services
100% of the MBS item 721 services examined by the Committee.
54 The Committee summarised its reasons for those findings in respect of each item. In respect of items 37, 597 and 5043, the Committee stated that its findings were for “one or more of the following reasons”:
the clinical input was inadequate for the service
the service did not meet the MBS requirements for this item
lack of contemporaneous clinical records.
55 In relation to its findings of lack of contemporaneous clinical records, the Committee said in respect of each relevant item that:
The entries in the clinical records contained insufficient information to enable another practitioner to effectively take over patient care.
56 For each relevant item, the Committee then listed the particular pieces of information it found were missing from some or all of the clinical records for the services it examined.
57 In respect of item 721, the Committee stated that its finding in relation to the services it examined was for “one or more of the following reasons”:
the clinical input was inadequate for the service
the service did not meet the MBS requirements for this item.
58 The Committee did not make a finding of lack of contemporaneous records in relation to the item 721 services.
59 In appendices 1 to 4 to its report, the Committee set out its detailed findings regarding the sampled services it examined from items 37, 597, 5043 and 721 respectively. I have extracted certain of those detailed findings at [89] to [90] below. The findings differ somewhat in relation to each service, but in relation to service number 1 of the item 37 services, for example, the Committee found that Dr Sevdalis’s clinical input was inadequate because he did not:
undertake a physical examination of the patient
perform a mental state examination
assess the patient’s risk of suicide
take an adequate history regarding the patient’s psychological illness or the problems the patient suffered from.
60 In relation to whether the service met the MBS requirements for item 37, the Committee found that:
Dr Sevdalis did not keep appropriate documentation as is required when rendering an item 37 service. The entry for the date of service did not adequately document the service Dr Sevdalis advised the Committee he provided and therefore, did not meet the MBS requirements for item 37.
This consultation should have been conducted at the practice as Dr Sevdalis advised that the patient’s parents were arguing and the patient did not want to be in the middle of these arguments. Therefore the Committee is of the opinion that a home visit was inappropriate and not warranted on this occasion.
61 The Committee then set out the particular information it found should have been included in the clinical record for the service and was not.
62 The Committee’s detailed findings in respect of each sampled service for each item follow a similar format, although the content of the findings varies according to the particular service.
The decision of the Determining Authority
63 Unlike the Committee (see s 106L of the Act), the Act did not require that the Determining Authority give reasons for its final determination. Nevertheless, it did so. The determination contains a summary of the Determining Authority’s decision, followed by relatively brief reasons for decision. In its reasons, the Determining Authority first set out the material it relied upon, including the Committee’s report and Dr Sevdalis’ submissions to the Determining Authority, as well as the procedural background and a summary of the Committee’s findings. It then set out its reasons for each direction that it made, relating to reprimand and counselling, repayment of medicare benefits, and disqualification.
64 At the outset of its reasons, the Determining Authority stated that it considered the inappropriate practice found by the Committee to be of a “serious nature”, noting the “very high proportion” of inappropriate practice in the services examined by the Committee and the Committee’s finding that Dr Sevdalis fabricated certain documents purported to be contemporaneous clinical notes. In relation to the fabrication of documents, the Determining Authority found at [25] that:
These actions indicate that Dr Sevdalis had not taken responsibility for his inappropriate practice, and did not accord appropriate respect to the processes of the Committee.
65 It also stated at [28] that:
The importance of clinical records in the management of patient care should not be understated. The inadequacies of Dr Sevdalis’ clinical records adversely affect his ability (and the ability of other practitioners) to provide effective and adequate care to his patients. The Committee’s finding is indicative of the importance and value that the profession places on clinical records.
66 In relation to the repayment of medicare benefits, the Determining Authority found that the Commonwealth “should not have to bear the cost of services in respect of which Dr Sevdalis had been found to have engaged in inappropriate practice”. While acknowledging the submissions that Dr Sevdalis had made regarding his difficult personal circumstances and his submission regarding the ameliorating effect those circumstances should have on any sanctions, the Determining Authority determined at [36] that:
When considering the serious nature and extent of the inappropriate practice, including the findings on inadequate clinical input, clinical records and the purpose of the Act, and the issues raised in submissions on behalf of Dr Sevdalis, the Determining Authority has, on balance, decided that it should exercise its discretion to make a direction for repayment of the whole of the Medicare benefit that was paid for those services in connection with which Dr Sevdalis was found to have engaged in inappropriate practice.
67 After discussing Dr Sevdalis’s submissions and the factors it considered relevant to the extent of any repayment direction, the Determining Authority again stated at [47] that it:
considers that a direction requiring repayment of the whole of the Medicare benefits that were paid for the proportion of the services is indicated in the circumstances.
68 While the Determining Authority discussed the competing considerations, it did not give detailed reasons for why it decided that the matters put by Dr Sevdalis were insufficient to persuade it that a lesser sanction should be imposed.
69 The Determining Authority also considered Dr Sevdalis’ submissions that a two year disqualification should not be imposed on him because it could disadvantage his patients and result in him losing medical skills. Nevertheless, the Determining Authority decided at [56] that:
The Determining Authority is of the view that inappropriate conduct can place patients at risk and that the directions in this determination are proportionate to the inappropriate conduct found by the Committee and also the previous conduct of Dr Sevdalis as set out in the previous final determination. Any possible adverse consequences to the patients of Dr Sevdalis of a disqualification may be managed by Dr Sevdalis’ patients for the period of the disqualification.
70 The Determining Authority therefore made the directions I have set out at [18] above.
Consideration of the applicant’s grounds for judicial review
71 In reaching a conclusion on each of the applicant’s grounds of review, it should be recalled that the structure of the legislative scheme involves an entitlement to receive a “medicare benefit” in respect of each “professional service” rendered (relevantly) in Australia to an eligible person. The amount to which the practitioner is entitled by way of medicare benefit is to be calculated in accordance with s 10(2), read with the relevant regulations, which I have set out above.
72 In other words, so long as what the practitioner does meets the definition of “professional service” in the Act – including, relevantly, because it is a “clinically relevant” service to which an item in the applicable regulations relates – the practitioner is entitled (again, relevantly to this proceeding and putting to one side hospital treatment) to either 100% or 85% of the Schedule fee set out in the regulations.
73 Part of the role and function of Pt VAA in the legislative scheme is to monitor and, if necessary, investigate whether what a practitioner has been paid by way of her or his entitlement under s 10 accords with the scheme. Since the introduction of the concept of “inappropriate practice” as the touchstone for the review, as well as the investigation and determination functions in Pt VAA, there is no doubt that practitioners’ conduct is exposed to review on broader grounds than their entitlement to payment in accordance with the Act and regulations.
74 In Pradhan v Holmes [2001] FCA 1560; 125 FCR 280, Finn J said (at [8]):
Previously the mechanism employed to protect public revenues was by policing “excessive servicing” by a practitioner. The change to concern with “inappropriate practice” was remarked on in the Second Reading Speech on the 1993 amending bill in the following terms (Australia, House of Representatives, Debates (1993) p 1551):
“A significant change in the bill is the replacement of the concept of excessive servicing with one of inappropriate practice. Whereas excessive servicing is currently defined as the rendering or initiation of services not reasonably necessary for the adequate care of the patient, the concept of inappropriate practice goes further. It covers a practitioner engaging in conduct in connection with the rendering or initiating of services that is unacceptable to his or her professional colleagues generally.”
75 The breadth of the concept of inappropriate practice as the touchstone for the review, investigation and determination functions in Pt VAA was also emphasised by French CJ and Gummow J in Wong v Commonwealth [2009] HCA 3; 236 CLR 573 at [64]:
The statutory criterion of conduct unacceptable to the general body of general practitioners, of which the appellants also complain, is an adaptation for the operation of the Act of principles of professional responsibility developed in the second half of the nineteenth century. The phrase “infamous conduct in any professional respect” found in s 29 of the Medical Act 1858 (UK) and memorably construed in Allinson v General Council of Medical Education and Registration with use of the phrase “disgraceful or dishonourable”, has been seen since as not necessarily requiring an appeal to a moral standard. The essential question in such cases is whether “the practitioner was in such breach of the written or unwritten rules of the profession as would reasonably incur the strong reprobation of professional brethren of good repute and competence”. The rendering of services not reasonably necessary for the care of the patient may be dubbed “overservicing”, but may also attract the reprobation just described.
(Footnotes omitted.)
76 Hayne, Crennan and Kiefel JJ made similar comments regarding the history of the regulation of professional misconduct by medical practitioners at [220]-[221] and continued at [222]:
More recent legislation regulating the conduct of professional practitioners such as medical and legal practitioners has moved away from the notion of “infamous conduct” and has provided for a much greater range of punishments for professional default than termination of the right to practise by striking off the appropriate register. And as Lord Hoffmann, delivering the opinion of the Judicial Committee of the Privy Council in McCandless v General Medical Council, pointed out, “the public has higher expectations of doctors and members of other self-governing professions [and] [t]heir governing bodies are under a corresponding duty to protect the public against the genially incompetent as well as the deliberate wrongdoers”.
(Footnotes omitted.)
77 As these observations make clear, the two-stage system established by Pt VAA for peer review by, first, a Committee and then, the Determining Authority, authorises a broad review and investigation of the way in which a practitioner delivered services to patients, well beyond whether the practitioner was entitled to a medicare benefit for a particular service in accordance with the Act and regulations.
78 Some of the findings made by the Committee about the applicant fall into this broader category. In the overview section of its decision, the Committee found that, for each class of services examined (items 37, 597, 721 and 5043) Dr Sevdalis’ “clinical input was inadequate for the service” and that “the service did not meet the MBS requirements for this item”. Those two findings are common to each of the classes of services investigated by the Committee. Common to three of the four classes (items 37, 597 and 5043) are further findings that there was a “lack of contemporaneous clinical records” for the services investigated and that the entries in the clinical records kept by Dr Sevdalis “contained insufficient information to enable another practitioner to effectively take over patient care”. Specific items of missing “essential clinical information” are listed after the latter finding in respect of each of the three classes of services, with the missing items differing according to the nature of the services in question.
79 For each randomly sampled service, these findings are expanded upon, under headings which correlate to the findings, in appendices 1 to 4. In that part of the Committee’s final report in which it dealt with submissions from Dr Sevdalis, there appears (on p 14) a heading “Requirements of MBS Items”. It is some of the statements by the Committee in this part of its report upon which the applicant fastens to advance his challenge as set out in ground 3. There is a further passage at [79] of the Committee’s report which is important in this respect. I return to those passages in my consideration of ground 3, below. It is somewhat difficult to tell, from the structure and content of the Committee’s report, when it is dealing with an analysis only of the correlation between the requirements of the regulations (through the MBS item) and the delivery of a “professional service”, and when it is dealing with the broader concept of inappropriate practice. Sometimes, the two appear to overlap entirely, while at other times the contrary appears to be the case.
80 However, I accept the first respondent’s submissions that care is necessary in examining the Committee’s report to ensure that the breadth of the statutory concept of “inappropriate practice”, and the Committee’s role in determining what constitutes inappropriate practice in respect of particular services provided by a practitioner, is not undermined or constrained in a way that is not provided for by the Act.
81 It is necessary to say something at a general level about the function of the Determining Authority. The legislative scheme allocates to the Committee the fact finding functions in reviewing and investigating a practitioner. There is no scope for the Determining Authority to proceed on the basis of different, additional or inconsistent factual findings to those made by the Committee. Nor is there any scope for the Determining Authority to depart from the characterisation of a practitioner’s conduct by the Committee as “inappropriate practice”, or to decide that there should be no consequence at all for the practitioner flowing from the Committee’s report. The terms of s 106U make it clear that the Determining Authority must impose some kind of consequence or sanction on a practitioner who has been found by a Committee to have engaged in inappropriate practice.
82 The Determining Authority’s function is to examine the material before the Committee and its findings, together with any submissions made by the practitioner, and form its own opinion about what, within the range of options set out in s 106U, is the appropriate sanction or consequence for that practitioner in the particular circumstances of the inappropriate practice identified. The opinion formed by the Determining Authority and implemented through the directions given under s 106U must be consistent with the purposes of Pt VAA as set out in s 79A, as well as (at a minimum) being rational, legally reasonable and based on probative material: Minister for Immigration and Citizenship v Li [2013] HCA 18; 249 CLR 332 at [24]-[30] (French CJ), [64]-[76] (Hayne, Kiefel and Bell JJ), [88]-[92], [105]-[113] (Gageler J); Minister for Immigration and Citizenship v SZMDS [2010] HCA 16; 240 CLR 611 at [124] (Crennan and Bell JJ); FTZK v Minister for Immigration and Border Protection [2014] HCA 26; 88 ALJR 754 at [16] (French CJ and Gageler J), [31] (Hayne J), [96] (Crennan and Bell JJ).
The Committee’s finding about adequate and contemporaneous records (grounds 3 and 4)
83 The Applicant did not press ground 4 of the application. That left ground 3, which in its terms is a challenge to the Committee’s construction of reg 5 of the Professional Services Review Regulations, relating to whether a record is “adequate”. In oral argument there was some emphasis put on a misconstruction of reg 6 of the same regulations, relating to whether a record is “contemporaneous”, but this would appear to travel outside the grounds as articulated. Nevertheless, the terms of reg 6 are of some relevance, as the first respondent also submitted, because in fact the phrase “adequate and contemporaneous records” is a composite phrase as used in the Act.
84 The phrase is found in s 82(3) of the Act. In its terms, it imposes a statutory obligation on the Committee to take a particular matter into account in making its determination whether a practitioner has engaged in inappropriate practice pursuant to s 82(1) on the referral given to it by the Director under s 93 of the Act. It is clear from s 82(3) that when the Committee is determining whether a practitioner has engaged in inappropriate practice in respect of the services in the Director’s referral and within the meaning given to that phrase in s 82(1) of the Act, the Committee is obliged to examine, and take into account, “whether or not the practitioner kept adequate and contemporaneous records of the rendering or initiation of the services”, as those services are set out in the Director’s referral. The keeping of adequate and contemporaneous records is a relevant consideration in the Committee’s determination concerning inappropriate practice: Minister for Aboriginal Affairs v Peko-Wallsend Ltd [1986] HCA 40; 162 CLR 24, 39-42 (Mason J), 56 (Brennan J). If the consideration is either not taken into account, or misunderstood, this is likely to be a legal error of a jurisdictional kind: Minister for Immigration and Multicultural Affairs v Yusuf [2001] HCA 30; 206 CLR 323, [37]-[39] (Gaudron J), [82] (McHugh, Gummow and Hayne JJ, Gleeson CJ agreeing).
85 The phrase is defined in s 81(1) and then in regs 5 and 6 of the Professional Services Review Regulations, which I have set out at [35] above.
86 I note that this definition describes the function of the regulations as prescribing “standards”. That description, combined with the text of the regulations themselves, indicates that there is some need for an evaluative exercise by the Committee, as fact finder, whether the records kept by the practitioner in respect of the relevant services meet the prescribed standard. The Committee complied with its obligation to take this matter into account: the applicant’s contention is that, in doing so, it misunderstood or misconstrued the consideration.
87 As developed on behalf of the applicant in oral submissions, the challenge had two aspects.
88 First, it was submitted that the Committee’s report demonstrated that it had introduced a gloss on, or an additional requirement in, the concept of adequate and contemporaneous records because it introduced a requirement that Dr Sevdalis’ records be “ readily accessible by other practitioners”, or (in other places) “readily available”. The applicant relied on the following passage in the Committee’s report:
On carefully considering their statements, very little can be drawn from them that would assist Dr Sevdalis to show, in relation to the services that the Committee examined, that he kept adequate and contemporaneous clinical notes that were readily accessible by other medical practitioners. Staff at the Medical Practice would have been aware only of those notes to which they had access. If the notes were not in the file they could not know whether or not notes existed or whether or not Dr Sevdalis had rendered or initiated a service.
89 The applicant submitted the approach in this paragraph was also reflected in the more detailed reasoning of the Committee in the appendices. An example used was a service in appendix 3, in relation to services rendered under Item 5043.
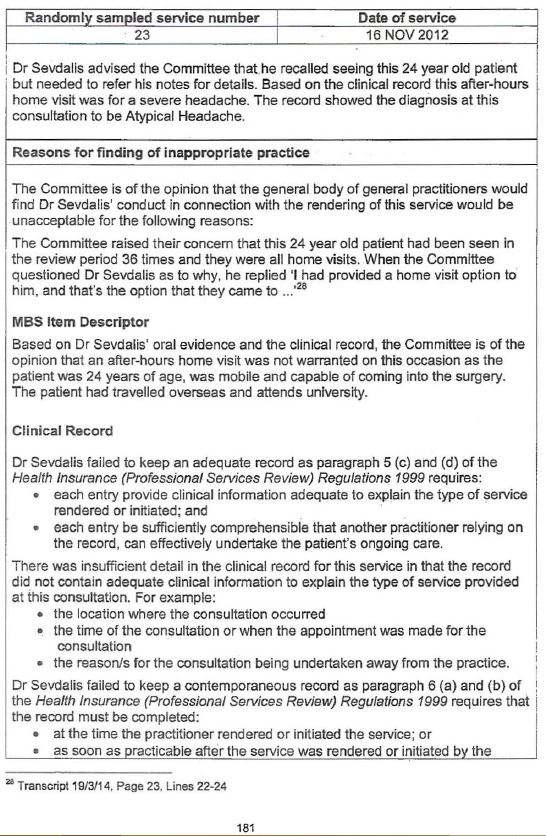
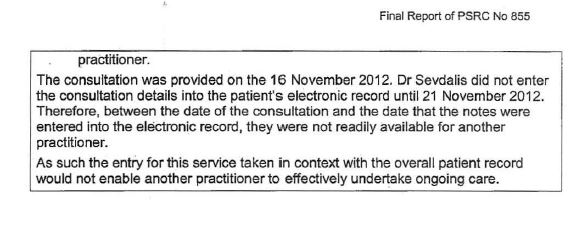
90 A further example was the following, also in appendix 3 concerning item 5043 services:
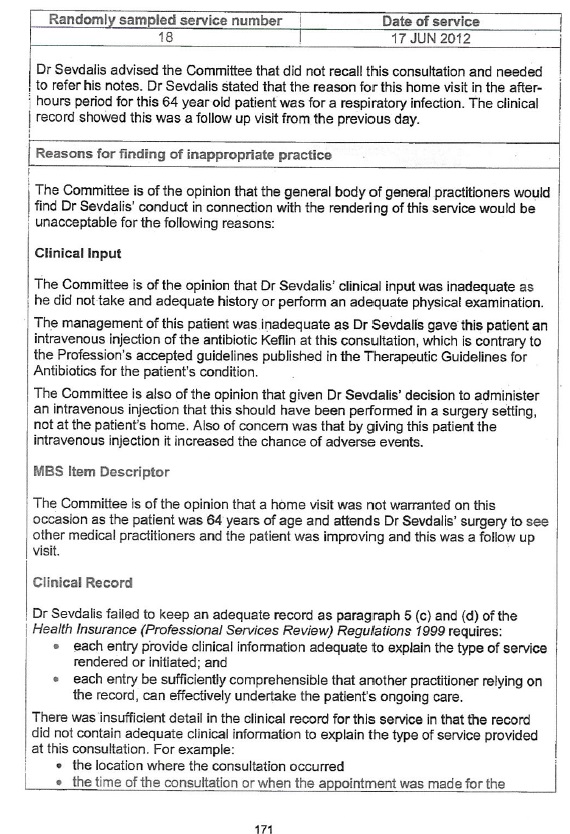
91 I understood the applicant’s submissions to accept that these examples are representative for the purposes of his argument.
92 It can be seen that, in both examples, the “accessibility” point made by the Committee is attached to the Committee’s interpretation of reg 6 and not reg 5.
93 The construction of reg 6 is not put in issue in the applicant’s ground 3.
94 However, the argument was certainly developed orally by reference to both reg 5 and reg 6 and the first respondent was on notice of the arguments as put. Indeed, it was the first respondent who submitted that the phrase “adequate and contemporaneous records” was a composite one. In those circumstances, I do not consider the omission of the words “and reg 6” from ground 3 to be an omission of such significance as to preclude the Court considering the applicant’s challenge on the basis that the Committee misconstrued regs 5 and 6 in terms of its approach to what standard Dr Sevdalis was required to meet in order to keep “adequate and contemporaneous” records of the services he provided.
95 Insofar as the applicant makes a distinction between what is meant in reg 5(d) by the standard that a record be “comprehensible” to another medical practitioner, I accept that this imposes a standard directed to something other than accessibility. It is about whether the record is adequate for the purposes of enabling another medical practitioner to understand the patient’s clinical history and past treatment sufficiently well that she or he can effectively treat the patient. “Adequate” in this context must, it seems to me, include whether the record contains enough information, and whether the information it contains is expressed and recorded in a way that a medical practitioner accessing it for the first time can understand and apply the information.
96 Accessibility, in contrast, concerns where a record is kept, in what form it is kept, and how it can be retrieved.
97 However, in neither of the representative examples relied upon by the applicant does the Committee deal with accessibility or availability of the records by reference to reg 5(d). In other words, the Committee clearly did not misunderstand reg 5(d), or put a gloss on it.
98 Rather, the Committee’s focus was on the standards set out in reg 6(a) and (b), both of which concern the timeliness of records made by a practitioner measured against the time at which a service was provided. Timeliness in making a record of what occurred during the provision of a service is no doubt important for reasons of maximising accuracy and ensuring that, if further treatment is required, past treatment is ascertainable. Further treatment for a patient may be required very soon after past treatment. It may be required when the medical practitioner who provided the past treatment is not available. It may be required by a different medical practitioner because of a choice made by the patient about where to go for treatment. Numerous other examples could be given.
99 In the approach it took to reg 6(a) and (b) and the standard of timeliness of record making, I can see no construction error in the Committee’s approach. It examined the chronology on the evidence before it and made findings of fact about the gaps in time between when a service was provided and when a record of that service was entered by Dr Sevdalis. Having done that, it found that the standard of timeliness had not been met, and it explained its reasoning by the proposition (self-evidently, in my opinion) that during the gap, the records would not have been available to another practitioner. As I have noted, there can be no doubt that at least part of the reason for this standard is precisely that. In my opinion, the reference by the Committee in [79] of its report to the question whether the records were “readily accessible” is to be understood in the same way, and does not involve any legal error in the construction of regs 5 or 6.
100 The applicant sought to further develop this ground by submitting that also inherent in this approach was a further gloss by the Committee: namely that the record had to be an electronic one, and that is all the Committee assessed for the purpose of deciding whether Dr Sevdalis had met the standards of adequacy and contemporaneity set by regs 5 and 6.
101 There was some initial attraction to this submission, as it does indeed appear to be the case that the Committee’s fact finding on the consideration in s 82(3) revolved around an assessment of Dr Sevdalis’ electronic records. However, I am satisfied the first respondent’s submissions answer the matter satisfactorily. The first respondent submitted that in answer to the notice to produce issued to Dr Sevdalis by the Committee, what Dr Sevdalis produced were predominantly electronic records. The transcript of the Committee hearing, which was in evidence, shows that to be the case. In other words, Dr Sevdalis did not produce, as his primary source for his records, handwritten notes. Rather, his evidence was that where he took handwritten notes, he sought to transfer these to the computer system but his evidence was that there were some delays, and some problems with doing this, in part because of his unfamiliarity with the electronic records system he was required to use.
102 In terms of handwritten notes, Dr Sevdalis produced four specific handwritten notes, upon which he relied for four services, and these were found by the Committee to have been fabricated. That finding is not challenged in this proceeding.
103 Separately, and in response to the Committee’s draft report, Dr Sevdalis submitted a number of letters from his colleagues and employees in his medical practice regarding his use of handwritten notes and paper files, whether they were considered accessible within the practice, and whether Dr Sevdalis’ record keeping caused any difficulties in patient care (the letters asserted it did not). At [78] of its report the Committee decided it could not give substantial weight to this evidence:
These letters were provided to the Committee after the hearing had ended and without leave to provide them as further evidence in the proceedings. Nevertheless, the Committee has had regard to them. However, without an opportunity to examine the persons purported to have written these letters, and noting that they are all current employees of Dr Sevdalis, the Committee does not give their evidence much weight.
104 That was a determination within the Committee’s authority and was not challenged in this proceeding. The Committee went on to explain some further difficulties it found existed with Dr Sevdalis’ handwritten notes in other respects related to his record keeping:
It is noteworthy that Dr Haralambakis indicated that he had some difficulties accessing the paper records from time to time, for which he needed the assistance of staff. In addition, while he stated that he had no problems with continuity of care, It [sic] was his service that was compromised by Dr Sevdalis’ failure to include his clinical notes in a timely manner in the patient record in relation to service 27 in Appendix 3.
It would appear from the curious way in which clinical notes were transcribed into the computer system that they were often not transcribed in any apparent date order, but transcribed somewhat randomly and many months and sometimes over a year after the event, and often not transcribed on the same occasion, but weeks or months apart. This tends to suggest that the paper records were kept loosely, out of sequence, and not in the same place. Consequently, it would have been very difficult to obtain an adequate and reliable history from the paper file clinical record.
The Committee also notes that Dr Sevdalis could not provide any notes in relation to a number of the services considered by the Committee. This indicates either that there was no systematic approach to filing handwritten notes, or that he did not write any notes for those attendances. The lack of a systematic approach is borne out by the different explanations that Dr Sevdalis gave throughout the hearing regarding how he kept his handwritten notes.
The Committee does not accept that the handwritten clinical notes, if they were, in fact, made contemporaneously to the consultation, would have been readily available to the other practitioners in the practice.
(Footnotes omitted.)
105 These are the kinds of findings, both at the level of fact and professional opinion, that a Professional Services Review Committee is entitled to make in coming to a conclusion about whether a practitioner has engaged in inappropriate practice within the meaning of s 82(1) of the Act. The Committee’s findings in this section of its report are not expressed to be confined to the terms of regs 5 and 6 of the Professional Services Review Regulations. Rather, they form part of the Committee’s broader assessment for the purposes of s 82(1).
106 I do not consider that these parts of the Committee’s report provide any support for the applicant’s contention that the Committee approached its task by construing regs 5 and 6 to require that electronic records be kept.
107 In accepting these submissions, I should not be taken to accept a different submission put by the first respondent. In his written submission, the first respondent submitted that where reg 6 requires that a record be “completed”, this should be taken to mean transferred from a handwritten to an electronic form. I do not accept that submission. The regulations say nothing about electronic data entry, just as they say nothing about handwritten entries. The standard is silent about the form of the record (whether electronic, typed or handwritten). That is presumably because of the myriad of circumstances in which medical practitioners may find themselves having to provide treatment, and the variety of resources available to practitioners depending on the nature and circumstances of their practices. Adequacy and contemporaneity can be achieved just as readily through a handwritten note as an electronic one, although whether the standard is met or not for a given service will depend on an evaluative assessment of that particular service. Illegible handwriting, for example, may render a record incapable of meeting the adequate standard in reg 5. Incompetent typing may do the same for an electronic one.
The Committee’s construction of MBS items 37 and 5043 (grounds 5 and 6)
108 MBS items 37 and 5043 concern professional attendances at a place other than consulting rooms, a residential aged care facility, or, in the case of item 5043, a hospital. The requirements for each item are set out in the general medical services table prescribed annually in regulations, which I have extracted at [38] above.
109 The applicant’s key submission was that the Committee misconstrued both items by imposing or reading into them a requirement that there be a clinical need for the consultation to occur at a place other than consulting rooms, or an aged care facility, or, in the case of item 5043, a hospital. That submission relied on the proposition that the description in both items said no such thing. What it said was that the activities in subparagraphs (a) to (e) in each item needed to be “clinically relevant”. There was, the applicant submitted, no indication in the terms of either item 37 or item 5043 that the medical practitioner needed to have a clinical justification for the location of the attendance, as opposed to a clinical justification for what she or he did during the attendance.
110 The applicant developed this submission by contrasting the text of items 37 and 5043 with the text of other items in the 2011 GMS Table Regulations, such as items 597 to 600 (found in Div 2.15 of Sch 1 to those regulations) which dealt with urgent attendances after hours. In each of those items, a claim can be made by a medical practitioner if the patient’s medical condition “requires urgent treatment”. Regulation 2.15.1 sets out what circumstances must exist for a patient’s medical condition to “require urgent treatment” :
Meaning of patient’s medical condition requires urgent treatment
(1) For items 597 to 600, a patient’s medical condition requires urgent treatment if:
(a) medical opinion is to the effect that the patient’s medical condition requires treatment within the unbroken after-hours period in, or before, which the attendance mentioned in the item was requested; and
(b) treatment could not be delayed until the start of the next in-hours period.
(2) For subclause (1), medical opinion is to a particular effect if:
(a) the attending practitioner is of that opinion; and
(b) in the circumstances that existed and on the information available when the opinion was formed, that opinion would be acceptable to the general body of medical practitioners.
111 It can be seen that not only must the medical practitioner herself or himself form a particular opinion, that opinion must be one that is justified in the eyes of the general body of medical practitioners (such assessment being part of the Committee’s function).
112 The applicant also points to the characterisation of items such as item 37 and item 5043 in the Medicare Benefits Schedule Book, relevant extracts of which were in evidence on this review. In an affidavit relied upon by the first respondent, the Book is described as a “Booklet” that is “published annually by the Department of Health and Ageing and used generally by the medical profession for information and guidance about Medicare service items prescribed under the Act”. As such, it does not have legal force and provides information and guidance only regarding rights and obligations the source of which is to be found in the relevant legislation, in particular the Act and the applicable regulations setting out the General Medical Services Table.
113 In the Book, items 37 and 5043 are described as “non urgent attendances”. The text of the book does not suggest any evaluative aspect to services claimed under these items, in contrast to the way it describes an “urgent attendance”. However, given the role of the Book, I am not persuaded this takes the applicant’s argument any further than the text of the regulations themselves.
114 The first respondent’s answer to this ground is to focus on the phrase “clinically relevant” in the text of each item. He does so by reference back to the definition of “clinically relevant service” in s 3 of the Act, which I have extracted at [41] above.
115 In my opinion, this submission involves a conflation of the defined term in s 3(1) and the text of items 37 and 5043 as set out in the regulations. The text in the items does not use the defined term “clinically relevant service”. Indeed, the adjectival phrase “clinically relevant” in the regulations relates not to the “service” as a whole, but to the five activities set out in each item. It is one of more of those activities which must be “clinically relevant”. In my opinion that means one or more of those activities (such as performing a clinical examination) must be relevant, in a clinical sense, to one or more of the “health related issues” a patient had at the time of the attendance.
116 There is simply nothing in the text or context of the regulations dealing with items 37 and 5043 which supports a construction of these items making it part of the Committee’s task to decide whether, in the Committee’s opinion, a “home visit” was justified.
117 Yet that is the analysis the Committee undertook. This is apparent from a number of entries in its report in which the Committee responded to Dr Sevdalis’s explanations regarding particular home visits (which I do not extract as they may identify the patient), examples of which include:
The Committee still does not understand why this patient could not have been seen at the clinic …
…
The Committee does not accept that this patient could not have attended the clinic.
118 An example of the Committee’s approach as reflected in the appendices can be found in the following extract from appendix 3 (which deals with services claimed by Dr Sevdalis under item 5043) (with redactions to avoid identifying details of the patient):
119 In all these instances, and others relied on the by the applicant in his submissions, the Committee is clearly reading into each of item 37 and item 5043 a requirement which is not there: namely, that the location of the attendance (i.e. out of the consulting rooms) must be necessary and justifiable, and (it appears the Committee considered this was also required) that the notes of the attendance should, contemporaneously, record the justification at a level of detail considered by the Committee to be sufficient.
120 The items do not require any such necessity or justification. Rather, in their text they require, at a factual level, a consultation of a certain duration (lasting at least 20 minutes), and a specific time of day (in usual hours for item 37, after hours for item 5043). The items also require the medical practitioner to have performed at least one of the five specified activities, which are to be clinically relevant to the patient’s health related issues as the patient presented at the time. Each of these requirements must be appropriately documented.
121 Unlike items 597 to 600, read with reg 2.15.1, the regulations do not require, or authorise, the Committee to engage in any evaluative exercise about whether in its opinion the attendance at a location other than the consulting rooms was justified. Nor do they authorise or require the Committee to engage in the function of determining whether the justification is one which would be acceptable to the body of medical practitioners the Committee represents.
122 The first respondent’s invitation to focus on the requirement in the item descriptions for there to be “appropriate documentation” for the attendance does not alter my opinion. The documentation required by this item description is documentation which is appropriate to describe the “health related issue” the patient was experiencing, which activity or activities of the five specified activities were performed by the medical practitioner during the attendance, and some indication of why that activity was “clinically relevant” to the health related issue.
123 Nevertheless, the first respondent is correct to submit that in each case in which a medicare benefit is claimed, a medical practitioner must meet the two requirements in the definition of “professional service” in s 3(1) of the Act in order to be entitled to the benefit as claimed under s 10. That means, as the first respondent submits, that for each service rendered and for which a medicare benefit is claimed, the service must be a clinically relevant service. This in turn imports an evaluative standard, as the terms of the definition of “clinically relevant service” in s 3(1) make clear. A Committee investigating a practitioner must, as part of its function, form a view whether the service rendered was one “generally accepted in the medical … profession … as being necessary for the appropriate treatment of the patient to whom it is rendered”.
124 The “service”, for the purposes of this assessment (and for the purposes of a practitioner’s entitlement), is a service “to which an item relates” under the regulations: see the definition of “professional service” in s 3(1) of the Act. Applying that to items 37 and 5043, the during hours and after hours attendances by Dr Sevdalis at places other than his consulting rooms or an aged care facility (or a hospital, in the case of item 5043) were, by the definition of “professional service” read with the definition of “clinically relevant service” in s 3(1) of the Act, required to be a service that was one “generally accepted in the medical … profession … as being necessary for the appropriate treatment of the patient to whom it is rendered”.
125 In some circumstances, an assessment of whether that requirement was met may touch upon some of the matters which were (in my opinion, wrongly) considered by the Committee in relation to item 37 and item 5043. Nevertheless, it remains the case that, looking at all the instances in which the Committee made an assessment, its approach introduced a gloss, or a consideration of a nature different to that required, by examining in quite an absolute way whether a patient “could have” gone to Dr Sevdalis’ consulting rooms. On no view, in my opinion, is the evaluation to be conducted at that absolute level. Even within the terms of the two definitions in s 3(1), the evaluation is what kind of attendance is “necessary for the appropriate treatment” of a patient. That is not an evaluation to be conducted in hindsight, perhaps years later, but on the information available to the practitioner at the time and it should not, in my opinion, be conducted by a Committee asking itself whether a patient “could” have gone to the surgery, even on the information available at the time. Rather, the correct question is whether a during hours or after hours service was, on the information available to the medical practitioner at the time, “necessary for the appropriate treatment of the patient to whom it is rendered”, and generally accepted in the medical profession to be so. In my opinion “necessary” imports a standard at the level of there being no reasonable alternative in the circumstances. It does not suggest the Committee should determine whether it was physically possible for a patient to have attended during hours or at the practitioner’s consulting rooms, which in my opinion is the standard the Committee seems to have applied.
126 In conclusion, in my opinion the applicant is correct in his contention that the Committee misconstrued MBS items 37 and 5043. There is no doubt on a reading of the Committee’s report that it made the findings it did, which I have identified at [117]-[118] above, solely because of how it understood the requirements in these items. In each specific case, the Committee’s analysis appears under the heading “MBS Item Descriptor”, and is thus directly linked to the item description in the regulations. In the body of its report, the Committee’s analysis is also directly linked in this way from [85] onwards.
127 However, that conclusion does not mean the applicant’s ground of review should be upheld. There is an earlier part of the Committee’s report which looks at Dr Sevdalis’ claims for these services through the prism of s 10 and the two definitions in s 3(1) of the Act. That analysis appears at [62]-[67] of the Committee’s report.
128 At [64], the Committee said:
One of the requirements is that “each entry provide clinical information adequate to explain the type of service rendered or initiated”. This requirement means that the record needs to explain the clinical reasons for providing the particular MBS item that was provided rather than some other MBS item. That is, for a home visit, it must explain what the clinical indications or reasons were for a home visit being required to be undertaken, and why the attendance needed to be undertaken at the particular time, if outside usual hours. If it was an MBS item that has a minimum time requirement, the clinical notes need to explain why the practitioner needed to spend at least that amount of time attending to the clinical needs of the patient on that occasion. Medicare benefits are paid at higher rates for services performed outside usual hours or as home visits, or for services that take a longer time to perform than a standard consultation. Such services are not to be funded by the Commonwealth unless there are clinical reasons for them to be provided.
129 For the reasons I have set out above in relation to regs 5 and 6, I do not consider that the regulations require what the Committee asserts in this passage. Those regulations do not require the recording of information by way of justification for the location of the attendance. They require recording of what was done, and, clinically, why it was done. This is another example of the Committee imposing a gloss, and a higher threshold, on the information a practitioner must either record, or otherwise demonstrate, under the regulations.
130 Then, at [65] the Committee addressed the s 10 and s 3(1) requirements of “professional service”, together with submissions made on behalf of Dr Sevdalis:
This is further supported by the requirement in the Act that Medicare benefits are payable only in respect of a “professional service” that is a “clinically relevant service”. This means that the particular service rendered must be a service that is generally accepted in the medical profession as being necessary for the appropriate treatment of the patient. If it was not necessary to conduct a home visit for the treatment of the patient, then it was not a clinically relevant service and was not eligible for the payment of a Medicare benefit. Consequently, a practitioner needs to document the clinical information adequate to explain the type of service rendered, which in respect of home visits should include the fact that it was a home visit, and the reason for having to go to that particular location on that occasion to attend to the patient. For after-hours visits, it should indicate when the attendance occurred and the clinical reasons for needing to attend to the patient at that time. For minimum timed services, the clinical record should record the actual time spent and indicate the clinical reasons for spending at least the minimum amount of time for the MBS item billed.
131 I am not entirely persuaded that the Committee fixed the correct threshold in this passage: “necessary to conduct a home visit for the patient” and “necessary for the appropriate treatment of a patient” may not set quite the same standard, the former tending to be more absolute. The former was, in my opinion, the standard the Committee applied in assessing Dr Sevdalis’ services.
132 In reviewing the reasoning of an administrative decision maker, courts have been reminded not to over-scrutinise that reasoning, nor to parse it, nor to separate it from its context: Minister for Immigration and Ethnic Affairs v Wu Shan Liang [1996] HCA 6; 185 CLR 259 at 271-2 (Brennan CJ, Toohey, McHugh and Gummow JJ). The written reasoning of an administrative decision maker, especially decision makers who are not legally trained, must be read fairly. ‘Fairness’ in this context includes reading the reasoning as a whole, because it is only by doing so that a reviewing court can gain a balanced appreciation of how the decision maker understood and applied the statutory concepts in issue.
133 Approaching the Committee’s report in that way has led me to conclude that, despite its erroneous interpretation of the requirements of MBS items 37 and 5043, it was substantially correct also to consider the requirements of s 10 of the Act, read with s 3(1). The latter are the most fundamental prerequisites to entitlement to a medicare benefit for a service. Although it is possible that, even in assessing Dr Sevdalis’ conduct against this requirement, the Committee took too absolute an approach, I am not persuaded on the balance of probabilities this was the case.
134 Accordingly, these grounds are not made out because, although the Committee’s approach was legally erroneous in relation to its interpretation of items 37 and 5043, its decision can (and was by the Committee itself) supported by another requirement in the Act: see Eastman v Commonwealth Director of Public Prosecutions (ACT) [2003] HCA 28; 214 CLR 318 at [124] (Heydon J); Australian Education Union v Department of Education and Children’s Services [2012] HCA 3; 248 CLR 1 at [34] (French CJ, Hayne, Kiefel and Bell JJ); Attorney-General (SA) v Corporation of the City of Adelaide [2013] HCA 3; 249 CLR 1 at [175] (Crennan and Kiefel JJ).
Whether the Determining Authority made directions which were punitive and not protective (grounds 7, 8 and 9)
135 These grounds challenge the Determining Authority’s decision, rather than the Committee’s report. One of the grounds (ground 9) was not the subject of any oral submissions, and both parties relied on their written submissions. The applicant’s contention in ground 9 is that the Determining Authority went beyond simply taking into account the fact that Dr Sevdalis was the subject of a previous final determination in 2004, in which sanctions were imposed on him. Instead, the Determining Authority’s reasons indicate it sought to punish the applicant again for that conduct. The applicant relies on the following passage from the Determining Authority’s reasons:
The Determining Authority is of the view that inappropriate conduct can place patients at risk and that the directions in this determination are proportionate to the inappropriate conduct found by the Committee and also the previous conduct of Dr Sevdalis as set out in the previous final determination. Any possible adverse consequences to the patients of Dr Sevdalis of a disqualification may be managed by Dr Sevdalis’ patients for the period of the disqualification.
136 This passage could have been expressed differently by the Determining Authority. On its face, it could be seen as having the effect for which the applicant contends. However, in my opinion in this passage the Determining Authority is reflecting on the protective purpose of Pt VAA, and on its sanctions power in particular. In doing so, it was open to the Determining Authority to take into account that this was not the first time Dr Sevdalis had been sanctioned under the Health Insurance Act, thus increasing the need for further specific deterrence, and a longer period of disqualification in order to reduce the risk he might engage in similar conduct in the future. In this passage the Determining Authority did so expressly on the basis of its view about a possible risk to patients, and this aspect of its reasoning was not challenged by the applicant on judicial review.
137 Ground 9 is not made out.
138 Grounds 7 and 8 challenge the cumulative imposition of sanctions by the Determining Authority under each and every relevant category available to it in s 106U(1). Counsel for the applicant referred to the “devastating” impact the direction to repay $453,656.75 would have on Dr Sevdalis, as well as the lengthy period of disqualification entirely from receiving medicare benefits. Counsel emphasised that none of the contraventions related to general consultations (item 23) and there was no need for the Determining Authority to remove Dr Sevdalis’ entitlement to medicare benefits for general consultations, when all the impugned services had been of other kinds.
139 Although at times during oral argument counsel for Dr Sevdalis disclaimed this, it seems to me the challenge involved in these grounds was based on an absence of reasoning by the Determining Authority as to why it had imposed the directions it had.
140 The applicant submitted the Determining Authority “never considered why a full disqualification from the MBS was necessary to satisfy the protective purpose of the scheme”, in circumstances where the Applicant had provided detailed submissions explaining a change in circumstances between the review period and the future. He contended his case had “some extraordinary mitigating circumstances”, but there was no analysis or assessment of the future risk of inappropriate practice by the Determining Authority in its reasons.
141 He also submitted that the Determining Authority “never considered” why a partial disqualification (from receiving medicare benefits in respect of certain item numbers) was not sufficient to satisfy the protective purposes of the scheme. It is important to recognise that the Committee did not review all services provided by the applicant during the review period, but only those under certain item numbers (such as off-site, after hours and care plans). Preventing the applicant from providing services under those item numbers, by limiting him to standard consultations only (item 23), could have neutralised any concern about his misuse of those item numbers in the future. Relying on Quinn v Law Institute of Victoria Limited [2007] VSCA 122; 27 VAR 1, the applicant submitted the Determining Authority was bound to consider this, but it did not.
142 The submission that the Determining Authority “never considered” why a full disqualification was appropriate and a partial disqualification was inappropriate, particularly given the tragic personal circumstances experienced by Dr Sevdalis and outlined to the Determining Authority, is put too high. The Determining Authority’s reasons make it plain the Determining Authority was aware of, and took into account, those circumstances. Similarly, it cannot be said the Determining Authority “never considered” why a partial disqualification would not satisfy the scheme’s protective purpose. This was Dr Sevdalis’ submission and the Determining Authority took that submission into account.
143 What is missing from the Determining Authority’s reasons, however, is any substantive examination of why it made the directions it did, in preference to the directions Dr Sevdalis contended would be appropriate (or any other directions for that matter). Its reasons are largely conclusory.
144 Such an approach can be criticised as less than best practice – it does not inform Dr Sevdalis, as the affected practitioner, why his submissions were so roundly rejected, nor does it inform a reviewing court as to why the Determining Authority reached the conclusions it did. Both are left to piece together a few observations made earlier in the Determining Authority’s reasons (such as those at [23]-[29] of its reasons) and infer that these were the matters the Determining Authority then decided weighed strongly in favour of full disqualification (and full repayment.
145 Nevertheless, such a criticism of the way the Determining Authority has expressed its reasoning process is not the same as a conclusion that it misunderstood its task and was intent on punishing Dr Sevdalis, rather than making directions it was satisfied would give effect to the protective purposes of the legislative scheme. While in parts of its reasons, it is critical of Dr Sevdalis, those criticisms are generally couched in the context of the Determining Authority explaining why the shortfalls in Dr Sevdalis’s behaviour may pose a risk to patients. An example is [28] of its reasons:
The importance of clinical records in the management of patient care should not be understated. The inadequacies of Dr Sevdalis’ clinical records adversely affect his ability (and the ability of other practitioners) to provide effective and adequate care to his patients. The Committee’s finding is indicative of the importance and value that the profession places on clinical records.
146 In Trade Practices Commission v CSR Ltd [1990] FCA 521; [1991] ATPR 41-076, French J (as his Honour then was) made the following observations regarding the distinction between punishment imposed for breaches of the criminal law and civil penalties imposed for statutory contraventions that are not criminal offences:
Punishment for breaches of the criminal law traditionally involves three elements: deterrence, both general and individual, retribution and rehabilitation. Neither retribution nor rehabilitation, within the sense of the Old and New Testament moralities that imbue much of our criminal law, have any part to play in economic regulation of the kind contemplated by Pt. IV [of the Trade Practices Act 1974 Cth)]. … The principal, and I think probably the only, object of the penalties imposed by s.76 is to attempt to put a price on contravention that is sufficiently high to deter repetition by the contravenor and by others who might be tempted to contravene the Act.
147 His Honour’s comments were recently cited with approval by a plurality of the High Court in Commonwealth v Director, Fair Work Building Industry Inspectorate [2015] HCA 46; 90 ALJR 113 at [55], with their Honours going on to state at [59] that “civil penalties are not retributive, but like most other civil remedies essentially deterrent or compensatory and therefore protective”.
148 Those cases deal with statutory contexts that differ from the Professional Services Review Scheme provided for by Pt VAA of the Health Insurance Act, but they demonstrate that civil sanctions may be imposed for purposes that include general and specific deterrence without necessarily straying into retribution, which is better seen as the province of criminal punishment. That those principles apply in the context of the Scheme can be seen from decisions such as Mukherjee v Medicare Participation Review Committee [2010] FCA 233; 114 ALD 148, in which Cowdroy J said that sanctions under an earlier version of the Scheme were “primarily intended to ensure the integrity of the Scheme’s operation and [are] not to be seen as a form of penalty or punishment simpliciter” (at [27]) but could “include an element of deterrence” (at [31]).
149 I am not satisfied that it would be correct to characterise the Determining Authority’s reasoning as punitive. Further, although this language does not appear in the Determining Authority’s reasons, in my opinion the Determining Authority was conscious of a need to deter both Dr Sevdalis and other medical practitioners from engaging in what it clearly regarded as significantly poor record keeping of attendances on patients, and poor clinical practice in terms of how Dr Sevdalis carried out his responsibilities as a medical practitioner. That it was not more sympathetic to Dr Sevdalis’s own personal situation may reflect one of the attributes of peer review. No doubt many medical practitioners know what it is like to balance a very demanding and responsible profession with life experiences. It may be that some peer reviewers are less sympathetic than might be expected to practitioners who are unable to maintain that balance. Whatever the case, it is not possible to identify from the reasons why there was not more sympathy for Dr Sevdalis’s situation. But the fact there was less sympathy than other minds might have brought to the decision is not a legal error. The issue was within the judgment and discretion of the Determining Authority.
The Determining Authority’s repayment direction (grounds 7.1.2, 10 and 11)
150 These grounds concern the way the Determining Authority calculated the amount the applicant would be directed to repay. It is true, as the applicant submitted, that the terms of s 106U gives the Determining Authority a discretion as to the amount a practitioner should be required to repay, and it need not be the entire amount of the medicare benefits paid for services the Committee has found were the subject of inappropriate practice.
151 The applicant did not challenge the use by the Committee of the sampling regime available to it under s 106K. His submissions before the Court emphasised that the sample size was small: 3.1% of item 37 services; 1.8% of item 597 services; 1.8% of item 5043 services; and around 9% for item 721 services (although only four of the latter services were examined because the remaining 24 in the sample were subject to a concession by Dr Sevdalis). That may be, but in the absence of any challenge to the methodology the sample size is no evidence of legal error.
152 Accepting that his is a challenge to an exercise of discretion by the Determining Authority, the applicant’s contention focuses on the failure by the Determining Authority to examine each of the sampled services (i.e. all 27 or 28 in each class) and to consider whether, in relation to each of those examined services, it was appropriate to require a full repayment depending on the problems identified. For example, it was submitted that, in the case of items 37 and 5043, the Determining Authority could have required repayment by Dr Sevdalis of only the additional amount payable for each home visit over the amount payable for a standard consult – in other words, that since Dr Sevdalis delivered treatment during an attendance, he should be allowed to retain that portion of the medicare benefit for that attendance that would have been payable had it occurred in his consulting rooms. The applicant submitted this approach was especially significant for the item 721 services in relation to management plans: if the management plans prepared by Dr Sevdalis were deficient only in limited areas (given the concession by Dr Sevdalis about two aspects of the plans was accepted by the Committee), then repayment should not be of the whole benefit paid because the patient otherwise derived a benefit and the service was otherwise performed.
153 All of these submissions may be persuasive submissions to the repository of the exercise of the discretion. I do not accept that the repository’s response to them in this case indicates any legal error.
154 The legal error relied on by the applicant is the failure to take into account a relevant consideration, and the matters which I have set out at [152] above are said by the applicant to be the kinds of considerations the Determining Authority was required to take into account.
155 That submission conflates a matter which the Act expressly or impliedly requires that a decision maker take into account with evidence before a decision maker which the decision maker has not, or has not sufficiently, dealt with in her or his reasoning: see Telstra Corporation Ltd v Seven Cable Television Pty Ltd [2000] FCA 1160; 102 FCR 517 at [131]-[136] per Beaumont, Moore and Gyles JJ; Rezaei v Minister for Immigration and Multicultural Affairs [2001] FCA 1294 at [57] per Allsop J; Paul v Minister for Immigration and Multicultural Affairs [2001] FCA 1196; 113 FCR 396 at [78]-[79] per Allsop J (with whom Heerey J agreed).
156 Insofar as the applicant identifies the consideration as “the question whether the applicant ought to be required to repay all amounts paid in respect of item 721 services”, in my opinion the reasons of the Determining Authority do disclose that it considered this at a general level, even though its reasons do not record any submissions by Dr Sevdalis about the item 721 services in particular, nor do the reasons address the specific repayment of the amounts for these services. The Determining Authority said at [47]:
In balancing the inappropriate practice that was found by the Committee with that submission and those other factors mentioned above, the Determining Authority considers that a direction requiring repayment of the whole of the Medicare benefits that were paid for the proportion of the services is indicated in the circumstances.
157 Again, this reasoning is almost entirely conclusory and does little to enlighten the reader at anything but the most general level. Reasons of that kind are far from best practice, as I have noted, but in the present case I see no legal error of the kind asserted by the applicant arising from them.
158 More critically, the power of the Determining Authority to require repayment stems, in this case, from the terms of s 106U(cb)(ii), which relates to a class of services. I have extracted that provision at [51] above.
159 Given that this provision applies where there has been sampling as authorised by s 106K, its terms authorise the Determining Authority to impose a repayment direction for a “class” of services. In this case, that meant the Determining Authority was authorised to impose a repayment direction for the class of item 37 services, for the class of item 597 services, for the class of item 5043 services, and for the class of item 721 services. That is what it did. The applicant’s submission that in doing so it needed to consider whether each and every service needed to be repaid by a close analysis of the circumstances of each sampled service is not supported by the authorising provisions.
Conclusion
160 None of the grounds of review upon which the applicant relied are made out and his applications for review under the Judiciary Act and the AD(JR) Act must be dismissed. There is nothing in the evidence or submissions to suggest that anything but the usual order as to costs should be made.
I certify that the preceding one hundred and sixty (160) numbered paragraphs are a true copy of the Reasons for Judgment herein of the Honourable Justice Mortimer. |
Associate:

