
FEDERAL COURT OF AUSTRALIA
Wake Forest University Health Sciences v Smith & Nephew Pty Ltd (No 2) [2011] FCA 1002
|
VICTORIA DISTRICT REGISTRY |
|
|
GENERAL DIVISION |
VID 143 of 2009 |
|
BETWEEN: |
WAKE FOREST UNIVERSITY HEALTH SCIENCES First Applicant KCI MEDICAL AUSTRALIA PTY LTD (ACN 056 073 468) Second Applicant SMITH & NEPHEW PTY LTD (ACN 000 087 507) Cross-Claimant |
|
AND: |
SMITH & NEPHEW PTY LTD (ACN 000 087 507) Respondent WAKE FOREST UNIVERSITY HEALTH SCIENCES First Cross-Respondent KCI MEDICAL AUSTRALIA PTY LTD (ACN 056 073 468) Second Cross-Respondent |
|
JUDGE: |
DODDS-STREETON J |
|
DATE: |
30 AUGUST 2011 |
|
PLACE: |
MELBOURNE |
REASONS FOR JUDGMENT
1 The first applicant and cross-respondent, Wake Forest University Health Sciences (“WFUHS”), and the second applicant and cross-respondent, KCI Medical Australia Pty Ltd (“KCI MA”) (collectively “KCI”), own and exploit respectively the Australian Patent 674837 (“the Patent”), which is directed at treating and healing wounds unlikely to respond to conventional treatments by the use of negative pressure. Since 1996, KCI has successfully marketed in Australia wound healing kits which constitute a commercial embodiment of the Patent. In this proceeding, KCI alleges that the respondent and cross-claimant, Smith & Nephew Pty Ltd (“S&N”) has, since about 2008, infringed 14 claims of the Patent by selling, marketing and supplying wound healing kits including, inter alia, a foam dressing and vacuum pump for applying negative pressure, together with brochures and instructions for their use. S&N denies infringement and, by cross-claim, alleges that the claims are invalid on a number of grounds.
2 For the reasons set out in detail below, I have found that S&N did not infringe any of the claims (which were all combination claims consisting of multiple integers), principally because KCI failed to establish that the S&N product possessed an essential integer common to all the combination claims. The integer in question was a screen (or dressing) sufficiently rigid to prevent wound overgrowth (“screen rigidity integer”). I have found that if (contrary to S&N’s contention) the screen rigidity integer were established, the evidence advanced by KCI was inadequate to prove its presence in the S&N product. More fundamentally, the evidence, in my view, established that the integer did not have the functional operation as claimed, lacked scientific meaning and was inherently unsound.
3 As S&N acknowledged, because the essential screen rigidity integer common to all the combination claims could not be established, its challenge to the validity of the claims based on novelty necessarily failed (as the purported integer was absent from the prior art). Nor, in my view, did S&N establish that the claims were invalid on the ground of obviousness (lack of inventive step). The fundamentally flawed nature of the screen rigidity integer nevertheless, in my view, rendered all the claims invalid on the basis of failure to satisfy the requirements of ss 40(2) and (3) of the Patents Act 1990 (Cth) (“the Act”) that, inter alia, they be clear and sufficient, as, despite the evidence of KCI’s expert witnesses, the evidence as a whole established that the skilled addressee would attribute no meaning to the integer. This was thus a rare case where fundamental lack of clarity in an essential integer rendered the claims invalid.
4 WFUHS is the proprietor of the Patent, which is described in more detail further below (see [33] to [67]) and briefly summarised here. KCI MA is the exclusive Australian licensee of the invention, which carries out its commercial exploitation.
5 In summary, the invention includes both a medical apparatus and a method for applying negative pressure to wounds which are unlikely to heal completely or at all by the use of conventional means.
6 The Patent is entitled “Method and Apparatus for Treating Tissue Damage”. It has a total of 123 claims in all and 18 independent claims, directed to the five aspects of the invention. The 14 claims in suit are all combination claims with multiple integers. They relate to either of two aspects of the invention, namely a method of treatment or an apparatus. At the outset, there were 40 claims in suit, which expanded to 70, reduced to 16, and ultimately reduced to the 14 claims remaining in issue.
7 The invention was made at Wake Forest University in North Carolina, USA by Dr Louis Argenta, a plastic surgeon, and Dr Michael Morykwas, a bioengineer.
8 The Patent has a priority date of 14 November 1991 (subject to S&N’s cross-claim discussed below, which alleges a deferred priority date of 7 November 1996).
9 The Patent results from an application under the Patent Co-operation Treaty (“PCT”) no. PCT/US92/09649 filed on 12 November 1992, claiming priority from US Application No. 792001, filed on 14 November 1991. (By s 88 of the Act, the PCT application is treated as a complete application for a standard patent). As filed, the specification had 52 claims.
10 When the application was examined by the Commissioner of Patents, the Examiner, pursuant to s 45 of the Act, reported that “there are lawful grounds of objection to… the complete specification”, because, broadly, specified claims did not define the invention as described. Thus, while the specification, as a whole, indicated that a “screen means” or dressing, made of material sufficiently porous to allow oxygen to reach the wound and sufficiently rigid to prevent wound overgrowth, was part of the invention, the claims did not include that feature.
11 On 10 October 1996 and 7 November 1996, following the Examiner’s report, the patentee included new claims and made amendments pursuant to which all the claims in suit refer to a screen means sufficiently porous to allow oxygen to reach the wound and sufficiently rigid to prevent wound overgrowth.
KCI product: V.A.C.® Therapy System
12 KCI’s commercial embodiment of the invention the subject of the Patent is the V.A.C.® Therapy System, an apparatus produced and marketed under the trademark “V.A.C.” It is a system of negative pressure wound therapy (“NPWT”). The product comprises a vacuum pump and a foam dressing kit, which includes a foam dressing (referred to in the Patent as a “screen means”), adhesive plastic films or drapes (referred to in the Patent as the “seal”), and connector tubes. KCI launched the V.A.C.® Therapy System worldwide (including Australia) in 1996 and has produced, promoted and marketed the product since that date. Broadly, although there are some variations, the V.A.C.® product is applied as follows:
(a) the foam dressing (screen means) is first cut to fit the size and shape of the patient’s wound (or “defect”) and placed in the wound;
(b) the adhesive film (“seal”) is placed over the dressing, extending beyond it, and adheres to the patient’s healthy skin on the periphery of the wound;
(c) the connector tubes (which have small perforations at the insertion end) are inserted into the foam dressing and connected to the vacuum pump, and hence to the wound; and
(d) when the vacuum pump is switched on, it results in the application of negative pressure (colloquially, suction) to the wound.
13 The V.A.C.® kits come with different sizes (small, medium and large) of foam dressing which is, in any event, cut to fit the size and shape of the wound being treated.
14 The treatment of a large wound using the KCI kit with a plastic film seal was demonstrated to the court by a film taken by Dr Pohl, an expert witness called by KCI.
15 KCI MA has a sales turnover of approximately AUS$25 million per annum, approximately 98% of which is attributable to the KCI V.A.C.® Therapy System.
16 Following its introduction to Australia, the V.A.C.® Therapy System has been used by relevant sectors of the medical profession in Australia for wound management in appropriate cases.
17 It was not disputed, and all expert witnesses attested, that the application of the therapy has had a positive impact on the treatment of wounds that are difficult to treat by conventional methods and significantly improved patient care and outcomes.
18 S&N is the largest wound care company in Australia. It is a subsidiary of a large multinational medical device and consumables company that supplies devices (including prosthetic joints, orthopaedic screws, pins and fixing devices), surgical equipment and wound dressings.
19 In May 2008 (about 12 years after KCI launched its product in Australia and worldwide), S&N launched two NPWT kits for applying negative pressure to wounds under the names “VISTA” and “EZCARE” in the Australian market. Initially, the S&N kits contained gauze, rather than foam, as the dressing (or screen means). Although some claims in suit (the method claims) do not specify that the screen means be foam, KCI does not allege that S&N kits containing gauze infringe the Patent. In about December 2008, however, S&N introduced kits which included foam for the screen means or dressing. KCI alleges that the S&N foam kits infringe specified claims of the Patent.
20 In June 2009, KCI obtained an interlocutory injunction restraining S&N from selling or disposing of its kits on the basis of its alleged infringement of claim 49 of the Patent: see Wake Forest University Health Sciences & Anor v Smith & Nephew Pty Ltd (2009) 81 IPR 530. On appeal, as discussed below, the Full Court set aside the injunction, holding that claim 49 (because it included an aseptic package which, while an essential integer, did not interact purposefully and functionally with the other integers) was invalid as a mere collocation: see Smith & Nephew Pty Ltd v Wake Forest University Health Sciences & Anor (2009) 82 IPR 467 (“Wake Forest”).
21 The S&N NPWT system consists of:
(a) a vacuum pump (VISTA, RENASYS EZ, RENASYS GO and EZCARE);
(b) a foam dressing kit (RENASYS-F) which includes a foam dressing with a channel in the top where the drain tube is located, adhesive plastic films (drapes) and a connector tube or tubes perforated at one end; and
(c) a foam dressing kit (RENASYS-F/P) which includes a foam dressing, adhesive plastic films (drapes) and connector tubes, which differs from the RENASYS-F in that the tube is connected to the foam by a central, disc-shaped pad which does not pierce the film. (The RENASYS-F/P is not alleged to infringe claims 50 and 52 of the Patent).
22 S&N’s foam dressing kits are intended to be used in conjunction with S&N’s vacuum pumps (which were either available prior to the introduction of the foam dressing kits or accompanied their introduction) in order to deliver negative pressure to the wound to promote wound healing. On visual inspection, unlike foam in the KCI kits, the foam in the S&N kits (other than the RENASYS-F/P) has a channel in the top where the drain tube (perforated at one end) is located. S&N markets its NPWT systems with brochures and instructions explaining the intended use of S&N’s vacuum pumps and foam dressing kits. Some of the S&N devices have one tube while others have two, which can be connected to each other to provide more space. It was not disputed that, broadly speaking, the S&N foam dressing kits are applied and operated in the same way as the V.A.C.® kits.
23 S&N published user guides for its “EZCARE”, “VISTA”, “RENASYS EZ” and “RENASYS GO” vacuum pumps, an instruction sheet for the “RENASYS-F” foam dressing kit and a report of an expert panel meeting held in February 2009 regarding NPWT.
24 The user guides for each S&N product are similar to one another. All user guides state that the device may promote wound healing, and that it is appropriate for use on a range of wounds, such as pressure ulcers and traumatic wounds. The guides set out steps for dressing a wound and indicate that the wound dressing or sealing kit should be changed 48 hours after the initial application of therapy.
25 The guides provide instructions for the selection and installation of a canister kit, and methods for operating the device. Each states that there are two modes of operation: constant/continuous and intermittent. In the intermittent mode, the device alternates between periods of active suction and periods of no active suction. The guides state that “constant [or continuous] mode is recommended for NPWT”.
26 The guides also provide advice on, inter alia, issues such as troubleshooting, maintenance, cleaning and storage of the device.
27 While the EZCARE and VISTA user guides refer only to gauze dressing, the RENASYS EZ and RENASYS GO guides provide instructions on the application of both gauze and foam dressing, while indicating that foam dressing may not be available in all markets.
Instruction sheet for RENASYS-F foam dressing kit
28 The instruction sheet states that the RENASYS-F foam wound dressing kit is intended to be used in conjunction with the S&N NPWT systems. The kit is intended for use on various wounds, including chronic, acute and traumatic wounds.
29 The instruction sheet sets out warnings and precautions for the use of the device. It includes a warning not tightly to pack or force foam into any areas of the wound, and a direction that all pieces of foam should be removed from the wound during dressing changes. It also instructs that negative pressure wound therapy should remain on the “constant” mode for the duration of the treatment.
30 The instruction sheet sets out steps for the application of the foam dressing, including cutting the foam to the appropriate size to fill the wound cavity, covering the foam with transparent film, inserting a drain through a small hole in the film, creating a seal, and testing the pump to ensure that the seal is secure. It specifies that dressings should be changed every 48 hours and more frequently for infected or heavily draining wounds.
Report of expert panel meeting
31 The report of the expert panel meeting summarises presentations given by various experts on NPWT at a meeting held in Milan on 13 and 14 February 2009, apparently sponsored or hosted by S&N.
32 The report indicates that, inter alia, Professor Raymond Dunn speculated on the possible mechanisms by which the therapy appears to stimulate healing, such as removal of wound fluid and bacteria and promotion of granulation tissue formation. Dr Malmsjo considered that the therapy may stimulate wound healing by a combination of increased and decreased blood flow, and that continuous pressure and intermittent pressure can both provide therapeutic benefits, depending on the wound type. The experts agreed that further work was needed to determine how NPWT achieves its beneficial effects.
33 The Patent is entitled “Method and Apparatus for Treating Tissue Damage”. It specifies a priority date of 14 November 1991 and a publication date of 15 June 1993. The applicant for the patent is Wake Forest University.
34 The Patent states that the invention “relates generally to wound healing, and more specifically is directed at wounds that are unlikely to heal completely under conventional methods.”
35 Under “Background of the Invention”, the Patent identifies the current deficiencies in wound treatment it aims to solve. It states that:
The treatment of open wounds that are too large to spontaneously close has been a troublesome area for many years. Wound closure requires that epithelial and subcutaneous tissue adjacent to the wound migrate toward and eventually close the wound. Some wounds are sufficiently large or infected that they are unable to close spontaneously. In such instances, a zone of stasis, an area in which localized swelling of tissues restricts the flow of blood to these tissues, forms near the surface of the wound. Without sufficient blood flow, the wound is unable to successfully fight bacterial infection and accordingly is unable to close spontaneously.
36 The Patent states that “the most common technique for closure of open wounds has long been the use of sutures or staples”, which mechanical closure methods “provide tension on the skin tissue at the wound border that encourages epithelial tissue to migrate toward the wound and cover it”. The major drawback of suturing or stapling wounds (while widely practised) is that the associated stress may cause the wound to burst open and, in any event, the methods are simply not feasible for all wounds. The Patent describes the problems and examples of affected wounds thus:
[T]he tensile force required to achieve closure with sutures or staples causes very high localized stresses at the suture insertion points, resulting in the rupture of the tissue at these points. Substantial rupture will eventually cause dehiscence in some wounds, which results in additional tissue loss. Moreover, some infected wounds harden and inflame to such a degree that closure by suturing is not feasible. Wounds not reparable by suturing or stapling generally require prolonged hospitalization, with its attendant high costs, and major surgical procedures, such as grafts of surrounding tissue. Examples of such wounds include large, deep, open wounds, pressure sores resulting from prolonged pressure, ulcers resulting from chronic osteomyelitis, and partial thickness burns that subsequently develop into full thickness burns.
37 The Patent states that a method for treating wounds not reparable by the mechanical closure methods of suturing or stapling was required, as:
To date, there has been no consistently satisfactory method for treating such wounds. What is needed is a method of closing the wound without the localized stresses that accompany suturing while at the same time treating any infection present in the wound along with a simple apparatus to carry out the method. Such a method and apparatus would reduce hospitalization and increase the probability of wound closure.
Summary of the invention – the five aspects
38 Under “summary of the invention” the Patent sets out five aspects of the invention, as follows:
(a) A first aspect of the invention is a method of treating tissue damage which comprises applying negative pressure to a wound over an area sufficient to promote the migration of epithelial and subcutaneous tissue toward the wound and for a time period sufficient to facilitate closure of the wound. The method is particularly useful for treating pressure sores.
(b) A second aspect of the invention is applying negative pressure to a burn wound area for long enough to inhibit it from getting deeper. (This aspect of the invention was of limited relevance to the present case, as KCI did not allege infringement, and S&N did not challenge the validity, of the burns claims of the Patent).
(c) A third aspect of the invention is applying negative pressure for long enough to reduce bacterial density so surgical closure can be attempted. (Again, in this case, the burns claims were not alleged to have been infringed or to be invalidated).
(d) A fourth aspect of the invention is a method of enhancing the attachment of adjacent tissue to a wound, comprising the application of negative pressure to a joined complex of wound and adjacent living tissue at sufficient magnitude and for a sufficient time to promote the migration of epithelial and subcutaneous tissue toward the complex. A preferred use of this method is enhanced attachment of adjacent tissue to tissues of the wound edge. Another use is enhanced attachment of an open skin graft.
(e) A fifth aspect of the invention is an apparatus for facilitating the healing of wounds which comprises:
vacuum means for creating a negative pressure on the area of tissue surrounding the wound, sealing means operatively associated with the vacuum means to maintain the negative pressure on the wound, and screen means for preventing the overgrowth of tissue in the wound area. A preferred embodiment of the invention comprises a section of open cell foam configured to be placed over a wound, a flexible tube inserted into the foam section for attachment to a suction pump, a flexible polymer sheet overlying the foam section and tubing and configured to be adhered to the skin surrounding the wound.
(emphasis added)
39 The Patent displays the following two drawings showing cross-sectional views of negative pressure devices, which are briefly described.
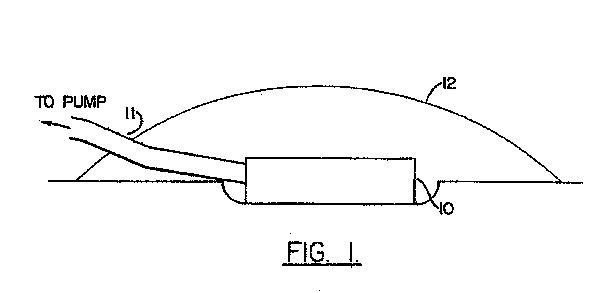
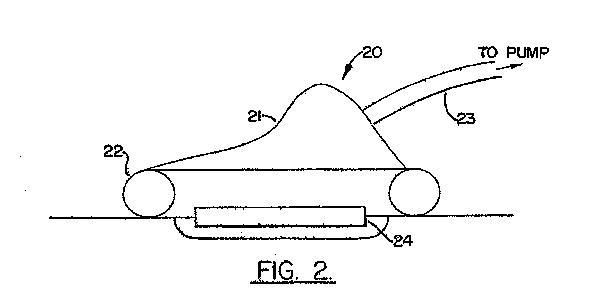
40 The description states that Figure 2 shows a cross-sectional view of a negative pressure device comprising, inter alia, a porous screen and “an inflatable cuff attached to a semi-rigid cup”.
Detailed description of the invention
41 The Patent describes:
a method of treating tissue damage which comprises the stages of applying negative pressure to a wound over an area sufficient to promote migration of epithelial and subcutaneous tissue toward the wound, with the negative pressure being maintained for a time sufficient to facilitate closure of the wound. Wound closure requires that epithelial and subcutaneous tissue migrate from the wound border toward the wound. The use of negative pressure provides tension on this border tissue that causes accelerated tissue migration. It has been observed that the use of the method also causes within the wound increased formation of granulation tissue, a matrix of collagen, fibronectin, and hyaluronic acid carrying macrophages, fibroblasts, and neovasculature that aids in healing.
(emphasis added)
42 The Patent states that the method is particularly suitable for use on pressure sores which can become infected, serious and even fatal, as negative pressure promotes the migration of wound border tissue, allowing healing. It is also suitable for decreasing the bacterial density in a wound by at least half, for burns to prevent them from becoming “full thickness” burns, and to enhance the attachment of living tissue flaps and open skin grafts, by promoting migration of epithelial and subcutaneous tissue towards the wound tissue complex, thus reducing the bacterial density and improving blood flow to the wound and “thereby improving the attachment of the grafted tissue”.
43 The Patent states that the method can be practised with the application of substantially continuous negative pressure (where the pressure is relieved only to change the dressing) or cyclically (alternate periods of application or non-application). The ratio of application to non-application can be as low as 1:10 or as high as 10:1, but is most preferably 1:1. A preferred pattern is five minutes of application followed by five minutes of relief. The Patent states preferable negative pressure ranges of 0.5 to 0.8 atmospheric and that the time period for using the method was:
preferably at least 12 hours but can be, for example, 1 day, 2 days, 5 days, 7 days, 14 days, 30 days or even longer. There is no upper limit beyond which use of the method is no longer beneficial; the method increases the rate of closure up to the time the wound actually closes.
44 The Patent describes in more detail the apparatus for facilitating the healing of wounds:
The apparatus comprises vacuum means such as a pump for creating a negative pressure on the area of skin surrounding the wound, sealing means such as an adhesive sheet operatively associated with the vacuum means for maintaining negative pressure on the wound by contacting the skin surrounding the wound, and screen means such as an open-cell foam section located within the sealing means for preventing the overgrowth of tissue in the wound area.
(emphasis added)
45 In relation to the screen means, the Patent states:
The screen means is placed over substantially the expanse of the wound to prevent its overgrowth. The size and configuration of the screen can be adjusted to fit the individual wound. It can be formed from a variety of porous semi–rigid materials. The material must be sufficiently porous to allow oxygen to reach the wound, and sufficiently rigid to prevent wound overgrowth. Most preferred is the use of an open-cell polymer foam, which permits direct connection of the screen means to the vacuum means through a flexible hose inserted into the foam. Such foam can vary in thickness and rigidity, although it is preferred that a spongy material be used for the patient’s comfort if the patient must lay upon the device during its operation. It can also be perforated to reduce its weight. Another embodiment comprises a section of honeycombed polyethylene sheet cut to the shape of the wound.
(emphasis added)
46 In relation to the sealing means, the Patent states:
Possible sealing means include a flexible sealing rim contacting the skin surrounding the wound, a flexible polymer sheet overlying the screen means and the vacuum means attached to the skin through an adhesive applied to the sheet surface facing the skin, and an inflatable sealing cuff that conforms to the skin when inflated and that is held in place by the suction of the vacuum means. If an adhesive sheet is used, it must have sufficient adhesion to remain in contact with the skin and form a seal under the negative pressure. Additionally, it must be sufficiently flexible to overlay the screen means and still conform to the skin around the wound. The sealing means also can include a semi-rigid cup that protects the wound from external contact. For example, a suitable cup-cuff assembly is provided by an adult CPR mask with an inflatable sleeve.
47 In relation to the vacuum means, the Patent states:
Suitable vacuum means includes any suction pump capable of providing at least [indecipherable] pound [per square inch (690 Pa)] suction to the wound, and preferably up to 3 pounds [per square inch kPa] suction, and most preferably up to 14 pounds [per square inch (96.6kPa)] suction, and a flexible hose that leads from the pump to a point within the pressurized volume created by the sealing means. The pump can be any ordinary suction pump suitable for medical purposes that is capable of providing the necessary suction. The dimension of the tubing are limited only by the pump’s ability to provide the suction level neede [sic] for operation. A ¼ inch [(0.64cm)] diameter tube has proven suitable. The vacuum means may operate substantially continuously, or may operate cyclically with alternate periods of application and nonapplication of pressure to the wound.
48 The Patent describes a preferred embodiment of the invention as shown in Figure 1 (see [39]).
49 The Patent further explains the invention by reference to the following eight examples:
(a) Two full thickness defects were made on each of a number of pigs. When negative pressure was applied to only one of the defects using a cup, the data showed an increased rate of wound closure and formation of granulation tissue at a statistically significant rate.
(b) Three burns were deliberately created on pigs. Suction apparatus cups were used to apply suction to two of the three burns. The burns thus treated were healthier and healing more quickly than non-suctioned burns.
(c) Two wounds on each of a number of pigs were injected with cultures of bacteria broth. One of the wounds was treated with negative pressure using a suction cup. On average, the non-treated wound was still infected after seven days, while the suctioned wound was disinfected after four days.
(d) A 45 year old diabetic paraplegic patient had a pressure sore and ulcer. When a flap was taken and placed onto the wound, it “dehisced”, resulting in a large open wound. Negative pressure was applied by the use of a device (not the cup) and the wound healed after six weeks.
(e) A 51 year old amputee had a large pressure sore for seven months, measuring eight inches x three inches at its widest. Cyclical negative pressure was applied and the wound reduced to three inches x one and a half inches after five weeks of treatment. It then had healthy granulation tissue which could accept a graft, and subsequently healed completely.
(f) A 50 year old patient had a colostomy revision which required wound dehiscence and evisceration. A large reduced pressure cup device was used and continuous negative pressure was applied. The wound became suitable for graft in parts and the remaining areas were closed with dressing changes.
(g) A 39 year old accident victim had an open ulcer and exposed bone on the ankle (due to osteomyelitis caused by an accident). Continuous negative pressure was applied using a cup device. After 14 days, granulation tissue had grown and the wound was smaller. It was healed with a graft.
(h) A burns victim had second and third degree burns to the face and upper extremities, including the hands. The hand was treated with vacuum applied cyclically (five minutes on and off) using a reduced pressure device until the necrotic tissue sloughed off or was excised, followed by split thickness skin graft placement.
50 The Patent noted that the above examples were illustrative of the invention and not limiting thereof.
51 The Patent stated that the invention was defined by the claims which it set out.
52 KCI alleges that S&N has infringed claims 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 49, 50, 52 and 121 of the Patent by entering the Australian market with NPWT system foam dressing kits which can be used with both existing and new S&N NPWT vacuum pumps. The 14 claims in suit consist of 11 method claims and three apparatus claims.
53 Claim 1 is a method claim. Claims 2, 3, 6, 7, 8, 9, 10, 11 and 12 are claims dependent on claim 1. Claim 121 is also a method claim. They are as follows.
54 Claim 1:
A method of treating tissue damage which comprises the steps of:
placing a screen means for preventing overgrowth of tissue in a wound, said screen means being sufficiently porous to allow gases to reach the wound and sufficiently rigid to prevent wound overgrowth, and
applying a negative pressure to said wound over an area sufficient to promote migration of epithelial and subcutaneous tissues toward the wound, with said negative pressure being maintained for a time sufficient to facilitate closure of the wound.
(emphasis added)
55 Claim 2:
A method according to claim 1, in which said negative pressure is maintained for a time sufficient to permit the formation of granulation tissue in the wound.
56 Claim 3:
A method according to claim 1, in which said wound is a pressure sore.
57 Claim 6:
A method according to claim 1, in which said time is at least 12 hours.
58 Claim 7:
A method according to claim 1, in which said time is at least 3 days.
59 Claim 8:
A method according to claim 1, in which said pressure is applied substantially continuously.
60 Claim 9:
A method according to claim 1, in which said negative pressure is cyclically applied in alternate periods of application and non application.
61 Claim 10:
A method according to claim 9, in which the ratio of said period of application to said period of non application is at least 10:1.
62 Claim 11:
A method according to claim 9, in which the ratio of said period of application to said period of non application is at least 1:1.
63 Claim 12:
A method according to claim 9, in which the ratio of said period of application to said period of non application is at least 1:10.
64 Claim 121:
A method of treating a wound comprising the steps of:
placing a screen means in the wound for preventing overgrowth of tissue in the wound, said screen means being sufficiently porous to allow gases to reach the wound and sufficiently rigid to prevent wound overgrowth;
applying a reduced pressure to the wound; and
maintaining said reduced pressure until the wound has progressed toward a selected stage of healing, wherein said maintaining of said reduced pressure is conducted in alternating periods of application and non-application of reduced pressure.
(emphasis added)
65 Claim 49 is an apparatus claim. It is as follows:
An apparatus for applying negative pressure to a wound beneath a fluid-impermeable seal comprising:
a screen means for positioning beneath said seal for preventing overgrowth of tissue in the wound, said screen means being sufficiently porous to allow gases to reach the wound and sufficiently rigid to prevent wound overgrowth, said screen means comprising an open cell polymer foam section configured to overlie the wound such that said negative pressure is maintained within said foam and applied to the wound;
a flexible tube having an inlet end inserted into said open cell polymer foam section and an outlet end for extending from beneath said seal and for supplying said negative pressure; and
wherein said apparatus is in an aseptic package.
(emphasis added)
66 Claim 50 is an apparatus claim as follows:
An apparatus for treating a wound, comprising:
a screen means for preventing overgrowth of tissue in the wound, said screen means being sufficiently porous to allow gases to reach the wound and sufficiently rigid to prevent wound overgrowth, said screen means comprising an open-cell foam section configured to overlie the wound;
a fluid-impermeable cover overlying said foam section, said cover adapted to form a seal with skin surrounding the wound for maintaining negative pressure beneath said cover; and
a single tubular member having a first end inserted beneath at least a portion of the foam section and having a second end extending from beneath said cover to a location external to said cover for supplying negative pressure beneath the cover.
67 Claim 52 is an apparatus claim dependent on claim 50. It is as follows:
The apparatus of claim 50 wherein said first end of the tubular member is embedded within the foam section.
68 KCI seeks injunctive relief restraining S&N’s allegedly infringing conduct, together with damages for infringement from the time of the introduction of the S&N foam kits.
69 By cross-claim, S&N alleges that the claims it has allegedly infringed are invalid on the following grounds:
(a) lack of novelty;
(b) lack of inventive step;
(c) manner of manufacture (method of human treatment/mere desiderata);
(d) failure to define the invention;
(e) lack of clarity;
(f) lack of fair basis;
(g) lack of sufficiency; and
(h) in relation to claim 49 only – mere collocation.
70 As discussed below, S&N contended (as an overarching defence to infringement) that the essential functional integer in the Patent of a screen means “sufficiently rigid to prevent wound overgrowth” was meaningless and a scientific nonsense. S&N conceded that the success of its defence based on the absence of that integer would be inconsistent with its allegation that the claims were invalid for want of novelty, because the relevant integer, consequently, could not be present in the prior art. It nevertheless pressed its allegations of invalidity on other grounds.
71 Further, by cross-claim S&N alleged that the priority date for the Patent claims is not 14 November 1991, but 7 November 1996. If the claims in suit are otherwise valid, and the later priority date applies, it will be necessary to take account of additional prior art and, indeed, the presence in the Australian market of the KCI kits.
72 By the order of Sundberg J made on 16 November 2009, the issues of infringement and validity of the claims in suit are to be determined prior to any determination of damages or other relief.
73 KCI relied on the evidence of the following witnesses:
(a) Mr Peter Hickey, who swore affidavits dated 2 March 2009 and 24 March 2009 and was cross-examined. Mr Hickey was the Managing Director of KCI MA and, since November 2008, Regional Managing Director for the KCI group across South East Asia, South Korea and the Pacific region. He has a general nursing qualification and a Masters of Business Administration;
(b) Professor Donald Marshall, who swore affidavits dated 17 September 2009 and 3 March 2010 and was cross-examined. After graduating from medical school in 1957, Professor Marshall’s career in plastic surgery spanned over 45 years, including positions held at the Royal Melbourne Hospital and Prince Henry’s Hospital;
(c) Dr Robert Wilkins, who affirmed an affidavit dated 4 March 2010 and was cross-examined. Dr Wilkins was a biomedical engineer with a Bachelor of Mechanical Engineering, a Masters in Biomedical Engineering and a PhD in medicine. He has practised biomedical engineering since 1980;
(d) Mr Taliesin Ellis, who swore an affidavit dated 9 March 2010 and was cross-examined. Mr Ellis was a registered nurse and Managing Director of WoundHeal Australia, an organisation offering, inter alia, wound management practice and training programs; and
(e) Dr Miklos Pohl, who affirmed an affidavit dated 9 March 2010 and was cross-examined. Dr Pohl was a consultant plastic surgeon at the Peter MacCallum Cancer Centre and the Skin and Cancer Foundation, and Head of the Department of Plastic Surgery with Western Health in Victoria. He was also Clinical Senior Lecturer in surgery at the University of Melbourne.
74 S&N relied on the evidence of the following witnesses:
(a) Professor Anthony Penington, who swore affidavits dated 19 March 2009, 23 December 2009 and 12 April 2010 and was cross-examined. Professor Penington held Bachelor degrees in medicine and surgery and specialised in plastic surgery since 1992. He was Associate Professor in the Department of Surgery, St Vincent’s Hospital, University of Melbourne, and a consultant plastic and reconstructive surgeon at St Vincent’s Hospital and the Royal Children’s Hospital;
(b) Professor Michael Stacey, who swore affidavits dated 11 December 2009 and 9 April 2010 and was cross-examined. Professor Stacey was Professor of Surgery at the University of Western Australia and Head of the Department of Vascular Surgery at Fremantle Hospital. He obtained Bachelor degrees in medicine and surgery in 1977, a Doctor of Surgery in 1991, and has edited journals on wound management;
(c) Professor Roy Kimble, who swore an affidavit dated 14 December 2009 and was cross-examined. Professor Kimble was Professor of Paediatrics and Child Health at the University of Queensland, Royal Children’s Hospital Brisbane, and has practised medicine for 25 years. He obtained a Doctor of Medicine from the University of Queensland in 2008;
(d) Dr Randolph Williams, who swore affidavits dated 22 December 2009 and 9 April 2010 and was cross-examined. Dr Williams was Head of Surgical Service and Senior Visiting Surgeon at Modbury Public Hospital, and has run a private surgical consulting practice since 1982. He was also Clinical Lecturer at teaching hospitals associated with the University of Adelaide; and
(e) Mr Roger Osmond, who affirmed affidavits dated 23 December 2009 and 8 April 2010 and was cross-examined. Mr Osmond has 28 years’ experience working in the medical equipment field and was, until recently, National Product and Business Development Manager of a radiology solutions company.
75 While both parties expressed reservation or muted criticism about the approach of some opposition witnesses, and the evidence of some witnesses on certain issues was more consistent, cogent, persuasive and hence, ultimately to be preferred over that of others, I considered that all the above were honest, responsive and highly conscientious witnesses who did their best to assist the court to determine the complex, voluminous and specialised issues in this case.
76 The parties relied on voluminous written submissions, some aspects of which were not addressed in oral submissions. They were as follows:
(a) outline of applicants’ submissions on validity dated 28 June 2010;
(b) outline of applicants’ submissions on infringement dated 28 June 2010; and
(c) outline of respondent/cross-claimant’s submissions dated 28 June 2010.
77 The parties’ expert witnesses were in broad if not complete agreement about the nature and various types of wounds and the natural processes and stages of wound healing.
78 A wound is a type of tissue damage which involves a break in the skin and may also, but not necessarily, involve breaks in the subcutaneous layers of tissue. There are many types of wounds, including acute wounds arising from surgery or trauma, wounds involving underlying fistulae, chronic wounds which (however they arose) will not heal (such as various leg ulcers, diabetic foot ulcers and pressure sores) and burns. Wounds may be classified as either uninfected or infected.
79 There are three common mechanisms of wound closure. The first, closure by primary intention, occurs where the non-infected wound’s edges can (after any necessary removal of material) be aligned and mechanically closed by, typically, sutures or staples. Alternatively, a skin graft or flap may be applied to close the wound.
80 The second method is a variant of the first, known as delayed primary closure. That occurs if the wound cannot be sutured or stapled within a short time, because, for example, it requires (for up to three days after injury) cleaning, monitoring or debridement, after which it is sutured or stapled.
81 The third method is closure by secondary intention, which occurs when the wound edges cannot be aligned or sutured. In this method, granulation tissue grows from the wound bed to fill the wound cavity, and wound contraction and “epithelial creep” occur, helping to close the wound. The development of an appropriate quantity and quality of “healthy” granulation tissue is essential to closure by secondary intention.
82 If a wound is too large, or it is otherwise inappropriate to close by secondary intention, the bed of healthy granulation tissue may, at a certain stage, eventually render it ready to take a skin graft.
83 It was not disputed that the normal healing of a wound, whether closed by primary or secondary intention, involves a number of phases which are interrelated and overlap. The parties differed somewhat on the precise number and features of the phases and the degree to which they are distinct. KCI identified the following four phases:
(a) clotting to control bleeding;
(b) inflammation as blood vessel walls become more permeable;
(c) cellular proliferation during which granulation tissue forms; and
(d) healing of the wound surface as surrounding tissue contracts to reduce the wound area, epithelial cells start multiplying and migrating and an immature scar forms.
84 S&N did not refer to the clotting phase and identified only three broad phases, viz:
(a) inflammatory;
(b) proliferative; and
(c) maturation, which S&N described as follows:
In the inflammatory "phase", bacteria and debris are broken down and removed. Growth factors which stimulate the migration and division of cells in the proliferative phase are released. Macrophages, which arrive around two days after the wound occurs, are attracted to the wound by the growth factors and they also break down bacteria and debris. They also excrete a number of growth factors and other cytokines, which further promote migration and division of cells as well as angiogenesis (growth of new blood vessels). These secretions attract other cells which are involved in the proliferation phase…
The proliferative "phase" merges with the inflammatory phase. During this phase, endothelial cells migrate to the area of the wound and angiogenesis is initiated, and, thereby, new blood vessels form and provide oxygen for other cells to function. Collagen and other structural proteins are deposited to strengthen the wound and granulation tissue is formed within the wound. Epithelial cells migrate across the newly formed granulation tissue and act as a barrier between the wound and the environment. Beginning around one week from wounding, myofibroblasts within the wound edges contract, causing the wound defect to reduce in size by the process of contraction…
The inflammatory phase merges with a process called maturation, which is the final phase of wound healing. Collagen is remodelled and realigned along tension lines and unwanted cells are removed…
85 KCI described the final phase as follows:
…epithelial cells at the edge of the skin start multiplying and migrating across the wound on top of the granulation tissue. This is called ‘epithelial creep’ and results in healing of the wound surface. The wound will close as connective tissue contracts and the epithelium grows across the wound to form a firm scar. The healed wound at this stage is an immature scar…
86 I was unable to determine whether there were, more accurately, three or four phases, but the evidence indicated that the phases were not clear-cut.
87 There was also broad agreement that from the late 1980s, moist wound healing theory, pioneered by George Winter in his widely known paper published in 1962, was being increasingly known and applied. Winter maintained that wounds should not be permitted to dry out completely in order to achieve the best success rate for healing, on the premise that decreasing cell dehydration decreased cell death. The Winter paper did not, however, define the ideal level of moisture for the healing phase.
88 S&N submitted that by November 1991, clinicians, having recognised that wounds permitted to dry out healed at a less successful rate, were using dressings that could maintain appropriate moisture levels.
89 Clinicians also recognised well before November 1991 that if a wound were too moist, the wound fluid (exudate) damaged the skin surrounding the wound (maceration), so they used dressings and/or techniques which absorbed or drained fluid out of the wound.
90 By the mid to late 1980s, gauze, gauze soaked in saline, and gauze soaked in Betadine, Lyofoam (an open-cell polymer or polyurethane foam) and Opsite (a liquid impermeable membrane) were available and were all in general use by surgeons and nursing staff. Other dressings capable of maintaining a moist wound environment were also on the market and in use. Allevyn, another foam dressing with an outer semi-permeable polyurethane film layer which is highly absorptive, was also available. Such cell foams were also used to manage fluid under skin grafts, thereby promoting the “taking” of skin grafts.
91 Prior to November 1991, various methods were employed to treat wounds that produced a moderate to high amount of fluid, with the primary objective of removing the undesirable excess. Such fluids might be removed by drainage or by dressings prior to November 1991. Suction may also have been used on open wounds, by means of a “sump drain” together with a tube.
92 KCI broadly agreed with the above description of moist wound healing theory and practice.
cOMMON GENERAL KNOWLEDGE AS AT 1991
93 The common general knowledge of the hypothetical addressee as at the priority date of the Patent is relevant to the construction of the Patent (as it must be read in its light), novelty and obviousness. In the present case, S&N challenged the priority date of 1991 on the ground of lack of a fair basis. As discussed below, I have found that the correct priority date was 14 November 1991.
94 In Minnesota Mining and Manufacturing Co v Beiersdorf (Australia) Ltd (1980) 144 CLR 253 (“Minnesota Mining”) at 292, Aickin J, (subsequently cited with approval in Lockwood Security Products Pty Ltd v Doric Products Pty Ltd (No 2) (2007) 235 CLR 173 (“Lockwood (No 2)”) at 196-197), stated that common general knowledge is: “the background knowledge and experience which is available to all in the trade in considering the making of new products, or the making of improvements in old”. It is well understood to be, as stated in Lockwood (No 2) at 196, “part of the mental equipment of those concerned in the art under consideration”.
95 It is not enough that information is publicly available. In Lockwood (No 2), the High Court stated at 197 that:
The effect of Minnesota Mining and Wellcome Foundation was that for the purpose of determining inventiveness prior disclosures which were publicly available information, but which were not part of common general knowledge, were excluded from consideration.
96 Information does not constitute common general knowledge merely because it might be found, for example, in a journal, even if widely read by persons in the art: see British Acoustic Films Ltd v Nettlefold Productions (1936) 53 RPC 221 (“British Acoustic”) at 250 affirmed in General Tire and Rubber Co v Firestone Tyre Rubber Co Ltd (1971) 1a IPR 121 (“General Tire”) at 135.
97 In Alphapharm Pty Ltd v H Lundbeck A/S & Anor (2008) 76 IPR 618 (“Alphapharm”) at 667, Lindgren J recently observed:
[I]t was held in Astra that information recorded in a document, even a document widely circulated within the art, is not part of general common knowledge merely because the skilled addressee could be expected to locate it. The question is whether it is "generally accepted without question" or "generally regarded as a good basis for further action" by the bulk of those in the art...
98 In Aktiebolaget HÄssle v Alphapharm Pty Ltd (2000) 51 IPR 375 the Full Federal Court made clear at 391 that “[w]hat might be found by a diligent searcher is not the same as “common general knowledge”.
99 A fact does not form part of the common general knowledge merely because it is known or even well known. Nor does the use of something per se qualify it, as Luxmore J in British Acoustic (cited by the Court of Appeal in General Tire at 135) stated at 250:
It is certainly difficult to appreciate how the use of something which has in fact never been used in a particular art can ever be held to be common general knowledge in the art.
Parties’ submissions and expert evidence
100 The parties differed on the common general knowledge about the treatment of wounds prior to November 1991.
101 KCI contended that:
(a) Passive drainage of closed sutured wounds was common. While there was also active drainage of closed wounds by RediVac or HemoVac bottles, wall suction or portable pumps, it was a rare practice which involved practical difficulties.
(b) The drainage of open wounds was not common, although Professor Marshall used a passive sump system or device on open wounds.
(c) The active drainage of fistulae and open wounds to which Dr Williams and Dr Pohl testified was neither widespread nor common general knowledge.
(d) Further, Dr Williams’ practice involved fistulae, which were not “wounds” proper, and the focus was on removing effluent, rather than using negative pressure for the trilogy of purposes expressed in the Patent.
(e) While Dr Williams’ veracity was unchallenged, his evidence about the active drainage of fistulae and open wounds contrasted with the ignorance of the practice expressed by Mr Ellis (a highly experienced wounds nurse working for some of the time in the same hospital) and Professor Marshall, and the fact that Professor Penington and Professor Stacey used drainage only on closed wounds and had neither seen nor used Dr Williams’ technique.
(f) Ultimately, only Dr Williams and Dr Pohl had used active suction on open wounds or seen it used prior to 1991.
(g) Further, while there was a range of dressings, gauze was most commonly used and foams, while available, had limited application, mainly confined to skin grafts and diabetic ulcers.
(h) Foam was not, on the evidence, placed in wounds and used in conjunction with negative pressure to achieve promotion of granulation tissue, prevention of wound overgrowth and drawing the wound closed.
(i) Gauze was used on the top of, and to pack, wounds.
(j) Covers or films were used to keep wounds moist, but subject to frequent dressing changes.
102 S&N contended that the evidence of Dr Williams, fortified by that of Mr Osmond, established that active drainage of open wounds with underlying fistulae and other moderate to heavily draining wounds occurred from at least the 1970s and as at 1991 and indeed, in some hospitals, fistulae and moderate to heavily draining open wounds were treated with open drainage suction comprising the following:
(a) a porous dressing laid across the surface of the wound in such a way so as to pack it;
(b) a tube laid on top of the porous dressing or across the wound beneath a gauze dressing;
(c) a cover such as a stoma bag or long bag or flexible plastic bag, which was attached to the skin surrounding the wound with an adhesive such as Stomahesive paste or Stomahesive tape to create an air tight cover over the wound or an adhesive film or adhesive dressing; and
(d) a tube which exited the cover in such a way so as to maintain the seal over the wound and which was attached to a source of suction, generally wall suction or a portable electric pump,
which system would be left in place for as long as required, depending on the nature of the wound, typically until ready for standard wound dressings. The system would be applied for a variable length of time depending on the nature of the wound.
103 Thus, in S&N’s submission:
Negative pressure (also called sub-atmospheric pressure, suction pressure, vacuum pressure and topical negative pressure, among others) had been used in Australia in relation to closed and open wound drainage systems before the alleged priority date…
It does not matter whether any particular installation at any one hospital was common general knowledge: their existence at various places including in Australia shows that the basic elements of negative pressure wound therapy were well known before the alleged priority date.
104 Thus, the parties and expert witnesses differed on several principal matters, namely, the use of foam, the drainage of wounds including by negative pressure (suction), the use of sealing means and the use of tubes in suctioning open wounds as at 1991.
105 It was common ground that foam dressings (in two main forms, Lyofoam and Allevyn) were available and used in the treatment of wounds prior to November 1991.
106 KCI submitted that gauze was the most common dressing in Australia in 1991, and that foam had only limited uses, being mainly restricted to, for example, skin grafts and diabetic foot ulcers. KCI disputed that Lyofoam was used prior to 1991 for other than those limited purposes or to absorb blood and fluids in fairly moist wounds. KCI also submitted that while Lyofoam and Allevyn were used, they were not placed in wounds prior to November 1991.
107 In contrast, S&N submitted that foams were widely available and used prior to 1991 and were placed in wounds. S&N contended that Lyofoam was used in fairly moist wounds as it was able to absorb blood and other tissue fluids by capillary action. It was useful in maintaining a moist environment at the surface of the wound, and in distributing an even pressure across the entire wound due to its open-cell form, which beneficially reduced pressure away from the site of the wound in diabetic foot ulcers and venous leg ulcers.
108 Mr Ellis’ evidence was that he did not recall seeing foams, and certainly not in any clinical environment, prior to 1991. While conceding that he was “struggling to recall”, he thought that he had seen foam in some overseas journals, but not in use in Australia at the time.
109 Mr Ellis was not certain that there were no foams in use and, indeed, acknowledged that they were in use elsewhere, but thought that:
they were very primitive foams, maybe Lyofoam and… another… produced by Merck Sharp & Dohme. I have got a picture of it but I never saw it or used it… The foams, really, in Australia came more into prominence during the early 90s so that…. it sort of started to increase in their use.
110 At trial, Professor Marshall stated that “for many years the gold standard” material for a dressing to be tied over a wound was “Acriflavine wool… a cotton wool impregnated with an antimicrobial”. Professor Marshall stated that when foam became available back in the 1950s and 1960s, “we started using foam because it was more kind to the patient and easier to use and did not become rock hard if it got blood in it and so on.”
111 Dr Pohl, in his affidavit, stated:
It was my experience as of 1991 that the tube used with open drainage systems was put into the wound but I was not aware of foam being used with these open drainage systems.
112 Professor Penington, in his second affidavit, stated that:
Once a skin graft has been applied [to treat a wound that cannot be sutured], it is standard practice now, and was before November 1991, to use a dressing over the graft to place pressure on the graft and hold the graft down on the wound bed… Prior to November 1991, I observed and had used, open-cell polymer foam dressings placed over skin grafts for this purpose. Typically, the foam would be stitched down around the wound which would compress it onto the wound and hold it in place.
113 Professor Stacey, in his first affidavit, stated that:
[T]he wounds that I came across and treated in my practice from 1978… and prior to November 1991… [included]:
…
(f) Diabetic foot ulcers, which I mainly treated by relieving pressure from the affected area. I covered the wound with a foam dressing, usually Lyofoam (an open cell foam available prior to November 1991), or a non-adherent dressing such as Adaptic;
(g) Pressure sores/ulcers… I treated the wound with a dressing, such as saline impregnated gauze or Lyofoam, or an alginate dressing.
…
I mostly used Lyofoam on diabetic ulcers, smaller venous ulcers and occasionally on pressure ulcers. I would select the dressing I used… with the goal of maintaining an appropriate moist wound environment.
…
I recall that Lyofoam was also available during the 1980s and 1990s… Lyofoam is an open cell, polyurethane foam. It is able to absorb blood and other tissue fluids by capillary action. The dressing was useful in maintaining a moist environment at the surface of the wound, which is conducive to the formation of granulation tissue and epithelialisation. Lyofoam was also useful in distributing an even pressure across the entire wound because of its open cell form.
…
Another dressing that was available prior to November 1991 was Allevyn. Allevyn is a foam dressing with an outer semi-permeable polyurethane film layer. It is highly absorptive. The outer is impermeable to wound fluid while allowing vapour to pass through it. It aids in preventing an excessively moist wound environment.
…
As at the late 1980s, I maintained a moist wound environment in wounds that were producing moderate to high amounts of exudate/fluid in one of five ways, depending on the type of wound… First, I used a highly absorbent contact layer dressing, such as Allevyn… which I might have covered with a cotton wool padding or similar such padding.
114 Dr Williams, in his second affidavit, stated that prior to 1991, “[i]n addition to hydrocolloids, alginates and hydrogels, I was aware from observing my surgical colleagues that foam was being used on skin grafts but it was not my personal practice to use it on skin grafts at that time.”
Drainage and negative pressure
115 It was not disputed that the drainage of wound exudates was common in 1991. Two types of drainage are, however, relevant in this context, namely, passive drainage (where the fluid simply drains from the wound by the force of gravity) and active drainage, where the fluid is sucked out of the wound by negative pressure.
116 The parties disagreed on:
(a) whether, in 1991, active suction was only used for closed wounds, or whether it was also used for open wounds. KCI submitted that active suction by the use of negative pressure was confined to closed wounds, while S&N stated that it was also used for open wounds. KCI conceded that passive drainage of open wounds was common, but submitted that active suction was not applied to those open wounds; and
(b) whether the purpose of drainage in 1991 was only to remove fluid from the wounds, or whether it was also to assist in wound closure as effected by the V.A.C.® invention. KCI submitted that the purpose of drainage at that time was only to remove fluid, thereby allowing the wound to heal naturally, rather than maintaining negative pressure to accelerate wound closure. S&N did not dispute that the purpose of drainage was to remove fluid, but submitted that it was consistent with, and assisted, the ultimate purpose of promoting wound healing and the normal growth of granulation tissue. Thus, in S&N’s submission, the distinction between the purposes of removal of fluid and wound healing was a false dichotomy.
117 Mr Ellis, Dr Williams, Dr Pohl, Professor Stacey, Professor Penington and Mr Osmond agreed that negative pressure (active suction) was used to drain exudates in the context of closed wounds (ie those that have been sutured).
118 Mr Ellis deposed that active suction was not used for open wounds in 1991, and that he had never seen suction applied to an open wound until he saw the V.A.C.® product. Similarly, Professor Marshall deposed that he was unaware of any medical application in 1991 of treating an open wound by sealing and suction. At trial, however, Professor Marshall conceded that he had used active suction on open wounds from time to time in order to avoid contamination of the skin.
119 Dr Williams deposed that active suction was regularly used for open wounds in 1991.
120 Dr Pohl deposed that he could not recall fistulae being drained by active suction in 1991, but nonetheless deposed that suction was maintained in “open drainage systems” as at 1991 for as long as required to remove effluent from the wound. He also deposed that “continuous suction” was sometimes used in open drainage systems, but not the regular “on/off cyclical application” of negative pressure claimed in the Patent. Accordingly, Dr Pohl appeared to acknowledge that active suction was used for open wounds at the relevant time.
121 Dr Williams deposed that, as at 1991, drainage promoted wound healing, including the growth of healthy granulation tissue, by removing harmful fluids which impeded the normal wound healing process. At trial, Dr Pohl agreed that fluids and exudates could impede the wound healing process.
122 In contrast, Mr Ellis deposed that the purpose of drainage was simply to remove fluid. At trial, he agreed that as at 1991, “the removal of exudate from wounds via drainage was certainly a common procedure… a common occurrence” but testified that the aim of removing fluid was to control the potential for infection and reduce the tension in the tissue. He rejected the proposition that reducing infection and tension were themselves directed at the overriding goal of promoting wound healing, but nonetheless accepted that drainage would achieve a “healing outcome” by reducing the chance of complications. He stated:
I would see it almost the other way around whereby the wound healing promotion is almost the secondary to the need for the removal of – so the drainage was more about, I guess, achieving a healing outcome by reducing the chance of complications.
123 Mr Ellis, in his affidavit, stated:
As at 1991… control of infection was another key aspect of wound treatment. For most wounds this meant keeping the wound clean, and clearing away debris and exudates… it was… commonly necessary to install an apparatus to drain infected or inflamed wounds of fluids and other exudates on an ongoing basis to facilitate healing.
124 While Mr Ellis acknowledged that drainage was used, he stated that:
[Up until 1990] [t]he vast majority of draining wounds I helped manage were “closed” wounds and therefore involved a “closed drainage system”. In my experience, the vast majority of drainage systems used at the Royal Adelaide Hospital for closed wounds were passive systems whereby any fluid build-up was simply drained away by the force of gravity.
125 Mr Ellis stated that although he was also involved in, or knew of, a few instances of closed drainage systems which used active drainage, (in that a non-mechanical vacuum apparatus was involved to apply suction to the cavity to remove the fluid), he recalled that they were rare when compared to the number of closed abdominal wounds with passive drainage systems.
126 Mr Ellis was also aware that the Royal Adelaide Hospital used an “open” but passive (gravity) drainage system, commonly for treating fistulae, and never saw or heard of any sort of active suction being used to assist with that fluid drainage.
127 Mr Ellis deposed that:
As at November 1991 I had never heard of… negative pressure or suction being applied to a wound, other than in the specific context of fluid being drained from a cavity in a wound which had already been surgically closed.
128 Mr Ellis deposed that when he first saw the V.A.C.® product in 1996, he considered it was a revolutionary method of wound management, as he had never previously seen a device which created a negative pressure environment or applied suction pressure directly to the surface of an open wound or read of such a system or concept. Mr Ellis deposed that:
Certainly with my experience at the Royal Adelaide Hospital and subsequently, I had never seen suction applied to an open wound.
…
Throughout my time at the Royal Adelaide Hospital no suction drainage was used on fistulae or open wounds to my knowledge. In fact as at November 1991 I was not aware of suction drainage being used anywhere in relation to open wounds or fistulae.
129 While aware that Dr Williams asserted that open drainage suction systems were used for moderate to heavily draining wounds since the mid 1970s, Mr Ellis stated:
While that may be the case elsewhere (although I am not aware of it), it certainly was not the case at the Royal Adelaide Hospital during my tenure, and does not accord with my understanding of historical trends and approaches to wound treatment. Drainage of such wounds at that time was passive.
…
Throughout my time at the Royal Adelaide Hospital and throughout my subsequent career involved in teaching wound healing and treatment approaches, the use of drains was a well understood technique. Nonetheless it is clear that the purpose of the drains was to remove fluid. I certainly did not consider, and it was never suggested to me by any colleagues, surgeons, or any literature I read, that suction drains had or could be used as a method of treatment which would have a therapeutic effect above and beyond the straight forward removal of fluid.
130 Mr Ellis described the different types of drains with which he was familiar in 1991 as first, a passive closed drainage system (which was installed at the time of the operation and allowed for the drainage of wound fluids to the external environment); secondly, RediVacs or HaemoVacs, which were small suction-type devices; and thirdly, placement of bags over the top of the wound to collect the fluid. The first two types of drains were placed over the wound to allow the fluid from the fistula or the sinus or the open wound to drain directly into it. For very large wounds, Cryovac bags would be used with a border of hydrocolloid to collect fluid passively, occasionally using a tube connected to one end of the Cryovac bag, allowing the fluid to drain into an external collection device.
131 When asked about active suction methods, such as portable electric pumps or wall suction, Mr Ellis stated:
My experience did not include the use of those. I do not remember seeing them there. But I accept that… obviously that was going on somewhere because plenty of other people do remember seeing them. But in my experience, it was largely the passive drainage systems and the modified drainage systems that the stomal therapists put in place.
132 Mr Ellis acknowledged that in his experience, especially as at 1991, the treating surgeon typically ordered or instructed the use of a vacuum system, rather than the nursing staff deciding how to treat or manage wounds.
133 In contrast to Mr Ellis, Dr Williams, who worked at the same hospital for five or six years (albeit that they did not know one another), was aware of open drainage prior to 1991 of fistulae and moderately to heavily draining wounds. He also maintained that suction was not uncommonly used in closed drainage systems.
134 In his first affidavit, Dr Williams stated that in draining wounds that could be closed by primary intention:
I recall that from at least the 1970s up to November 1991, a suction drain would be placed in the cavity of the wound in circumstances where there was the potential for the build up of fluids. The suction drain was passed through the healthy skin adjacent to the wound and then laid along the base of the wound. The wound was then sutured shut and, in some cases, an adhesive seal or cover was applied over the wound. This was (and still is) known as a closed suction drainage system. The drains were generally used following hernia repairs, removal of pilonidal sinus disease, removal of a subcutaneous tumour or a cyst, many intra abdominal procedures and following a mastectomy. I personally saw and used these systems in the surgical wards in the Royal Adelaide Hospital during this period.
135 Dr Williams also recalled that from at least the 1970s up to November 1991, open drainage was used for fistulae with either a passive (gravity) drain or (especially for higher output fistulae) by the use of active (suction) drainage. Dr Williams maintained that since the mid 1970s the open drainage suction system was also used in other types of moderately to heavily draining wounds (such as a chronic abscess, chronic wound infection or a post-operative wound infection). Dr Williams stated that the open drainage system incorporated:
(a) a tube with an ending containing multiple perforations;
(b) a porous dressing, such as cotton gauze or ‘combine’ gauze, which is cotton wool between pieces of gauze or other porous fabric;
(c) a cover, such as a stoma bag or a long bag or a flexible plastic bag;
(d) an adhesive, such as Stomahesive, Stomahesive paste, which is like a glue, or Stomahesive tape, which is a 2mm thick material, which is adhesive on both sides so that it sticks to the skin surrounding the wound; and
(e) a source of suction (vacuum), such as wall suction, or one of the portable, electric suction units.
All of the items listed directly above were readily available for use in hospitals as at November 1991.
The system was applied to a heavily draining wound by packing the wound with the porous dressing. The perforated end of the tube was then laid across the wound bed, on top of the dressing. A portion of the skin surrounding the wound was covered with an adhesive, such as Stomahesive. The plastic cover was attached to the Stomahesive to form a sealed area around the wound. The tube came out through the plastic cover in such a way as to maintain the seal over the wound. The tube was then attached to a suction device and the fluid was sucked out of the wound into a canister.
136 Dr Williams further deposed:
The negative pressure wound dressings in common use today utilise the same principles and features as in the system I have described above. Over the course of the past decade or so, it has become generally accepted by clinicians involved in wound care that the negative pressure wound dressings in common use today improve the rate of healing in both wet and dry wounds.
137 In his second affidavit, Dr Williams disputed Mr Ellis’ comment that active suction in closed drainage systems was rare. Dr Williams deposed:
Based on my experience and observations, I know there were more than a “few instances”… of the use of active suction prior to November 1991 in closed drainage systems. Active suction was used regularly in heavily draining wounds in this period. It was almost always used when the wound was producing a lot of fluid, as the use of gravity alone to drain the fluid was not efficient. The source of the suction would differ, depending on the nature of the wound and available resources, but included the RediVac or HaemoVac pumps, wall suction or the portable, electric suction pump units.
138 Dr Williams also disagreed with Mr Ellis’ assertion that active suction was not used in the open drainage of fistulae or sinuses. Dr Williams deposed:
I recall that active suction was regularly used in open drainage systems for heavily draining wounds and fistulae… When a fistula or other type of wound was high output, active suction from either wall suction or from a portable electric suction pump was used as part of a sealed, open drainage system prior to November 1991.
139 Although Mr Ellis maintained that it was “startlingly new… that the negative pressure treatment was said to actually help accelerate the development of healthy granulation tissue in the wound” and he had “never seen a device which created a negative pressure environment or applied suction pressure directly to the surface of an open wound before I saw the VAC system”, Dr Williams deposed that applying suction to an open wound was not new. He stated “as I have said, there were certain types of draining wounds and fistulae to which my colleagues and I applied scaled, open wound drainage systems with active suction before November 1991. In doing so we created a negative pressure environment under the seal and on the wound.”
140 Dr Williams further deposed:
At or before November 1991 I knew, and I am aware from my discussions with surgical and nursing colleagues at the time that they also knew, that removing irritating or infected fluid from the wound promoted wound healing, and that the process of healing involved the growth of healthy granulation tissue. This is because the acidic or alkaline fluid in a wound can damage the wound and the skin surrounding the wound when they come into contact. If you can remove the unhelpful fluid then normal wound healing processes can commence and granulation tissue can begin to grow in the wound within two to four days.
…
KCI claims the KCI VAC accelerates healing by promoting granulation tissue growth. It is said by KCI in its promotional material that this is one of the main functions of the KCI VAC. The purpose of the sealed, open wound drainage systems I have described was to remove harmful fluids from the wound and the skin surrounding the wound, so that those fluids did not impede or prevent the normal wound healing processes, which of course includes the growth of granulation tissue and the contraction of the wound. Ultimately I do not consider the differences between the two systems in terms of their effect on wound healing to be significant.
…
Mr Ellis says… that as at November 1991 he was not aware of suction drainage being used anywhere in relation to open wounds. As I have said this was not my experience. Nor does it appear to be the experience of Mr Pohl… whom I understand to be recollecting the use of sealed, open wound drainage systems [in] his affidavit.
141 In cross-examination, Dr Williams agreed that the purpose of, and the effect of, a closed drainage system in a sutured wound is to clean the fluid out of the wound so that the wound can heal spontaneously or naturally. He stated that the object in managing the effluent from the fistulae to which an open drainage system was applied was to remove it to avoid damage to the surrounding skin and tissue, and to minimise the need for wound dressing changes.
142 Dr Williams explained that in passive drainage a stoma bag or the like would be put over the wound, and the fluid from the fistula would be allowed to drain into the plastic bag which would be emptied periodically. If, however, active drainage were used, tubing would be placed into the bag and sealed around the outlet of the bag and connected to some form of suction, which would remove fluid continuously into a container. That technique was to drain the effluent away until such time as the clinician formed the view that the harmful fluid had reduced to a level where it could be contained with a dressing, after which the natural wound healing process could commence.
143 Dr Williams testified that in such cases granulation tissue might commence to form, even before two days. He also agreed that ordinarily, if the undesirable fluid were removed, normal wound healing processes could commence and granulation tissue would begin to grow within about two to four days. Fluid would suppress normal wound healing, which relied on the formation of granulation tissue. The latter might nevertheless form even whilst drainage is in process, if the wound was otherwise clean, but not at a normal rate.
144 Dr Williams said that the purpose of the active drainage system was to clean the wound of harmful fluids so they did not impede the normal wound healing process, with the added benefit of minimising the number of frequently painful dressing changes. The active drainage system both promoted healing and facilitated closure.
145 Dr Pohl, in his affidavit, agreed that “[i]n 1991, it was common practice to insert drains under closed wounds following surgery”.
146 He deposed that:
In my time working in the [Colon and Rectum Unit at Sydney Hospital], and in the subsequent period prior to 1991, it was my experience that fistulae were drained passively and I do not recall fistulae being drained by active suction.
…
As at 1991, it was my experience that the porous dressings, such as gauze, that were used with open drainage systems were used to absorb fluid from a wound and debride dead material, not to prevent hypergranulation.
…
It was my experience using open drainage systems as of 1991 that suction was only maintained for as long as it was required to remove effluent from the wound.
…
It was my experience as of 1991 that continuous suction was sometimes used in open drainage systems, not the uniform ratios or regular on/off cyclical application of negative pressure claimed in the Patent.
…
It was my experience as at 1991 that drains as depicted [by Figure MCS-B of the Stacey affidavit] were often used under sutured wounds that were closed by primary intention. However, I do not recall continuous active suction attached to wall suction being used with this or any other type of closed wound.
147 At trial, Dr Pohl agreed that in addition to infection, fluids or exudates could impede the wound healing process.
148 Professor Marshall, in his first affidavit, deposed that he was:
aware in 1991 that various suction devices had been used in surgery (including plastic surgery) for a long time, at least from the late 1950s – early 1960s to prevent the accumulation of fluids or exudate. A suction device was usually inserted into a cavity within the body. The suction technique consisted of inserting one end of a drain tube into the cavity space, and the other side of the tube would then be connected to a suction bottle that applied continuous suction… The Patent teaches that an open wound may be treated by sealing it and applying suction to it. As at 1991 I was not aware of a medical application of suction in this way.
149 At trial, Professor Marshall agreed that it would have been reasonable, in 1991, to use suction to remove excess fluids and that there were methods of doing it without closing the wound. He stated:
[W]e would use what was called a sump drain… which was to put a tube within the wound to the bottom of the wound with holes in it to act like the sump of a motor car, so any fluid collecting would be in the bottom of it, and then put a tube down the middle of that sump drain connected to suction but without sealing it. Just, as I say, as open suction.
150 Professor Marshall stated:
[B]ecause I was so steeped in the notion that I could use suction within a closed surgical wound and that an open wound was a different thing that could drain on its own, I have to confess to you, I did not [think to put a seal over the top of an active suction system].
151 When asked whether he used active suction on open wounds from time to time, he responded “[y]es, in the system that you were describing to avoid the contamination of the skin.”
152 Professor Stacey, in his first affidavit, deposed that as at the late 1980s:
[D]rainage bottles with vacuum were used to remove fluid from cavity wounds which were closed surgically in order to remove excess blood or tissue fluid and to maintain appropriate moist wound environments. I used wall suction to create the negative pressure in the drainage bottle, or pre-vacuumed bottle. Once I had done this, I closed the valve on the tubing attached to the bottle, connected this tubing to a drainage tube that I had inserted into the patient, opened the valve on the bottle, and relied on the suction to extract the fluid from the cavity.
…
It was well known in Australia even before the 1980s that it was important to drain fluid out of a cavity wound, otherwise that fluid collects in the wound and prevents the apposition of the wound edges, thereby delaying the healing process and possibly acting as a site for infection. The removal of the excess fluid reduces the dead space and thus the size of the wound cavity, which means the wound can heal more quickly, quite simply because there is a smaller cavity to fill… The removal of excess fluid also assisted in maintaining an optimum moist wound environment that is conducive to healing. The mechanism for removing fluid… meant less dressing changes were required.
153 Professor Penington, in his first affidavit, deposed that during the period from 1987 to November 1991, he used “vacuum drains to drain fluid (wound exudate) from closed surgical wounds”.
154 Mr Osmond, in his first affidavit, deposed that he developed “a device in the mid-1980s that was directed to draining wounds which had been closed by suturing… Ultimately, however, I abandoned the commercialisation of my device, primarily through lack of funds.”
155 In his second affidavit, Mr Osmond deposed that:
In use for wound drainage, the Clements regulator I sold in the 1980s was connected to the wall suction and then connected, via a tube, to a collection bottle. The collection bottle was then connected to a second bottle via another tube. The second bottle was then connected to the patient via another tube… It was part of my role with Clements to visit hospitals in Australia and observe systems in use, and I saw wall suction being used in this way for drainage of closed wounds many times.
…
I recall that during the 1980s I did see wall suction being used, with low suction regulators, to actively drain closed sutured wounds many times.
…
While I agree [with Mr Ellis] that it is likely that the “majority” of closed wounds were drained at that time at Royal Adelaide by passive (gravity) drainage, I am aware that the hospital also used non-mechanical active suction, such as RediVac systems, as well as mechanical active suction, that is, electric pumps, for closed wound drainage in this period.
…
During my time selling pumps for Clements, as I have stated above and in my First Affidavit, I visited hospitals regularly to observe procedures and demonstrate products. I recall observing active suction, using electric pumps or wall suction, being used to drain both cutaneous and sub-cutaneous wounds. I do not recall at which hospitals I saw this being done, but saw it being done a number of times. The systems I observed for cutaneous wounds included a drain tube, connected at one end to the suction source, laid across the wound, gauze covering the tube and then a plastic adhesive film or adhesive dressing covering the tube and gauze in order to seal the wound. If the wound was sub-cutaneous, the drain tube was laid beneath the skin.
156 KCI relied on Professor Marshall’s evidence to establish that as at 1991, a seal was not used in the context of suction applied to open wounds. That conflicted with the evidence of Dr Williams, on whom S&N relied. Dr Williams asserted that a sealing means and a tube connecting the vacuum means to a screen were used as at 1991 in the context of open wounds.
157 It was common ground that, as at 1991, tubes were used in the wound treatment process. While Professor Stacey and Mr Osmond deposed that they used, or were aware of the use of tubes for closed wounds, Dr Williams deposed that they were used in open drainage systems too.
158 Professor Marshall, in his first affidavit, stated that “[t]he Patent teaches that an open wound may be treated by sealing it and applying suction to it. As at 1991 I was not aware of a medical application of suction in this way.”
159 At trial, Professor Marshall acknowledged that, as at 1991, drainage of an open wound could be effected by using a sump drain in an open wound by open suction, as described above. He stated that in that situation he did not seal the wound, because:
As a surgeon of that era, I would not have thought of putting a seal over it because it was draining to a certain degree anyway by being open, and if I wanted to protect the skin around it, I would organise some sort of suction device which would stop the fluid from getting onto the skin. So I wouldn’t want to put a sheet onto the skin to close it because that may make, in my eyes, would perhaps have made it worse…
160 When asked if it would be natural to put a seal over the top to maintain the suction, Professor Marshall replied:
With hindsight, it astounds me that I didn’t think to do it, but I assure you that at the time, because I was so steeped in the notion that I could use suction within a closed surgical wound and that an open wound was a different thing that could drain on its own, I have to confess to you, I did not make that connection.
161 Professor Stacey, in his affidavit, deposed that:
[As at the late 1980s]… [D]rainage bottles with vacuum were used to remove fluid from cavity wounds which were closed surgically in order to remove excess blood or tissue fluid and to maintain appropriate moist wound environments. I used wall suction to create the negative pressure in the drainage bottle, or pre-vacuumed bottle… The seal was maintained by suturing the edges of the wound together. Sometimes the wound was covered with a seal, such as Opsite or similar, as a protective measure.
162 Professor Stacey deposed that he also recalled, as at the late 1980s at Fremantle Hospital, small, portable electric pumps were used, primarily in chest drainage systems:
I do not recall the brand name of the pumps, but I and other staff at the hospital called them portable pumps. I recall, in particular, the system was used by a doctor called Dr Nazir Ahmed in 1985, before I left Perth to take up a role at St Thomas’ Hospital in London in or about April 1986. I observed Dr Ahmed connect the pumps to a sealed bottle using a tube to obtain the suction or negative pressure level required. He then attached a second tube from that sealed bottle and connected this to a tube that had been inserted into the patient’s wound to remove fluid. The wound was sutured together so that negative pressure could be maintained in the wound cavity. Sometimes a seal such as Opsite was used as a protective dressing over the wound.
163 Mr Osmond, in his second affidavit, deposed as set out above: see [155].
164 On the basis of the evidence of Dr Williams, Professor Penington, Professor Marshall and Professor Stacey, I am satisfied that prior to 1991 foams, including Lyofoam and Allevyn, were widely available and were not uncommonly placed on certain types of wounds such as skin grafts, diabetic foot ulcers and other types of ulcers in order, as Professor Stacey emphasised, to maintain an appropriate moist wound environment at the surface of the wound.
165 Thus, as KCI submitted, it was not common practice to place foam inside wounds prior to November 1991, although it was used by some practitioners to cover wounds such as skin grafts and various kinds of ulcer. Accordingly, I find that the use of such foams on wounds other than skin grafts and ulcers, and in wounds rather than on them, was neither commonly practised in Australia nor part of the common general knowledge as at 1991.
166 Further, I was not persuaded that it was a widespread or common practice to apply negative pressure to open wounds prior to November 1991. Dr Williams expressly deposed that active suction (negative pressure) was regularly used on open wounds in 1991. Dr Pohl agreed that active suction was used in that context (though suction was applied continuously, rather than in the method of the Patent). Professor Marshall’s evidence, however, (while somewhat contradictory, in that he at one point apparently conceded that he had sometimes used active drainage on open wounds), was predominantly to the effect that he did not regard it as the norm or usual practice. Mr Ellis explicitly rejected the assertion that negative pressure was applied to open wounds. Accordingly, in my view, (given that a practitioner such as Professor Marshall was not clearly conversant with, and an experienced wounds nurse such as Mr Ellis was ignorant of, the practice) on the weight of the evidence, negative pressure was applied, only to a very limited extent, to open wounds as at November 1991. I conclude that the application of active suction to an open wound was not part of the common general knowledge prior to the priority date.
167 The expert evidence on the purpose of drainage was broadly consistent. In 1991, drainage was immediately directed at the removal of fluid, rather than the promotion of wound closure through the maintenance of active suction. While drainage did promote the normal growth of granulation tissue by removing the impediment to normal wound healing posed by fluid build-up, and thus served the ultimate goal of wound healing, the treatment was maintained only while there was excess fluid in the wound.
168 I am satisfied that, on the basis of Dr Williams’ evidence, both tubes and a sealing means (namely Stomahesive paste or Stomahesive tape) were used as at 1991 to facilitate suction of fluid in the context of open wounds. The use of an adhesive to seal at least certain types of wounds as at 1991 was also supported by the evidence of Professor Stacey and Mr Osmond.
169 Professor Marshall was, however, unaware of use of a seal in the context of a suction device to remove fluid from wounds as at 1991, and perforce did not himself use one. While the evidence established that tubes were used for closed wounds, only Dr Williams was aware of their use in open drainage systems. I conclude that the use of seals and tubes in open drainage systems was not part of the common general knowledge as at 1991.
170 The principles governing the construction of claims are largely settled and were not in dispute. The proper construction of a patent is a matter of law (see DÉcor Corporation Pty Ltd & Anor v Dart Industries Inc (1988) 13 IPR 385 (“DÉcor”) at 400), but as it is to be undertaken by a person skilled in the art or science to which the specification relates, it is usually the subject of expert evidence: see Vidal Dyes Syndicate Ltd v Levinstein Ltd and Read Holliday & Sons Ltd (1912) 29 RPC 245 at 272.
171 If the terms of the claim are clear and unambiguous, it is neither necessary nor permissible to refer to the main body of the specification to construe them.
172 In DÉcor, the Full Federal Court rejected the appellants’ contention that a specialised meaning given to a term in the specification also applied to the term when used in the claims. In the main body of the specification, a flexible disc included in the plastic sealing lid (the subject of the respondent’s patent) was described as “biased, corrugated, fluted or similar”, but the claims described the disc as requiring “a biased area radially emanating from a central portion thereof”.
173 The Full Court rejected the appellants’ submission that their article did not infringe the relevant claims because its disc was smooth and featureless and, (while neither corrugated nor fluted), was not “biased”, because the word “biased” in the specification indicated “having a tendency to collapse upon itself” and should be interpreted thus in the claims.
174 Lockhart J (at 391) stated:
In one sense it is right to say that the specification must be read as a whole, but the specification is a whole made up of several parts and those parts have different functions. It is not legitimate to reduce or enlarge the meaning of the words of a claim by glosses derived from other parts of the specification, or to confine the scope of the claims by reference to some limitation which may be found in the body of the specification but is not expressly or by inference reproduced in the claims themselves. In ascertaining the width of a particular claim it is not permissible to vary or qualify the plain and unambiguous meaning of the claim by reference to the body of the specification: Welch Perrin & Co Pty Ltd v Worrell (1961) 106 CLR 588, per Dixon CJ, Kitto and Windeyer JJ at 610. However, if an expression in the claim is not clear, it is then permissible to resort to the body of the specification in order to define or clarify the meaning of words used in the claim without infringing the rule that clear and unambiguous words in the claim cannot be varied or qualified by reference to the body of the specification.
175 Lockhart J (with whom M L Foster J agreed on those issues) found (at 392) that the word “biased” in the claims (construed in isolation from the body of the specification) bore its dictionary meaning of an “oblique or slanting line”. It was neither unclear nor ambiguous in the context of the claim, and thus it was “neither necessary nor permissible to construe the term in the light of the body of the specification that precedes the claims” (at 392). Had it been necessary to do so, it would not have altered Lockhart J’s construction.
176 M L Foster J (at 419) stated:
I am by no means persuaded that it is legitimate, in this case, to look beyond the wording of the claims to determine their construction. I doubt that any relevant ambiguity exists requiring recourse to other portions of the specification to explain it.
177 His Honour nevertheless considered (at 421) the specification and observed that the passages said to be the source of the highly specialised meaning of the word “bias” in the relevant claim all dealt with the preferred embodiment, the description of which indicated that “biased” was not intended to be synonymous with “fluted or corrugated”, but rather, was used interchangeably with “conical”. As the appellants’ closure was biased in the sense of being conical, it was not saved from infringement because it lacked the corrugations and flutings specified in the preferred embodiment (at 422).
178 Sheppard J also ultimately found that the description of the preferred embodiment did not require the word “biased”, when used in the claims or elsewhere, to bear the special meaning of similar surfaces when corrugated or fluted.
179 In Welch Perrin & Co Pty Ltd v Worrel (1961) 106 CLR 588 (“Welch Perrin”), Dixon CJ, Kitto and Windeyer JJ stated (at 609) that:
[I]n every patent case, it is necessary to determine from [the specification] what exactly is the invention it describes and for which a monopoly is claimed, before proceeding to consider objections to the validity of particular claims.
180 In Welch Perrin, the appellant argued that the specification was muddled and ambiguous. The High Court acknowledged (at 610) that:
If it is impossible to ascertain what the invention is from a fair reading of the specification as a whole, that, of course, is an end of the matter. But this objection is not established by reading the specification in the abstract. It must be construed in the light of the common knowledge in the art before the priority date.
181 Their Honours noted (at 610) that the specification was not:
a written instrument operating inter partes, but a public instrument which must, if it is to be valid, define a monopoly in such a way that it is not reasonably capable of being misunderstood… But it is a whole made up of several parts, and those parts have different functions. Courts have often insisted that it is not legitimate to narrow or expand the boundaries of monopoly as fixed by the words of a claim by adding to those words glosses drawn from other parts of the specification. Similarly, if a claim be clear it is not to be made obscure simply because obscurities can be found in particular sentences in other parts of the document.
182 In Kimberly-Clark Australia Pty Ltd v Arico Trading International Pty Ltd (2001) 207 CLR 1 (“Kimberly-Clark”), the High Court affirmed at 16:
It is well settled that the complete specification is not to be read in the abstract; here it is to be construed in the light of the common general knowledge and the art before... the priority date; the court is to place itself “in the position of some person acquainted with the surrounding circumstances as to the state of [the] art and manufacture at the time”.
183 In Sachtler GmbH and Co KG (formerly Sachtler AG) v RE Miller Pty Ltd (2005) 65 IPR 605, Bennett J recently summarised the principles as follows (at 613 and 614):
• When determining the nature and extent of the monopoly claimed, the specification must be read as a whole. As a whole it is made up of several parts and those parts have different functions. The claim, cast in precise language, marks out the legal limits of the monopoly granted by the patent. What is not claimed is disclaimed. The specification describes how to carry out the process claimed and the best method known to the patentee of doing that.
• Although the claims are construed in the context of the specification as a whole, it is not legitimate to narrow or expand the boundaries of monopoly, as fixed by the words of a claim, by adding to those words glosses drawn from other parts of the specification. If a claim is clear and unambiguous, it is not to be varied, qualified or made obscure by statements found in other parts of the document.
• Terms in the claim which are unclear may be defined or clarified by reference to the body of the specification.
• Reference may be made to the body of the specification to understand the context in which words have been used.
• It is legitimate to refer to the rest of the specification to explain the background to the claims, to ascertain the meaning of technical terms and to resolve ambiguities in the construction of the claims. Where the language of the claim is obscure or doubtful the doubt is sometimes resolved by referring to words in the body of the document to explain it.
• It is not necessary first to construe the claims without reference to the specification and then to determine whether or not ambiguity exists.
• There is a fine line between, on the one hand, reading down the words of a patent claim to reflect how a person skilled in the art would understand it in a practical and commonsense way and, on the other hand, impermissibly limiting the clear words of a claim because a reader skilled in the art would be likely to apply those wide words only in a limited range of all the situations they describe.
• The construction of the claim determines infringement, on both textual and substantive bases. It is a question of whether the alleged infringement is covered by the language of the claim.
• A patent should be given a purposive construction. However, that does not involve extending or going beyond the definition of the technical matter for which the patentee seeks protection in the claims. The question is always what the person skilled in the art would have understood the patentee to be using the language of the claim to mean. For this purpose, the language chosen is usually of critical importance.
• Purposive construction, permitting consideration of whether the person skilled in the art would understand a variant that does not strictly comply with the particular descriptive word used in the claim may still fall within the monopoly, does not arise where the variant would in fact have a material effect upon the way the invention worked.
(citations omitted)
184 It is thus an accepted principle that the purpose of the specification and the knowledge of the skilled addressees are relevant to the construction of the specification.
185 In Catnic Components Ltd & Anor v Hill & Smith Ltd [1982] RPC 183 at 242-3, Lord Diplock observed that in the specification, the patentee, in words of his own choice, informed those skilled in the art of the essential novel features (or “pith and marrow”) of the invention. His Lordship described the purposive approach to construction of the specification as follows:
A patent specification should be given a purposive construction rather than a purely literal one derived from applying to it the kind of meticulous verbal analysis in which lawyers are too often tempted by their training to indulge. The question in each case is: whether persons with practical knowledge and experience of the kind of work in which the invention was intended to be used, would understand that strict compliance with a particular descriptive word or phrase appearing in a claim was intended by the patentee to be an essential requirement of the invention so that any variant would fall outside the monopoly claimed, even though it could have no material effect upon the way the invention worked.
186 His Lordship concluded that if it were apparent to skilled readers that a term could not have been intended to exclude a minor variant which obviously would not affect how the invention worked, strict compliance with the particular description was not required.
187 In Kirin-Amgen Inc v Hoechst Marion Roussel Ltd (2004) 64 IPR 444 (“Kiren-Amgen”) at 454-455, Lord Hoffman observed that a purposive construction could not legitimately extend the subject of the monopoly claimed. His Lordship stated:
“Purposive construction” does not mean that one is extending or going beyond the definition of the technical matter for which the patentee seeks protection in the claims. The question is always what the person skilled in the art would have understood the patentee to be using the language of the claim to mean. And for this purpose, the language he has chosen is usually of critical importance. The conventions of word meaning and syntax enable us to express our meanings with great accuracy and subtlety and the skilled man will ordinarily assume that the patentee has chosen his language accordingly. As a number of judges have pointed out, the specification is a unilateral document in words of the patentee's own choosing. Furthermore, the words will usually have been chosen upon skilled advice. The specification is not a document inter rusticos for which broad allowances must be made. On the other hand, it must be recognised that the patentee is trying to describe something which, at any rate in his opinion, is new; which has not existed before and of which there may be no generally accepted definition. There will be occasions upon which it will be obvious to the skilled man that the patentee must in some respect have departed from conventional use of language or included in his description of the invention some element which he did not mean to be essential. But one would not expect that to happen very often.
188 In the present case, S&N submitted that the circumstances invoking a purposive construction were not present as there was no question of assessing the effect of a variant on the working of the invention. Rather, in the present case, it was simply a question of whether or not the principal disputed integer were present.
189 Further, as S&N submitted, no subsequent authority has modified the High Court’s recognition in Kimberly-Clark that the plain and unambiguous meaning of a claim cannot be varied or qualified by reference to the body of the specification, although the latter may be used to define or clarify terms in the claim which are unclear.
190 The construction of a patent is thus governed by the principles of Welch Perrin and Kimberly-Clark which, although acknowledging that the patent should be read in context, purposively and as a whole, preclude the limitation or expansion of claims by a gloss drawn from the body of specification.
191 Although the documents comprising the Patent must be read as a whole, each has a different function. By s 40 of the Act, while the specification as a whole describes the invention and the best method of performing it known to the applicant, the claims define it.
The hypothetical addressee of the Patent
192 It was common ground that in this case, the specification was addressed to a clinician experienced in wound care (of which a plastic surgeon was a good exemplar), assisted, where necessary, by a biomedical engineer, such as Dr Wilkins, in his or her understanding of the physics of negative pressure as it applied to the foam and its interface with the wound bed. It was not disputed that such a clinician constituted the non-inventive, skilled worker in the relevant field, and was the hypothetical addressee contemplated in the analysis in Kimberly-Clark at 16.
193 On that basis, Professor Marshall, Dr Pohl, Professor Penington, Professor Stacey and Professor Kimble (assisted where required by Dr Wilkins) were all relevant addressees.
194 The hypothetical addressee is taken to read the specification with the common general knowledge of persons skilled in the relevant art, knowing that its purpose is to describe and demarcate an invention.
195 Although skilled in the art and with practical knowledge and experience, the hypothetical addressee is unimaginative and without inventive capacity.
196 S&N acknowledged that the Patent was concerned with assisting wound healing by using NPWT, which worked by promoting or encouraging the growth of granulation tissue, and that, in the context of the apparatus, the foam placed in the wound with the application of negative pressure assisted that process.
197 S&N nevertheless submitted that the language of the claims was central, and that some central integers were (by reference to any cogent scientific or medical theory) obscure, unclear or meaningless and would, according to the more persuasive expert evidence, be so construed by the hypothetical addressee. Other integers simply amounted to claiming “that which naturally happens”.
198 S&N contended that various integers were introduced into claims merely in order to overcome the effect of prior art (which would otherwise render them invalid). Most importantly, the screen rigidity integer common to all claims in suit was nonsensical and a limitation by result, which simply did not occur.
199 S&N also initially challenged the common integer of a screen means sufficiently porous to allow gases to reach the wound (“screen porosity integer”) on a similar basis but, as discussed below, ultimately conceded that it was valid and present in its products.
200 S&N submitted that KCI had attempted substantially to redefine the screen rigidity integer and a number of other integers to ascribe some meaning to accord with the evidence.
201 S&N submitted that in particular, on KCI’s case, a screen means for preventing overgrowth of tissue in a wound should be read as “a screen means for modulating growth of tissue in a wound so that a clinician can remove the screen means to prevent overgrowth”; a screen means “sufficiently porous to allow gases to reach the wound” should be read as a screen means “sufficiently porous to allow air to pass through the screen means”; “sufficiently rigid to prevent wound overgrowth” should be read as “sufficiently rigid to modulate wound overgrowth”; “time sufficient to promote migration of epithelial and subcutaneous tissue toward the wound” should be read subject to the rider “by excluding such migration caused by drainage from the wound”; and “time sufficient to facilitate closure of the wound” should be read subject to the rider “said facilitation excluding any cleaning or draining of the wound”.
202 S&N also alleged that a number of other integers in various claims were inessential, because they were arbitrary matters of clinical judgment or mere desiderata. (Therefore, although failure to take such integers would not preclude infringement, if S&N took all the essential integers of a claim, absence of the inessential integers in the prior art would not preclude anticipation of the relevant claims).
203 It is convenient to consider the principal disputed integers separately.
Construction of screen rigidity integer
204 As stated above, S&N submitted that the screen rigidity integer was added to the combination claims only in order to overcome the criticisms of the Examiner and the prior art which would otherwise deprive the patent of novelty, but the integer, which was common to all the combination claims in suit, was exposed as nonsensical by the evidence.
205 In contrast, KCI relied on Professor Marshall (and to a lesser extent on Dr Pohl), in order to establish that the screen rigidity integer was both valid and present in S&N’s product. Although the evidence on those issues overlaps, I discuss them separately.
206 In my opinion, Professor Marshall’s evidence concerning the meaning of wound overgrowth and the operation of the screen means sufficiently rigid to prevent it was shifting, relatively vague and, ultimately, unpersuasive. Dr Pohl’s evidence was to some extent inconsistent with that of Professor Marshall and also unpersuasive. For the reasons discussed below, I preferred the contrary evidence of other expert witnesses, principally Professors Stacey, Penington and Kimble.
207 Because the screen rigidity integer is central both to the infringement and invalidity cases, and in that sense potentially dispositive of the entire proceeding, it is convenient at this point to consider in detail the conflicting submissions and evidence on that crucial integer. In order to understand the integer it is necessary to determine the meaning of both wound overgrowth and a screen means which is sufficiently rigid to prevent that phenomenon.
208 As was clear from the terms of the Patent, it promised a trilogy of benefits comprising stimulation of granulation tissue, prevention of wound overgrowth and closure of the wound.
209 KCI contended that the word “for” both in the detailed description and in the claims meant “suitable for achieving the purpose of” preventing the overgrowth of tissue. KCI submitted that there was no inconsistency between stimulation of “growth of granulation tissue” and the screen’s prevention of “wound overgrowth” although the latter was simply an excess quantity of the former. It submitted that the screen should first be viewed as a barrier which “controls the growth of weeds on the way up to the top” which, although its removal required the exercise of clinical judgment, was a tool that armed the physician with the capacity to stop hypergranulation.
210 KCI submitted that an aspect of the screen’s rigidity was that it did not collapse on itself and was capable of transmitting even pressure.
211 Additionally, and somewhat inconsistently, KCI at one point submitted that the screen should not be construed as stopping overgrowth and S&N’s witnesses had erred in interpreting it thus, while at another point, KCI submitted that “rigidity… is the aspect that stops overgrowth”.
212 KCI ultimately submitted that the integer must be construed in a practical, commonsense way as a screen “which is suitable, when used by a clinician, for controlling the unwanted upward growth of granulation tissue so that it develops in an even and controlled manner…”. As overgrowth did not occur in practice when the device was used, in KCI’s submission, the practical approach required in Olin Corporation v Super Cartridge Co Pty Ltd (1977) 180 CLR 236 supported that construction and no complicated assessment or trial was required. It sufficed to visually inspect the screen or dressing and determine whether it had the requisite structural integrity to resist the compressive load exerted when the device was operating.
213 Professor Marshall and Dr Pohl gave evidence, supported or amplified by that of Dr Wilkins, that the KCI foam possessed the screen rigidity integer and functioned to prevent wound overgrowth.
214 Professors Penington, Stacey and Kimble denied that the screen means or foam could or did prevent hypergranulation or indeed, granulation.
215 Professor Marshall, who had read the Patent according to the state of knowledge as at 1991, discussed, in his first affidavit, the requirement that the screen means be placed over the expanse of the wound to prevent its overgrowth.
216 Professor Marshall described wound overgrowth as the “over-proliferation of granulation tissue”, and noted that granulation tissue could sometimes “over-proliferate to the extent that it bulges above the level of the surrounding skin”.
217 He stated that although he would not have personally used the term “wound overgrowth” or “overgrowth” in 1991, he would have understood it to refer to “the over-proliferation of granulation tissue”. He deposed:
In an ideal case, granulation tissue grows relatively evenly across a wound bed [but] in some circumstances granulation tissue develops faster in some regions of the wound than others, or potentially not at all… However granulation tissue can sometimes over-proliferate to the extent that it bulges above the level of the surrounding skin… Consequently, as at 1991 I would have understood the term ‘prevention of wound overgrowth’ to mean the development of even and controlled granulation tissue without over-proliferation.
218 Professor Marshall referred to the rigidity of the screen (preferably open-cell polymer foam) being important for preventing wound overgrowth and deposed that having read the detailed description in the Patent “would have recognised that to prevent overgrowth the screen must have sufficient rigidity or structural firmness to transmit even pressure onto the wound bed and not collapse in on itself”. He stated that “[t]herefore the screen needs to be sufficiently rigid or firm to resist the downward force of the seal under vacuum to ensure that the pressure exerted by the seal is transmitted evenly to the wound bed”.
219 In his second affidavit, Professor Marshall reiterated that the requirement of a screen means sufficiently rigid to prevent wound overgrowth meant a screen sufficiently rigid to prevent wound overgrowth during the application of the treatment by its ability to transmit the pressure exerted by the seal evenly to the wound bed (and, while a seal was not mentioned in claim 1, it was implicitly necessary to apply the negative pressure).
220 Professor Marshall stated that the application of pressure to a wound could affect granulation tissue and in his experience prior to 1991, applying a pressure dressing would result in less granulation tissue.
221 Professor Marshall confirmed that in his experience, the application of the V.A.C.® therapy in conjunction with the foam dressing prevented the overgrowth of granulation tissue.
222 Professor Marshall did not understand the Patent to teach that the claimed methods of treatment prevented the growth of granulation tissue, but rather “the overgrowth of granulation tissue (hypergranulation)”. In the light of his experience in 1991, Professor Marshall would have understood that the plastic surgeons still needed to decide when the amount of granulation tissue was “appropriate for the next step in the wound healing process”. Ultimately, Professor Marshall did not see the treatment as purporting (as he took Professor Kimble to maintain) simultaneously to promote and to prevent granulation tissue growth.
223 In cross-examination, Professor Marshall stated that he believed that “the negative pressure through the interstices of the foam applied to the surface of the wound… is encouraging the granulation tissue”.
224 He did not think that the growth of tissue up into the mesh of the foam could become hypergranulation, as “overgrowth is where the granulation tissue grows above the level of the epithelium of the wound”, and if there were any “islands of granulation tissue” above that level, even if only two or three millimetres above the surface of the skin, “they are above the epithelium and I would call that hypergranulation”.
225 Professor Marshall gave evidence that he rarely saw hypergranulation in his own practice, even prior to 1991, because he changed the dressings before the granulation reached that stage, although he saw hypergranulation in poorly managed cases that were referred to him. Hypergranulation was a problem only “uncommonly”. He removed hypergranulation by using a scalpel rather than using silver nitrate.
226 In his own practice, before the advent of V.A.C.®, Professor Marshall exercised his clinical judgment to change the dressing to avoid overgrowth, and, when using V.A.C.®, believing that hypergranulation was undesirable, he prevented it by applying a force to the wound bed, and exercised clinical judgment to remove the dressing at an appropriate time. Professor Marshall expressly agreed, however, that even with V.A.C.® therapy, hypergranulation could occur if the pressure were kept on. Professor Marshall stated that granulation tissue could grow “exuberantly” and too quickly. When asked to explain how the screen or foam could both promote the growth of granulation tissue and prevent hypergranulation, (that is, result in “net good granulation tissue, but no hypergranulation”), Professor Marshall stated:
I think it ends up because the positive pressure is preventing the hypergranulation but the negative pressure is encouraging granulation, and because the – it is able to suck away debris and discharge, it is creating an environment in which the granulation tissue can grow into the small interstices but can't grow too exuberantly because the sponge, the solid part of the sponge, is pushing down slightly.
227 Professor Marshall conceded that he had no expertise in physics. He had difficulty in explaining how the Figure 2 CPR mask depicted in the Patent (which was used in many of the examples referred to in the Patent) would push down to prevent wound overgrowth according to his theory, unless it were filled with foam. Professor Marshall stated in that context that the foam slowed the general growth upwards of the whole wound bed, and it was a matter of clinical judgment to stop it before it got above the surface of the surrounding good tissue. He agreed that “it’s not stopping hypergranulation per se; it modulates the growth until the surgeon chooses to intervene…by taking the dressing off.”
228 Professor Marshall stated that some areas of granulation tissue developed faster than others and applying a certain amount of pressure to a wound encouraged an even growth. He envisaged that while positive pressure was applied, the height above the wound base level was held back a little, but it was also slowly increasing.
229 Ultimately, Professor Marshall stated that he took overgrowth of tissue in the Patent to mean the following:
You will notice that in the earlier sentence I used the term, "proliferative granulation" in that same paragraph. In other words, what I regard as hyper – I accept the definition that everyone seems to want to use that once granulation tissue is above the level of the surrounding skin you can certainly call it hypergranulation but –
230 The following exchange then occurred:
HER HONOUR: But, professor… is that simply a particular stage that hypergranulation has reached?
Correct.
But more generally, hypergranulation means over exuberant or biologically growing too fast?
Correct.
Or too proliferatively?
Correct. Correct, your Honour. You could liken it to the growth of weeds in a paddock. Once the weeds are above the level of the fence you could say they are overgrown, but everyone knows that they are growing to get to that point.
231 Professor Marshall agreed that, in his affidavit, he described overgrowth as over-proliferating “to the extent that it bulges above the level of the surrounding skin”, which he would call “hypergranulation”. He conceded that in the course of the evidence, he had modified his definition of overgrowth from granulation tissue growing above the level of the epithelium of the wound.
232 Professor Marshall appeared, at one point, to maintain that overgrowth could include proliferation below the level of the epithelium, but stated “it is a continuing process and the point comes at some stage in that proliferation when it becomes undesirable that the level of granulation tissue and, yes, one would then call it hypergranulation… Or in terms [of the Patent], overgrowth”.
233 Ultimately, over the course of cross-examination, Professor Marshall:
(a) conceded that the foam did not stop hypergranulation per se, but rather “modulated” the growth of granulation tissue until such time as the clinician intervened to stop it from rising above the surface of the surrounding tissue;
(b) agreed that the modulation of granulation tissue growth was due to the combination of the positive pressure of the foam and the negative pressure of the vacuum;
(c) agreed that he had not seen overgrowth of granulation tissue in his own clinical practice partly due his practice of “getting there in time to forestall it”;
(d) stated he would not submit to a peer reviewed journal his conclusion that S&N’s product was sufficiently rigid as to prevent wound overgrowth; and
(e) conceded that there is no valid scientific proof that the V.A.C.® therapy prevented wound overgrowth because of the rigidity of the foam alone.
234 Dr Pohl, who was requested to read the prior art documents prior to reading the Patent, described what the Patent would have taught him, given his knowledge and experience in 1991.
235 Dr Pohl deposed:
The Patent states that the invention includes an apparatus for facilitating the healing of wounds and the way the apparatus works is explained… The Patent states that the apparatus includes a screen means which will prevent the overgrowth of tissue in the wound… From my reading of the Patent, I would have understood the term "screen means" to be a reference to an open-cell polymer foam and the phrase "overgrowth of tissue" to refer to hypergranulation. As at 1991, it was my experience that granulation tissue will naturally try to fill up space in a healthy wound and if left untreated, it will heap up in the wound so that it sits above the skin surface. This is called hypergranulation. Although hypergranulation occurred in some wounds, it was not a significant problem from a surgeon's perspective because it could be scraped back. As at 1991 in Australia, hypergranulation was not uncommon and I would have seen between two and three examples of this each year. It usually occurred in neglected wounds, that is wounds that had not been attended to within a normal space of time and it was therefore more common for me to see this in the third world when travelling with Interplast…
The Patent states that the screen means can be formed from a variety of porous semi-rigid materials… I would have understood that the foam needs to be porous in order for the negative pressure to exist throughout the foam. This would ensure that the negative pressure was present at the whole screen/wound interface. It also needs to be semi-rigid so that it can fill the wound cavity.
The Patent states that the screen means must be sufficiently rigid to prevent wound overgrowth… As at 1991, I would have read this as meaning that a degree of rigidity is required for the foam to expand to fill the wound, including the under-surface of the wound. Wounds are rarely as simple as the diagrammatic depictions in Figures 1 and 2 of the Patent. A wound can be like an `iceberg' in the sense that there can be a small defect in the skin surface, but a large cavity beneath. The foam has to be able to conform to wound defects of complex shape. I also would have understood from the Patent that the foam acts to moderate granulation tissue. Where there is no or poor granulation tissue, the device encourages its growth but the pressure that is put on the wound by the device through the foam would also prevent overgrowth of granulation tissue. The pressure from the atmosphere pushes down on the seal (because you have negative pressure in the wound) and this pushes down on the foam. The foam therefore allows transmission of the pressure that arises from the difference between atmospheric pressure above the seal and negative pressure below the seal, to the foam-wound interface via the fibres of the foam. I would also expect negative pressure to be present at the foam-wound interface in the pores of the foam between the fibres of the foam. As granulation tissue grows, this would become a foam-granulation tissue interface and the granulation tissue would experience the pressure. To be able to push down on the wound, the foam has to have the right physical properties to transmit the pressure from the seal.
236 In cross-examination, Dr Pohl stated that he understood that a “screen means sufficiently rigid to prevent overgrowth” meant that the screen used with the vacuum “promotes granulation tissue to grow into the wound. But the pressure exerted by the vacuum itself on the sides of the wound limits excessive granulation tissue from growing” as the screen was pushed down to the sides of the wound. The granulation tissue grew into the screen means due to the dual effect of the vacuum and the foam.
237 Thus, in Dr Pohl’s opinion, the pressure encouraged granulation tissue to grow into the screen and the inert pressure of the foam also may have encouraged it, but the two systems pointed in opposite directions, with the vacuum “drawing fluid and tissue and encouraging granulation tissue to accumulate”, while also “pressing on the actual dressing pushing down onto the bed and the walls of the cavity”.
238 Dr Pohl conceded that the process was confusing. He acknowledged that it would be a “nice balance” in judging the degree of rigidity that the foam must possess to support the two modes of growth in opposite directions.
239 Dr Pohl stated that hypergranulation tissue was never seen when using the vacuum dressing with the foam, but only in untreated wounds. The treatment progressed to a stage when the clinician could judge that a wound was ready for reconstruction or would close by itself. He described the prevention of wound overgrowth as a “by-product of the system”.
240 Dr Pohl stated that it would be a matter of “trial and error” to select a foam that was, on the one hand, sufficiently rigid to stop hypergranulation (a rare condition occurring on small wounds) but which, on the other hand, encouraged good granulation.
241 Dr Pohl was asked to explain how the Figure 2 CPR mask embodiment of the invention, which was used in the majority of the examples, would prevent wound overgrowth consistently with his theory that the screen prevented wound overgrowth by the material pushing down. As the cup was semi-rigid plastic designed not to collapse, it would not push down on the surface when negative pressure was applied unless it were filled with foam, which, as Dr Pohl acknowledged, the Patent did not describe.
242 Although with use of the Figure 1 embodiment, the seal would come down and overlie the wound, Dr Pohl acknowledged that in contrast, “the cup is semi-rigid as you stated and would stay up unless you filled it completely with foam and then applied vacuum… [in which case it would] have enough material in it to make contact.”
243 Dr Pohl explained that the screen rigidity integer referred to two operating factors, namely, the vacuum exerting negative pressure on the wound (which encouraged tissue to grow into the foam) and actual pressure created in the environment on the walls of the wound (which prevented excessive granulation tissue).
244 Dr Pohl said that in 1991, he would have used trial and error to select foam with the right degree of rigidity for its pores to enable granulation tissue to grow up, while the solid areas would push down on the wound. Alternatively, he would have gone back to the Patent to see whether it accurately described the foam.
245 Professor Kimble was also asked to read the Patent as he would have understood it in 1991. Professor Kimble made the overriding observation that, in his opinion, the Patent was “very poorly written” and did not use the language he would “expect to see in a medical patent or a scientific paper”. He further deposed:
If I had read the Patent in November 1991, not having the advantage of having used the system apparently described in the Patent, I would have found it difficult to follow. The scientific concepts are confused and at times without proper basis and the description of the apparatus in the claims is unclear. For example, I would not know what dressing to select if I was directed to select one that was "sufficiently rigid to prevent wound overgrowth". Further, the examples set out in the Patent do not provide any guidance as to whether the Patent actually achieves its stated purpose.
...
First, the phrase "overgrowth of tissue" is not a proper or common medical term. It is more than likely a reference to the growth of excess granulation tissue, which is generally called hypergranulation. Hypergranulation is uncommon and occurs in circumstances that cannot be predicted. When it occurs, granulation tissue grows across the base of the wound in the standard, desirable manner to begin with, but for some reason the granulation tissue keeps growing upwards, generally to above the surface of the skin surrounding the wound. I generally use chemicals such as silver nitrate to destroy the excess granulation tissue thus allowing the skin cells (kerationcytes) to grow across.
Secondly, I do not believe that such a thing exists as a "screen means for preventing overgrowth of tissue". I have used both the gauze and foam dressings with negative pressure therapy and I have observed that the rate of granulation tissue increases with both dressings when compared to wounds on which negative pressure therapy is not used. I cannot accept that negative pressure therefore prevents hypergranulation because my clinical experience is that negative pressure encourages granulation tissue growth. I am not aware of any sound evidence that explains why it does this but I observe that this happens. My own view is that the negative pressure in fact causes a decrease in the rate of blood flow (perfusion) to the wound area. As blood flow decreases, the granulation tissue, which is comprised of blood vessels, grows into the wound cavity, to increase the blood supply to the wound.
246 In examination in chief, Professor Kimble amplified his views on the phrase “screen means sufficiently rigid to prevent wound overgrowth”. He stated, inter alia, that the overgrowth of tissue was not a medical term and in the Patent appeared to refer to overgrowth of granulation tissue, the medical term for which was “hypergranulation, where the tissue actually goes beyond the original margins of the wound, usually up the way”.
247 In relation to the concept of a screen means sufficiently rigid to prevent wound overgrowth, Professor Kimble stated:
What they are really saying is that by applying this, you will prevent the overgrowth of granulation tissue. However, that does not mean anything to me at all, simply because the product is advertised – in the patent it says, encourages the formation of granulation tissue and they use one of their studies at the beginning to show that. I think that is study 1 which they use, it says it promotes the formation of granulation tissue. But in this statement, they're saying they're actually preventing the overgrowth of granulation tissue, so it makes no sense to me, and certainly in clinical practice, a negative pressure device will encourage a wound to form granulation tissue and if you use it for long enough, it will always produce an overgrowth of granulation tissue. So the statement, as far as I'm concerned, is wrong.
248 In cross-examination, Professor Kimble said that granulation tissue would start to form invisibly in the first two days, not necessarily evenly, and, if left unchecked or uncontrolled, would eventually exceed the upper margins of the wound, which would be undesirable. It was a matter of judgment to stop clinical treatment before hypergranulation occurred.
249 Professor Kimble stated that some wounds did not form granulation tissue. Those with poorer blood supply formed more, and there could be an uneven formation with a particular wound. Professor Kimble thought that negative pressure encouraged the formulation of granulation tissue in response to tissue ischemia.
250 Professor Kimble considered the Patent lacked scientific rigour and exhibited major flaws. He considered that the application of negative pressure required a screen which was necessary for the migration of tissue and increased formation of granulation tissue, as the system could not work without a tissue dressing interface. In Professor Kimble’s opinion, if the foam making contact with the wound bed provided a substantial barrier to the upward growth of tissue, and worked as the inventors suggested, then “you wouldn't get any granulation tissue formed at all, never mind overgrowth”. In his view, it did not “work that way”, and if the pressure down on the screen prevented the overgrowth of granulation tissue, the “same force will prevent any granulation tissue forming in the first place”.
251 In Professor Kimble’s view “no screen that I know of prevents the overgrowth of granulation tissue because it's something we see in our wounds… With negative pressure devices, if you use them for long enough, you will get overgrowth of granulation tissue, hypergranulation”.
252 Professor Kimble himself, in using the device, stopped before granulation tissue reached that stage. He used his clinical judgment to cease using the screen before hypergranulation occurred. The intervention of the clinician, not the screen itself, prevented overgrowth or hypergranulation, which would often occur with the use of the screen if left on too long.
253 Professor Kimble stated that a wound was dynamic, and “simple physics” did not apply to it. Granulation tissue would grow despite the force down on it. He disagreed that the screen controlled the upward extent of growth.
254 He rejected the proposition that, if the claims did not assert that the screen was adapted to stop the growth of granulation tissue, then there was no inconsistency between the dual requirements of promoting the growth of granulation tissue and using the screen to prevent the granulation tissue overgrowing the margins of the wound (subject to clinical judgment).
255 Professor Kimble denied that the use of the foam and the downward compressive force where the foam made contact with the wound bed (as described by Dr Wilkins) could provide a substantial barrier to the upward growth of granulation tissue. He made clear that he did not interpret the language of the claim to mean that the screen must stop the growth of granulation tissue, but said that if it were true that enough pressure “down” with the screen would prevent overgrowth of granulation tissue, then it would also prevent any growth at all.
256 Professor Stacey, in his first affidavit, also addressed the meaning of overgrowth in November 1991, and considered that while it was not a medical term, he would have understood it to mean overgranulation or hypergranulation, which was an uncommon condition. He deposed:
"Overgrowth" is not a term used in medicine to describe tissue growth, nor is it used to describe any phenomenon that occurs with wounds. However, if I had heard the terms "overgrowth of tissue" and "wound overgrowth" before November 1991, I would have understood them to mean overgranulation or hypergranulation. Overgranulation or hypergranulation refer to the same thing. Hypergranulation occurs when the wound is still open. It is the rising up or overgrowth of blood vessels and connective tissue which comprise the granulation tissue, from the base of the wound, generally to above the level of the healthy skin surrounding the wound. Hypergranulation is uncommon and, in my experience, it is not considered a problem by most clinicians and is quickly and simply treated and cured when it arises.
While hypergranulation is not fully understood, hypergranulation is, and was before November 1991, usually attributed to the presence of infection in the wound (bacteria invading healthy tissue) or bacterial contamination in the wound (bacteria on the surface of the wound, which is more superficial than infection). While the wound is fighting the infection or bacterial contamination the epithelialisation process stops and the granulation tissue continues to grow. The bacteria stimulates responses within the wound that stop epithelial cells from migrating across the wound to close it over. Other reasons that hypergranulation is considered to occur are the presence of foreign bodies within the wound and the use of occlusive dressings on open wounds.
As at November 1991 I would have treated hypergranulation with a topical antimicrobial such as Inadine, or in the absence of infection, with topical steroids.
Hypertrophic scarring, which occurs once epithelialisation of the wound has occurred, and which I was aware of before November 1991, is more common than hypergranulation, particularly in relation to incisional wounds, healed open wounds and burns (particularly burns). The terms "overgrowth of tissue" and "wound overgrowth" could conceivably refer to hypertrophic scarring, since that condition also refers to a raised up area of skin caused by an abnormal healing response below the epithelial layer in the wound. Hypertrophic scarring is a more common condition than hypergranulation and it is more difficult to cure, particularly when it causes contracture across a joint or moving surface. It is generally treated with pressure garments and is sometimes treated with topical or intralesion injection of steroids or with surgery.
257 In relation to a screen means for preventing overgrowth of tissue in a wound, Professor Stacey stated that the term had no practical relevance to him and was unaware of evidence that a screen means could prevent hypergranulation. In his view, it would, in any event, be almost impossible to tell whether a screen means could prevent hypergranulation because hypergranulation was so uncommon. Professor Stacey deposed:
I was asked by Blake Dawson to assume for the purpose of interpreting this phrase that a "screen means" is a type of wound dressing. Prior to being told this I did not know what was meant by the term.
A wound dressing "for preventing overgrowth of tissue" has no practical relevance to me. As I have said, hypergranulation is an uncommon complication, so preventing it is not a treatment objective. There are many other treatment objectives, primarily encouragement of wound healing as quickly as possible, and those objectives, considered in the context of the wound under treatment, will define the nature of the wound dressing. In any event, there is no evidence of which I am aware that a "screen means" can prevent hypergranulation.
If I had been told to select a dressing that will prevent hypergranulation in November 1991 (or now for that matter) I would not have known what to select other than possibly a dressing which incorporated an antimicrobial agent. I do not think it is possible to select a dressing that prevents hypergranulation or hypertrophic scarring and I would ignore such a directive and select a dressing that suited the clinical circumstances, including the nature of the wound; the age of the patient; the patient's mobility needs; the amount of pain the patient was experiencing; the amount of exudate being produced by the wound; and whether the exudate was odorous (which is commonly an indication of the level of bacterial contamination).
258 In examination in chief, Professor Stacey amplified his views. He testified that proof that the frequency of a very uncommon condition had altered would require an “enormous study” and the recollection of observations which were, unless documented, unreliable.
259 In cross-examination, Professor Stacey stated that overgrowth of tissue and wound overgrowth were lay, rather than medical terms, and of potentially uncertain meaning, as “one is not always sure what that word means in one person’s mind as against another person’s mind”. In the Patent, however, Professor Stacey assumed that it referred to hypergranulation, albeit it could possibly refer to hypertrophic scarring.
260 Professor Stacey agreed that the normal interpretation of overgranulation was that “the upward growth of granulation tissue has exceeded the margins of the wound”. He stated “if you continued using this therapy, you would get overgranulation. So the therapy itself is not stopping it; the thing that stops it is your clinical decision to stop using the therapy.”
261 He agreed that the clinician would normally stop the therapy before hypergranulation or growth of granulation over the margins of the wound “but that, to me, doesn’t mean that the device is preventing overgranulation; it means you, as the clinician, are preventing overgranulation”.
262 Professor Stacey stated that hypergranulation was basically exactly the same tissue, cellularly and biologically, as normal granulation tissue, save that there was more of it. He stated:
Normally when you have hypergranulation, it is basically that you have exactly the same tissue being formed and the reason normally is the bio chemical signals for the cells to keep reproducing go unchecked or they are being continually stimulated to produce those signal pathways. In the normal wound healing process, that process is controlled and is shut down, but in wounds that overgranulate, for some reason it is persisting, so they just keep on producing the same types of tissue.
HER HONOUR: So that if a suitably trained person were to look at some granulation under a microscope, that person couldn't tell out of context whether it was hypergranulation or ordinary granulation?
No. Your Honour, that is my understanding. It may be if it has been there for a long period of time, it might take up some different protein structure which may be a little bit more of a scarring structure, if it has been there for a long time. But certainly as it is forming, no, I don't believe there is any difference that one could see under the microscope
263 Professor Stacey suspected that granulation tissue would not grow at a faster rate without the screen. When asked whether the foam screen at least provided a barrier to the upward growth of granulation tissue, Professor Stacey said:
[T]he points of contact have got an increased pressure above atmospheric. So one would make the assumption that at those points there would be less production of granulation tissue”. However, coming back to the points made earlier, the whole dressing system is sitting on the wound but not as a whole exerting a downward pressure. The granulation tissue can simply move, so that the downward pressure is only right at the point of contact, but beneath there is no increased pressure. So in fact the wound beneath can continue to produce tissue and move the whole thing upwards.
264 Professor Stacey stated that he viewed something rigid as being able to provide a barrier. It was not clear to him that the relevant phrase meant that the screen had to have sufficient structural integrity to prevent it collapsing on itself and occluding pores. He pointed out that that was different, in any event, from rigidity to prevent wound overgrowth.
265 In cross-examination, it was put to Professor Stacey that the “inventors were telling us” that the screen, (for example, foam) must have a sufficient structural integrity to allow downward force to be applied between the foam and the wound bed. Professor Stacey, in that context, apparently accepted Dr Wilkins’ evidence that there was increased downward pressure at contact points, and between them, reduced downward pressure. He appeared at that point to agree that when the application of negative pressure created simultaneous upward and downward forces, the barrier posed by the screen would inhibit the growth of granulation tissue due to its downward force. Professor Stacey also apparently conceded that the solid parts of foam would reduce the growth of granulation tissue but stated that he was not sure whether it was scientifically correct. I accept, however, that those responses (which were inconsistent with his clear earlier and later evidence) were on the qualified basis of Professor Stacey’s “reading” of Professor Wilkins’ theory of upward and downward pressure.
266 Professor Stacey subsequently made clear that he adhered strongly to his earlier views. He stated “I accept the things you have been saying, but when I read something that says “prevent wound overgrowth”, I interpret that as meaning preventing production of hypergranulation or production of granulation tissue”.
267 Professor Stacey again expressly rejected the proposition that because the clinician would remove the screen before hypergranulation occurred, the screen therefore (while the method and apparatus was in use) provided a barrier suitable for inhibiting granulation tissue from rising above the upper level of the wound. He stated: “I don’t think it is that that inhibits it; I think it is your clinical decision to remove it that stops it at that point”.
268 Professor Penington deposed in his second affidavit that the term “wound overgrowth” was neither a common term nor a term of art but it could describe a rare condition known as hypergranulation. He deposed:
I believe I had heard the term "wound overgrowth" before November 1991, however, it was not a term of art and not in common use then, or now. The term "wound overgrowth" may be describing the effect that I know as hypergranulation. This is also sometimes described as proud flesh or overgrowth. This is normal granulation tissue that does not stop growing in a wound when it should and ends up rising above the level of the surrounding skin/plane of the wound. I explain the process of granulation tissue formation further below. I was aware of hypergranulation before November 1991.
In my experience, hypergranulation is rare and I observe about 3 or 4 cases a year in my patients. When it does occur it only occurs at a very late stage of wound healing. Hypergranulation can occur in large open wounds and between the edges of the graft pieces in skin grafts made up of multiple skin pieces or between the edges of the graft and wound border. Usually if I see hypergranulation in one of my patients I will burn it off with a silver nitrate stick. It is also possible to remove it using other silver dressings such as Acticoat…
In the context of what I consider would have been my normal understanding of the term "wound overgrowth" in 1991, that is, as referring to hypergranulation, the term "a dressing for preventing overgrowth" would not provide any direction to me. Prior to November 1991 was not aware of any dressing that could prevent hypergranulation. The Acticoat dressing I have mentioned above was not available before November 1991.
269 In relation to the screen means sufficiently rigid to prevent overgrowth, Professor Penington deposed that the term made no sense and was meaningless to him. He deposed:
If I had been instructed to select a wound dressing in 1991 that had the characteristic of preventing wound overgrowth, I would not have known what this meant and consider I would not have been able to do so.
In the context of what I consider would have been my normal understanding of the term "wound overgrowth" in 1991, that is, as referring to hypergranulation, the term "a dressing that is sufficiently rigid to prevent wound overgrowth" is meaningless to me and makes no sense. If I had been instructed to select a wound dressing in 1991 that had the characteristic of being sufficiently rigid to prevent wound overgrowth, I would not have known what this meant and consider I would not have been able to select such a dressing. Furthermore, I would not have characterised many of the wound dressings that were available to me in 1991 as "rigid", for example, foam, gauze and cotton wool are not rigid in my opinion. One dressing that could be described as rigid is Quinaband, a bandage that is wrapped around a limb and which then hardens. This dressing is used in the treatment of venous leg ulcers, and has been since well before November 1991, often in conjunction with a pressure bandage. While this treatment seems to assist in the healing of venous leg ulcers, I would not have considered Quinaband to be a dressing that could prevent hypergranulation.
270 Professor Penington deposed that he had not seen any evidence that the use of the V.A.C.® device, or the foam dressing, prevented overgrowth. In his view, negative pressure therapy is generally only used on open wounds until they have progressed to the desired stage of healing (ie before hypergranulation occurs), so the absence of hypergranulation does not establish that the treatment has prevented it.
271 Professor Penington was not cross-examined on the above views at trial.
272 Dr Wilkins had no direct experience of NPWT in treating tissue damage as described in the Patent, but had worked extensively on portable vacuum pumps for wound drainage, surgical site drainage and airway clearing.
273 Dr Wilkins stated that:
When the suction pump is turned on, a partial vacuum will be drawn under the polymer sheeting. In other words, the pressure below the polymer sheet becomes less than the ambient atmospheric pressure above the sheet. The pressure inequality between atmospheric pressure above the sheet and the partial vacuum under the sheet causes the sheet to be pushed towards the wound cavity.
If the partial vacuum drawn is 100 mmHG, then an imbalance of pressures on the two sides of polymer sheet of 100 mmHG arises. The outside is subjected to 760 mmHG (atmospheric pressure), while the underside of the sheet is subjected to a pressure of 660 mmHG (atmospheric pressure less 100 mmHG). The polymer sheet will continue to be pushed towards the wound cavity until the suction under the sheet is balanced by the supporting force of the open-celled foam in the wound cavity. At that point, there is an equilibrium situation where the atmospheric pressure on the polymer sheet is equal and in the opposite direction to the pressure exerted by the foam and the partial vacuum in the wound cavity.
274 Dr Wilkins explained that the solid parts and pores of the foam had contact and non-contact with the wound bed respectively, and pressure at the points of the contact was above, and at points of non-contact was below, atmospheric pressure, and a partial vacuum. Thus, there were areas of suction where the pores were located and areas of compressive force where the fibres made contact with the wound bed. The porosity of the screen or foam permitted ambient air comprising the negative pressure beneath the seal to pass through the foam to and from the wound bed.
Conclusion – meaning of wound overgrowth
275 Thus, while S&N’s witnesses expressed the view that the term “overgrowth” was not a common or medically accepted term, all witnesses, including Professor Marshall and Dr Pohl, appeared to agree that, in the Patent, the term was likely to refer to an over-proliferation of granulation tissue to the point where it bulged above the level of the surrounding skin, that is, hypergranulation, which is a rare condition.
276 Professor Marshall’s evidence shifted on that issue. He conceded that he had redefined the term in the course of evidence to include islands of growth in the wound below that level. While KCI submitted that Professor Stacey agreed that it could mean tissue that was growing too fast, the ultimate effect of his evidence was that it was not usual to refer to granulation tissue as hypergranulation unless it grew above the level of the skin.
277 Ultimately, Professor Marshall’s initial evidence accorded with the consistent views of the other expert witnesses that hypergranulation occurred where granulation tissue grew above the level of the surrounding skin. There was no evidence to suggest that granulation tissue which grew above the level of surrounding skin and therefore amounted to hypergranulation was cellularly or biologically different from granulation tissue which did not grow in that way, so its hallmark was the extent of the growth in exceeding the “boundary” of the level of the skin.
Conclusion – meaning of “sufficiently rigid to prevent wound overgrowth”
278 The quality of sufficient rigidity in the screen means is defined by its capacity to prevent wound overgrowth which I accept, in the context of the Patent, is the growth of ordinary granulation tissue above the surface level of the skin surrounding the wound.
279 As noted above, in KCI’s ultimate submission, the screen rigidity integer referred to a screen means suitable for preventing overgrowth, but was not required to “stop” hypergranulation. Rather, “the screen modulates the growth of granulation tissue until the surgeon makes a clinical decision to intervene… it serves to limit the hills of granulation tissue” and “provides a barrier which controls the growth of the weeds on the way up to the top of the fence”. KCI submitted that the object of the screen was to ensure “even, controlled growth” of granulation tissue before it got to the level of surrounding skin; that is, the phrase “prevent overgrowth of granulation tissue” in all the relevant claims should properly be construed as a reference to the modulation of the growth of granulation tissue. Viewed in that light, the screen did not prevent hypergranulation but rather, its rigidity, if of the correct degree, modulated the unwanted upward growth, so that the granulation tissue developed in an even, controlled way. Once that were accepted, there was no need for complicated clinical trials with the sufficient degree of rigidity, and no contradiction between the device promoting granulation growth, yet the rigidity of the screen preventing its overgrowth. KCI relied on Professor Marshall’s ability to understand the integer and Professor Stacey’s acknowledgement that Dr Wilkins elegantly described the workings of the screen. KCI submitted that Professor Kimble’s continuing perplexity indicated a stubborn or untutored approach.
280 In my opinion, the construction of the screen rigidity integer ultimately advanced by KCI did not reflect the language of the claims. It required the integer to be construed as a screen means for modulating the growth of tissue in a wound and sufficiently rigid to modulate the growth of granulation tissue. The weight of the evidence established, however, that the only plausible meaning attributable to the phrases “wound overgrowth” or “overgrowth of tissue” was hypergranulation, a rare medical condition. Hypergranulation is nevertheless biologically identical to ordinary granulation and distinguishable in the relevant context only when and because the quantity of granulation tissue is such that it exceeds the surface of the wound. Granulation tissue itself is, as the Patent recognises, essential to the wound healing process, and a central teaching of the Patent is that its methods and apparatus promote the growth of granulation tissue to that end.
281 Viewed in that light, hypergranulation is simply an advanced but medically and aesthetically undesirable stage in a continuum of growth of granulation tissue, which is promoted by the Patent’s methods and apparatus and is terminated or prevented, not by any component or element thereof, but by their withdrawal or removal.
282 KCI submitted that the court should reject the evidence of Professors Kimble and Stacey that clinical judgment prevented overgrowth rather than the sufficiently rigid screen. Their testimony was, however, in my opinion, persuasive, and indeed, fortified by that of KCI witnesses. The evidence as a whole also established that the growth of granulation tissue was in fact promoted by use of the KCI apparatus, that the screen was, in practice, essential to the application of negative pressure, that the growth continued while the device was used, and that practitioners accordingly exercised their clinical judgment to cease using the device before granulation growth reached the hypergranulation stage.
283 While construction is ultimately a matter for the court, Professors Kimble, Stacey and Penington maintained consistently that they would not have understood what a screen means sufficiently rigid to prevent wound overgrowth meant and were still, for cogent and clearly expounded reasons, unable to attribute meaning to the phrase.
284 There is, in my view, a clear distinction between, on the one hand, the promotion of even granulation tissue or the modulation of growth of such tissue, and, on the other hand, preventing an excessive quantity of such tissue or its growth beyond a particular level of the wound. Further, it was unclear whether KCI submitted that such modulation would necessarily prevent granulation tissue from growing higher than the surface of the wound.
285 Even if it were accepted that the achievement of modulated growth of granulation tissue would “prevent” or forestall wound overgrowth, the latter would merely be a particular consequence of a wider and more complex process.
286 Despite allowing for the schematic character of the drawings in the Patent, which did not literally depict the contact which would be made with the wound while they were functioning, Figure 2 (the inflatable CPR mask or cuff which was used in a majority of the examples referred to in the Patent) could not be reconciled with Dr Pohl’s and Professor Marshall’s explanations of how the sufficient rigidity of the foam operated to prevent wound overgrowth.
287 In my opinion, the language of the claims, read in context, required the degree of rigidity of the screen means (whether foam or gauze) to prevent hypergranulation, but there was no evidence that the functional limitation was achieved, achievable, logically cogent or scientifically tenable in the context of the Patent.
288 The Patent teaches that a beneficial growth of granulation tissue will be achieved through using the device. While KCI submitted that the screen should be viewed as a tool which prevented overgrowth when used by the physician, the fact that progression caused by applying a device is halted by ceasing the application does not establish that the device (or any element thereof) has prevented the progression. So to maintain is to conflate the negation of a process caused by using a device with an active preventative function of the device.
289 KCI’s construction of the screen rigidity integer emerged at a relatively late stage, principally from the shifting testimony of Professor Marshall on the topic, and in the light of testimony that the growth of granulation tissue would progress while the device was in use. If the screen rigidity integer were (despite the language of the claims and, indeed, the specification) properly to be construed as a screen means the rigidity of which modulated the growth of granulation tissue, rather than preventing overgrowth, no persuasive explanation of any mechanism or scientific basis by which the screen means (foam) could or did achieve modulation was advanced.
290 KCI’s principal expert witness, Professor Marshall, who made many concessions and vague assertions, successively expressed a number of different and (potentially) inconsistent views. He at one point proposed a theory that the integer produced the result by the fibres of the foam pushing down while the pores sucked up, but, as stated above, he acknowledged that there was no scientific proof (by way of a clinical trial) to establish that the V.A.C.® device or the KCI foam prevented wound overgrowth, and conceded that he would not submit his conclusion to that effect to a peer reviewed journal. He also conceded that the foam itself did not modulate the growth of granulation tissue, but rather postulated that modulation was achieved by the combination of the foam and the negative pressure generated by the device. Professor Marshall (consonant with the evidence of the other expert witnesses) testified that he intervened to remove the device prior to hypergranulation occurring, which while it did not positively disprove, nevertheless undercut the conclusion that the foam, by its sufficient degree of rigidity, prevented overgrowth.
291 Dr Pohl, on the other hand, appeared to consider that the screen means itself both encouraged the growth of granulation tissue while preventing its overgrowth, which, as he acknowledged, was confusing. Dr Pohl conceded that the CPR mask device embodiment of the device could not push down on the surface of the wound (thus preventing wound overgrowth on this theory) unless it were filled with foam, which he agreed that the Patent did not require or describe.
292 I was not persuaded that the screen means operated as a barrier or that it, or its quality of rigidity, controlled or modulated the growth of granulation tissue or prevented the overgrowth of granulation tissue or hypergranulation. Nor did I accept that Professor Stacey ultimately endorsed or accepted the theory propounded by KCI.
293 Not only did KCI’s construction of the screen rigidity integer represent a major departure from, and reformulation of its literal meaning, but no construction accorded with any cogent explanation or tenable theory advanced in evidence. The meaning of the prevention of wound overgrowth by the sufficient rigidity of the screen means and how the screen means should be constructed to achieve that result remained unclear.
Construction of screen porosity integer
294 S&N initially submitted that the screen porosity integer was, like the screen rigidity integer, scientifically unsound.
295 Professor Stacey, in his first affidavit, deposed “The term [“sufficiently porous to allow gases to reach the wound”] has no meaning for me now nor would it have had in 1991 and it does not make sense scientifically”. Professor Penington deposed that it does “not appear to me to be sensible” to allow gases to reach the wound, because oxygen is a slow diffusing molecule and would take a long time to move from the atmosphere into a cell.
296 Professor Kimble was unaware that there is, or was prior to November 1991, “such as thing” as a dressing sufficiently porous to allow gases to reach a wound in negative pressure treatment. He emphasised that the goal of negative pressure was not for gases to reach the wound from the outside, but rather to allow suction out of the wound.
297 At trial, Professor Stacey was directed in cross-examination to Dr Wilkins’ evidence of the areas where the foam did and did not make contact with the wound bed, including areas of suction where the pores did not contact the wound bed, and areas of compressive force where the fibres adjacent to the pores made positive contact with the wound bed.
298 In the light of that evidence, Professor Stacey, as revealed by the following exchange, accepted that the screen porosity integer should be read as a requirement that the foam have such porosity as would enable ambient air to pass through the foam both to and from the wound bed:
Having now seen Dr Wilkins' explanation as to how the porosity of the foam assists the exertion of negative pressure and indeed compressive forces at the wound bed, it is a fair reading of that passage, isn't it, to suggest that the inventors are there describing the porosity of the screen simply by reference to its capacity to allow ambient air to pass through the pores of the foam?
I think it's a fair reading to interpret it in that way, although it is not obvious immediately, yes.
299 S&N ultimately conceded, and I accept, that the screen porosity integer bore the meaning contended by KCI.
Construction of integer re “migration of epithelial and subcutaneous tissue”
300 Claim 1 and its dependent claims (claims 2, 3, 6, 7, 8, 9, 10, 11 and 12) contain the integer of “applying a negative pressure to said wound over an area sufficient to promote migration of epithelial and subcutaneous tissue toward the wound”. The specification states that “[t]he use of negative pressure provides tension on this border tissue that causes accelerated tissue migration”.
301 It was broadly agreed that during the wound healing process, a bed of granulation tissue is formed in the wound, and epithelial cells multiply and migrate over that granulation tissue to close the wound, which is known as “epithelial creep”. As KCI acknowledged, epithelial cells in that context broadly refer to skin.
302 S&N, while acknowledging the role of epithelial creep, contended that the integer lacked a sound basis in physics and medicine, relying in that context on Professor Stacey’s assertion that (contrary to the language of the integer) cellular structures within subcutaneous tissue migrated. S&N disputed the theory in the specification that rather than subcutaneous tissue itself, tension on the border tissue causes accelerated tissue migration, on the basis of the evidence of Dr Wilkins and Professor Penington that wounds close by first filling from the base upwards with granulation tissue (rather than by closing from the border).
303 S&N submitted that the movement of tissue towards the centre of the wound when the V.A.C.® therapy is in operation, demonstrated in the DVDs shown at trial, was a different concept from that implicit in the integer. In S&N’s submission, the integer did not refer to the physical reduction in size of the wound that occurs through the application of negative pressure therapy.
304 KCI submitted that the invention applied pressure to the margins of the wound, resulting in a mechanical force, which pulled the subcutaneous tissue inward, thus reducing the defect required to be filled by granulation tissue. The epithelium therefore did not need to travel as far in order to close the wound.
Expert evidence
305 Dr Pohl, in his affidavit, interpreted the integer, in so far as it relates to epithelial tissue, as meaning that epithelial cells creep across to cover the wound. He was aware in 1991 that tension may stimulate the surrounding tissues to stretch and stimulate cell growth. Dr Pohl also stated that it was clear from his experience that NPWT draws the edges of the wound together via a mechanical force on the tissue surrounding the wound.
306 During the trial, after a DVD made by Dr Pohl was shown in court, he testified that the DVD demonstrated that the vacuum draws in the surrounding tissue. He stated that the vacuum “pulls it all together”.
307 Mr Ellis deposed to his attendance at a meeting of the Australian Wound Management Association in Sydney in 1996, where KCI presented on its V.A.C.® system. He deposed that the system seemed to be drawing the edges of the wound together (which, he asserted, has subsequently proved to be the case).
308 Professor Marshall, in his first affidavit, deposed that in 1991, he would have been sceptical about whether the use of negative pressure would have an impact on tissue migration and would have speculated that the tension on the wound border tissue would (assuming it worked) accelerate tissue migration by facilitating increased blood flow to the site of a wound. He deposed that he had since, however, become aware of recent research which showed that pressure applied to a tissue can make tissue migrate.
309 Professor Marshall stated that a DVD made by KCI shown at trial demonstrated how the wound is pulled in towards the centre, so that “it looks smaller than it did when you first started”.
310 Professor Stacey, in his first affidavit, objected to this integer on the basis that subcutaneous tissue could not “migrate”. In cross-examination, Professor Stacey asserted that only the cellular structures within subcutaneous tissue migrate. He also maintained that epithelial cells do not migrate from the edges of the wound until they have a healthy base of granulation tissue to move across.
311 Professor Stacey deposed that he could not understand the term “area sufficient”, as it “provides no meaningful direction”. He considered that the term would only be logical if the negative pressure were applied over the whole wound.
312 In cross-examination, Professor Stacey acknowledged that the Patent claimed that the tension applied to the border of the wound exerts a “mechanical force” on the tissues that make up the periphery of the wound, drawing them in towards the centre of the wound. He accepted that on a fair reading, the Patent teaches that the subcutaneous tissue is pulled in so that the defect required to be filled by granulation tissue becomes smaller (although he expressed doubt as to whether this, in fact, happens). Consequently, on the Patent’s description, the epithelium would not have to travel as far in order ultimately to close the wound. Professor Stacey also accepted in cross-examination that one could read the word “migrate” as referring to “move” or “contract”.
313 Professor Penington, in his second affidavit, deposed that the language of the integer was “unusual” because tissue does not migrate. Rather, cells migrate, so the reference to epithelial tissue in the Patent must be read as a reference to epithelial cells (which make up epithelial tissue). He interpreted the Patent as referring to the migration of epithelial cells to cover and close a wound.
314 Professor Penington deposed that the statements in the Patent about how the wound might close from the border with the application of negative pressure were flawed. He knew before November 1991 that full thickness open wounds close by filling from the base upwards with granulation tissue.
Conclusion
315 Although Professors Penington and Stacey doubted the accuracy of the wording of the integer, their evidence did not in my view outweigh Dr Pohl’s testimony that NPWT draws the edges of the wound together via a mechanical force on the tissue surrounding the wound, supported by Professor Marshall’s testimony that pressure applied to a tissue can make tissue migrate, and the evidence of Dr Pohl and Professor Marshall, based on the DVDs shown at trial, that the vacuum draws the wound in.
316 Therefore, in my opinion, the text of the integer broadly accorded with the evidence on how it worked.
317 S&N accepted that the fluid impermeable or semi-permeable sealing means which permitted negative pressure to be delivered was essential and was present in its products.
Allegedly inessential integers
318 S&N, in reliance in Gummow J’s observations in Nicaro Holdings Pty Ltd v Martin Engineering Co (1990) 91 ALR 513 (“Nicaro Holdings”), alleged that a number of integers of the claims in suit which were not expressly stated in prior art (such as “area sufficient…”, “time sufficient…”, minimum length of application, and the ratios of time of application to non-application) were mere mechanical variations of clinical judgment or clinical desiderata rather than essential integers of the claims in suit. The essentiality of the integers is relevant to both infringement and invalidity, as infringement depends on taking all essential integers of a combination patent, but the absence of inessential integers from the prior art would not preclude anticipation of a claim if all its essential integers were disclosed, whether expressly or by inference.
319 S&N submitted that the integers relating to the placement of the screen means in relation to the wound in claims 49, 50, 52 (“overlie the wound”) and 121 (“in the wound”) were inessential because the specification so indicated, and that feature was expressed in a number of alternative ways in various other claims not in suit, as follows:
(a) claims 36, 62, 74 and 89 required the screen means to be positioned “at the wound within the sealing means”;
(b) claim 118 required the screen to be placed “over the graft”; and
(c) claims 51, 108, 111 and 116 required the screen to be “configured to overlie only a region of said wound within the margin of said wound”.
320 Further, S&N submitted that claims 49, 50 and 52 required the screen to be positioned to overlie the wound, while in contrast, claim 1 required it to be placed “over an area sufficient to promote migration…”.
321 More accurately, however, claims 49, 50 and 52 require the screen to be configured (which I take to mean “shaped”) to overlie the wound and the screen means to be “for positioning beneath the said seal”, while claim 1 more accurately requires “placing” of the screen means “in a wound”, as does claim 121.
322 S&N submitted that the following “duration” integers were inessential:
(a) “said negative pressure being maintained for a time sufficient to facilitate closure of the wound” (claim 1);
(b) “maintaining said reduced pressure until the wound has progressed toward a selected stage of healing” (claim 121);
(c) “said negative pressure being maintained for a time sufficient to permit the formation of granulation tissue in the wound” (claim 2);
(d) “said time is at least 12 hours” (claim 6); and
(e) “said time is at least 3 days” (claim 7).
323 S&N argued, in particular, that the integers specifying minimum periods for applying negative pressure were inessential, because in practice, clinicians decided to leave the device on for as long as they wished.
324 KCI submitted that in the absence of a clear indication, the relevant claims were not inessential, and were deliberately inserted by the patentee. It contended that the claims of “at least 12 hours” and “at least 3 days”, while “open-ended at the top end”, were appended to claim 1, marked the boundaries of the monopoly by reference to those time limits, and were plainly essential.
325 S&N submitted that the following integers concerned with the duration or mode of application of negative pressure were inessential:
(a) “applying a negative pressure to said wound over an area sufficient to promote migration of epithelial and subcutaneous tissue toward the wound” (claim 1);
(b) “pressure is applied substantially continuously” (claim 8);
(c) “pressure is cyclically applied in alternate periods of application and non-application” (claim 9);
(d) “method according to claim 9, in which the ratio of said period of application to said period of non-application is at least 10:1” (claim 10);
(e) “method according to claim 9, in which the ratio of said period of application to said period of non-application is at least 1:1” (claim 11);
(f) “method according to claim 9, in which the ratio of said period of application to said period of non-application is at least 1:10” (claim 12); and
(g) “pressure is conducted in alternating periods of application and non-application” (claim 121).
326 S&N submitted in particular that the alternative integers directed to cyclical application of negative pressure within a range were inessential as the ratios of cyclic application, limited by the words “at least”, also suggested that the ratio could go up to infinity. KCI contended that the claims of continuous and cyclic application delimited claim 1 by reference to those two modes of operation. Moreover, the ratio claims, while broad, were clearly inserted for a reason.
327 S&N submitted that the following alternative integers relating to the placement of the tube were inessential.
(a) “a single tubular member having a first end inserted beneath at least a portion of the foam section” (claim 50);
(b) “having an inlet end inserted into said open-cell polymer foam section” (claim 49); and
(c) “said first end of the tubular member is embedded within the foam section” (claims 52).
328 S&N relied particularly on Dr Pohl’s testimony that the tube could be placed anywhere, including onto or underneath the screen or foam. Dr Pohl’s observation was, however, expressly directed at the device in one of the prior art documents known as “Bagautdinov I” (discussed below in relation to novelty) in which, as he stated, the tube was for drainage, and once the vacuum was applied, it drew to it. I was not persuaded that the integers related to duration, cyclical or continuous application, ratios of non-application to application or placement of the tube were inessential.
329 In Fisher & Paykel Healthcare Pty Ltd v Avion Engineering Pty Ltd (1991) 103 ALR 239 (“Fisher & Paykel”), the Full Court (Black CJ, Lockhart and Gummow JJ) stated (at 256):
It has become the practice in a claim for a combination of common integers, to set out in considerable detail the elements or integers. Failure to do so may result in want of compliance with s 40. Also, those drafting such claims should do so in the light of the prior art; this may make them rightly fearful of claiming too much, as Lord Upjohn pointed out in Rodi and Wienenberger AG v Henry Showell Ltd [1969] RPC 367 at 392. Accordingly, as his Lordship also emphasised, there is a need for caution in accepting in an infringement suit the suggestion by the patentee that what appears to be a limitation upon the claimed subject matter is merely the product of a slip of the pen and thus not to be held too readily against the patentee.
330 There is a disposition to construe integers as essential. As observed in Fisher & Paykel, drafters of claims based on a combination of common integers typically set out in considerable detail the elements of integers, cognisant of the requirements of s 40 of the Act and the potential impact of prior art on excessive claims. Thus, as Lord Upjohn indicated in Rodi and Weinenberger AG v Henry Showell Ltd [1969] RPC 367 at 392, in the context of an infringement proceeding, a patentee’s claim that a limitation was merely “a slip of a pen” should be viewed with caution.
331 In the present case, KCI characterised all the relevant integers as essential. Although the specification indicated that the duration of application of negative pressure treatment could vary depending on the nature and size of the wound, the clear language of the claims should not be narrowed or expanded by reference to the specification. The integers related to duration, cyclical or continuous application, the ratio of application to non-application and the placement of the foam were not optional extras or additions. In contrast to the aseptic package in Wake Forest, they appeared to interact with all the other elements of the relevant claims to produce a new result or product.
332 In Melbourne v Terry Fluid Controls Pty Ltd (1994) 28 IPR 302, the Full Court, in reliance on Welch Perrin, held that the primary judge erred in by implying a period of duration for electrical isolation of a piston rod to match the general expectation of those skilled in the art, although no such period of time was included in any claims. Their Honours observed (at 309) that it was not permissible to vary or qualify the plain and unambiguous meaning of a claim by reference to the body of the specification, nor to imply a limitation to match the expectations of those skilled in the art. Conversely, the limitations constituted by the above integers in the present case should be given effect.
333 As S&N acknowledged, integers are rarely inessential. Rather, they are deliberately selected and inserted for the significant purpose of demarcating the extent of the monopoly claimed. In my opinion, the relevant integers are essential. They must be both taken in order to infringe the claims in which they appear and disclosed by the prior art for the purposes of anticipation.
Relevant legislation and legal principles
334 While the Act does not define infringement, its elements may be deduced from the general law in the light of the statutory monopoly to exploit the invention and to authorise others to do so conferred by s 13 of the Act, which provides:
(1) Subject to this Act, a patent gives the patentee the exclusive rights, during the term of the patent, to exploit the invention and to authorise another person to exploit the invention.
(2) The exclusive rights are personal property and are capable of assignment and of devolution by law.
(3) A patent has effect throughout the patent area.
335 The infringement of a patent pursuant to s 13 of the Act thus requires conduct amounting to exploitation of the invention as claimed in a relevant claim contrary to the patentee’s exclusive rights, or conduct authorising someone else to do so.
336 The Act also provides for a more indirect form of liability pursuant to s 117 of the Act which relevantly provides:
(1) If the use of a product by a person would infringe a patent, the supply of that product by one person to another is an infringement of the patent by the supplier unless the supplier is the patentee or licensee of the patent.
(2) A reference in subsection (1) to the use of a product by a person is a reference to:
(a) if the product is capable of only one reasonable use, having regard to its nature or design—that use; or
(b) if the product is not a staple commercial product—any use of the product, if the supplier had reason to believe that the person would put it to that use; or
(c) in any case—the use of the product in accordance with any instructions for the use of the product, or any inducement to use the product, given to the person by the supplier or contained in an advertisement published by or with the authority of the supplier.
337 Whether s 13 rather than s 117 applies to infringing conduct does not depend solely on whether the infringer itself exploits the invention in breach of the patentee’s exclusive rights, as authorising someone else to do so amounts to a “direct” infringement under s 13.
338 It was not disputed that “authorising” in that context bore the construction applied to s 36 of the Copyright Act 1968 (Cth) and by the High Court in University of New South Wales v Moorhouse (1975) 133 CLR 1 (“Moorhouse”), where Gibbs CJ observed at 13:
[A] person who has under his control the means by which an infringement of copyright may be committed -- such as a photocopying machine -- and who makes it available to other persons, knowing, or having reason to suspect, that it is likely to be used for the purpose of committing an infringement, and omitting to take reasonable steps to limit its use to legitimate purposes, would authorize any infringement that resulted from its use.
339 In the same case, Jacobs J (with whom McTiernan ACJ agreed) stated at 21:
It is a wide meaning which in cases of permission or invitation is apt to apply both where an express permission or invitation is extended to do the act comprised in the copyright and where such a permission or invitation may be implied. Where a general permission or invitation may be implied it is clearly unnecessary that the authorizing party have knowledge that a particular act comprised in the copyright will be done.
340 As extracted above, s 117(1) of the Act provides that a person may be liable for infringement by supplying a product to another if “the use of the product” as defined in s 117(2) by a person would infringe the patent.
341 In Northern Territory of Australia v Collins & Anor (2008) 235 CLR 619 (“Northern Territory”), the High Court considered the meaning of “staple commercial product” in s 117(2)(b), which is not defined by the Act. In Northern Territory, the proprietors of a patent for a method of producing essential oils from species of cypress pine trees alleged that, by licensing another party to take cypress pines from a plantation, the Northern Territory had infringed their patent under s 117 of the Act.
342 The High Court considered that unmilled cypress timber constituted a staple commercial product. Gummow ACJ and Kirby J adopted French J’s statement below that millable timber was suitable for use in a variety of applications for which timber generally is used.
343 Crennan J (with whom Heydon J agreed) also held that the timber was a staple commercial product, observing at 653 that:
s 117(2)(b) operates to limit liability for contributory infringement. Policy arguments in favour of imposing liability for contributory infringement are much weaker with a product that has significant non-infringing uses. The legislative intention… is to except from liability, the supply of products with significant non-infringing uses…
344 Hayne J, who also held that the timber was a staple commercial product, considered that the term should be widely construed and required that a product could be used and traded for use in a variety of ways. His Honour considered that a staple commercial product required an established wholesale or retail market.
345 In the present case, KCI alleged that S&N infringed the apparatus claims both directly and indirectly, by selling and supplying the foam dressing kits and authorising and encouraging its customers to use them. In contrast, KCI alleged that S&N infringed the method claims only indirectly, pursuant to s 117 of the Act or as a joint tortfeasor, by arming and inducing its customers to infringe those claims.
346 In particular, KCI alleged that S&N had infringed the apparatus claims (claims 49, 50 and 52) by exploiting and authorising its kits as follows:
(a) pursuant to s 13 of the Act, by, inter alia, selling and supplying its foam dressing kits;
(b) pursuant to s 117 of the Act, by the supply of its foam dressing kits;
(c) pursuant to s 13 of the Act, by authorising third persons to use its foam dressing kits; and
(d) pursuant to s 13 of the Act, by procuring or inducing third persons to use its foam dressing kits.
347 KCI alleged that S&N had infringed the method claims (claims 1, 2, 3, 6, 7, 8, 9, 10, 11, 12 and 121) by use of pumps with kits as follows:
(a) pursuant to s 117 of the Act, by the supply of its vacuum pumps together with its foam dressing kits;
(b) pursuant to s 13 of the Act, by authorising third persons to use its vacuum pumps together with its foam dressing kits; and
(c) pursuant to s 13 of the Act, by procuring or inducing third persons to use its vacuum pumps together with its foam dressing kits.
348 In Populin v HB Nominees Pty Ltd (1982) 59 FLR 37 (“Populin”), the Full Federal Court (Bowen CJ, Deane & Ellicott JJ) considered the construction of claims in the context of alleged infringement of a combination patent. The Full Court affirmed the established principle that the defendant must take all the essential integers in order to infringe a combination patent. Conversely, infringement could not be avoided merely by omitting inessential integers of, or making immaterial variations to, a combination patent (at 41). In Populin, it was held that the respondents’ sugar cane planting machine did not infringe the appellants’ patent rights to an invention relating to a machine and method for planting sugar cane.
349 The Full Court found (at 47) that the separate nature of a small bin and the large container in the appellants’ machine was an essential feature of the invention described in the claim. As the separate nature of the small bin and supply container was essential, and the respondents’ machine had combined the features in a single large container, there was no infringement (at 47). The Full Court stated (at 41):
Many patents are combination patents. That is to say, they consist of the combination of a number of known integers which work in relation to one another so as to produce a new or improved result.
350 Their Honours observed that in the case before them, none of the elements claimed in the patent was new in itself. Rather, what was new was “the working relationship of the various elements to produce a new and improved machine for planting cane” (at 41). They noted a practice of setting out the elements and integers of the invention at great length in the claim and commonly adding to or varying the first claim in the subsequent claim, thereby progressively adding the elements to the combination, which made it more difficult to attack the patent on the basis of want of subject matter or novelty, but progressively narrowed the area of the monopoly claimed.
351 The Full Court recognised that claims determine the extent of the monopoly, in that they operate as a disclaimer of what was not specifically claimed. Because infringement of a combination patent required the defendant to take “each and every one of the essential integers of the patentee’s claim” (at 41), if the patentee of a combination patent did not claim only the essential integers in combination, or failed to distinguish what was essential from what was inessential, an alleged infringer could escape liability by omitting only one essential integer in a particular combination.
352 Nevertheless, the Full Court stated that infringement could not be avoided merely by adopting immaterial variations, or omitting an inessential part and adopting another part or step as its equivalent (at 41). The substance of the invention could not be taken with impunity unless the wording of the claims made clear that the relevant area was deliberately left outside the claim (at 42).
353 It follows that in order directly to infringe any of the claims in suit, which are all combination claims, S&N must have itself exploited a method or product which possessed all the essential integers thereof, or alternatively must have authorised a third party to do so.
354 S&N would be liable for “indirect” infringement pursuant to s 117 of the Act for supplying its products to other persons if the use of the products by a person would infringe the Patent in the sense that:
(a) the products were capable of only one reasonable use, having regard to their nature or design and were used in that way (s 117(2)(a));
(b) if the products were not a staple commercial product (that is, broadly, if there were not a variety of innocent uses and ways of trade), any use, if S&N had reason to believe that the recipient would put it to that use (s 117(2)(b)); or
(c) in any case, the use of the products in accordance with any instructions for their use or any inducement to use the products, given to the recipient by S&N, or contained in an advertisement published by or with S&N’s authority (s 117(2)(c)).
355 The Schedule 1 Dictionary to the Act defines “supply” to mean supply by way of sale, exchange, lease, hire or hire-purchase; and offer to supply (including by those means).
356 KCI contended that, having regard to the nature of S&N’s products and the instructions for use supplied by S&N to its customers with those products, S&N had, pursuant to s 117, infringed the relevant claims of the Patent.
357 KCI also submitted that S&N was, on the basis of the same conduct, liable as a joint tortfeasor at common law, in reliance on Ramset Fasteners (Aust) Pty Ltd v Advanced Building Systems Pty Ltd (1999) 44 IPR 481 at 500, where the Full Court made clear that liability required more than mere facilitation of infringement by another person. The Full Court stated:
These authorities show that liability for infringement may be established, in some circumstances, against a defendant who has not supplied a whole combination (in the case of a combination patent) or performed the relevant operation (in the case of a method patent). The necessary circumstances have been variously described: the defendant may “have made himself a party to the act of infringement”; or participated in it; or procured it; or persuaded another to infringe; or joined in a common design to do acts which in truth infringe. All these go beyond mere facilitation. They involve the taking of some step designed to produce the infringement, although further action by another or others is also required. Where a vendor sets out to make a profit by the supply of that which is patented, but omitting some link the customer can easily furnish, particularly if the customer is actually told how to furnish it and how to use the product in accordance with the patent, the court may find the vendor has “made himself a party to the [ultimate] act of infringement”. He has indeed procured it. So to hold is not in any way to trespass against the established line of authority which, as Dixon J made clear in Walker v Alemite, is based upon the need to confine a monopoly to the precise area in which it operates. That protects the mere vendor of an old product, though selling with knowledge of the purchaser's intention to infringe a combination patent; but it affords no excuse to the person who sets out to induce customers to do what falls fairly within the area of the monopoly.
Whether KCI established infringement
358 KCI bears the burden of establishing infringement on the balance of probabilities. Section 140 of the Evidence Act 1995 (Cth) (“Evidence Act”) states:
(1) In a civil proceeding, the court must find the case of a party proved if it is satisfied that the case has been proved on the balance of probabilities.
(2) Without limiting the matters that the court may take into account in deciding whether it is so satisfied, it is to take into account:
(a) the nature of the cause of action or defence; and
(b) the nature of the subject-matter of the proceeding; and
(c) the gravity of the matters alleged.
359 As S&N contended, infringement would not be established according to the applicable standards unless KCI’s case were more probable than that of S&N. It is also necessary that there be an actual persuasion that the relevant conduct had occurred.
360 In CEPU v ACCC (2007) 162 FCR 466 at 480, the Full Federal Court (Weinberg, Bennett and Rares JJ), discussing s 140(2), stated:
Even though he spoke of the common law position, Dixon J’s classic discussion in Briginshaw v Briginshaw (1938) 60 CLR 336 at 361-363 of how the civil standard of proof operates appositely expresses the considerations which s 140(2) of the Evidence Act now requires a court to take into account. Dixon J emphasised that when the law required proof of any fact, the tribunal must feel an actual persuasion of its occurrence or existence before it can be found. He pointed out that a mere mechanical comparison of probabilities independent of any belief in its reality, cannot justify the finding of a fact.
361 S&N contended that, under the correct approach to the standard of proof in a civil proceeding under s 140 “the strength of the evidence necessary to establish a fact in issue on the balance of probabilities will vary according to the nature of what is sought to be proved”, as discussed in Neat Holdings Pty Ltd v Karajan Holdings Pty Ltd (1992) 110 ALR 449. S&N submitted that in the present case, the standard was not satisfied.
362 S&N’s overarching defence was that the screen rigidity integer, which was common and essential to all the claims in suit, was not, or was not proved to be, present in its foam kits. In S&N’s submission, at best, the evidence in relation to that integer gave rise to no more than “conflicting inferences of equal degrees of probability so that the choice between them is a mere matter of conjecture”.
363 Further, S&N submitted that:
Professor Marshall did not observe the Respondent's product in use. He relied solely on his inspection of the Respondent's RENASYS-F foam dressing kit, his review of the Respondent's product brochures and instructions, and his experience of using the VAC Therapy System and the Second Applicant's foam dressings. The Respondent respectfully submits that this is a not a proper way to prove the presence of a limitation by result.
… Professor Marshall said that the dressing kits are "the same" or "substantially identical". [H]e concluded that the Respondent's foam must be "sufficiently porous to allow gases to reach the wound" because its porosity is “indistinguishable” from the Second Applicant's foam. In coming to that conclusion, Professor Marshall merely assumed that the Second Applicant's foam possesses this feature. See also paragraph 101…:
I know from my experience with the application of V.A.C.® therapy that the KCI foam dressing prevents overgrowth of granulation tissue.
364 The first tranche of method claims was claim 1 and its dependent claims. Claim 1 does not refer to a sealing means but it (and necessarily, each of its dependent claims) requires the placing of a screen means (dressing) in a wound for preventing overgrowth of tissue in a wound, which is sufficiently porous to allow gases to reach the wound and sufficiently rigid to prevent wound overgrowth.
365 It was not disputed that the screen rigidity integer was essential and must be taken by S&N in order to establish infringement. More fundamentally, the integer was a limitation by result integer, the validity of which required proof that the screen means was so constructed as to achieve the claimed result. S&N submitted that not only had KCI failed to prove that it had taken the screen rigidity integer, but the evidence positively disproved the integer because the promised result “does not happen”.
366 The material for the screen means (dressing) in claim 1 and its dependent claims is not specified. Thus, the method claims in claim 1 and its dependent claims and in claim 121 are not limited to foam, although the preferred embodiment requires a section of open-cell foam configured to be placed over the wound. As noted at [19], S&N initially entered the market with kits containing gauze as a screen means or dressing rather than foam, but KCI contended only that S&N’s more recent foam kits included a screen means sufficiently rigid to prevent wound overgrowth and sufficiently porous to allow gases to reach the wound.
367 S&N disputed that its foam kits contained a screen means sufficiently rigid to prevent wound overgrowth, even if, contrary to its anterior principal submission, that integer were valid and meaningful.
368 KCI relied, in that context, principally if not exclusively on the evidence of Professor Marshall, who had used the KCI product.
369 In concluding that S&N’s kits contained a screen means (foam) sufficiently rigid to prevent wound overgrowth, Professor Marshall examined S&N’s RENASYS-F kit and compared it with the KCI product, with which he was familiar from previous experience. Professor Marshall also examined photographs of the foam in the RENASYS-F kit taken by the solicitors for KCI, and observed that they revealed a kit substantially identical to the kit he inspected, except that there was only a single tube.
370 Professor Marshall deposed to his examination of the S&N kit as follows:
Inside the packaging there are two transparent, flexible tubes, a piece of foam and a number of adhesive drapes. The foam is rectangular, with a channel extending down the centre on one surface. Based on my experience with KCI's V.A.C.® therapy, I would say that the foam has a porosity and firmness that is indistinguishable from the V.A.C.® therapy foam. I am informed by Freehills and believe that it is not disputed that the foam is made from a polymer.
One end of the shorter tube is perforated with many holes. In that respect the tube is similar in design to standard suction drain tubes that surgeons use to drain closed cavities. The perforations along one end of the tube are designed to draw in fluid along multiple sections and to minimise the risk of the tube clotting, or becoming blocked as a consequence. The tube is apparently intended to lie in the channel in the foam. Depending on the size of the foam that is needed to fit the wound, the perforated end of the tube would be trimmed so that the perforations are within the substance of the foam and don't go beyond it. That would ensure that the vacuum is transmitted through the foam. There is a moveable clip on the tube to seal the tube to maintain the vacuum and contain fluids while canisters are replaced or when dressings are changed. The second, longer tube appears to be an extension tube to connect the shorter tube to the vacuum pump.
The drapes are self-adhesive and would be applied over the foam in the wound and sealed to the skin. Self-adhesive plastic drapes are common in general surgery. There is a small self-adhesive drape which appears to be intended to seal around the area where the tube penetrates the main drape that is over the foam.
My initial impression of the RENASYS-F Kit at Exhibit DRM-4 is that it is for all intents and purposes the same as the wound dressing kits that I have used in V.A.C.® therapy.
I am informed by Freehills and believe that they inspected and took the photographs of the RENASYS-F foam dressing kit at pages 119 to 131 of Exhibit DRM-4. The photographs show a foam dressing kit that is substantially identical to the RENASYSF Kit that I have inspected, except that there is only a single tube. The tube is perforated at one end and appears to be longer in length than the perforated tube in the RENASYS-F Kit.
(emphasis added)
371 Professor Marshall reviewed claim 1 of the Patent and the RENASYS-F instructions and relevantly opined:
That direction is consistent with statements in the Patent that the screen should substantially fill the wound… `Wound overgrowth' in Claim 1 is the proliferative granulation tissue that I describe at paragraph 76 above. I know from my experience with the application of V.A.C.® therapy that the KCI foam dressing prevents overgrowth of granulation tissue. As I mention at paragraph 87 above, the rigidity of the foam dressing in the RENASYS-F Kit is indistinguishable to me from the rigidity of the KCI foam dressings that I have used. In my opinion, the foam section in the RENASYS-F Kit is `sufficiently rigid' such that when cut to fit the size and shape of the wound in accordance with the RENASYS-F Instructions, it will serve to prevent wound overgrowth.
(emphasis added)
372 As S&N submitted, the Patent is a combination patent and the functional integer of a screen means sufficiently rigid to prevent wound overgrowth was an essential integer common to all the claims, both method and apparatus, in suit. S&N submitted primarily that the relevant integer was “nonsensical” as the evidence established that the rigidity of the dressing (screen means) or the dressing itself neither could nor did prevent the overgrowth of granulation tissue, whether when used in the KCI kits or (perforce) in S&N’s kits. As stated above, I accept that submission.
373 For completeness, however, I now consider S&N’s subsidiary submission that (even if it were accepted that the screen rigidity integer were valid and present in KCI’s products) KCI had not, on the basis of Professor Marshall’s evidence, established to the requisite level of proof that S&N’s products possessed that integer.
Whether S&N’s product possessed screen rigidity integer
374 S&N contended, in that context, that on analysis, Professor Marshall’s evidence was perfunctory and based on a series of flawed or unsustainable and undemonstrated assumptions.
375 First, although Professor Marshall’s conclusion depended on the assumption that the screen means prevented wound overgrowth because he had not seen wound overgrowth when the V.A.C.® product was used, it did not logically follow from the absence of wound overgrowth that the rigidity of the screen means prevented its occurrence.
376 Secondly, Professor Marshall’s assumption that the S&N kits also possessed that functional integer depended on his visual inspection of the S&N product (which he had not used), from which it appeared indistinguishable from the KCI foam or screen means. Professor Marshall further assumed from the visual similarity that the S&N foam would function in the same way as the KCI V.A.C.® product. Professor Marshall’s inspection did not, however, even amount to a side by side comparison of the two products. He simply inspected the S&N RENASYS-F product in isolation, compared it with his “recollection” of the appearance of the V.A.C.® product and formed an impression accordingly.
377 In that context, S&N emphasised that the plain and unambiguous meaning of a claim may not be varied or qualified by reference to the body of the specification. Further, while a level of proof tantamount to that which would satisfy an authority such as the Federal Drugs Administration in the United States of the efficacy and safety of a drug was not required in the context of alleged infringement of a claim, the proof must have, at least, a scientific character and rise above mere visual comparison and multiple assumptions in order to satisfy the civil standards of balance of probabilities under s 140 of the Evidence Act. Section 140(2) required the court to take into account the nature of the cause of action or defence, the nature of the subject matter of the proceeding and the gravity of the matters alleged when deciding whether a case has been proved on the balance of probabilities.
378 S&N submitted that Professor Marshall’s evidence failed to provide the minimum element of scientific rigour necessary in a patent infringement proceeding whereby KCI asserted a monopoly on methods and devices for treating tissue damage or wounds, in a specialised medical field.
379 KCI conceded that Professor Marshall merely inferred the performance capacity of the S&N foam and accepted that there was no scientific proof in the sense of clinical trials, but his confidence was based on sound clinical experience. KCI submitted that it was not established that Professor Marshall failed to carry out a side by side comparison of the KCI and S&N foams, and his evidence as a whole was sufficient to establish the existence of the screen rigidity integer. As the accuracy and veracity of his account of inspecting both pieces of foam (even if not side by side) and the features he had visually observed was not challenged in cross-examination, the absence of contemporaneous clinical notes was irrelevant to the reliability of his uncontradicted practical clinical assessment.
380 The validity of Professor Marshall’s approach to establishing that the rigidity of the screen achieved the claimed result of preventing wound overgrowth was challenged by Professors Stacey and Penington.
381 Professor Stacey did not consider that the mere non-occurrence of a rare condition could establish that it was prevented by use of a certain item or method. He deposed:
Associate Professor Marshall is essentially saying that, since the Smith & Nephew and KCI foams are similar, then the Smith & Nephew foam will also prevent overgrowth because in his experience, the KCI foam prevents overgrowth. In my view there is a problem with this reasoning. It is not appropriate as a matter of proof to say that just because you do not see a condition, you prevented it by doing a certain thing or using a certain method, particularly in circumstances where you are referring to an uncommon condition.
382 Professor Penington also, despite equivalent experience of using the KCI V.A.C.® kits, disagreed with Professor Marshall’s conclusion. Professor Penington deposed:
Marshall states that he knows from his experience that the KCI foam dressing prevents overgrowth of granulation tissue. As I state above, I have also used the KCI VAC device and have not seen any evidence that the use of the system, or the foam wound dressing, prevents overgrowth (as that term is used in the patent), whether that term means hypergranulation or something else. If the term "overgrowth" as used in the Patent does refer to hypergranulation, it would be very difficult to establish in clinical practice that use of negative pressure therapy prevents hypergranulation as, in my experience, this treatment is generally used on open wounds only until they have progressed to the desired stage of healing. Rarely, in my experience, as I state above, is the desired stage of healing closure of the wound. It is more likely that negative pressure therapy will be used until the wound can be closed with a skin graft or skin flap or until the wound appears to be healing well. Accordingly, in my experience, as I state above, the treatment is usually stopped before a wound is progressed to the stage of healing where hypergranulation can occur, so the absence of hypergranulation does not establish that the treatment is preventing hypergranulation.
383 In cross-examination, Professor Marshall conceded that not every foam would serve the relevant purpose and to assess the suitability of a piece of foam he would usually feel it to ensure that in compressing it:
… there was some significant resistance to that compression. And finally, the test would be in the operating room, having put the foam in, applied the suction and evacuated a certain amount of the air to see that the foam behaved in the way that one would expect. In other words, if I had been asked, given each of those foam [pieces] in the operating room, I would have cut them and put them in the wound to test them to see whether they would do what I would [have] expected.
384 Professor Marshall, in the present case, had not cut the S&N foam, placed it in a wound or tested it by reference to whether it produced the expected result. He agreed that his conclusion that the rigidity of the S&N foam prevented wound overgrowth was not something he would have committed to an article or submitted to a peer review journal. He conceded that he relied on clinical experience only and had not controlled for variables, including how snugly the dressing was fitted, and the possibility that negative pressure contributed to lack of overgrowth, as distinct from the physical pressure.
385 In cross-examination, Professor Marshall was shown some white KCI foam which he had not seen before, and when asked whether he would regard it as having sufficient rigidity and porosity, said that he would be suspicious, as it did not seem to have as much aeration as the foams to which he was accustomed, and it was wet, which “gives it a different feel”.
386 Professor Marshall also agreed that there was no scientific proof, based on his described experience, “that the V.A.C.® therapy prevents overgrowth because of the rigidity of the foam alone”. At another point, Professor Marshall said that the prevention of hypergranulation was helped by the screen pushing down. He conceded that he had not conducted a clinical trial, and would need a large trial size to prove prevention of a relatively rare condition rather than its occurrence. He conceded that he did not believe that the pressure of the foam per se controlled hypergranulation, but rather, the combination of that pressure and the negative pressure.
387 Given the nature of the present proceeding, the gravity of the matters alleged (which delimit a monopoly on methods and apparatus for the treatment of serious tissue damage and wounds), and the nature of the integer in question, which was a limitation by result, a reasonable level of scientific or clinical rigour was, in my view, required to establish on the balance of probabilities the presence of the relevant functional integer in S&N’s products. Extensive formal clinical trials were not necessary, but visual inspection of the S&N foam, without any recorded physical testing or evaluation as the basis of a comparison with the KCI product, was inadequate. Moreover, on the better view of Professor Marshall’s evidence, he compared the S&N foam with merely recollected KCI foam. Professor Marshall himself acknowledged that even in a merely clinical context, he would cut the foam, place it in the wound, and use the foam in the operating room and see if it did what he expected.
388 Professor Marshall’s suspicion of the KCI white foam also exposed the frailty of the mode of proof of infringement adopted in the present case.
389 Further, Professor Marshall’s conclusion, which was expressed in terms of impression, depended on the cascading assumptions that the visual resemblance he detected between the S&N and KCI foams assured an identical structural rigidity, and that because, in his clinical experience, the KCI product prevented overgrowth, it possessed a screen means with sufficient rigidity to achieve that function (which, given the visual similarity of the foam in the S&N kits, they too possessed).
390 I have discussed the meaning of the screen rigidity integer and its functional limitation in detail above. As observed, Professor Marshall’s evidence on that issue was unpersuasive due, inter alia, to its inconsistency, and his acknowledged failure, in observing the coincidence of an absence of hypergranulation (a rare condition in any event) and the use of the KCI product, to control for any variables, including the role played by negative pressure per se, the “snugness” of the dressing or the removal of the dressing prior to the stage of hypergranulation, which, rather than the rigidity of the screen, may have prevented wound overgrowth. Professor Marshall invariably removed the screen himself prior to that stage, but had seen cases of wound overgrowth in less well managed wounds referred to him after treatment with the KCI V.A.C.®.
391 In my opinion, it was not established that the S&N products possessed the essential integer of a screen means sufficiently rigid to prevent wound overgrowth common to all the claims. Therefore, S&N has not infringed any of the claims in suit.
Whether infringement would be established absent finding on screen rigidity integer
392 As S&N’s product did not possess the screen rigidity integer, infringement is not established. Further, as discussed below, I have found that the claims are invalid for non-compliance with ss 40(2) and (3) of the Act (and claim 49 was invalid on the additional ground that it constituted a mere collocation). It is therefore unnecessary to determine whether other essential integers of the various claims were present in S&N’s products or whether S&N’s supply of products was for a use within the meaning of s 117(2)(a)-(c), for the purposes of establishing direct or indirect infringement of any claims. For completeness, I briefly consider the position in relation to infringement if that conclusion be wrong.
393 S&N conceded that its supply of kits (save for the new RENASYS F/P kits) would directly infringe the apparatus claims if their essential integers were present in its product. (If so, it would be unnecessary to determine whether the apparatus claims (if valid) were indirectly infringed).
394 S&N ultimately conceded that the screen porosity integer was valid and that the foam in its kits possessed that integer. S&N did not dispute that the sealing means was essential and was present in its products.
395 S&N submitted, however, that KCI had not proved that the tubular member positioning integers (claims 49, 50 and 52) were present in the RENASYS-F foam, which had a channel. Therefore, if (contrary to S&N’s primary submission) the tubular member positioning integers were essential, infringement of the relevant claims was not established. I have found that the integers were essential.
396 KCI relied on Professor Marshall’s evidence to establish the presence of those integers in the S&N foam. Professor Marshall relevantly deposed of the RENASYS-F kit:
When the drain tube is placed ‘into the channel in the foam’ in accordance with Step 6 [in the RENASYS-F Instructions], it will be ‘inserted into’ the foam as required by Claim 49.
…
From my inspection of the RENASYS-F Kit, when the drain tube is positioned in the channel in the foam section it is below the top surface of the foam on either side. In my opinion, the drain tube is beneath at least a portion of the foam. In use, I see no practical difference between the two descriptions in Claim 49 and Claim 50… When the RENASYS-F Kit is applied to a wound and negative pressure applied, I would expect the foam section to compress and envelope the drain tube. In use, the drain tube would be ‘inserted into’ and ‘inserted beneath at least a portion of’ the foam section. The drain tube would also be ‘embedded within’ the foam section, within the meaning of that phrase in Claim 52.
397 S&N submitted that, contrary to Professor Marshall’s evidence, the foam “looked flush” and thus was not inserted beneath at least a portion of the foam as required by claim 50, nor embedded within it, as required by claim 52.
398 Further, S&N submitted that Professor Marshall purported impermissibly to construe the integer in opining that the drain tube was beneath at least a portion of the foam because, as he asserted, it lay beneath at least a portion of the foam. He merely “expected” that the S&N foam would envelope the drain tube during the application of negative pressure, based on his visual inspection and his experience with the KCI kits.
399 In my opinion, Professor Marshall’s inspection of the S&N RENASYS-F foam sufficed to establish on the balance of probabilities (albeit by a slim margin) that the drain tube, when placed into the channel, was “inserted into” the foam, as required by claim 49, and was “inserted beneath a portion of the foam”, as required by claim 50.
400 I was not, however, satisfied that Professor Marshall’s expectation based on experience with the KCI foam established that the tube would be “embedded within” the RENASYS-F foam, as required by claim 52.
401 Thus, KCI failed to establish infringement of claim 52 on a basis additional to the screen rigidity integer.
402 As S&N contended, the more recent RENASYS-F/P kits would not infringe the kit claims (claims 49, 50 and 52) because, inter alia, the foam had a pad and the tube was therefore not inserted into the foam (49), inserted beneath at least a portion of the foam (50) nor embedded within it (52). Nor was the previous tube with a channel inserted into the foam or embedded within it.
403 S&N also alleged that a number of integers were mere mechanical variations or matters of clinical judgment. As discussed above, I have found that, as KCI submitted, the relevant integers were essential. S&N would thus not infringe unless it had taken all essential integers of any particular combination claim.
404 KCI alleged that the method claims were only indirectly infringed under the three headings of s 117, authorisation (s 13) and procuring (joint tortfeasors). Although it was not entirely clear, KCI appeared to allege that the method claims would be indirectly infringed by supply of the kits together with the vacuum pumps. S&N submitted, persuasively, in my view, that the last two were unlikely to add anything, as if KCI did not succeed under s 117, it could not succeed on the other grounds, because authorisation required control together with sanctioning, approval or countenancing of the infringement (Moorhouse at 12 and 20-21; Cooper v Universal Music Australia Pty Ltd (2006) 156 FCR 380 at 408-409). Further, joint tortfeasorship required “a concurrence in the act or acts causing damage” (The Koursk [1924] P 140) and, usually, “two or more persons acting in concert” (Thompson v Australian Capital Television Pty Ltd (1996) 186 CLR 574 at 581), as well as “participation, rather than mere facilitation” (Best Australia Ltd & Ors v Aquagas Marketing Pty Ltd & Ors (1988) 83 ALR 217 at 221). A common design is necessary.
405 Further, authorisation would not be made out if there were substantial non-infringing uses and the alleged authoriser did not control the primary infringer’s acts. (Australian Tape Manufacturers Association v The Commonwealth (1993) 176 CLR 480 at 498).
406 S&N defended allegations of infringement under s 117 of the Act, authorisation or procurement on various grounds, including that the kits were staple commercial products with many potential non-infringing uses and that it had not provided instructions in relation to various integers.
407 I was not persuaded that the kits were other than staple commercial products, or that they were capable of only one reasonable use or only infringing uses. The pumps, foam, tube and seal were well-known items of medical equipment supplied for various uses.
408 If, contrary to my findings, it became necessary to consider in detail indirect infringement of the method claims, as S&N submitted, s 117 would apply “claim by claim”, because the “use” of the method referred to in each claim was different, (for example, by reference to the duration of treatment and whether it were continuous or not).
409 Liability under s 117(2)(c) would depend on the instructions or inducements for use of the product, in relation to which S&N set out a detailed table, which I do not consider exhaustively.
410 S&N’s instructions in a number of instances were, however, inconsistent with particular integers of the various method claims. For example, the direction for use of the foam dressing kit and vacuum pumps was expressly to apply constant pressure, rather than to use the product with the application of cyclic negative pressure (as in claim 9) or in any ratio of application to non-application of negative pressure (claims 10, 11, 12 and 121).
411 Further, according to the testimony of Professors Penington and Kimble, physicians did not use pressure intermittently and S&N had no reason to believe that its product would be used with the application of cyclic negative pressure or any ratio of application to non-application of negative pressure. As Professor Penington deposed:
In using the KCI VAC device, I use the default pressure setting on the pump which I recall is about 120mmHg. Although the pump has both intermittent and continuous settings, I do not use the intermittent setting as patients have complained in the past that it is painful. The intermittent setting turns the pump on and off. I apply the treatment typically for three to four days then examine the wound. I stop treatment when the wound has reached what I consider to be an appropriate stage of healing which can vary depending on my treatment objective. In many cases, it is my intention to apply a skin graft to close the wound so I treat the wound with the KCI VAC until the wound has developed a good bed of granulation tissue suitable for grafting. Where I do not intend to apply a skin graft, I typically discontinue the treatment when the wound is close to healed, that is, when it has formed a nice bed of granulation tissue and is reducing in size. I may also discontinue treatment if the vacuum therapy does not appear to be helping the wound to heal and place a flap on the wound instead.
412 S&N’s instructions for use of the RENASYS-F foam dressing kit did not instruct to position the flexible tube so that it has an inlet end inserted into said open-cell polymer foam section (claim 49). Its instructions were to position the tube in the “channel in the foam”, so infringement under s 117(2)(b) and (c) would not be made out.
413 S&N’s instructions did not instruct to position the flexible tube so that it has a first end inserted “beneath at least a portion” of the foam section (claim 50). As stated above, its instructions for use of the RENASYS-F foam dressing kit contained an express instruction to position the tube into the “channel in the foam” rather than beneath it. Nor did S&N’s instructions contain any instruction to position the flexible tube so that it is embedded within the foam section (claim 52).
414 Further, S&N’s instructions did not recommend cyclic use, although some of its pumps were capable of it.
415 The grounds of revocation of a patent are set out in s 138(3) of the Act which provides:
After hearing the application, the court may, by order, revoke the patent, either wholly or so far as it relates to a claim, on one or more of the following grounds, but on no other ground:
(a) that the patentee is not entitled to the patent;
(b) that the invention is not a patentable invention;
(d) that the patent was obtained by fraud, false suggestion or misrepresentation;
(e) that an amendment of the patent request or the complete specification was made or obtained by fraud, false suggestion or misrepresentation;
(f) that the specification does not comply with subsection 40(2) or (3).
416 Section 18(1) of the Act states what is necessary for a patentable invention as follows:
(1) Subject to subsection (2), a patentable invention is an invention that, so far as claimed in any claim:
(a) is a manner of manufacture within the meaning of section 6 of the Statute of Monopolies; and
(b) when compared with the prior art base as it existed before the priority date of that claim:
(i) is novel; and
(ii) involves an inventive step; and
(c) is useful; and
(d) was not secretly used in the patent area before the priority date of that claim by, or on behalf of, or with the authority of, the patentee or nominated person or the patentee’s or nominated person’s predecessor in title to the invention.
417 The Schedule 1 Dictionary defines “invention” as follows:
invention means any manner of new manufacture the subject of letters patent and grant of privilege within section 6 of the Statute of Monopolies, and includes an alleged invention.
418 Section 40(2) of the Act provides:
A complete specification must:
(a) describe the invention fully, including the best method known to the applicant of performing the invention; and
(b) where it relates to an application for a standard patent—end with a claim or claims defining the invention…
…
419 Section 40(3) of the Act provides:
The claim or claims must be clear and succinct and fairly based on the matter described in the specification.
420 S&N by cross-claim alleges that the 14 claims it has allegedly infringed are invalid on the following grounds:
(a) novelty;
(b) lack of inventive step;
(c) manner of manufacture (method of human treatment/mere desiderata);
(d) failure to define the invention;
(e) lack of clarity;
(f) lack of fair basis;
(g) lack of sufficiency; and
(h) claim 49 only – a mere collocation.
421 The prior art is relevant to the novelty and lack of inventive step grounds of alleged invalidity. A summary of the main contents of the prior art documents in chronological order is set out below.
“Device for drainage of wounds” – a German Patent Office Patent published 25 August 1952 (“Wustmann”)
422 This patent document notes that the use of rubber sponge tampons to protect purulent or secreting wounds had a beneficial effect on healing, but fluids could accumulate, requiring frequent removal, which was unpleasant for the patient.
423 The invention described in this patent document removed or reduced the deficiencies. It had an open suction line in a soft fine porous tampon, which drew out fluid from the wound, or could supply liquid or disinfectant to the wound.
Svedman, “A dressing allowing continuous treatment of a biosurface” (IRCS Journal of Medical Science, May 1979) (“Svedman”)
424 This article describes a dressing consisting of a sheet of fluid-absorbent open-cell material made of crossing fibres of viscose, polyamide and polyester, coated with a thin film of plastic. Plastic tubes pass into opposing edges of the sheet, a treatment solution is connected to one of the tubes and suction is applied to the other.
425 The article states that the dressings were used on 12 patients with various types of ulcers; tyrodes solution was used as treatment; and suction was set at 20kPa. The patients became rapidly free of pain; rubor and oedema disappeared mostly within one to two days; excretions diminished; and healthy granulation tissue appeared rapidly so that skin grafting could be performed.
Johnson, “An improved technique for skin graft placement using a suction drain” (Surgery, Gynecology and Obstetrics, December 1984) (“Johnson I”)
426 This article describes a technique for fixing a skin graft to create “tight coaptation between graft and recipient site”. The method uses gauze impregnated with antibiotic ointment, dry gauze and a suction drain. The article also contains a diagrammatic representation of the technique.
Johnson, “Expanded use of suction drains” (Surgery, Gynecology and Obstetrics, May 1985) (“Johnson II”)
427 This article describes a technique for airtight closure of surgical wounds so as to allow effective use of suction drains. The technique involves application of an occlusive membrane dressing over the suture line, a thin strip of ointment-impregnated gauze and a synthetic, transparent, flexible adhesive film dressing.
428 The article provides a pictorial representation of a radical mastectomy and the way in which the occlusive membrane dressing renders the wound airtight. The paper notes that after investigating the technique in dogs, the authors found it applicable even if a portion of the incision is left fully open for any reason.
NA Bagautdinov, “Variant of External Vacuum Aspiration in Treatment of Purulent Diseases of Soft Tissues” (Current Problems in Modern Clinical Surgery, Interdepartmental Collection, 1986) (“Bagautdinov I”)
429 This article notes that active drainage of purulent wounds with lengthy vacuum aspiration promotes outflow of tissue fluid from the walls of the wound and its cavity, a reduction in perifocal edema, intratissue pressure, improvement in blood and lymph circulation, a collapse of the cavity and limitation of the infectious focus. It describes this as a method of physical treatment of antisepsis of the purulent focus and a means to accelerate healing of the wound process.
430 The article states that an apparatus of a “blood suction cup” is “now used” by being placed on the skin in the area of the inflammation focus. Vacuum treatment is accomplished in the range of 10-500 mmHg below atmospheric pressure for a few seconds to a few hours, which is often determined not by scientific-clinical argumentation, but also by the subjective viewpoint of the physician. The apparatus cannot be used where the bone protrudes or where there are physiological bends in the surface of the body. Further, using gauze rubber strips does not ensure uniform vacuum treatment of the entire cavity/surface of the wound, which leads to adhesion of the walls, difficulties in outflow of the wound secretion and products of necrolysis.
431 The authors propose a method of vacuum treatment of primary and secondary purulent wounds, which is devoid of these shortcomings. The treatment consists of the following.
432 After surgical treatment of the purulent wound and hemostasis, a drain of polyurethane foam adapted in shape and size is placed on the surface or cavity of wound. The surrounding skin is smeared with sterile Vaseline, antiseptic or inert salve on an oil base and covered with a polyurethane film.
433 During localisation of the purulent abscess on the forearm, shoulder, shin and thigh, isolation from the atmosphere is accomplished with a polyethylene sleeve, which is “attached to the skin on the periphery of the segment of the extremity distal and proximal to the wound with plaster”. For isolation of the hand, fingers and feet, polyethylene sacks are attached to the skin by a similar method proximal to the wound.
434 Regardless of the method of sealing, a tube is hermetically installed through the hole in the polyurethane, and connected to a vacuum pump through a collection vessel. At a vacuum of 10 to 60 mmHg, the film encloses the wound strictly along its skin boundaries, with uniform vacuum treatment of the walls only on the side of the cavity, and elimination of exudate because of the porous structure of the drain. The duration of treatment varies according to the degree of vacuum, ranging from 30 minutes to two hours, after which the polyethylene is removed and the gauze bandage placed. Sessions are conducted daily until the wound is clean, which takes approximately three to four days.
435 In patients with extensive purulent foci with a large amount of purulent secretion, continuous aspiration treatment was conducted using a tube above the polyurethane with a U-shape. A mini-irrigator was passed through one branch through an elastic plug and then to the wound. The second branch was connected to suction.
436 The article notes that polyurethane foam has a good suction effect. After 24 hours the polyurethane foam drain was impregnated with wound secretion in an amount 10 times exceeding the weight of the drain.
437 The article states that according to M. F. Kamaev, clearing of the wound occurred four to five days after surgical treatment, which was checked by the pH, total protein content in the exudate, the dynamics of the change in area and volume of the wound, and the result of cytological studies by surface biopsy. In 50% of patients with extensive wound defects, primary emergency or early secondary sutures were then placed.
438 According to the article, wounds healed without complications in all cases, and during comparative evaluation with the traditional methods of treatment (170 observations), healing and rehabilitation accelerated.
439 The article concludes that the proposed purulent disease treatment of soft tissues is “technically simple and clinically effective”. Vacuum aspiration accelerated the cleaning and sealing of the wounds of the 170 patients observed.
Kuznetsov and Bagaudinov, “Vacuum and vacuum-sorption treatment of open septic wounds” (“Bagautdinov II”)
440 This article states that the authors developed and tested methods of vacuum and vacuum-sorption treatment on septic wounds and abscesses on 170 patients.
441 After surgical treatment of the infected area, a drain made from polyurethane foam was placed in the wound. For sorption treatment, it was filled with activated charcoal powder. Sealing was done in several ways, depending on the localisation of the septic nidus.
442 Vacuum aspiration was conducted through a drainage tube using constant suction. The polyethylene film “clenched” the wound strictly at its edges, and the sorbent made secure contact with the walls. The porous structure of the drain allowed for removal of exudate and vacuumisation of the wound only from the cavity side.
443 According to the article, the session lasts one to two hours with negative pressure of 10-40 mmHg, after which the isolation is removed. The drain was changed one to two times daily and the vacuum treatment was continued for three to four days.
444 These patients had faster reduction of edema and tissue infiltration in comparison with the control group of patients treated with traditional methods of passive wound drainage, and also experienced disappearance of lymphangitis and hyperemia. Within the first two days of vacuumisation, a significant amount of wound exudate with a pH of 8.3±0.2 was removed, compared with initial values of 5.8±0.3. The ratio of solid to liquid of the material removed changed from 1:6 to 1:10.
445 As a result of the decompression-sorption effect, within the first day, the initial volume of the wound cavity declined by three to eight times. The wound was cleaned for four to five days on average, with the appearance of granulated tissue, proven by cytological testing. On average the duration of in-patient treatment reduced from approximately 12 bed days compared to the control group’s 17 bed days.
446 The article concluded that the recommended methods of treating open septic wounds were simple, available and clinically and economically viable.
“Method and apparatus for vacuum treatment of epidermal surface” – a UK patent application published 7 April 1988 (“Thorn”)
447 This patent document describes a method of applying subatmospheric pressure or partial vacuum to an epidermal surface. It does not describe treatment of a wound or damaged tissue, and S&N did not address this publication in its closing oral or written submissions.
Chariker et al, “Effective management of incisional and cutaneous fistulae with closed suction wound drainage” (Contemporary Surgery, June 1989) (“Chariker”)
448 This article states that management of fistulae requires a team approach. Ventral incisions complicated by enterocutaneous fistulae are particularly challenging, as containing the effluent is difficult.
449 The authors devised a closed suction wound drainage system which effectively drains from difficult sites, obviates skin damage, improves wound granulation and contraction and minimises dressing and nursing.
450 The authors tried to design a dressing that conforms to the wound bed. This conformation and the effectiveness of the continuous closed suction are critical to fistula closure and wound contraction. The most important facet of the authors’ system was its ability to remove effluent continually from the wound bed. This, in conjunction with an occlusive dressing, maintained the hydration of the tissue and prevented eschar formation (thus decreasing the inflammatory phase of wound healing). This, in turn, decreased granulation tissue and increased the rate of re-epithelialisation.
451 The article describes a closed wound drainage system. The dressing package consists of a Hemovac drain, one 2x2 inch square, 4x4 inch gauze squares, saline, a “Christmas tree” adapter, skin sealant, adhesive film to seal the wound site, Stomahesive paste, pink tape, and a continuous suction system.
452 Under the system, the drain is placed in the wound bed, gauze squares are to fill the wound, skin sealant is put on and adhesive film is placed over intact skin. The tube is connected to a continuous suction system.
453 The article notes that moist gauze packing is critical to the efficacy of the system. It states that the system contributes to wound closure by second intention, and sets out profiles of seven patients who were managed with the system.
454 The article concludes by stating that the closed suction wound drainage system has revolutionised the management of enterocutaneous fistulae complicating ventral abdominal wounds. It notes that initial evaluation has demonstrated that the system limits the degree of fibroplasia, which improves wound contracture and augments re-epithelialisation.
Jeter et al, “Managing draining wounds and fistulae: new and established methods” (Chronic Wound Care, 1990) (“Jeter”)
455 This article notes that the morbidity and mortality associated with enterocutaneous fistulae are universally recognised. Fistulae usually result from infection, obstruction, trauma, carcinoma, radiation, and Crohn’s disease. Spontaneous closure is impeded or prevented by these same factors and distal obstruction, presence of a foreign body, disruption of bowel continuity, malnutrition, and the “maturation” of the mucocutaneous opening.
456 The authors propose a closed suction wound drainage system to enhance management of incisional and cutaneous fistulae. The article states that the drainage system is effective in collecting drainage from the most difficult sites, appears to enhance wound closure, obviates skin damage, minimises nursing requirements and dramatically reduces the cost associated with conventional dressings and containment.
457 The article notes that Montgomery, Betancourt and Everett have described variations of the system, but these clinicians have not described a dressing that conforms to the wound bed. This conformation, combined with moist wound healing principles, is critical to fistula closure and wound contraction.
458 The article states that the most important part of the closed suction wound drainage system is the continuous evacuation of effluent from the wound bed. This, in conjunction with occlusive dressing, maintains optimal tissue hydration, and prevents necrosis and eschar formation, which are mechanical barriers to wound healing.
459 While the authors acknowledge that the results can only be compared to the results of traditional methods of management, it is believed that an increased rate of granulation and re-epithelialisation is seen with the closed suction wound drainage system.
460 The article states that a dressing package has been developed including one Jackson-Pratt Mini-Snyder Flat Hemovac drain, one 2x2 gauze square, 4x4 non-sterile gauze squares, normal saline, skin-sealant (eg Brad Barrier Film, Skin-Prep, etc.), transparent film dressing (eg AccuDerm, Bioclusive, Opraflex, Op-Site, Tegaderm, etc.) to seal the wound site, Stomahesive paste, pink waterproof tape, and a continuous suction system (wall or Emerson).
461 The closed wound draining system is broadly created in the following manner: (1) cleanse wound with normal saline; (2) moisten gauze square with normal saline; (3) trim fenestrated drain as needed to fit the wound; (4) open moistened gauze to line wound bed and place fenestrated drain in wound; (5) fluff wet gauze over fenestrated drain; (6) prepare surrounding skin with skin sealant; (7) cover with transparent film dressing and crimp the dressing around the tube; (8) “caulk” the tube exit site with Stomahesive paste; and (9) seal exit site with pink tape and attach to continuous suction.
462 The article states that there is a significant difference in costs. The traditional gauze and non-woven dressings for draining wounds can cost up to $1,400 per week. The maximum patient account for the closed suction wound drainage system is $205 for the first week and less thereafter.
463 Several patient profiles are described in the article. For example:
(a) A 42-year-old white male was transferred to the hospital’s intensive care unit with 13 plastic retention sutures from xiphoid to pubis. A small bowel fistula was located in his midline defect. The skin beneath and around the retention sutures was inflamed and denuded. There were Penrose drains in both upper and lower quadrants. After cleansing of the damaged skin and the retention sutures using a Water-Pik, a drain was threaded underneath the retention sutures along the midline wound defect. A wet gauze covering was threaded through to cover the drain. The entire abdominal surface was then covered with film dressing, encasing the retention sutures. Closed suction was achieved. The patient was comfortable, the skin healed, and the fistula closed in seven days.
(b) In the case of a patient with a renal fistula after a partial nephrectomy, the use of an ostomy pouch would have been impossible because of the size and location of the incision. The staff would have been unable to ascertain the amount of urine loss with leaking pouches or conventional dressings. In fact, it was concluded during the first three days of management with the closed suction wound drainage system that all the urine produced by the left kidney was draining from the flank. Once the fistula closed, the flank healed rapidly, the wound contracted, and only a small narrow scar remained. The patient had a small bowel fistula located in a midline wound defect that developed after a laparatomy for exploration of multiple abdominal abscesses. The fistula was managed in the same fashion and it closed in 11 days. In addition to these two draining wounds, the patient had a urostomy and a colostomy, both of which required pouches, and there would have been no space on the abdomen for a third pouching system.
464 The article states that the authors’ clinical observations suggested fistula effluent inhibits wound healing. They advocated continuous suction and found it superior to intermittent suction and gravity drainage with ostomy or wound management pouches. With the damp overlay gauze sponge, the wound bed would tolerate continuous low suction, and efficiency of the drainage system was maintained because the fenestrations were not occluded.
465 The combination of an occlusive dressing with the suction system effectively prevented tissue desiccation and necrosis. By minimising the inflammatory response, fibroplasia was reduced. The authors believed this encouraged rapid wound contraction and re-epithelialisation.
466 The article concluded by stating that the closed suction wound draining system had revolutionised the management of difficult draining wounds. The system had been invaluable for patients with enteric fistulae, a urinary fistula in a deep flank incision, a cutaneous lymph fistula, and an enteric fistula deep in a perineal wound. The system was far more effective in the authors’ hands and less cumbersome than other techniques described in the literature.
467 The authors preferred the closed suction wound drainage system for patients with all types of fistulae, unless the effluent is too thick to be evacuated by continuous low suction, because it encourages fistula closure with optimal wound healing, affords patients remarkable comfort, and results in dramatic cost savings.
Zamierowski, “Wound Dressing and Treatment Method” – a United States Patent published 13 November 1990 (“Zamierowski”)
468 This patent document describes that in the practice of the invention, a wound dressing is provided, which includes a cover membrane comprising a semi-permeable material with adhesive skin contact surfaces. An opening is formed in the interior of the membrane. An intermediate layer of material may be placed between the wound and the membrane contact surface, and a tube is used for either evacuating fluids from the wound or for passing liquid medication to the wound site. Both evacuation and introduction can be either active or passive.
469 The patent document states that membranes comprising semi-permeable materials are often preferred for wound dressings, because they can increase patient comfort and lower the risk of skin infection. However, problems arise with semi-permeable membranes when they are placed over draining wounds, because they tend to retain fluid.
470 The fluid often accumulates under a semi-permeable membrane during a draining period, which can macerate the underlying tissue, cause infection and otherwise inhibit healing. Past procedures which have involved opening or changing wound dressings tend to have problems associated with exposing a wound to greater risk of infection and are uncomfortable for patients.
471 The document states that a variety of wounds can be treated with the invention, including burns, cuts and ulcers.
472 The treatment method involves a tube or sheath adapted to fluidically communicate with the wound site through the membrane opening. It includes a proximate end, which extends through the membrane opening, and a distal end. The tube distal end is adapted for connection to a source for introducing liquid medication to the wound site, or suction source for evacuating fluid therefrom.
473 The first modified embodiment in the document provides for considerable flexibility in locating the wound dressing appropriately on the wound site. After the primary wound cover is positioned, the opening is formed at the chosen location and the wound dressing may be applied, much like a patch, with the tube distal end extending through the primary wound covery opening. Wound dressings may be changed as needed without changing the primary wound cover.
474 The second modified embodiment includes an intermediate layer of material between a wound site and a cover membrane. The intermediate material layer can comprise a number of materials with varying properties such as absorbency, wicking or capillary action and surface contact action. The intermediate material layer is primarily located in a chamber formed between the wound and the membrane.
475 As I have found that the screen rigidity integer was not established, it follows that, as S&N conceded, its allegation of invalidity due to lack of novelty must fail. For completeness, however, I consider the parties’ principal submissions on novelty assuming that, contrary to my finding, the screen rigidity integer was established in accordance with KCI’s submissions.
Relevant legislation and legal principles
476 Section 7(1) of the Act provides for when an invention is taken to be novel when compared with the prior art base. It relevantly provides:
For the purposes of this Act, an invention is to be taken to be novel when compared with the prior art base unless it is not novel in the light of any one of the following kinds of information, each of which must be considered separately:
(a) prior art information (other than that mentioned in paragraph (c)) made publicly available in a single document or through doing a single act;
(b) prior art information (other than that mentioned in paragraph (c)) made publicly available in 2 or more related documents, or through doing 2 or more related acts, if the relationship between the documents or acts is such that a person skilled in the relevant art in the patent area would treat them as a single source of that information;
…
477 The Dictionary defines “prior art information” used in s 7(1) to mean information that is part of the “prior art base”. As stated in KCI’s submissions, the applicable historical version of the Act defined “prior art base” to mean:
(a) in relation to deciding whether an invention does or does not involve an inventive step:
(i) information in a document, being a document publicly available anywhere in the patent area; and
(ii) information made publicly available through doing an act anywhere in the patent area; and
(iii) where the invention is the subject of a standard patent or an application for a standard patent – information in a document publicly available outside the patent area; and
(b) in relation to deciding whether an invention is or is not novel:
(i) information of a kind mentioned in paragraph (a); and…
…
478 It was not disputed that for the purposes of this case, the “patent area” should be treated as a reference to Australia.
479 Section 7(1) implicitly casts the onus of establishing that an invention is not novel, in the light of any one of the kinds of information specified in sub-paragraphs (a), (b) or (c), upon the party denying its novelty.
480 In determining whether a so-called invention is novel, it is necessary to compare the invention as claimed in the claims of the patent and prior art information, so as to ascertain whether the prior art anticipates what is claimed (H Lundbeck A/S & Anor v Alphapharm Pty Ltd (2009) 177 FCR 151 (“Lundbeck”) at 192 per Bennett J).
481 It was common ground that novelty was to be assessed by reference to the “reverse infringement test”, which was described by Aickin J in Meyers Taylor Pty Ltd v Vicarr Industries Ltd (1977) 137 CLR 228 (“Meyers Taylor”) as follows (at 235):
The basic test for anticipation or want of novelty is the same as that for infringement and generally one can properly ask oneself whether the alleged anticipation would, if the patent were valid, constitute an infringement.
482 Thus all the essential integers of the combination claims in suit must be disclosed by the prior art information sufficiently to enable the skilled addressee to perform the invention before the priority date.
483 In Lundbeck, Emmett J stated (at 169):
If the prior art information discloses information that enables the so-called invention to be performed, the so-called invention will not be novel. Whether prior art information does so will depend upon the claims made in respect of the so-called information. Thus, it is necessary to identify the so-called invention, so far as claimed in a particular claim. Once the so-called invention has been properly identified, it is a question of whether the prior art information discloses sufficient information to enable the relevant skilled addressee, at or before the priority date for the claim of the so-called invention, to perform the invention.
484 In Bristol-Myers Squibb Co v FH Faulding & Co Ltd (2000) 97 FCR 524 (“BMS”), Black CJ and Lehane J held (at 548) that:
[A] prior publication, if it is to destroy novelty, must give a direction or make a recommendation or suggestion which will result, if the skilled reader follows it, in the claimed invention.
485 In Hill v Evans (1862) 1A IPR 1 at 6 to 7 (“Hill v Evans”), Lord Westbury LC stated the classic test of the standard of disclosure required for a prior publication to anticipate an alleged invention:
I apprehend that the principle is correctly thus expressed: the antecedent statement must be such that a person of ordinary knowledge of the subject would at once perceive, understand, and be able practically to apply the discovery without the necessity of making further experiments and gaining further information before the invention can be made useful. If something remains to be ascertained which is necessary for the useful application of the discovery, that affords sufficient room for another valid patent… the question is, what is the nature and extent of the information thus acquired which is necessary to disprove the novelty of the subsequent patent? There is not, I think, any other general answer that can be given to this question than this: that the information as to the alleged invention given by the prior publication must, for the purposes of practical utility, be equal to that given by the subsequent patent. The invention must be shewn to have been before made known. Whatever, therefore, is essential to the invention must be read out of the prior publication. If specific details are necessary for the practical working and real utility of the alleged invention, they must be found substantially in the prior publication. Apparent generality, or a proposition not true to its full extent, will not prejudice a subsequent statement which is limited and accurate, and gives a specific rule of practical application.
The reason is manifest because much further information, and therefore much further discovery, are required before the real truth can be extricated and embodied in a form to serve the use of mankind. It is the difference between the ore and the refined and pure metal which is extracted from it.
Again, it is not, in my opinion, true in these cases to say, that knowledge, and the means of obtaining knowledge, are the same. There is a great difference between them. To carry me to the place at which I wish to arrive is very different from merely putting me on the road that leads to it. There maybe a latent truth in the words of a former writer, not known even to the writer himself; and it would be unreasonable to say that there is no merit in discovering and unfolding it to the world.
Upon principle, therefore, I conclude that the prior knowledge of an invention to avoid a patent must be knowledge equal to that required to be given by a specification, namely, such knowledge as will enable the public to perceive the very discovery, and to carry the invention into practical use.
(emphasis added)
486 To similar effect, it was observed in General Tire at 138 that:
To anticipate the patentee's claim the prior publication must contain clear and unmistakable directions to do what the patentee claims to have invented: Flour Oxidising Co Ltd v Carr & Co Ltd (1908) 25 RPC 428 at 457, line 34, approved in BTH Co Ltd v Metropolitan Vickers Electrical Co Ltd (1928) 45 RPC 1 at 24, line 1. A signpost, however clear, upon the road to the patentee's invention will not suffice. The prior inventor must be clearly shown to have planted his flag at the precise destination before the patentee.
487 It has been frequently reiterated that the test for anticipation by a prior document or patent is quite rigorous. As Finkelstein J stated in Root Quality Pty Ltd v Root Control Technologies Pty Ltd & Ors (2000) 49 IPR 225 at 243, “[t]he prior publication must give directions which will inevitably result in something within the claim”.
488 It was observed in General Tire (at 485-486) that:
[I]f carrying out the directions contained in the prior inventor's publication will inevitably result in something being made or done which… would constitute an infringement… the patentee's claim has in fact been anticipated.
489 The nature of the test has been described in other authorities in the following language:
(a) “[a]ny information as to the alleged invention given by any prior publication must be for the purpose of practical utility, equal to that given by the subsequent patent”: Canadian General Electric Co Ltd v Fada Radio Ltd (1930) 47 RPC 69 at 90;
(b) “clear description of, or clear instructions to do or make, something that would infringe the patentee’s claim if carried out after the grant of the patentee’s patent”: General Tire at 138; and
(c) in the case of anticipation by doing an act in public, one can usually ask “what information was given” to a person skilled in the art by the use in question: Insta Image Pty Ltd & Anor v KD Kanopy Australasia Pty Ltd & Ors (2008) 78 IPR 20 at 44-45 (“Insta Image”).
490 In Lundbeck, it was alleged that a patent which claimed the (+) enantiomer of a compound lacked novelty because it had either been anticipated by prior art information which disclosed a racemic mixture of (+) and (-) enantiomers, or by prior art information which disclosed the (-) enantiomer as such, but did not characterise the (+) enantiomer, the preparation of which would require another inventive step to be taken. The prior art considered in Lundbeck did not disclose the very thing claimed under the patent in suit, so the result of that case is not directly applicable to the facts of the present case.
491 In Lundbeck, Bennett J (with the assent of Middleton J) analysed the law of novelty. Her Honour summarised the principles at 190 as follows:
The following general propositions emerge from the authorities:
• An invention is a piece of information… It follows that a disclosure is the communication of information.
• Commonly the only question may be whether the prior publication describes the claimed invention with sufficient clarity…
• The disclosure is assessed by reference to the skilled addressee, a person of ordinary skill in the art.
• The question is whether the prior publication is sufficient to make the claimed invention apparent to the skilled addressee…
• A prior publication does not invalidate a patent unless it supplies sufficient information to enable a person of ordinary skill to produce the product subsequently claimed… A specification is not to be read as in a vacuum but by the reader having at least the common knowledge of the art…
• The requirement is that a person of ordinary knowledge of the relevant subject would be able practically to apply the prior published discovery without the necessity of making further experiments…
• The further experiments do not include those that formed part of standard procedure or common general knowledge. They are experiments with a view to discovering something not disclosed…
• The further experiments do not mean ordinary methods of trial and error…
• If the alleged anticipation is to a process that produces the claimed product, it is not an anticipation if the process would not necessarily achieve the result claimed for it…
• Something less than a full description of the invention allegedly anticipated may be sufficient to invalidate it for want of novelty…
• Something less than a full description of an effective means by which the combination claimed in a patent may be produced may be sufficient to a reader having common general knowledge in the art…
• A direction, recommendation or suggestion may be implicit in what is described…
• A disclosure that describes an effective means by which a claimed invention may be produced falls short of anticipation if it requires the exercise of inventive ingenuity or the taking of any inventive step…
• Where the prior disclosure is to a broad chemical claim encompassing many compounds, there may not be anticipation in the absence of the skilled addressee understanding or perceiving a specific compound in the disclosure… That is, there is no actual description of the particular compound to the skilled addressee; there is no relevant disclosure. There may be a distinction, albeit fine, between a “fleeting” or “paper” disclosure or the “intellectual content” of a disclosure on the one hand and a “disclosure for novelty purposes” or “enabling disclosure” on the other… It depends on what the skilled reader would understand.
(citations omitted)
492 Bennett J considered Hill v Evans and continued (at 192-193):
Care must be taken to distinguish between the tests for novelty and want of inventive step, in particular when looking to see what the prior art “teaches”. The concept of novelty in Australia involves a comparison between the invention as claimed in the claims of the patent and prior art information. Often, this must be determined by looking to prior publications which are to be read by the skilled addressee to determine what they disclose. Generally speaking, the consideration of what a prior publication “teaches”, especially when one talks of “teaching away” from the claimed invention, tends to be relevant to questions of obviousness and inventive step.
As Lord Hoffmann said in Merrell Dow 33 IPR at 8, an invention is a piece of information and making matter available to the public therefore requires the communication of information. Whether or not such information has been communicated depends on the subject matter of the claim and the extent of the prior disclosure to the skilled addressee.
Where the prior publication discloses exactly what is claimed, there is anticipation. This can be objectively determined and, apart from an understanding of terms of art, the evidence of the skilled addressee is not likely to be of much further assistance. However, this does not always occur and many of the authorities contain discussions of the extent to which a disclosure less than the entirety of the claim constitutes an anticipation of a product or a process to deprive the claimed invention of novelty.
If the prior art discloses some but not all integers of a claimed patent to a product, such as a combination, there is anticipation if the skilled addressee would add the missing information as a matter of course and without the application of inventive ingenuity or undue experimentation.
It may be that the prior disclosure is of a method that produces the claimed product. If that method leads inexorably to the product, there is anticipation (General Tire 1A IPR at 138). If it may or may not result in the claimed product, there is no anticipation.
It is these last two examples that, in Australia, could be said to be within a shorthand description of “enabling disclosure”. That is, the disclosure is not complete but it is sufficient to enable the skilled addressee, in the ordinary course and without invention, to add what is missing in the prior publication to obtain the claimed invention. The term “enabling disclosure” may also be apposite to disclosure to the skilled addressee of an asserted prior use: whether what the skilled addressee observes on inspection is sufficient to enable him or her to comprehend the complete invention (eg Insta Image Pty Ltd v KD Kanopy Australasia Pty Ltd (2008) 78 IPR 20; Jupiters), that is, whether it is sufficient to amount to a disclosure of the invention.
493 Bennett J then considered the speech of Lord Hoffman in Smithkline Beecham plc’s (Paroxetine Methanesulfonate) Patent [2006] RPC 10, and in particular, the UK requirements of disclosure and “enablement” on a want of novelty case. Her Honour continued (at 194):
For the purposes of disclosure, the prior art must disclose an invention which, if performed, would necessarily infringe the patent. Once the very subject matter of the invention has been disclosed, the person skilled in the art is assumed to be willing to make trial and error experiments to get it to work. For the purposes of disclosure, the disclosure is either of an invention which, if performed, would infringe the patent, or it is not. When Lord Hoffmann went on to say that, for the purposes of enablement, the question is no longer what the skilled person would think the disclosure meant but whether he was able to work the invention which the Court has held it to disclose, his Lordship was talking of what, in Australia, is covered by sufficiency of disclosure or description.
It follows that, where the prior publication is of the subsequently claimed invention, that is sufficient. Where the prior disclosure falls short of a complete disclosure, the question of the sufficiency of that disclosure arises. It is there that consideration must be given to the quality of a disclosure to the skilled addressee armed with common general knowledge. It is in that context that, in a limited fashion, questions of “enablement” can be said to arise. The use of that expression tends to cause confusion between anticipation and sufficiency. Rather, the Court, armed with the evidence of the skilled addressee as to terms of art and the nature and extent of the disclosure in the prior art document, must determine whether the prior disclosure is sufficient to enable the skilled addressee to perceive, understand and, where appropriate, apply the prior disclosure necessarily to obtain the invention.
494 In Apotex Pty Ltd v Sanofi Aventis (2008) 78 IPR 485, Gyles J stated at 525:
Anticipation is deadly but requires the accuracy of a sniper, not the firing of a 12 gauge shotgun.
495 In Nicaro Holdings at 527-532, Gummow J stated:
This is because to establish infringement of a combination patent the patentee must show that the defendant has taken each and every one of the essential integers of the plaintiff’s claim; if on its true construction the claim is for a particular combination of integers and the alleged infringer omits one of them, the infringer escapes liability: Populin v HB Nominees Pty Ltd (1982) 59 FLR 37 at 41. Further, where what is in question is an inessential integer, a device which contains the essential integers will fall within the claim, whether or not an inessential integer is replaced by an obviously equivalent device or omitted altogether; hence, the expression “mechanical equivalent”: Walker v Alemite Corp (1933) 49 CLR 643 at 650, 657; Sunbeam Corp v Morphy-Richards (Australia) Pty Ltd (1961) 35 ALJR 212 at 217; Blanco White, Patents for Inventions, 4th edn, para 2-208.
…
It follows from the English authorities as they have been applied in Australia that, whilst Hill v Evans does not require a literal disclosure and something less may suffice, and whilst an alleged paper anticipation is to be treated as read by a skilled addressee, a disclosure will fall short of an anticipation by description of an effective means by which the combination claimed in the patent in suit might be produced, if what is required of the skilled addressee is the exercise of any inventive ingenuity and the taking of any inventive step.
…
In R D Werner & Co Inc v Bailey Aluminium Products Pty Ltd (1989) 12 IPR 513; 85 ALR 679, King J, at first instance, used the terms “workshop variation” and “mechanical equivalent” in the course of dealing with an objection to grant for want of novelty (see 13 IPR at 537; 85 ALR at 703). I accepted the proposition, drawn from his Honour’s reasoning, that where the alleged anticipation disclosed all the essential integers of the claimed combination, the conclusion as to lack of novelty which would follow therefrom was not avoided and the invention claimed would not be saved “merely because there were differences which might be described as mere mechanical equivalents or workshop variations” (see 85 ALR at 708, 716). The use of the expression “workshop variation” was not designed to introduce any concept of the presence or absence of a further step which was an inventive step or any notions drawn from the law as to obviousness. (It may be noted that in Sunbeam Corp v Morphy-Richards (Australia) Pty Ltd (1961) 35 ALJR 212 at 220, Windeyer J, when dealing with want of novelty, spoke simply of the doctrine of mechanical equivalents.) In any given case, there may well be an overlap between novelty and obviousness on the evidence before the court, and to use a mechanical equivalent may be to effect a workshop variation; but that should not encourage any blurring between the legal norms of novelty and obviousness.
(emphasis added)
496 In Apotex Pty Ltd v Sanofi-Aventis (2009) 82 IPR 416 (“Apotex”), Bennett and Middleton JJ reiterated the above propositions at 433-434 as follows:
From the consideration in Lundbeck, the following is apposite to the consideration of anticipation by the prior art patents in this case:
• Where the prior publication discloses exactly what is claimed, there is anticipation: Lundbeck at [180].
• There is anticipation if the skilled addressee would add missing information to what is disclosed in the prior art as a matter of course and without the application of inventive ingenuity or undue experimentation: at [181]. A disclosure is sufficient if it enables the skilled addressee, in the ordinary course and without invention, to add what is missing in the prior publication to obtain the claimed invention: at [183].
• If the prior art discloses the very subject matter of the invention, the person skilled in the art is assumed to be willing to make trial and error experiments to get it to work: at [189]. If the disclosure is of an invention which, if performed, would infringe the patent, there is anticipation.
• The question is whether the disclosure is sufficient to enable the skilled addressee to perceive, understand and, where appropriate, apply the prior disclosure necessarily, but within the ordinary limits of trial and error, to obtain the invention: at [190].
497 S&N’s primary overarching contention was that the screen rigidity integer was nonsensical and was added to the claims to satisfy the Examiner’s requirements for conformity with the inclusion of a like reference in the detailed description and the body of the specification, which was, in turn, directed at overcoming the prior art that would otherwise invalidate the claims for want of novelty. S&N alleged, in that context, that the terminology of many integers employed in the claims was pseudo science designed to elevate a simple pump to a therapy unit, or a dressing to a “screen means to prevent wound overgrowth”, and thus disguised, with meaningless labels for commonplace items, the lack of inventiveness.
498 S&N’s challenge to the validity of the claims based on lack of novelty was subsidiary and alternative to its fundamental attack on the screen rigidity integer. It acknowledged that success in its overarching argument would be inconsistent with a finding that the screen rigidity integer was disclosed by the prior art.
499 Subject to its overriding concession based on the non-existence of the screen rigidity integer, S&N in written submissions asserted that the claims were not novel pursuant to s 18(1)(b) of the Act, having regard to disclosures in the following ten documents considered individually, which are briefly summarised above:
(a) Bagautdinov I;
(b) Bagautdinov II;
(c) Zamierowski;
(d) Chariker;
(e) Jeter;
(f) Johnson I;
(g) Johnson II;
(h) Svedman;
(i) Wustmann; and
(j) Thorn.
500 At trial, however, S&N relied principally on Bagautdinov I, Zamierowski, Chariker and Jeter (individually), and Jeter and Chariker (read together) to establish that the essential integers of the claims in suit were anticipated and hence lacked novelty.
501 S&N also relied upon the prior use to which Dr Williams testified, discussed at [133] to [144].
502 The prior art is to be considered in this context as at the priority date which, as discussed below, I have found to be 14 November 1991.
503 Had the priority date been deferred to 7 November 1996 as alleged by S&N, the following additional disclosures would have been relevant:
(a) the disclosure in PCT Application No. 93/09727, “Method and Apparatus for Treating Tissue Damage”, laid open to public inspection at the World Intellectual Property Organization on 27 May 1993;
(b) the disclosure in Australian Patent Application No. 31303/93, “Method and Apparatus for Treating Tissue Damage”, laid open to public inspection at the Australian Patent Office on 15 June 1993;
(c) the sale, display or offering for sale in Australia by KCI of the products referred to in paragraphs 2-22 of the affidavit of Peter Denis Hickey made on 2 March 2009; and
(d) the display and use in Australia in the early 1990s by KCI of the KCI V.A.C.® Therapy System as referred to in the affidavit of Professor Donald Roger Marshall sworn 17 September 2009.
504 S&N did not submit that any prior art document, including Bagautdinov I and Zamierowski, on which it principally relied, exactly, completely and expressly disclosed all the integers of the relevant claims.
505 It submitted, however, that some of those integers were meaningless or alternatively, inessential, so that the absence from the prior art did not preclude anticipation. Alternatively, S&N, relying on Lundbeck, Apotex and Nicaro Holdings, submitted that relevant directions were implicit in what was described; that some integers, although not disclosed, would be added by the skilled addressee; or that as a matter of course, the method described would lead inexorably to the product or reproduce the results, irrespective of the lack of any express reference.
506 S&N acknowledged that the 14 claims in suit contained a large number of variations (about 30 in all) of the following fundamental elements of the combination (method or apparatus) described in the Patent:
(a) vacuum means;
(b) sealing means associated with the vacuum means to maintain negative pressure on the wound;
(c) screen means positioned at, on or in the wound; and
(d) a tube connecting the vacuum means to the screen.
507 S&N submitted:
The “fifth aspect” of the consistory clauses at p2 line 29 – p3 line 37 (esp p3 lines 24-30) is a convenient starting point. It has the essential elements of:
A fifth aspect of the invention is an apparatus for facilitating the healing of wounds which comprises vacuum means for creating a negative pressure on the area of tissue surrounding the wound, sealing means operatively associated with the vacuum means to maintain the negative pressure on the wound, and screen means for preventing overgrowth of tissue in the wound area.
The preferred embodiment (p3 lines 30-37) is also relevant:
A preferred embodiment of the invention comprises a section of open-cell foam configured to be placed over a wound, a flexible tube inserted into the foam section for attachment to a suction pump, and a flexible polymer sheet overlying the foam section and tubing and configured to be adhered to the skin surrounding the wound.
The preferred embodiment thus narrows the fifth aspect by specifying that the screen means be open-cell foam, that the sealing means be a flexible polymer sheet, and by adding the flexible tube.
Of the claims asserted by the Applicants:
(a) All claims require the screen means. The claims which specify that it be open-cell foam are 49, 50 and 52. The remainder are met by gauze.
(b) Claims which possess the tube are 49, 50, 52, 110 and 112.
(c) No claims are limited by the vacuum means.
(d) Claims which possess the sealing means are 49, 50 and 52.
508 S&N acknowledged that because there were such a large number of differently expressed integers in the claims in suit, a novelty analysis by reference to the large quantity of prior art was “very daunting”. Ultimately, its written submissions did not deal exhaustively with what was allegedly disclosed even by the four principal documents, and did not deal with the subsidiary prior art. The following discussion similarly does not purport exhaustively to compare all the integers in all the claims with alleged disclosures in all the prior art.
509 If a large number of integers were either characterised as inessential or held to be inherently disclosed by a teaching, the likelihood of anticipation of many claims by the prior art would be much greater. I have already discussed the allegedly inessential integers above in relation to infringement. I concluded that they were essential. Therefore the prior art would have to disclose such integers as a necessary precondition of invalidating a relevant claim on the grounds of novelty.
510 S&N submitted that integers of the claims in suit were inherent in Bagautdinov I and Zamierowski and other prior documents as follows:
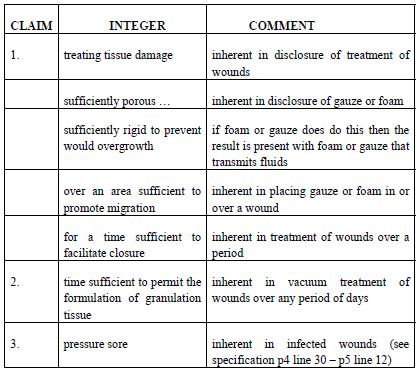
511 The most important integers alleged to be inherent were the screen rigidity and the screen porosity integers. In S&N’s submission, KCI was effectively “hoist on its own petard” as it either could not establish infringement on the basis of the mere presence in S&N’s product of foam that was sufficiently porous to transmit fluids and did not collapse on itself, or alternatively, would lose on novelty because the relevant integers were present in the prior art on the same basis.
512 KCI submitted that the above submission mischaracterised its infringement case. Further, in the present case, no prior publication anticipated any of the combination claims, as none disclosed all of the essential integers of the combination. It denied S&N’s assertions that various integers of the relevant claims were “not proper functional limitations” and “d[id] not operate to distinguish the claims over the prior art”, were inessential, meaningless or inherently disclosed.
513 Further, KCI emphasised that none of the prior art publications could be “mosaiced” together for the purposes of anticipating an invention unless they would be read together by the person skilled in the art.
514 Where the alleged anticipation does not disclose all the integers of the patent in suit, the fact that the skilled addressee could come from the alleged anticipation to the patent in suit without the exercise of inventive ingenuity in the light of common general knowledge did not suffice to establish lack of novelty.
515 For the purposes of “novelty”, the prior art against which the novelty of the claimed invention is to be assessed includes any information made publicly available in a document anywhere in the world.
516 Information will be made “publicly available” if it is accessible to a member of the public in circumstances where that person would be free in law and equity to make such use of it as they saw fit. While KCI initially denied that Bagautdinov I and Bagautdinov II were publicly available, ultimately, it was not disputed.
Submissions and evidence on Bagautdinov I
517 Bagautdinov I was dedicated to cleaning purulent wounds and the drainage of unwanted fluids (principally pus) in infected wounds by a system of treatment applied in brief daily sessions of 30 minutes to two hours, after which the film was removed while the foam remained in place for the remainder of the day. It also described a modification comprising a continuous irrigation system which could be applied to wounds with multiple foci of infection, simultaneously with negative pressure.
518 S&N submitted that Bagautdinov I anticipated the apparatus claims in suit. While initially S&N also relied on Bagautdinov II, ultimately it conceded that it added nothing to Bagautdinov I in the present context. In S&N’s submission, Bagautdinov I disclosed a method and an apparatus for treating wounds (in particular, purulent wounds) using a vacuum pump, with a screen of polyurethane foam adapted in shape or size to the wound. It also disclosed a polyurethane film seal and Vaseline, a vacuum of 10 to 60 mm Hg, and a tube connected to a pump, which is used either intermittently or continuously, and that the method and apparatus worked highly successfully to clean and heal wounds.
519 The method claim 1, disclosed as the “area sufficient” integer, was met because the negative pressure in Bagautdinov I was applied over the whole wound, and the “time sufficient” integer was met by the three to four or four to five days stated in Bagautdinov I, which, as healing was a continuum, would “facilitate closure”.
520 Claim 2 was met because granulation tissue would be forming. Claim 3 was met because an infected wound included a pressure sore. Claims 6 and 7 were met as the Bagautdinov I treatment was for three to five days. Claim 8 was covered because the combined treatment in Bagautdinov I was substantially continuous. The cyclic and ratio claims in the Patent depended, in S&N’s submission, on non-essential integers, so their absence from Bagautdinov I did not preclude anticipation.
521 S&N also relied on the following findings by the English Court of Appeal, described as follows in S&N’s written submissions:
In the United Kingdom the Court of Appeal (and Wyand J at first instance) held that Bagautdinov disclosed:
(a) a method and an apparatus [29], [92] CA; [26] Wyand J;
(b) for treating wounds (in particular “purulent wounds”) [30] CA;
(c) using a vacuum pump [42], [46] CA; [33] Wyand J;
(d) with a screen (“drain”) of polyurethane foam [42]-[46] CA; [33] Wyand J;
(e) adapted in shape or size (to the wound) [42], [46] CA; [33] Wyand J;
(f) placed on the surface or in the cavity [42], [46] CA; [33] Wyand J;
(g) sealed by a polyurethane film and Vaseline [42], [46] CA; [33] Wyand J;
(h) at a vacuum of 10 to 60 mm Hg [42], [46] CA; [33] Wyand J;
(i) with a tube connected to a pump [42], [46] CA; [33] Wyand J;
(j) used either intermittently or continuously [120] CA;
(k) that the method and apparatus worked highly successfully to clean and heal wounds [32] CA; [32] Wyand J.
522 KCI submitted that Bagautdinov I was directed to a device for removing pus from a purulent defect, and, unlike the Patent, was not concerned with a mechanism for actively promoting healing. The technique described in Bagautdinov I was used to drain pus and once the wound was clean, the drainage sessions were stopped. There was no false dichotomy between promoting healing and removing exudate, because in contrast to the Patent, Bagautdinov I did not link the application of suction to the formation of granulation tissue or the closure of the wound. It did not mention the rigidity of the foam or its suitability for preventing wound overgrowth. Therefore, Bagautdinov I did not give the requisite “clear and unmistakeable directions” to do what the patentee claimed.
523 Professor Penington, who gave evidence in relation to Bagautdinov I, testified that variants of a suction cup used in its treatment were not encountered in modern Western medicine, but rather, were suggestive of alternative or medieval medicine.
524 In his first affidavit, Professor Penington set out the existing disadvantages of treating an infected wound (which could apparently be either open or closed) by the application of a suction cup described in Bagautdinov I, the method of treatment it advocated and the promised advantages of vacuum aspiration of purulent wounds.
525 Professor Penington observed that many of the claimed advantages were similar to those provided by vacuum treatment.
526 He deposed:
If I had read this article before 13 November 1991, I would have understood it as a method for treating purulent (infected) wounds.
If I had read the paper prior to 1991 and wished to replicate the technique, I would have used the available materials to hand. Foam rubber, which I believe is polyurethane foam, was and is available sterile in operating theatres where it is used for dressings on skin grafts and to spread skin preparation solutions. For the polyethylene film, the obvious substitute would have been the adhesive film dressings OpSite or Tegaderm which were widely available in operating theatres in a range of sizes. Tubing was also widely used in closed wounds and would have been an obvious choice to supply the vacuum. The arrangement made in attempting to replicate the description given in the paper would therefore have closely resembled the early vacuum dressings that were used clinically in Australia from about 1992.
On the basis of the description in the article I would have applied the technique to infected wounds.
527 As discussed above, Professor Penington could assign no meaning to the prevention of wound overgrowth, but assuming that the treatment with the Patent’s device did prevent it, he thought that the technique he would have devised to replicate the Bagautdinov I technique would have the same result. Similarly, he deposed that he would have read Bagautdinov I as describing the advantage of formation of blood vessels, the faster formation of granulation tissue in relevant wounds and a faster rate of skin closure, which he would have identified with the facilitation of wound closure described in the Patent.
528 Although Bagautdinov I indicated an average duration of three to four days’ treatment, Professor Penington would have considered applying it for longer to wounds which would benefit. From Bagautdinov I’s references to polyurethane foam as a porous structure and “a drain”, he would have understood that it must be open-cell foam, so that it could draw fluid into it and act as a porous drain.
529 Professor Penington deposed that he would have assumed that the polyethylene film described in Bagautdinov I was fluid impermeable and would have used OpSite and Tegaderm. He would have placed the tube in the centre of the foam to prevent its blockage with wound exudate and to prevent the plastic cover from blocking the holes in the top of the tube.
530 In cross-examination, Professor Penington agreed that he had read Bagautdinov I only after reading the Patent and using the KCI V.A.C® product for over a decade.
531 Professor Penington agreed that a number of terms used in Bagautdinov I were not “terms of medical precision” and lacked specificity. He conceded that although it was clear that the treatment was applied to infected wounds, that was the only delimiting factor and there was no reference to ulcers or pressure sores.
532 He considered that the Bagautdinov I instructions implied that the foam was to be placed in the wound, but did not specify that it be so confined. Further, although there was no specification that the foam have any particular porosity, he assumed that it must be porous enough to work as a drain.
533 Professor Penington agreed that the reader was told nothing of the relationship between the tube and the foam, or the basis on which to select a time within the stated range of 30 to 120 minutes for particular wounds. He did not think that the reference to “uniform vacuum treatment” of the side walls only could mean that fluid should be sucked only from the walls and not the base of the wound, as that was hard to imagine.
534 He envisaged that the foam was to be left in the wound after the treatment, but agreed Bagautdinov I did not say what was done with it. He was unsure if fresh foam were to be placed in the wound each time, but suspected that it was not. That suspicion was fortified by the paper’s description of weighing fluid-impregnated foam after a 24 hour period.
535 Professor Penington agreed that Bagautdinov I indicated that the wound was considered clean after the procedure ceased, which was, on average, after three or four days. He conceded that the average duration was inconsistent, albeit not “dramatically” so, with the four to five days later mentioned in the paper. He agreed that Bagautdinov I revealed nothing about any longer treatment for wounds that were responding beneficially, and said that he would draw on his own experience in applying treatment for a longer period.
536 While not surprised at the concept of suction drains to suck fluid from an infected wound, Professor Penington associated a suction cup referred to in Bagautdinov I with alternative medicine and would have believed it to be very inefficient. He would not have been enthusiastic about the teachings of Bagautdinov I.
537 Professor Penington agreed that Bagautdinov I gave no specific information about its modified technique of wound irrigation, including the number of patients who had been subjected to it, the circumstances in which it was to be applied or its interaction with the standard method in Bagautdinov I. The paper did not explain the basis for the specified duration of the treatment and left vague significant details, such as the intervals for changing the foam drain and the proportion of the 170 persons treated whose wounds underwent a simultaneous application of negative pressure and irrigation. Nor could he explain what the early secondary sutures used in 50% of the patients were.
538 Professor Penington was not familiar with the described technique of checking the cleaned wound by pH total protein content and was unable to explain its objective, or how any reduction could definitely be detected, but agreed that it was probably directed at assessing a change in inflammation, which was an impediment to wound contraction.
539 Professor Penington agreed that Bagautdinov I’s claim that the wounds of 170 patients healed without complication was very ambitious. He considered that the paper was not written according to scientifically robust standards and its assessments were unsupported by data. He considered both Bagautdinov I and Bagautdinov II to be clinical papers rather than scientifically based.
540 Further, Bagautdinov I did not discuss any process responsible for the benefits claimed, other than evacuation of fluid.
541 Professor Penington believed that he could, as at 1991, have assembled components which would function as the apparatus and produce like results. In cross-examination, however, he acknowledged the lacunae, absence of instructions, inconsistencies and mystifying references in Bagautdinov I.
542 In particular, he agreed that in Bagautdinov I, wound contraction was to be achieved by drainage of pus and reduction of inflammation, not the application of negative pressure; the time frames for application of negative pressure to achieve the formation of granulation tissue were not specified; the position of the tube relative to the foam was not specified; nothing was taught in relation to the application or the maintenance of continuous negative pressure or alternative periods of cyclical negative pressure.
543 Dr Pohl also gave evidence on Bagautdinov I. He was unfamiliar with many terms it used, some of which made no sense to him. He took Bagautdinov I to refer to the introduction of a vacuum drain into purulent infective wounds to drain the wound cavity and keep them free of purulent inflammation such as blood and pus.
544 He observed that Bagautdinov I did not specify how the film was attached to the skin, but assumed that sticking plaster was used. It did not say where the tube was to be positioned relative to the foam.
545 Dr Pohl also read the reference to “enclose the wound strictly along its skin boundaries” and the application of uniform vacuum only to the side of the cavity as indicating that the base of the wound should not be treated, which he would not know how to achieve.
546 Dr Pohl would have understood that the physical properties of the foam allowed the egress of pus and fluid through it, on the application of the vacuum.
547 He observed that the foam was weighed to measure the extent of its impregnation with wound secretion, but Bagautdinov I gave no guidance on the relationship between that measurement and the duration of treatment or the level of suction to be applied. Thus “[i]t just shows that the foam can be permeated by the contents of the wound, is absorbent and can store a large volume of material.”
548 Dr Pohl noted a number of other apparent contradictions, particularly about the duration of time required to clean the wound and deficiency of instructions and terms that he could not comprehend. He would have been sceptical of the assurance that the wounds of 170 patients healed without problems or complications and would have found the language unclear and contradictory.
549 Dr Pohl agreed that although Bagautdinov I did not mention the promotion of granulation tissue, it could be assumed by virtue of the fact that the wounds were cleaned and were reducing in size. He thought that to the extent that disadvantageous exudate was removed, granulation tissue would be enhanced.
550 S&N relied particularly on Dr Pohl’s evidence to establish the inherency of the screen porosity and screen rigidity integers in Bagautdinov I, submitting that those qualities could be inferred from the reference to polyurethane foam. Dr Pohl initially agreed that the foam referred to in Bagautdinov I must be porous and probably open-celled in order to suck fluid through. He conceded that as a reasonable inference, it was sufficiently porous to allow oxygen or gases to reach the wound. At a subsequent point, however, Dr Pohl appeared to retract his concession and stated that he would make that inference only on the assumption that all polyurethane foams were the same. In relation to the rigidity of the foam, the following exchange occurred:
Would you agree that it is reasonable to infer that the Bag[autdinov] foam is rigid enough to fill the spaces of the cavity as you have described?
Well, the fact of it is that you can interpret it how you wish to interpret it. I can’t tell from that, as it is also difficult in the patent, the exact properties and I can’t compare one to the other. All I can say is they were referring to polyurethane foam in this and there is a polyurethane foam referred to in the patent, and the physical properties are we are surmising. And so, you can say yes or you can say no.
We know that the foam is sufficiently rigid to maintain its patency so that fluids are able to be sucked out?
I do not think it’s unreasonable but, again, there is just not a lot of information in either document because we are getting very particular about something that isn’t actually written.
I am accepting it’s not fully written. I am asking you, from your position as a skilled reader of this, whether you think it is reasonable to infer that the foam is not collapsing in on itself?
I think that’s reasonable.
551 Dr Pohl also accepted that it was reasonable to infer from Bagautdinov I that the mass of the foam would be pushing downwards on the wound.
552 Subsequently, when asked whether the porosity of the foam could be inferred from the description in Zamierowski, Dr Pohl stated: “[i]f we assume that all those polyurethane foams are the same then, yes, obviously you can infer one to the other but we actually do not know”. Dr Pohl was requested to put aside that assumption and to draw inferences simply from the properties described in Zamierowski. The following exchange, which included reference to Bagautdinov I, then occurred:
[I]t’s reasonable to infer, from your knowledge of how negative pressure works, that there will be areas where the foam meets the wound bed. That’s right, isn’t it?
Yes, yep.
And there will be two types of interface with the wound bed: some of them would be where a pore meets the wound bed, and some of them would be where the material meets the wound bed?
Correct, yes.
As you described with your hand with respect to Bag[autdinov], it’s reasonable to infer that there will be cells sucking up above the wound bed; do you agree?
Yes, yes.
There will be plastic material pushing down on the wound bed?
Yes.
Conclusion: screen rigidity and screen porosity integers in Bagautdinov I
553 I was not persuaded that the screen rigidity integer (if otherwise valid) could, although not expressed, be inferred from Bagautdinov I, which referred to polyurethane foam to act as a foam drain and to absorb pus from the purulent wounds. As KCI submitted, its infringement case did not depend on that inference but on the allegedly indistinguishable rigidity and the porosity of the S&N foam from the KCI foam. It contended that the foam must possess the structure and firmness necessarily to enable the even transmission of pressure onto the wound bed.
554 Further, I was not persuaded that Dr Pohl’s evidence in cross-examination constituted a concession that the Bagautdinov I foam disclosed the screen rigidity integer (assuming its validity) on the basis that it would perform like the KCI foam. While Dr Pohl apparently conceded that the material would “push down” on the wound bed and that the Bagautdinov I foam would “not collapse in on itself”, I was not satisfied that such characteristics sufficed to establish, nor constituted agreement to, the proposition that the foam was “sufficiently rigid to prevent wound overgrowth” in the sense contended by KCI.
555 Accordingly, I consider that Bagautdinov I did not disclose the essential screen rigidity integer. It follows that even if, contrary to my earlier finding, the screen rigidity integer has meaning as contended by KCI, Bagautdinov I does not anticipate the integer so as to deprive the Patent of novelty.
556 On the other hand, while Dr Pohl’s evidence on the question was somewhat elusive, on balance he appeared to concede that the Bagautdinov I foam would have the requisite porosity to enable gases to reach the wound. While it was unclear to me that the foam would remain porous throughout the Bagautdinov I treatment, which apparently retained purulent exudate in the foam for weighing after 24 hours, I conclude that the Bagautdinov I foam would possess the requisite porosity.
Other integers allegedly disclosed by Bagautdinov I
557 S&N submitted that the following were also disclosed by Bagautdinov I:
(a) a method… and an apparatus…,
(b) for treating wounds (in particular “purulent wounds”)…,
(c) using a vacuum pump…,
(d) with a screen (“drain”) of polyurethane foam…,
(e) adapted in shape or size [to the wound]…,
(f) placed on the surface or in the cavity…,
(g) sealed by a polyurethane film and Vaseline…,
(h) at a vacuum of 10 to 60 mm Hg…,
(i) with a tube connected to the pump…,
(j) used either intermittently… or continuously…, and
(k) that the method and apparatus worked highly successfully to clean and heal wounds….
558 KCI submitted that in addition to the different emphases, vague, language and lacunae in instructions, the evidence established that Bagautdinov I failed to disclose a number of integers, discussed below.
559 I have already found that Bagautdinov I did not disclose “a screen means for preventing overgrowth of tissue” or a screen means that is “sufficiently rigid to prevent wound overgrowth” (common to claims 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 49, 50, 52 and 121).
560 Nor in my opinion did Bagautdinov I disclose the essential integer of the application of “negative pressure… over an area sufficient to promote migration of epithelial and subcutaneous tissue toward the wound” common to claims 1, 2, 3, 6, 7, 8, 9, 10, 11 and 12. The evidence indicated that the shrinkage of wound area and volume in the treatment of Bagautdinov I occurred as swollen tissue reduced when pus was sucked from the wound, and as inflammation, an impediment to wound contraction, reduced. Inward movement of epithelial cells or subcutaneous tissue under the Bagautdinov I treatment was thus not due to vacuum assisted closure.
561 In my opinion, Bagautdinov I did not disclose the maintaining of negative pressure “for a time sufficient to facilitate closure of the wound” (common to claims 1, 2, 3, 6, 7, 8, 9, 10, 11 and 12). Bagautdinov I prescribed the application of suction for only short daily periods until the wound is “clean”, after which the drainage sessions are stopped. The Bagautdinov I technique was to clean wounds by draining unwanted pus and fluids away by using suction. It did not disclose an association between the application of the suction and granulation tissue formation or wound closure.
562 In my opinion, Bagautdinov I did not disclose the integer of maintaining of negative pressure “for a time sufficient to permit the formation of granulation tissue in the wound” (claim 2). Bagautdinov I does not mention granulation tissue and does not associate the application of suction to granulation tissue formation. Suction was applied to clean the wound and ceased when that was achieved, so if the formation of granulation tissue occurred during the Bagautdinov I treatment it would be incidental to the normal healing process (which may be impeded by the presence of exudate and infection), rather than the direct object of, and coterminous with, the application of negative pressure.
563 Bagautdinov I did not disclose the essential integer of negative pressure maintained “for at least 12 hours” (claim 6) or “for at least 3 days” (claim 7). Bagautdinov I describes the application of suction for only short daily periods of between 30 minutes and two hours.
564 In my opinion, Bagautdinov I did not disclose the essential integer of a single tubular member having a first end “inserted beneath at least a portion of the foam” (claim 50), or “embedded within the foam” (claim 52). There is no direction in Bagautdinov I as to where the tube is to be positioned relative to the foam drain.
565 Bagautdinov I did not disclose the integer of a vacuum means that is operated cyclically to provide “periods of application and non-application” of negative pressure or reduced pressure (claims 9, 10, 11, 12 and 121). Bagautdinov I describes the application of suction for only a short period each day until the wound is “clean”. By inference, the suction is not applied between the applications as the polyethylene sheet is removed and a gauze bandage is applied. The pressure as claimed is not disclosed. Nor is the application of alternate periods of negative pressure in uniform ratios in a regular “on/off” cycle as claimed.
566 In my opinion, Bagautdinov I did not disclose the essential integer of maintaining negative pressure “until the wound has progressed toward a selected stage of healing” (claim 121). As stated above, Bagautdinov I describes the application of suction for only a short period each day until the wound is clean. The suction is not maintained in the sense described in the Patent until the wound has progressed toward a selected stage of healing.
567 As S&N submitted, the English Court of Appeal upheld the finding of the trial judge that a related but distinct European patent was anticipated by Bagautdinov I. The European patent nevertheless related only to apparatus claims and not to claims of a method of treatment. It is also clear from the extracts referred to in the judgment of Warren LJ (with whom Jacob and Ward LLJ agreed) that a number of aspects of the specifications and the claims in relation to the apparatus were (despite some overlapping terminology and a strong general similarity) quite differently expressed.
568 Further, the question of novelty was assessed against different legislation and expert evidence on common general knowledge, the understandings of the patent and the meaning of Bagautdinov I.
569 The finding that the screen rigidity integer is meaningless rendered inevitable the failure of S&N’s challenged based on novelty. Any assessment of novelty, assuming its validity or its notional abstraction from the relevant claims, is therefore artificial.
570 Subject to that caveat, assuming, contrary to my finding, that the screen rigidity integer was valid, in my opinion, neither it nor a number of other essential integers of the claims was disclosed by Bagautdinov I. Further, as the authorities recognised, the disclosure must be “enabling” and communicated sufficiently to permit the skilled addressee (prior to the priority date) to understand and apply the invention. While some trial and error is permitted, the evidence, including Professor Penington’s testimony, established that Bagautdinov I was obscure in a number of respects and did not give clear and unmistakable directions to do what the patentee claimed.
571 S&N submitted that the Zamierowski patent (which had been acquired by KCI) anticipated the claims of the Patent.
572 S&N contended that Zamierowski disclosed a method and an apparatus for treating wounds using a vacuum source, including a pump, and a screen means consisting of an “intermediate layer of material”, which may include polyurethane foam and polyurethane mesh. It also disclosed a semi-permeable membrane seal, fluid drawn from the wound site, and a tube connected to a pump used continuously or intermittently. As with Bagautdinov I, S&N submitted that disclosure of the screen rigidity integer could, on KCI’s case, be inferred from the mere presence of foam.
573 S&N submitted that the following essential integers of claim 1 were therefore disclosed by Zamierowski:
(a) “method of treating tissue damage”;
(b) “screen means for preventing overgrowth”;
(c) “said screen means being sufficiently porous to allow gases to reach the wound and sufficiently rigid to prevent wound overgrowth”;
(d) “applying a negative pressure to said wound over an area sufficient to promote migration of epithelial and subcutaneous tissue toward the wound”; and
(e) “said negative pressure being maintained for a time sufficient to facilitate closure of the wound”.
574 In relation to the screen porosity and screen rigidity integers, S&N again submitted that, as with Bagautdinov I, they could be inferred from the mere presence of foam, consistently with KCI’s case on infringement. S&N noted in this context that claims 49, 50 and 52 of the Patent required that the screen means be “an open cell polymer foam suction”. It submitted that Dr Pohl agreed that Zamierowski’s foam must be open-cell. Further, there were no likely materials other than foam as at the priority date for the intermediate layer, as the evidence was that doctors would not use hydrocolloids, and foam was also readily available.
575 S&N contended that Zamierowski referred to the intermediate layer as being “primarily located” in the chamber between wound and screen, as it is in claims 1 and 121. The wound would heal in the natural way referred to in the claims. Zamierowski disclosed the screen means, the cover (ie seal) and the tube (claim 50). Zamierowski disclosed the use of the screen means, application of reduced pressure and maintenance of the pressure towards a selected stage of healing, including alternating periods of application and non application (claim 121).
576 S&N’s allegations of disclosure of integers of the dependent claims were set out in a schedule to its written submissions.
577 S&N submitted that the thrust of Zamierowski was not the introduction of fluids, but rather, an equipoise between the introduction and evacuation of fluids. Further, there was a sufficiently clear disclosure of the intermediate layer. The claims in the Patent comprehended infected wounds, at which Zamierowski was directed. Although the “intermediate layer” in the diagram in Zamierowski appeared to extend past the wound site, when sucked, it would be pressed down.
578 S&N submitted, in reliance on Bitech Engineering v Garth Living Pty Ltd (2010) 86 IPR 468, that the mere addition of an element would not avoid infringement if all the essential integers in the claim were taken.
579 KCI submitted that Zamierowski was expressly directed at solving problems associated with semi-permeable dressings, rather than those of the Patent. Further, its purpose was a wound dressing which promoted the introduction of medical fluids that prevented or treated infection (or fluids that might promote healing), and also the evacuation of drained fluids.
580 Zamierowski did not, in KCI’s submission, describe the creation and maintenance of negative pressure to actively promote wound closure. It did not say anything about the migration of epithelial cells, the formation of granulation tissue or the rigidity of the wound dressing, nor disclose the cyclical application of negative pressure.
581 KCI submitted that Zamierowski did not disclose:
(a) “a screen means for preventing overgrowth of tissue” or a screen means that is “sufficiently rigid to prevent wound overgrowth” (claims 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 49, 50, 52, and 121);
(b) the application of “negative pressure… over an area sufficient to promote migration of epithelial and subcutaneous tissue toward the wound” (claims 1, 2, 3, 6, 7, 8, 9, 10, 11 and 12);
(c) the application of negative pressure “for a time sufficient to facilitate closure of the wound” (claims 1, 2, 3, 6, 7, 8, 9, 10, 11 and 12);
(d) the application of negative pressure “for a time sufficient to permit the formation of granulation tissue in the wound” (claim 2);
(e) a single tubular member having a first end “inserted beneath at least a portion of the foam” (claim 50), or “embedded within the foam” (claim 52);
(f) a vacuum means that is operated cyclically to provide “periods of application and non-application” of negative pressure or reduced pressure (claims 9, 10, 11, 12 and 121); and
(g) “placing a screen means for preventing overgrowth of tissue in a wound” (claims 1, 2, 3, 6, 7, 8, 9, 10, 11, 12 and 121).
Expert evidence
582 Professor Stacey, having described the two treatment methods in Zamierowski for the delivery and drainage of fluids to and from wounds which could be used either separately or in combination, discussed the background and the objectives of the paper, which included maintaining a moist wound environment. He deposed that as at 1991 (or now) there was no single dressing capable of maintaining appropriate moisture in a wound with high levels of exudate without frequent dressing changes. Professor Stacey described the Zamierowski apparatus and possible dressings for which one suggestion was a polyurethane foam, so that in Professor Stacey’s view, Zamierowski taught “the use of an open cell polyurethane foam”, as it referred to a dressing with a “wicking or capillary action”.
583 Professor Stacey, in 1991, on reading Zamierowski, would have used foam to treat a deeper or heavily draining wound, wounds which need improved distribution of suction pressure on their surfaces and, perhaps, over skin grafts.
584 Professor Stacey noted that Zamierowski allowed for both passive and active drainage, and he would have been more inclined to use active drainage for a heavily draining wound.
585 Although Zamierowski gave no direction as to strength of the suction, Professor Stacey would have used the 50-100mmHg pressures he had used on wall suction systems.
586 Zamierowski described a period of at least two days’ treatment for skin grafts and for other draining wounds, but Professor Stacey would have used the treatment until there was no further need to drain.
587 Professor Stacey deposed:
I think the system described in the Zamierowski Patent is very similar to the method described in the Patent and the apparatus in Figure 1 because both:
(a) are a treatment method for open wounds and skin grafts;
(b) recommend a range of dressings, including open cell foam;
(c) use an adhesive cover over the wound;
(d) use suction or negative pressure and create the sealed environment for the negative pressure by using an adhesive seal over the wound and on the skin immediately surrounding the wound;
(e) both claim to aid in the removal of toxins and bacteria;
(f) both drain fluid from the wound via tubing inserted under the adhesive seal with the aid of negative pressure or suction; and
(g) both claim to promote healing.
588 Professor Stacey deposed that if he assumed that:
(a) the prevention of overgrowth of tissue;
(b) the formation of granulation tissue;
(c) a reduction in bacteria by half or by 1,000 fold; and
(d) the facilitation of closure of the wound,
were achieved by the application of the method described in the Patent, then he would also expect to see them if he applied the method described in the Zamierowski patent, as the Zamierowski patent claimed to promote healing (which included promoting granulation tissue growth and epithelial migration and proliferation and facilitating wound closure). It also taught that the removal of toxins and bacteria was an important aspect of the fluid drainage phase of the healing process, and that its system removed serum and secretions and minimised the risk of infection.
589 Professor Stacey deposed that, contrary to Dr Pohl’s view, the Zamierowski patent included a screen means “being an open-cell foam configured to overlie the wound” (claims 50, 52, 104, 109, 110 and 112) by referring to the need for a dressing with a wicking or capillary action, which would include a polyurethane foam. Without foam it would be extremely difficult to draw the fluid from the wound and through the intermediate layer or dressing with the use of suction in accordance with a primary goal of the Zamierowski system (namely to promote healing by draining unwanted fluids from the wound), so it was obvious that an open-cell foam would be required.
590 While the Zamierowski patent did not refer to the migration of epithelial and subcutaneous tissue, in Professor Stacey’s view it included the integer of the application of “negative pressure... over an area sufficient to promote migration of epithelial and subcutaneous tissue toward the wound” (claims 1, 2 and 3), as those processes occur naturally in a healing wound and promoting healing was an objective of the treatment described in the Zamierowski patent.
591 As the Zamierowski patent directed the reader to use the treatment method for a time period “necessary to achieve the treatment objectives”, Professor Stacey considered that it included the integer of the application of negative pressure “for a time sufficient to facilitate closure of the wound” (claims 1 and 3). He stated that “[a]s the wound heals, progressively smaller amounts of fluid will ooze therefrom and the frequency and duration of the drainage operations can be correspondingly reduced and finally discontinued altogether”. It also directed the reader to use the method until the wound has healed to the desired point, which, in Professor Stacey’s view, was the same as “for a time sufficient to facilitate closure of the wound”.
592 The Zamierowski patent did not explicitly refer to use for a time sufficient to permit formation of granulation tissue (claim 2), but Professor Stacey stated that granulation tissue growth occurs naturally in a healing wound and healing of wounds was one of the objects of the Zamierowski patent.
593 Professor Stacey deposed as follows in relation to other claims of the Patent:
(i) a “cover adapted to form a seal with the skin surrounding the wound for maintaining a negative pressure beneath” the cover (Claims 50, 52, 104, 109, 110 and 112). I disagree with Mr Pohl and consider the adhesive membranes described in the Zamierowski patent at column 3, lines 53-56), particularly the Tegaderm (or “Tagoderm” as he calls it) with which I am familiar, are consistent with the seals disclosed in the Patent, in that all are capable of maintaining a negative pressure beneath the cover with the application of negative pressure or suction to the wound;
(j) a "sealing means for maintaining negative pressure on [the] wound by contacting the skin surrounding the wound" (Claims 62 and 89). I refer to and repeat my comments at subparagraph 22(i) above;
(k) a single tubular member having a first end "inserted beneath at least a portion of the foam" (Claims 50, 104 and 110), or "embedded within the foam" (Claims 52, 109 and 112). Figure 10 in the Zamierowski patent provides a helpful representation of the vacuum suction or negative pressure treatment system described in the Zamierowski patent. The representation appears to require that the perforations in the tube be placed facing away from the adhesive membrane so that the adhesive membrane does not adhere to the perforations and impede the suction efficiency of the system;
(l) a vacuum means that is operated cyclically to provide "periods of application and non-application" of suction or reduced pressure (Claims 62 and 121). I understand the directions at column 6, lines 4-18 of the Zamierowski patent to require that the suction drainage method be used for the period of time required and either continuously or intermittently, again as required;
(m) a vacuum source supplying "negative pressure between about 1.01 and 100.3 kPa". I am informed by Blake Dawson that the range equates to 7 - 752mmHg. It would be almost impossible for the Zamierowski patent not to apply suction in the range of 7 - 752mmHg for the active suction method described in the Zamierowski patent. If I had read the Zamierowski patent in November 1991 1 would have used suction in the range of 50-100mmHg for the reasons I have stated at paragraphs 103-4 of my First Affidavit and I would have expected that Dr Zamierowski would have used a similar pressure range.
If I had read the Zamierowski patent in November 1991 I would have regarded it as relevant to the treatment of a range of wounds including bums, open lacerations, abrasions and ulcers of various types, including pressure sores (decubitus ulcers) (as described at column 3, lines 20-23) and skin graft donor sites (column 3, line 37), as well as the wounds referred to at paragraphs 18(e) and 24 above. I would have used the method described in the Zamierowski patent.
594 In cross-examination, Professor Stacey agreed that all of the components of the device were equally suitable for passive or active drainage, but the evacuation mode was preferred if a dressing were used.
595 Professor Stacey agreed that the “intermediate material layer” was shown in a diagram extending outside the margins of the wound, indicating that it was not included within the margins of the wound. In re-examination, Professor Stacey stated that he took the intermediate material layer to be mainly placed over the surface of the wound. Of the three types of recommended material, Professor Stacey agreed that the invention just referred to polyurethane foam or mesh without any further discussion or description. He agreed that claims 1, 2, 3 and 4 of the patent did not refer to an intermediate material layer; claim 5 referred to it but did not describe it; claim 6A referred to it as “could be a hydrocolloid”; claim 7A referred to it as “could be non-absorbent”; and claim 9 referred to it as “could include a hydrocolloid” and a “non-absorbent fabric sheet”, but no claims referred to polyurethane foam or foam at all.
596 Professor Stacey acknowledged that no particular type of suction device, nor the way of applying it, was referred to in the specification.
597 In the Zamierowski patent, the tube was depicted on top of the wound cavity rather than the wound bed, but Professor Stacey thought it would reach the wound bed when sufficient fluid was removed. The tube was not depicted as embedded.
598 Professor Stacey agreed that he would know what pressure to use from his experience and would expect that the fluid sitting on the wound surface would then pass through the dressing.
599 Professor Penington also discussed Zamierowski and described how he would have used the method it described as follows:
The treatment method at column 5, line 34 proposes that the method be applied for 48 hours in evacuation mode at a skin graft donor site. If I had applied this method before November 1991 I would have applied the treatment for 48 hours as suggested and then examined the wound. I would have trialled different treatment times and applied the treatment for whatever time seemed appropriate for the wound I was treating and my treatment objectives for the wound.
The second and third forms of the wound dressing are described at columns 7 and 8 of the patent. The methods for using the wound dressings are the same as for the first form of dressing. The second form of the dressing shown in Figure 8 includes a primary wound cover that is placed underneath another cover. The third form of the dressing shown in Figures 9 and 10 and described a [sic] column 7 line 43 to column 8 line 27, incorporates a cover membrane, an intermediate layer of material (dressing), which is then connected to a tube and active or passive drainage can then occur.
600 Professor Penington noted that various materials were described for the intermediate layer, including hydrophilic colloids, a mesh or sheet of synthetic material such as rayon or Envinet mesh, or polyurethane foam or polyurethane mesh. Had he read the patent before November 1991 and wished to make the third form of the dressing it described, he would have used polyurethane foam for the intermediate layer because it would have been the only one of the materials available which he considered suitable. He would not have used a hydrophilic colloid but an open-cell polyurethane foam, because the method requires the intermediate layer to remove fluid from the wound by wicking or capillary action.
601 Professor Penington deposed that because the third type of wound dressing described in this patent was similar to Figure 1 of the Patent in that it has an open-cell screen (dressing), a flexible hose connecting the screen to a suction source and a flexible polymer sheet overlying the foam, if treatment with the device described and shown in Figure 1 of the Patent were shown to prevent wound overgrowth, or to be capable of doing so, then he would expect the treatment technique described in Zamierowski using the third type of wound dressing to do so too. Professor Penington was, however, sceptical of prevention of wound overgrowth, adding “whatever that means”.
602 Professor Penington would have expected that the treatment described in Zamierowski would facilitate closure of the wound. He also considered that the reference to promoting healing suggested that the treatment time would be sufficient for granulation tissue to be forming in the wound. The treatment time described in the patent was 48 hours, and before November 1991 he would have expected to see granulation tissue starting to appear in the wound by the end of that time period.
603 Dr Pohl discussed Zamierowski as follows:
In column 8 on page 7, "polyurethane foam" is stated to be a material which can be used for the intermediate material layer. I would have inferred that the foam would be used for its liquid absorbent properties.
604 Dr Pohl deposed that Zamierowski would not have disclosed a large number of integers of the claims in suit.
605 As to “a screen means for preventing overgrowth of tissue” or a screen means that is “sufficiently rigid to prevent wound overgrowth”, Dr Pohl observed that although Zamierowski described a wound dressing with an “intermediate material layer”, it did not say anything about tissue overgrowth or whether the intermediate material layer had any particular rigidity.
606 As to a screen means that is “sufficiently porous to allow gases to reach the wound” or “sufficiently porous to allow gases to reach the burn”, Dr Pohl observed that Zamierowski did not mention porosity and did not describe a relationship between the intermediate material layer and gases.
607 As to a screen means “being an open-cell foam configured to overlie the wound”, Dr Pohl observed that Zamierowski stated that the intermediate material layer could be polyurethane foam but did not state whether the foam is open-celled.
608 As to the application of “negative pressure... over an area sufficient to promote migration of epithelial and subcutaneous tissue toward the wound”, Dr Pohl noted that Zamierowski did not mention the migration of epithelial cells or contraction of subcutaneous tissue.
609 As to the application of negative pressure “for a time sufficient to facilitate closure of the wound”, Dr Pohl noted that Zamierowski disclosed a wound dressing, which was to drain wounds and to introduce medical fluids. Zamierowski described an “evacuation mode of operation” whereby suction could be applied for “forty-eight hours or so after removal of a split-thickness skin graft at a donor site”. The document did not otherwise describe the length of time that the suction is applied for and did not say anything about the device facilitating granulation tissue formation or wound closure.
610 As to the application of negative pressure “for a time sufficient to permit the formation of granulation tissue in the wound”, Dr Pohl observed that Zamierowski did not mention granulation tissue or an association between the length of time that the suction is applied for and granulation tissue formation.
611 As to a “cover adapted to form a seal with the skin surrounding the wound for maintaining a negative pressure beneath” the cover, Dr Pohl observed that Zamierowski disclosed a semi-permeable membrane which forms a “relatively liquid-tight adhesive bond” with the skin around the wound, but Dr Pohl would not have understood it to be a seal of the kind claimed in the Patent.
612 As to a single tubular member having a first end “inserted beneath at least a portion of the foam” or “embedded within the foam”, Dr Pohl observed that Zamierowski disclosed a tube which is inserted through a seam in the semi-permeable membrane, but did not disclose the insertion or embedment of the tube within the intermediate layer.
613 As to a vacuum means that is operated cyclically to provide “periods of application and non-application” of suction or reduced pressure, Dr Pohl observed that Zamierowski disclosed the alternating introduction of a liquid and drainage of a wound. Dr Pohl would not have considered that to be the same as the uniform ratios or regular on/off cyclical application of negative pressure claimed in the Patent.
614 Dr Pohl deposed that if he had read Zamierowski in 1991, he would not have regarded it as relevant to solving the problem of chronic open wounds described in the Patent, because it described a wound dressing designed to overcome specific problems associated with semi-permeable dressings, which was a different problem from that of chronic open wounds.
615 After reading Zamierowski in 1991, Dr Pohl would not have been directly led as a matter of routine to try the solutions claimed in the Patent. Many of the features of the claims of the Patent were not disclosed in Zamierowski. The treatment in Zamierowski associated wound healing with passing “liquid medications” through a dressing, which was very different to the method of treatment described in the Patent, which relates wound healing to the application of negative pressure.
616 Zamierowski was specifically directed to overcoming deficiences with semi-permeable dressings revealed by prior art which tended to retain fluid and did not accommodate the introduction of liquid medications, rather than the problems the Patent identified. The invention was a wound dressing which allowed the introduction of medicinal or antibiotic fluids to the wound and the evacuation of drained fluids, by which means healing was promoted. Its operation in evacuation mode continued only until undesirable fluids were present, and negative pressure was not applied to promote wound closure per se.
617 While Zamierowski’s second modified embodiment called for an intermediate layer of material to be included in the wound dressing to draw fluid from the wound, its primary suggestion was for hydrocolloid material, which was discussed in detail. The observation that polyurethane foam or mesh could be used was not amplified or further explained and it was not specified that such material could be used with a suction device. Zamierowski did not in my view clearly direct the use of an open-cell foam. Thus, Zamierowski did not, expressly or inherently, disclose “a screen means for preventing overgrowth of tissue” or a screen means that is “sufficiently rigid to prevent wound overgrowth” or sufficiently porous to allow gases to reach the wound (claims 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 49, 50, 52, and 121). Zamierowski described a wound dressing with an “intermediate material layer” but it did not say anything about tissue overgrowth or whether the intermediate material layer has a particular rigidity or porosity. I have discussed Dr Pohl’s evidence on this question above.
618 Similarly, Zamierowski did not disclose wound contraction or the migration of epithelial cells or contraction of subcutaneous tissue (claims 1, 2, 3, 6, 7, 8, 9, 10, 11 and 12).
619 Although Zamierowski described an “evacuation mode of operation” where suction may be applied for “forty-eight hours or so after removal of a split-thickness skin graft at a donor site”, it did not state the length of time for the application of suction, and evacuation mode was operated only until unwanted fluids were drained. Further, when used in active drainage mode, Zamierowski is for draining excess fluid from the wound. It thereby facilitates healing only in a generalised sense, rather than the specific sense of facilitating granulation tissue formation and wound closure directed by the Patent. It therefore did not disclose the application of negative pressure “for a time sufficient to facilitate closure of the wound” (claims 1, 2, 3, 6, 7, 8, 9, 10, 11 and 12).
620 Zamierowski did not refer to formation of granulation tissue or, perforce, any association between it and the time for which suction is applied. It therefore did not disclose the application of negative pressure “for a time sufficient to permit the formation of granulation tissue in the wound” (claim 2).
621 Zamierowski disclosed a tube which was to be inserted through a seam in the semi-permeable membrane. As Professor Stacey stated, it sat on top of the intermediate layer and had an opening facing down towards the wound surface. Zamierowski did not disclose the insertion or embedding of the tube within the intermediate layer, and therefore did not disclose claims 49, 50 or 52.
622 Zamierowski did not disclose cyclical application of negative pressure as described in the Patent, and therefore did not disclose a vacuum means operated cyclically to provide “periods of application and non-application” of negative pressure or reduced pressure (claims 9, 10, 11, 12 and 121).
623 Professor Stacey conceded that no intermediate layer was depicted in some of the figures in the paper, and where it was depicted in some of the figures, it extended beyond the wound site to the surrounding healthy skin. Zamierowski therefore did not disclose “placing a screen means for preventing overgrowth of tissue in a wound” (claims 1, 2, 3, 6, 7, 8, 9, 10, 11, 12 and 121). Further, the skilled addressee would have to use the variables of active drainage, the intermediate layer dressing option and the foam for the material together in order to perform the invention in the Patent.
624 Therefore, in my opinion, Zamierowski did not give enabling “clear and unmistakeable directions” to do what the patentee claims.
625 S&N submitted that each of the method (non-foam) claims in suit was anticipated by Chariker and Jeter (read separately) as well as Chariker and Jeter (treated together as a single source of information). (It did not allege that the apparatus claims were anticipated by Chariker and Jeter, as the apparatus claims specified foam).
626 Chariker describes a closed suction wound drainage system, consisting of a method and apparatus which collects drainage from wound sites; obviates skin damage; improves wound granulation and contraction; facilitates and contributes to closure and healing; treats tissue drainage and damaged tissue; and minimises dressing/nursing requirements and reduces costs. S&N submitted that Chariker discloses the use of a porous screen; laying down a gauze screen across the wound bed; laying a tube on top of the gauze; fluffing the gauze into the wound; sealing the wound with skin sealant and adhesive film dressing; connecting the tube to a suction source at a vacuum of 60-80 mHg; and taught that the treatment lessens the degree of fibroplasia and hence hypergranulation. While Chariker concerned the treatment of fistulae, S&N submitted that the witnesses agreed a fistula is a type of wound.
627 S&N submitted that Jeter disclosed a system almost identical to that described in Chariker, and that Jeter specifically refers to using the technique in relation to draining wounds as well as fistulae. Jeter further contemplated the use of foam and intermittent suction.
628 KCI submitted that Chariker described a system to drain fistulae, rather than the use of negative pressure for the active promotion of wound healing in the manner of the Patent. It described a method of continuous removal of effluent from the wound bed, which decreased the inflammatory phase of wound healing and prevented the formation of eschar (scab) and fibroplasia.
629 KCI described Jeter’s purpose as the continuous evacuation of effluent from the wound bed. The paper was, in KCI’s submission, directed to creating conditions in which the fistulae can heal by draining effluent, and was not concerned with the creation and maintenance of negative pressure to actively facilitate healing.
Submissions as to claims in suit
630 KCI submitted that neither paper disclosed a screen means “for preventing overgrowth” or a screen means “sufficiently rigid to prevent wound overgrowth”. Chariker disclosed the use of moist gauze and Jeter disclosed gauze, but neither drew a link between the gauze and the prevention of tissue overgrowth. S&N, while primarily submitting that the screen did not (in fact) operate to prevent overgrowth, contended that, if KCI’s case were correct, the integers “for preventing overgrowth” and the screen rigidity integer were inherently disclosed by the use of gauze. It was thus unnecessary for Chariker or Jeter expressly to refer to them.
631 KCI submitted that neither paper disclosed a screen means “sufficiently porous to allow gases to reach the wound”. Neither paper said anything about the porosity of the gauze, and Dr Pohl’s evidence was that moist gauze saturated with fistula effluent would not possess the requisite porosity to enable negative pressure to be exerted on the wound bed in the way described in the Patent. S&N submitted that on KCI’s case, that integer was inherent in the provision of foam and gauze. It contended that on the evidence, gauze was suitable for use in NPWT, but in any event, (in reliance on the evidence of Professors Penington and Stacey and Dr Pohl), in applying Chariker and Jeter, foam may have been selected instead of gauze.
632 KCI submitted that neither paper disclosed a screen means “being an open cell foam configured to overlie the wound” or a tubular member having a first end “inserted beneath at least a portion of the foam” or “embedded within the foam”, because they did not disclose the use of foam. Indeed, Chariker expressly stated that the use of moist gauze was “critical to the efficacy of our system” and Jeter explicitly referred to the virtues of gauze. As stated above, S&N submitted that in applying Chariker and Jeter, foam may have been selected instead of gauze.
633 KCI submitted that Chariker did not disclose a method of treating tissue damage “where the wound is a pressure sore”, because it discussed fistulae. S&N submitted that the integer followed from any disclosure of wounds generally.
634 KCI contended that neither paper disclosed negative pressure maintained “for at least 3 days”, because, as revealed in the evidence of Dr Pohl and Professor Marshall, moist gauze would not permit negative pressure to be exerted on the wound bed for any length of time in excess of around 12 hours. S&N, relying on the evidence of Professors Penington and Stacey and Dr Pohl, submitted that both Chariker and Jeter disclosed continuous treatment for at least three to five days.
635 Finally, KCI submitted that neither paper disclosed cyclic periods of application and non-application of negative pressure, because they disclosed continuous suction. S&N submitted that the integer was inessential, but contended that Jeter, in any event, disclosed that intermittent suction is available (albeit that the author preferred continuous suction).
Conclusion on Chariker and Jeter
636 I was satisfied, as KCI submitted, that Chariker and Jeter (whether read individually or together) did not give “clear and unmistakeable directions” to do what the patentee claims.
637 For similar reasons to those expressed in relation to Bagautdinov I and Zamierowski, I was not persuaded that the screen rigidity integer or the screen porosity integer could be inferred from Chariker and Jeter as an inherent property of the gauze. While it is therefore unnecessary to consider the remaining claims, in my opinion, a number of other integers were not disclosed by Chariker and Jeter with sufficient accuracy to anticipate the claims.
638 The evidence of Dr Williams, Mr Ellis and Mr Osmond (among others) regarding the use of drainage and negative pressure as at 1991 has been set out above at [117] to [155]. S&N relied on Dr Williams’ and Mr Osmond’s evidence both in relation to common general knowledge and to demonstrate “prior use” depriving the Patent of novelty.
639 As set out in detail above, Dr Williams deposed that an “open drainage system” for fistulae and moderately to heavily draining wounds was used as early as the 1970s, which incorporated a tube, a porous dressing, a cover, an adhesive, and a source of vacuum suction. He deposed that:
The system was applied to a heavily draining wound by packing the wound with the porous dressing. The perforated end of the tube was then laid across the wound bed, on top of the dressing. A portion of the skin surrounding the wound was covered with an adhesive, such as Stomahesive. The plastic cover was attached to the Stomahesive to form a sealed area around the wound. The tube came out through the plastic cover in such a way as to maintain the seal over the wound. The tube was then attached to a suction device and the fluid was sucked out of the wound into a canister.
640 Dr Williams stated that active suction was used regularly in heavily draining wounds prior to November 1991, and that negative pressure wound dressings in use today utilise the same principles and features as the system he described. He further deposed that the purpose of the open drainage system was to remove harmful fluids from the wound, thereby preventing those fluids from impeding the normal wound healing process, including the growth of granulation tissue and the contraction of the wound.
641 Mr Osmond deposed, inter alia, to his observation of active suction being used for drainage of closed wounds prior to 1991.
642 Mr Ellis stated that as at November 1991 he had never heard of negative pressure or suction being applied to an open wound. Further, he stated that drainage, while a well-understood technique at the time, was not known as having a therapeutic effect above and beyond the straightforward removal of fluid. During the trial, Mr Ellis accepted that active suction methods were “obviously… going on somewhere because plenty of other people do remember seeing them”.
643 S&N submitted that the evidence of Dr Williams and Mr Osmond revealed prior use of the essential elements of KCI’s V.A.C.® device, namely a seal, a tube, a dressing (admittedly gauze) and a pump. It submitted that while Mr Ellis had not seen or used negative pressure on open wounds, his evidence was necessarily based on his own limited personal knowledge and experience.
644 KCI submitted, and I accept, that the prior use of Dr Williams did not disclose a number of integers of the claims in suit, namely:
(a) “a screen means for preventing overgrowth of tissue” or a screen means “sufficiently rigid to prevent wound overgrowth”. Dr Williams used gauze dressings to absorb fluid and there was no evidence that a compressive downward force was exerted on the gauze at all;
(b) a screen means “being an open cell foam configured to overlie the wound”, and a single tubular member having a first end “inserted beneath at least a portion of the foam” or “embedded within the foam”. Dr Williams’ prior use did not disclose foam;
(c) the application of negative pressure “for a time sufficient to facilitate closure of the wound”. Dr Williams left the drainage system in place only for as long as was required to remove effluent;
(d) the application of negative pressure “over an area sufficient to promote migration of epithelial and subcutaneous tissue toward the wound”. There was no evidence that Dr Williams’ system caused wound contraction; and
(e) a vacuum means operated cyclically to provide “periods of application and non-application” of negative pressure or reduced pressure. There was no disclosure in Dr Williams’ system of periods of application and non-application of negative pressure.
645 An essential integer common to all combination claims, and integers present in a number of individual claims, were thus not disclosed by Dr Williams’ prior use.
646 S&N submitted that if the invention were not invalid for want of novelty by reason of prior disclosure, the claims should nevertheless be revoked because the invention did not involve an inventive step and would have been obvious to the skilled addressee in the light of common general knowledge together with the further information permitted by the Act.
647 S&N submitted that in addition to common general knowledge (discussed above), the information in the prior art documents, Johnson I and Johnson II (as they satisfied the criteria in s 7(3)), would be available to the skilled addressee, to whom the invention consequently would have been obvious. Alternatively, S&N advocated an avowedly novel construction of s 7(2), which would permit the skilled addressee access to any one of the prior art documents as a starting point in assessing whether there were an inventive step.
648 KCI denied that the invention would have been obvious. In that context, it denied that the criteria rendering Johnson I and Johnson II available to the skilled addressee pursuant to s 7(3) were satisfied and challenged S&N’s novel construction of s 7(2) (asserting that the provision did not depart from previous law in the radical way asserted).
649 I have found, as discussed below, that the claims are invalid for lack of clarity due to the purported screen rigidity integer, but discuss the question of an inventive step for completeness.
650 Section 18(1) of the Act relevantly provides:
Subject to subsection (2), a patentable invention is an invention that, so far as claimed in any claim:
…
(b) when compared with the prior art base as it existed before the priority date of that claim:
…
(ii) involves an inventive step…
651 As set out in KCI’s submissions, section 7 of the Act relevantly provides:
(2) For the purposes of this Act, an invention is to be taken to involve an inventive step when compared with the prior art base unless the invention would have been obvious to a person skilled in the relevant art in the light of the common general knowledge as it existed in the patent area before the priority date of the relevant claim, whether that knowledge is considered separately or together with the information mentioned in subsection (3).
(3) The information for the purposes of subsection (2) is:
(a) any single piece of prior art information; or
(b) a combination of any 2 or more pieces of prior art information;
being information that the skilled person mentioned in subsection (2) could, before the priority date of the relevant claim, be reasonably expected to have ascertained, understood, regarded as relevant and, in the case of information mentioned in paragraph (b), combined as mentioned in that paragraph.
652 The applicable definition of “prior art base” in Schedule 1 to the Act is extracted at [477].
653 Obviousness under the Act is assessed against different prior art from that relevant to novelty.
654 By s 7(2) of the Act, an inventive step will be inferred unless the invention would have been “obvious” to a person skilled in the relevant art in the light of the common general knowledge as it existed in Australia before the priority date of the relevant claim, whether considered separately or together with any information available under s 7(3) of the Act. In Pfizer Overseas Pharmaceuticals & Ors v Eli Lilly and Co & Ors (2005) 68 IPR 1, the Full Court stated at 59:
Section 7(2) has the effect that a claimed invention lacks an inventive step compared with the prior art base only if “the invention would have been obvious to a person skilled in the relevant art in the light of the common general knowledge as it existed in the patent area before the priority date of the relevant claim”.
(emphasis added)
655 Section 7(2) implicitly imposes the onus of disproving an inventive step on S&N in this case, as the provision, by its language, “indicate[s] that the onus to establish the absence of an inventive step rests upon the party challenging validity”: Firebelt Pty Ltd v Brambles Australia Ltd (t/as Cleanaway) & Ors (2002) 54 IPR 449 (“Firebelt”) at 457.
656 It has been held that the term “obvious” means “very plain”: Aktiebolaget HÄssle & Anor v Alphapharm Pty Ltd (2002) 212 CLR 411 (“Aktiebolaget”) at 427. Merely because it was obvious to try something within the scope of the claims would not render the invention obvious. Rather, the skilled person must have been “directly led as a matter of course to try” the invention as claimed “in the expectation” that it might well work: Aktiebolaget at 433. In Alphapharm, Lindgren J observed at 661 that in the context of obviousness, the High Court “insisted on the two elements: (1) being led as a matter of routine to the desired result; and (2) having a reasonable expectation of achieving that result”.
657 The inventive ingenuity required is not extensive. It need be only “a scintilla of inventiveness” and “no smallness or simplicity will prevent a patent being good”: Meyers Taylor at 249.
658 As the entire invention as claimed in each claim must be considered for the purposes of an inventive step (s 18(1)), if the invention is a combination of integers, the question is whether the combination as a whole, rather than a selection of one or some of the integers, is obvious. In Aktiebolaget, the High Court stated at 429 that “the selection of the integers out of “perhaps many possibilities”… must be shown… to be obvious, bearing in mind that the selection of the integers in which the invention lies can be expected to be a process necessarily involving rejection of other possible integers”.
659 The High Court, in Lockwood (No 2) at 198, endorsed the recognition by Fletcher Moulton (in The Present Law and Practice Relating to Letters Patent for Inventions, Butterworths, 1913, p 24) that:
An invention may, and usually does, involve three processes. Firstly, the definition of the problem to be solved or the difficulties to be overcome; secondly, the choice of the general principle to be applied in solving this problem or overcoming these difficulties; and thirdly, the choice of the particular means used. Merit in any one of these stages, or in the whole combined, may support the invention.
660 The assessment of obviousness under the Act departs from the position that applied under the previous legislation, under which lack of inventive step was to be assessed by reference to common general knowledge, without reference to further available documents and acts.
661 Section 100(1)(e) of the Patents Act 1952 (Cth) (“the 1952 Act”) provided for revocation of a claimed invention if it “was obvious and did not involve an inventive step, having regard to what was known or used in Australia on or before the priority date of that claim”. As Aickin J indicated in Minnesota Mining at 292, the term “known or used” is a reference to common general knowledge in Australia: see Lockwood (No 2) at 196-197.
662 The meaning of the phrase “common general knowledge” is discussed at [94] to [99] of these reasons.
663 The provisions in the present Act dealing with an inventive step were introduced following the recommendation of the Industrial Property Advisory Committee (“IPAC”) (Patents, Innovation and Competition in Australia, Advisory Council on Intellectual Property, 1984) to raise the level of invention required to support a standard patent as follows:
treat[ing] as within the common general knowledge of the art, not merely information which is generally known and used in the art, but also information which is publicly available in recorded form anywhere in the world which a skilled person working in the art at the relevant time should reasonably have been expected to find, understand, and regard as relevant.
664 The IPAC recommendation was to broaden the notion of common general knowledge by the specific inclusion of a limited class of defined publications. There was no recommendation that the test under the 1952 Act should be altered in any other respect.
665 The IPAC recommendation was implemented by the introduction of ss 7(2) and (3) of the present Act which initially restricted the publicly available information to locally available documents and acts. An amendment in 2001, however, permitted foreign documents and acts to be taken into account.
666 The High Court in Firebelt stated at 458:
… it is apparent that there has been an expansion of the legislative text dealing with the ascertainment and content of the common general knowledge relevant for the determination of the obviousness of a claim, whether it be to a combination or otherwise.
667 In Lockwood (No 2) the High Court confirmed at 222 that s 7(3) now permitted the use of prior disclosures other than the common general knowledge at the priority date. It stated at 194:
Previously, only common general knowledge was taken into account when assessing an inventive step. Now, additional information which was publicly available as at the priority date must also be taken into account. Broadly speaking, s 7(3) has as its purpose the specification of the additional publicly available information (s 7(3) information) which must be added to common general knowledge for the purposes of deciding whether an alleged invention is obvious when compared with the prior art base.
668 In Aktiebolaget and Lockwood (No 2), the High Court also recognised that the Australian and UK approaches to obviousness had increasingly diverged. In Aktiebolaget, it stated at 431 and 432:
The divergence in the case law marked by Minnesota Mining has since been widened by changes in statute law…
…
The result in Britain of the shift in grundnorm is exemplified in the observation by Laddie J that the skilled worker (identified in s 3 of the 1977 UK Act): “is assumed to have read and understood all the available prior art.” The treatment of the point by Aickin J in Minnesota Mining, as indicated above, expressly rejected any assumption as to what in such a way may be expected of and attributed to the hypothetical addressee.
(emphasis added in original)
669 In Lockwood (No 2) the High Court stated at 222 and 223:
Given the history, context, purpose and specific words of limitation in s 7(3), all of which were addressed by this Court in Firebelt, the phrase “relevant to work in the relevant art” should not be construed as meaning relevant to any work in the relevant art, including work irrelevant to the particular problem or long-felt want or need, in respect of which the invention constitutes an advance in the art. The phrase can only be construed as being directed to prior disclosures; that is, publicly available information (not part of common general knowledge) which a person skilled in the relevant art could be expected to have regarded as relevant to solving a particular problem or meeting a long-felt want or need as the patentee claims to have done. Otherwise the words of limitation in the last forty words of s 7(3) would have no role to play. Any piece of public information in the relevant art would be included, as is the case with the much broader and quite different formulation in the cognate provisions in the United Kingdom, which do not depend on the standard of a skilled person’s opinion of the relevance of the information.
The question of what a person skilled in the relevant art would regard as relevant, when faced with the same problem as the patentee, is to be determined on the evidence. The starting point is the subject matter of the invention to be considered together with evidence in respect of prior art, common general knowledge, the way in which the invention is an advance in the art, and any related matters. It should be mentioned that the starting point is not necessarily the inventive step as claimed, or even agreed between the parties, because the evidence, particularly in respect of a combination of integers, may support a different inventive step.
(emphasis added)
670 Thus, whether or not particular prior art is additional information “relevant” within terms of s 7(3), depends on the skilled person’s opinion, when faced with the same problem as the patentee, of the relevance of the information.
671 It is clear that the effect of s 7(3) of the Act was to liberalise the restrictive approach of the 1952 Act, under which prior art not proved to be part of the common general knowledge at the priority date could not be used in assessing whether there was an inventive step.
672 In Lockwood (No 2), the High Court at 221-222 explained the expansion as follows:
The exercise, of which s 7(3) is an integral part, is the exercise of determining whether “an invention” (s 7(2)) as disclosed “in any claim” (s 18(1)) “involve[s] an inventive step when compared with the prior art base” (s 7(2)). The “prior art base” for s 7(2) is enlarged by s 7(3), so as to go beyond common general knowledge and to bring into consideration “prior art information” which “could ... be reasonably expected to have [been] ascertained, understood and regarded as relevant to work in the relevant art” (s 7(3)) by “a person skilled in the relevant art” (s 7(2)). This brings to mind Lord Reid's reference to a “diligent searcher” in Technograph Printed Circuits Ltd v Mills and Rockley (Electronics) Ltd and suggests a person skilled in the relevant art familiar with some, but not necessarily every piece of, publicly available information in the relevant art beyond common general knowledge.
673 The conditions which must be satisfied to render information available under s 7(3) have been discussed in the authorities.
674 In Commissioner of Patents v Emperor Sports Pty Ltd (2006) 149 FCR 386 at 393 (“Emperor Sports”), the Full Federal Court held that “ascertained” means discovered or found. If the relevant prior art is disputed, there must be proof that the relevant document would reasonably have been ascertained by the skilled addressee. The searches that the skilled person might be reasonably, rather than “fancifully”, expected to undertake when faced with the problem at hand, must be considered. In Emperor Sports, the Full Court stated at 394:
Simply stated, we think it self-evident that it could not be reasonably expected that a Rugby League or Australian Rules coach, referee, umpire or administrator would conduct a search in the United States Patent Office. Such an expectation would be fanciful rather than reasonable.
675 In Lockwood (No 2), the High Court stated at 219 that “understood” means that, having discovered the information, the skilled addressee would have “comprehended it” or “appreciated its meaning or import”.
676 In Ajinomoto Company Inc v NutraSweet Australia Pty Ltd (2008) 166 FCR 530 at 550 and 552 to 553, the Full Court acknowledged that the expression “relevant to work in the relevant art”, as contained in the applicable historical version of s 7(3), created a precondition to the use of any information over and above the common general knowledge that work of the relevant kind had been undertaken in Australia at the relevant time.
677 S&N submitted that Johnson I or Johnson II could be taken into account pursuant to s 7(3), and their disclosures taken with common general knowledge would render the claims obvious.
678 In order for the information contained in Johnson I or Johnson II to be taken into account under s 7(3) in determining whether there were an inventive step, S&N must establish that a person skilled in the art could, before the priority date, have been reasonably expected to have ascertained, understood and regarded such information as relevant.
679 KCI submitted that the skilled addressee in the present context was “a professional or team of professionals involved in advanced or chronic wound care and, more specifically, a plastic surgeon”. On this basis, S&N submitted that the Johnson papers would have been ascertained, understood and regarded as relevant to plastic surgeons (as well as to a broader team, including vascular and specialist general surgeons). Such persons treat advanced or chronic wounds, and the Johnson papers respectively taught, relevantly, about fluid drainage from open or closed wounds (Johnson II) and a means of immobilising skin used in a graft and eliminating dead space in wounds (Johnson I).
680 S&N submitted that the evidence established that the skilled addressee would have ascertained Johnson I and Johnson II, as they were published in Surgery, Gynecology & Obstetrics in 1984 and 1985 respectively and were available to any member of the public in the National Library of Australia or through the Australian inter-library loans system, on (or shortly after) 23 September 1985 and 14 April 1986 respectively.
681 Professor Stacey regularly read Surgery, Gynecology & Obstetrics from the mid-1980s and early 1990s because it was then particularly relevant to his work and research interests. He was aware that the journal was available at two libraries he used, namely the Royal Perth Medical Library and the University of Western Australia Medical Library. Professor Kimble and Dr Williams also read the journal on a regular or semi-regular basis prior to November 1991.
682 KCI submitted, and I accept, that S&N failed to demonstrate that the information in the prior art documents was part of common general knowledge in Australia at November 1991. Professors Stacey and Penington were first provided with copies of the prior art documents for the purpose of giving evidence and had not read them, practised the technique they described or seen anyone else do so.
683 Professors Stacey and Penington were provided with copies of Johnson I and II for the purpose of providing evidence, and while Professor Stacey read the relevant journal when doing surgical training, he did not do so as a practising surgeon, and could not recall reading Johnson I or II or recall that they were brought to his attention.
684 Further, as S&N ultimately conceded, Johnson I or II were at the edges of satisfying the criteria for availability under s 7(3). I was not persuaded that they would have been ascertained, understood or regarded as relevant to the problem faced by the patentee, and were thereby available when assessing whether there was an inventive step.
685 Moreover, I was not persuaded that if Johnson I or Johnson II were available, it would have been obvious in the light of common general knowledge to arrive at the combination of components of the apparatus or method claims.
686 Professor Penington testified that if he had read Johnson I before the priority date and sought to practice its technique, it was “likely I would have tried this technique with… foam” rather than gauze. Thus, at the highest, he would have placed foam over an already closed wound.
687 Professor Stacey testified that if he had read Johnson I before the priority date, he “might have considered whether it had wider application to wounds that produce a lot of unwanted fluid”, which, at the highest, would have resulted in gauze being placed over a skin graft or a highly exudatory wound. Professor Stacey did not maintain that he would have considered the use of foam.
688 Professor Penington regarded Johnson II as describing a technique of using suction to drain closed surgical wounds which he had used before November 1991. He testified that “if I had turned my mind to the problem of drainage of open wounds before November 1991”, he would have used a cover film to create an airtight space around the wound so that suction could be applied to drain the wound (this is not the problem faced by the inventors), but did not claim that he would have used a screen with negative pressure to accelerate wound closure or that he would cover any open portion of the wound.
689 Professor Stacey testified that “if I had applied this technique [in Johnson II] to the open wound… in November 1991, then I would have applied the gauze across the open wound, lain the tube across the gauze to absorb the wound fluids and to prevent the transparent cover from sticking directly to the wound, and sealed the area with a cover… with the tube coming out through the cover”. He considered the technique described in Johnson II very similar to the suction drainage systems he had earlier used and did not claim that he would have used a screen with negative pressure to accelerate wound closure.
690 Further, S&N’s witnesses did not explain what steps they might have taken at November 1991 if they were faced with the problem addressed by the inventors.
691 Dr Pohl’s uncontradicted evidence was that although he knew of open drainage systems as described by Dr Williams, he would not have been directly led “as a matter of routine” to try the solutions claimed in the Patent.
692 The uncontradicted evidence of Mr Ellis was that “I certainly did not consider, and it was never suggested to me by any colleagues, surgeons, or any literature I read, that suction drains had or could be used as a method of treatment which would have a therapeutic effect above and beyond the straight forward removal of fluid”.
693 Professor Marshall testified that he would not have thought of sealing an open wound to which he applied suction drainage, so would not have been led to a device for achieving vacuum assisted closure of an open wound.
694 Professor Kimble implicitly distinguished the KCI V.A.C.® therapy system (introduced commercially about five years after the priority date), which he described as “the very first negative pressure treatment for a surface wound”, from the previously available suction drainage techniques.
695 Professors Stacey and Penington testified that they knew of suction sources, wound dressings, covers and tubes and the use of those components in (closed) wound drainage systems, but gave no evidence of any steps they may have taken to arrive at an improved method or apparatus for use to accelerate wound closure.
696 Further, as KCI submitted, the weight of the evidence of Professors Penington, Stacey, and Kimble, in relation to whether there was an inventive step involved in the claimed invention, must be tempered in recognition of the dangers of hindsight, as they had reviewed the Patent before giving evidence in relation to the prior art (which the Full Federal Court in Minnesota Mining & Manufacturing Co v Tyco Electronics Pty Ltd (2002) 56 IPR 248 described at 258 as being “tantamount to leading the witness”) and had used the KCI V.A.C.® device, in some cases for many years.
697 It is thus almost impossible to exclude the effect of the witnesses’ subsequent exposure to information, knowledge of the invention or information about any prior art acquired after the priority date. As Aickin J stated in Minnesota Mining at 293:
It is in relation to this process that the misuse of hindsight is most common. When once an idea or an object or a process or a combination, admittedly novel, has been published, it is very easy to say after perhaps months of search and study in the Patent Office and the public libraries that the integers into which the patent might be dissected could be found scattered amongst the prior documents by a person who already knew the solution to the problem and therefore knew what to look for and what to discard. But that process does not demonstrate lack of an inventive step. The opening of a safe is easy when the combination has been already provided.
698 In Aktiebolaget at 423, the High Court said:
The defendant to an infringement action who cross-claims for revocation on the ground of obviousness bears the onus of establishing that case. This obliges the defendant to lead evidence looking back to the priority date, sometimes, as here, many years before trial. In those circumstances, the warnings in the authorities against the misuse of hindsight are not to be repeated as but prefatory averments and statements of trite law. The danger of such misuse will be particularly acute where what is claimed is a new and inventive combination for the interaction of integers, some or all of which are known. It is worth repeating what was said by Lord Diplock in Technograph Printed Circuits Ltd v Mills & Rockley (Electronics) Ltd:
Once an invention has been made it is generally possible to postulate a combination of steps by which the inventor might have arrived at the invention that he claims in his specification if he started from something that was already known. But it is only because the invention has been made and has proved successful that it is possible to postulate from what starting point and by what particular combination of steps the inventor could have arrived at his invention. It may be that taken in isolation none of the steps which it is now possible to postulate, if taken in isolation, appears to call for any inventive ingenuity. It is improbable that this reconstruction a posteriori represents the mental process by which the inventor in fact arrived at his invention, but, even if it were, inventive ingenuity lay in perceiving that the final result which it was the object of the inventor to achieve was attainable from the particular starting point and in his selection of the particular combination of steps which would lead to that result.
699 In Lockwood (No 2) at 193, the High Court repeated the caveat against the misuse of hindsight in relation to patents which are a new and inventive combination of known integers.
700 KCI also relied on the commercial success of the KCI V.A.C.® therapy system as an indicator of inventiveness. While S&N argued that the commercial success could be attributable to matters other than the invention, the evidence suggested “a long-felt want”. In my view, the commercial success fortified, but was unnecessary to, the conclusion that obviousness was not established.
701 S&N also advocated a novel interpretation of s 7(2) which, if accepted, would tend to assimilate the Australian law on obviousness to UK law, and would, in the present case, permit consideration of information in any one of certain prior art documents (Bagautdinov I, Zamierowski, Chariker and Jeter (individually), and Jeter and Chariker (read together)) combined with common general knowledge as the “starting point” for assessing whether an invention involved an inventive step. In that context, S&N relied on the statement in s 18(1)(b)(ii) of the Act that an invention claimed must possess an inventive step “when compared with the prior art base”. The prior art base is defined in Schedule 1 to the Act to include information in a document publicly available anywhere (or information made publicly available by doing an act).
702 S&N submitted that under s 7(2) of the Act, the comparison required by s 18(1)(b)(ii) is to be undertaken both “in the light of the common general knowledge” and the specified comparator of the prior art base which (in contrast to s 100(1)(e) of the 1952 Act), s 7(2) invoked.
703 In S&N’s submission, Aickin J’s well known caveat in Minnesota Mining that the common general knowledge could not be “mosaiced” with prior art was confined to the process of assessing the inventive step, and was not a comment on where the statutory step commences. In Minnesota Mining, there was no need to deal with the statutory starting point separately from the assessment, as in that case, there was a problem or a known need which was common general knowledge.
704 S&N submitted that Minnesota Mining thus neither dealt with where the statutory step commences or the “starting point” of that assessment referred to in Apotex at 441. Nor did it preclude a construction of the present legislation which permitted access to a prior art document for that purpose. The reasoning in Apotex also supported the distinction between a starting point and the assessment.
705 In Wellcome Foundation Limited v VR Laboratories (Aust) Pty Ltd (1981) 148 CLR 262 at 286, Aickin J said:
The test is whether the hypothetical addressee faced with the same problem would have taken as a matter of routine whatever steps might have led from the prior art to the invention, whether they be the steps of the inventor or not.
706 S&N submitted that:
[T]he common general knowledge (which can be supplemented, if s7(3) applies) is the equipment that the hypothetical skilled addressee has on the journey. The inventive step is assessed “in light of”, or “having regard to” that background knowledge. Under the 1990 Act, the starting point is a document made publicly available anywhere in the world. That document is the comparator; common general knowledge and s7(3) are used for the comparison.
707 S&N submitted that s 7(3) did not confine the prior art base comparator for the purposes of s 7(2). Rather, it expanded the equipment that may be used for the comparison. The “information” referred to in s 7(3) is broader than the prior art base (because the items can be combined).
708 KCI submitted that, contrary to S&N’s construction, s 18(1)(b)(ii) of the Act referred to a comparison with the prior art base in the context of directing an enquiry as to whether there is an inventive step, which was in turn to be determined by the combined operation of ss 7(2) and (3).
709 KCI submitted that the High Court’s analysis in Lockwood (No 2), far from supporting S&N’s construction, recognised that the background art against which “inventive step” is to be tested consisted of common general knowledge according to Minnesota Mining, but expanded by any information now available under s 7(3). In examining the question of “inventive step” in Firebelt and Lockwood (No 2), the High Court gave no indication that the reference in s 7(2) to “prior art base” now permitted any further information to be taken into account.
710 Further, KCI submitted that “the “alternative” approach advanced by S&N would take the Australian prior art base for obviousness very close to that of the UK”, which was contrary to the High Court’s recognition in Aktiebolaget and Lundbeck of the divergence.
711 S&N’s alternative argument would permit the skilled person to start from the prior art base, which would be, according to the definition in Schedule 1, any one piece of information in a document publicly available in or out of the patent area or made publicly available through the doing of an act in or out of the patent area. The skilled person would have access to the comparator (in the present case, for example Bagautdinov I or Zamierowski) and then in assessing whether the invention was obvious from that starting point, would consider, in the light of common general knowledge and any information available under in s 7(3) (being a single piece of information, or a combination of two or more pieces thereof), if it meets the further requirements that the person would be reasonably expected to have ascertained, understood, regarded as relevant or combined.
712 S&N’s construction may be open on a literal reading of s 7(2), which by the words “when compared with the prior art base” picks up the s 18(1)(b) requirement for a comparison with the prior art base. It was, however, ultimately unpersuasive.
713 Section 7(3) sets out with precision the information to which the skilled person may have access and imposes multiple restrictive preconditions. S&N’s construction would render s 7(3) largely irrelevant (but not otiose, as s 7(3) potentially allows items to be combined). It is improbable that a radical assimilation to the UK position, which the High Court recognises as divergent, would be effected so obliquely. The position which would result was not recommended by IPAC and is inconsistent with the relevant authority.
714 S&N’s construction also appears inconsistent with that adopted by the Full Federal Court in Insta Image, where Lindgren, Bennett and Logan JJ stated at 35 to 36:
It is not necessary to dwell on the concept of the prior art base because of the deeming effect of s 7(2).
It follows from the provisions of the Act outlined above that in determining the issue of obviousness, it is necessary:
(1) to identify the invention “so far as claimed in any claim”;
(2) to identify the “person skilled in the relevant art”;
(3) to identify the common general knowledge as it existed in Australia before the priority date;
(4) to inquire under s 7(2) whether the invention referred to in (1) above would have been obvious to the person referred to in (2) above in light of the knowledge referred to in (3) above; and
(5) to inquire whether that invention would have been obvious to that person in the light of that knowledge when that knowledge is considered together with either kinds of information mentioned in s 7(3) (additional prior art information).
715 Their Honours did not refer to S&N’s construction. Rather, they apparently concluded that the reference in s 7(2) to the prior art comparator should be deemed inoperative, and the steps they identified as relevant to determining obviousness made no reference to access to the prior art base as a starting point.
716 In “The Curious Case of the Inventive Step and Innovative Step Provisions Under the Patents Act 1990: A Drafting Flaw?” (2010) 21(1) AIPJ 4, Dr Geoffrey Levy identified, at the heart of the disputed construction of the inventive step provisions, a drafting flaw. Dr Levy observed that s 7(2) had a comparison component, the role of which was overlooked in the case law, save for Insta Image referred to above. Dr Levy, while critical of the “deeming” analysis in Insta Image, nevertheless considered that there was “good reason to ignore the comparison component in s 7(2)” (at 8).
717 Dr Levy stated:
If s 7(2) did require a comparison between the invention and the prior art base, that would render s 7(3) irrelevant. Because the prior art base, as defined, consists of information in a document that is publicly available, or information made publicly available through doing an act, in either case anywhere in the world, there would be no need ever to utilise s 7(3) with its triple hurdles of “ascertained, understood and regarded as relevant”.
Conclusion
718 It follows that, in my opinion, the novel construction of s 7(2) advanced by S&N should be rejected. Therefore, Bagautdinov I, Zamierowski or any other prior art document would not be available to the skilled addressee as a starting point and it is unnecessary to consider their effect as such in relation to obviousness.
719 S&N did not establish that the invention lacked an inventive step in that it would have been obvious to the person skilled in the art in the light of common general knowledge and any s 7(3) prior art information.
720 S&N did not establish that the criteria for consideration under s 7(3) were satisfied in relation to Johnson I, Johnson II or any other piece of prior art information.
721 As Dr Levy argued, s 7(2) may embody a drafting flaw, which was addressed in Insta Image by a deeming approach. S&N’s construction of s 7(2) was unpersuasive and, in my opinion, the relevant skilled addressee would not have available as a comparator or starting point any one of the prior art items.
722 S&N alleged that the Patent’s priority date of 14 November 1991 was lost, because on 7 November 1996, the applicant for the Patent made amendments by which the claims were extended and “travelled beyond the specification as filed”. The claims in suit were consequently not disclosed in the priority documents and thus invalidated.
723 Section 102(2)(a) of the Act provides:
An amendment of a complete specification is not allowable after the relevant time if, as a result of the amendment:
(a) a claim of the specification would not in substance fall within the scope of the claims of the specification before amendment.
724 Section 114 of the Act provides:
Where a claim of a complete specification claims matter that was in substance disclosed as a result of amending the specification, the priority date of the claim must be determined under the regulations.
725 Reg 3.14 of the Patents Regulations 1991 (Cth) provides:
If subsection 114(1) of the Act applies to a claim of a specification, the priority date of the claim is:
(a) in the case of an amendment to which subsection 89(4) or (5) of the Act applies — the date on which the amendment is taken to have been made under that subsection; and
(b) in any other case — the date of filing of the statement of proposed amendments that resulted in the disclosure referred to in subsection 114(1) of the Act.
726 The Patent specification states that the material of the screen means “must be sufficiently porous to allow oxygen to reach the wound” (“the oxygen reference”).
727 On 10 October 1996 and 7 November 1996, the applicant for the Patent further amended the specification, added new claims and added to claims the following: “… said screen means being sufficiently porous to allow gases to reach the wound” (emphasis added) (“the gases reference”).
728 In Delnorth Pty Ltd & Anor v Dura-Post (Aust) Pty Ltd & Anor (2008) 78 IPR 463, Gyles J referred to Re Stauffer Chemical Co’s Application [1977] RPC 33 at 54 where Buckley LJ stated:
If, on the other hand, the additional feature involves a new inventive step or brings something new into the combination which represents a departure from the idea of the invention described in the earlier document, it could not, I think, be properly described as fairly based upon the earlier document.
729 S&N initially submitted that the reference to oxygen embodied the idea that atmospheric oxygen assists in wound healing. In S&N’s submission, while that idea was fallacious and without scientific foundation, the reference reflected the inventors’ awareness in 1991 that wound sites are deficient in oxygen, and the consequent assumption that allowing oxygen to be delivered to the wound was desirable. Drs Argenta and Morykwas, the makers of the invention, published a paper on hyperbaric oxygen, which fortified the likelihood of reference to that concept.
730 S&N conceded, in that context, that the idea of delivering oxygen to the wound site was medically absurd, as all expert witnesses agreed that oxygen is brought to the wound by capillaries. It submitted, however, that it could not be assumed that the inventors appreciated that in 1991.
731 S&N also ultimately conceded that (as contended by KCI) the reference to gases in the claims expressed the notion that the porosity of the foam enables air to pass through it, permitting an even distribution of negative pressure throughout the wound. Indeed, S&N accepted that its products possessed the porosity integer, understood in that sense.
732 S&N nevertheless contended that the integer of a screen means sufficiently porous to allow gases to reach the wound (which it conceded meant the transmission of negative pressure) was a completely different concept from the oxygen reference in the specification, which was a genuine medical concept that did not in substance disclose the integer in a real and reasonably clear manner.
733 S&N submitted that the reference was not a mere infelicity that the skilled addressee could correct. To the contrary, the skilled addressee would simply dismiss the oxygen reference in the specification as “stupid” and identify the gases reference in the claims as an entirely new idea.
734 S&N submitted that Professor Marshall equivocated and resorted to context to “save” the oxygen reference.
735 Alternatively, S&N submitted that the oxygen reference in the specification was to the established theory of hyperbaric oxygen which, at a higher pressure, could play a role in wound healing, a topic on which Drs Argenta and Morykwas had published.
736 S&N alleged that there was, on that basis, a disconformity between the notion of air, expressed as gases, passing through the porous fibres of the screen and permitting even distribution of negative pressure, and the notion underpinning the reference to oxygen, which would impermissibly broaden the scope and alter the meaning of the claims in suit.
737 S&N submitted that consequently, each of the claims in suit claimed matter that was, in substance, disclosed only as a result of the amendments. It submitted that the priority date for all claims in suit therefore shifted to 7 November 1996.
738 By that date, KCI had already been using the method and apparatus disclosed in the patent, so all the claims in suit were not novel or inventive as at that date.
739 Further, the reference to oxygen in the specification did not provide “real and reasonably clear disclosure” of the notion on which the gases reference is based. Therefore, the claims were not fairly based.
740 KCI submitted that on a proper construction, the oxygen reference and the gases reference were synonymous. The reference to “oxygen” in the specification was, it submitted, merely a loose reference to gases generally, which in turn was a reference to air.
741 KCI submitted that both terms described the requisite porosity which could allow gases to pass through the foam (screen) in order to enable the device to exert negative pressure at the wound bed, according to Professor Wilkins’ explanation. On a practical construction, neither term described a requirement that atmospheric oxygen or other gases be delivered from outside the apparatus into the wound site, because, as all experts agreed, wounds receive oxygen from the blood supply, so it would be perversely literal to interpret the phrases as teaching a medical and scientific absurdity.
742 KCI contended that the screen enabled negative pressure created beneath the plastic film seal to be delivered to the wound bed, as atmospheric gases (of which oxygen is one) were drawn away from the wound bed through the porous screen. The porosity of the screen was necessary in order for the relevant sucking force to be exerted on the wound bed.
Expert evidence
743 Professor Marshall deposed that he did not interpret the oxygen phrase to mean that the invention delivered oxygen into a wound, because all bodily tissues receive oxygen from the capillary blood supply, so there was no need for oxygen to reach a wound through the screen. He understood the gases reference in the claims as a requirement that the negative pressure applied by the suction device, via the screen, be in contact with the whole of the wound.
744 In cross-examination, Professor Marshall initially conceded that he “may have thought” the oxygen reference was to something similar to hyperbaric oxygen (that is, the idea that oxygen should be delivered to the oxygen-poor environment of a wound) but in the context of the whole document (which also referred to gases) would have assumed that the oxygen reference was a loose description of gases more generally. He subsequently stated that he would only have interpreted the oxygen reference as referring to hyperbaric oxygen in a “non-medical context”, and that, as a surgeon, he would not have entertained that notion.
745 Professor Penington deposed that, in his view, the gases reference was not “sensible”, as it would take a long time for oxygen to move from the atmosphere into a cell, and oxygen is, in any event, supplied by the blood flowing in the capillaries in and near the wound. He considered “unconvincing” Professor Marshall’s attempt to reconcile the words of the Patent with the fact that the suction tube does not transmit oxygen to the wound. Rather, Professor Penington considered that the drafting of the Patent revealed conceptual misunderstanding.
746 Professor Stacey deposed that the gases reference would have had no meaning to him in 1991, and had no meaning now. He deposed that allowing gases to reach the wound from outside was not an important goal in wound healing, as wounds obtain their nutrients from the blood. Nor could he see how gases could reach a wound in a negative pressure environment, given that the purpose of such environment was to provide suction.
747 Professor Stacey deposed that he could not understand Professor Marshall’s interpretation of the gases reference. He considered it impossible to read the requirement that gases reach the wound as a requirement that negative pressure be in contact with the whole wound.
748 In cross-examination, Professor Stacey indicated that the oxygen reference was perplexing, because there was no scientific evidence that delivering oxygen to the wound from outside was beneficial. He referred to “topical oxygen”, a concept of delivering oxygen to wounds at the surface, which was probably practised around 1991, but he did not suggest that he interpreted the oxygen reference as referring to topical oxygen.
749 Professor Stacey conceded in cross-examination that there was no reference elsewhere in the specification to oxygen or to any other gas being delivered to the wound from outside the apparatus.
750 In the light of Dr Wilkins’ explanation of how the porosity of the foam assists the exertion of negative pressure at the wound bed, Professor Stacey conceded that on a fair reading of the Patent, the inventors described the foam’s capacity to allow ambient air to pass through its pores. However, he stated that such a reading was “not obvious immediately”, and that it was “unusual” to suggest the purpose was to deliver gas if it was really to draw gas away.
751 Dr Pohl deposed that, as at 1991, he would have understood the gases reference as a requirement that the screen means be porous enough to allow negative pressure to be transmitted to the whole interface of the screen and wound.
752 When asked in cross-examination whether the oxygen reference may have referred to hyperbaric oxygen or the notion that the wound would be benefited by oxygen reaching it, Dr Pohl responded that “oxygen will be beneficial, certainly, yes.”
753 Professor Kimble deposed that that goal of negative pressure was not for gases to reach the wound from the outside, but rather, to allow fluids and gases to flow out of the wound with the use of suction. Accordingly, he was “at a loss” as to how to achieve the aim of having gases reach the wound while using suction.
754 In cross-examination, Professor Kimble stated that he thought it unnecessary to enlist the aid of a biomedical engineer to understand the requirement of sufficient porosity.
755 Dr Wilkins deposed that the points where the foam contacts the wound bed involved higher contact pressure than the points of non-contact associated with the open cells of the foam.
756 When taken to Dr Wilkins’ evidence of alternating areas of compression and suction where foam is placed in a wound, Professor Kimble agreed that because the pores communicate with one another from the top of the foam to the bottom, if gas could reach the wound, it could also be drawn off the wound. He did not, however, consider it fair to read the oxygen reference as referring to the “free flow of gas and fluid” in that sense. The oxygen reference was not, in Professor Kimble’s view, a logical way of expressing that concept. He stated “I can’t… for the life of me see why it was written that way”.
Conclusion
757 I was satisfied that when the reference to gases in the claims were construed practically, in the context of the whole document, in the light of the physics of the interaction of negative pressure with the wound bed (as explained by Dr Wilkins, amplified by Professor Marshall, conceded by Professor Stacey and ultimately by S&N), and in light of the universally acknowledged absurdity of a literal construction of the reference to oxygen, both the oxygen and gases references, while inelegant, described the same phenomenon, namely, the capacity of the screen to allow ambient air to pass through the foam.
758 The failure of any witness to construe the oxygen reference as a reference to hyperbaric oxygen or to identify the nature of the differences alleged between the oxygen and gases references, fortified that conclusion.
759 Therefore, in my opinion, the alleged disconformity was not established. The priority date should not be deferred on the basis alleged. Nor was the absence of fair basis made out.
760 S&N alleged that claims 1, 2, 3, 6, 7, 8, 9, 10, 11, 12 and 121 were invalid because they comprised mere clinical desiderata or mere collocations of known integers performing known functions. The invention was thus not “a manner of manufacture within the meaning of s 6 of the Statute of Monopolies”, as required by s 18(1)(a) of the Act.
761 As S&N acknowledged, in contrast to the position in the UK and Europe, the Full Court has recognised that a method of treatment of the human body is in principle patentable: see Anaesthetic Supplies Pty Ltd v Rescare Ltd (1994) 50 FCR 1 (“Rescare”) and BMS.
762 In Rescare, Lockhart J (with whom Wilcox J agreed) stated at 19:
In my opinion, there is no justification in law or in logic to say that simply because on the one hand substances produce a cosmetic result or a functional result as opposed to a curative result, one is patentable and the other is not. I see no reason in principle why a method of treatment of the human body is any less a manner of manufacture than a method for ridding crops of weeds as in NRDC. Australian courts must now take a realistic view of the matter in light of current scientific development and legal process; the law must move with changing needs and times.
763 In BMS, Black CJ and Lehane J endorsed the majority view in Rescare, stating at 529 to 530:
[W]e consider that we should adopt and apply the view of the majority in Rescare: a view reached after a close and persuasive analysis of principle and authority. In taking this course, we are fortified by two considerations. The first of these is what seems to us to be the insurmountable problem, from a public policy viewpoint, of drawing a logical distinction which would justify allowing patentability for a product for treating the human body, but deny patentability for a method of treatment: see per Davison CJ in Wellcome Foundation Ltd v Commissioner of Patents [1979] 2 NZLR 591 at 620 and per Gummow J in Rescare at 238. This seems particularly the case where, as here, the claim is for an invention for the administration of a product.
The second compelling consideration is the very limited extent to which the parliament dealt with patents with respect to the human body when it enacted the 1990 Act, bearing in mind, too, that it did so at a time when the long-standing practice in Australia was (as we are informed it still is) to grant patents for methods of medical treatment of the human body.
764 While a method of treating wounds thus falls within the concept of “manner of manufacture” in terms of s 18(1)(a), S&N submitted that the present case was distinguishable from Rescare and BMS, because in those cases, the invention was tightly defined either by the apparatus to be used (Rescare) or the dosage regime (BMS). S&N argued that in contrast to Rescare and BMS, in the present case, elements of the methods claimed were left to the clinician (such as the reference to “area sufficient…” in claim 1, its dependent claims and claim 121). As such, they did not discover a method which resulted in a new apparatus or process or an old apparatus with a new and improved result. The claims therefore failed to disclose a manner of manufacture: see, for example, Grant v Commissioner of Patents (2006) 154 FCR 62. Rather, the evidence established that the elements were merely desirable components.
765 S&N submitted that the evidence established that each of the claims in suit simply described “what surgeons do” and were mere desiderata.
766 S&N relied in that context on Wilcox J’s statement in NV Philips Gloeilampenfabrieken & Anor v Mirabella International Pty Ltd (1992) 24 IPR 1 at 35 that “it is not an invention, or a manner of new manufacture, for someone to specify the criteria required to be met, in the manufacture of a known product from known materials, in order to achieve vendibility”. On appeal, the Full Court majority upheld that view in NV Philips Gloeilampenfabrieken & Anor v Mirabella International Pty Ltd (1993) 44 FCR 239, where Lockhart J (with whom Northrop J agreed) stated at 265:
[W]hat the patentee has done in this case is to choose two desirable characteristics of the known phosphors and to claim lamps using all phosphors, present and future, possessing those characteristics… [T]he patentee has essentially “formulated requirements”… and claimed them as limitations on the luminescent material. I agree with his Honour’s finding that this is not an invention.
767 In Eli Lilly and Co v Pfizer Overseas Pharmaceuticals (2005) 64 IPR 506 (“Eli Lilly”), Heerey J stated at 542 to 543:
A mere method or scheme is not an invention... Nor is a "mere desideratum", that is to say something which is disclosed as no more than a wished for result…. These criteria are to be applied to the specification on its face…
768 In National Research Development Corporation v Commissioner of Patents (1959) 102 CLR 252 (“NRDC”), the High Court stated at 261-262 that:
[T]he Commissioner may properly reject a claim for a process which is not within the concept of a “manufacture”. But… even if the process is within the concept the Commissioner is not bound to accept the allegation of the applicant that it is new, if it is apparent on the face of the specification, when properly construed, that the allegation is unfounded.
769 The High Court continued at 275:
... a process, to fall within the limits of patentability which the context of the Statute of Monopolies has supplied, must be one that offers some advantage which is material, in the sense that the process belongs to a useful art as distinct from a fine art… that its value to the country is in the field of economic endeavour.
770 The Explanatory Memorandum which accompanied the Patents Bill 1989 stated at paragraph 29:
The requirement in paragraph 18(a) that an invention, in order to be patentable, must be a “manner of manufacture” invokes a long line of UK and Australian court decisions. It means little more than that an invention must belong to the useful arts rather than the fine arts.
(emphasis added)
771 In my opinion, the alleged distinction from Rescare and BMS (which was not amplified) was unpersuasive. Nor, on a fair construction, is the invention claimed in the Patent and the relevant claims merely a method or product described by reference to a set of obviously desirable parameters. It claims a new process and a new apparatus (albeit a combination of known items) to achieve an improved method of wound treatment. The Patent specification teaches the means of achieving the desired end by the method and apparatus for the application of negative pressure to promote tissue migration and increase the formation of granulation tissue so as to facilitate closure of the wound. In my view, the claims were not “mere desiderata”.
772 Nor was it apparent from matters disclosed on the face of the specification of the Patent that the invention lacked the necessary quality of newness or inventiveness.
773 In Commissioner of Patents v Microcell Ltd & Ors (1959) 102 CLR 232 (“Microcell”), the High Court stated at 250:
Here the specification does not on its face disclose more than a new use of a particular known product. To use Lord Buckmaster’s words, no new product is obtained, and there is no new method of manufacture suggested or an old one improved. Tubular self-propelled-rocket projectors were at the relevant time well-known articles of manufacture. Synthetic resinous plastics reinforced with mineral fibres, and in particular polyester plastics reinforced with glass or asbestos fibres, were well-known materials. These things are to be gathered from the specification itself, which contains no suggestion of novelty in relation to the article to be manufactured or the material to be used.
774 The High Court concluded that merely because it had not previously occurred to anyone to make a rocket projector out of reinforced plastic, it did not follow that the specification disclosed an inventive idea.
775 In NV Philips Gloeilampenfabrieken v Mirabella International Pty Ltd (1995) 183 CLR 655 (“Philips”), the High Court majority (Brennan, Deane and Toohey JJ) upheld the holdings below that the claimed invention of a low pressure mercury vapour discharge lamp was no more than a new use of a known material (phosphorus), to make known articles for which the properties of phosphorus made it suitable. It was thus not a manner of manufacture nor, consequently, a patentable invention (at 668). Their Honours apparently accepted, in that context, the importance of the traditional patents law threshold question of whether it was apparent on the face of the specification, when properly construed, that the subject matter lacked the requisite inventiveness and thus was not a manner of manufacture (at 662). They stated at 663-664:
In the light of what has been said above about what is involved in an alleged manner of new manufacture, that threshold requirement of “an alleged invention” will, notwithstanding an assertion of “newness”, remain unsatisfied if it is apparent on the face of the relevant specification that the subject matter of the claim is, by reason of absence of the necessary quality of inventiveness, not a manner of new manufacture for the purposes of the Statute of Monopolies. That does not mean that the threshold requirement of “an alleged invention” corresponds with or renders otiose the more specific requirements of novelty and inventive step (when compared with the prior art base) contained in s 18(1)(b). It simply means that, if it is apparent on the face of the specification that the quality of inventiveness necessary for there to be a proper subject of letters patent under the Statute of Monopolies is absent, one need go no further.
776 The majority in Philips rejected the submission that Microcell was decided on the question of newness, rather than manner of manufacture (at 665).
777 In Advanced Building Systems Pty Ltd & Anor v Ramset Fasteners (Aust) Pty Ltd (1998) 194 CLR 171 (“Ramset Fasteners”), the majority of the High Court (Brennan CJ, Gaudron, McHugh and Gummow JJ) identified Philips with a category of cases where the lack of an inventive step appeared on the face of the specification (at 192 to 193).
778 In contrast, Ramset Fasteners concerned the validity of combination claims in the light of prior publications. The majority concluded that the Full Federal Court erred in considering, under s 100(1)(d) of the 1952 Act (concerned with whether the invention claimed was not an invention within the meaning of that Act), matters that could have arisen under the grounds of obviousness and lack of novelty.
779 In Lockwood (No 2), the High Court referred at 211 to the:
… narrow proposition that a Commissioner of Patents, or his or her delegate, may refuse an application for patent protection where a specification “on its face” shows the invention claimed is not a manner of new manufacture. This may arise, for example, from admissions concerning novelty. The decision in Microcell has not always been properly understood; it does not involve a separate ground of invalidity or a discrete “threshold” test.
780 In Lockwood (No 2), the High Court recognised the limited nature of this ground of invalidity, observing at 211 that such cases “are likely to be rare”.
781 In Dura-Post (Aust) Pty Ltd v Delnorth Pty Ltd (2009) 177 FCR 239 (“Dura-Post”), the Full Court indicated that a Microcell or Philips type manner of manufacture objection should be based on the face of the specification. Kenny and Stone JJ stated:
We accept, moreover, that Microcell stands for “a narrow proposition that a Commissioner of Patents, or his or her delegate, may refuse an application for patent protection where a specification ‘on its face’ shows the invention claimed is not a manner of new manufacture”… As their Honours there said in Mirabella, “if it is apparent on the face of the specification that the quality of inventiveness necessary for there to be a proper subject of letters patent under the Statute of Monopolies is absent, one need go no further.”
782 Their Honours observed that in Dura-Post, the objection was not made out on the face of the specification.
783 In my opinion, in the present case, it was not apparent on the face of the specification that the claims in suit amounted to no more than a new use of known products with suitable properties for such use. The relevant claims were not, in my view, invalid because their subject matter lacked inventiveness and was not a manner of manufacture.
Claim 49: “mere collocation”
784 S&N submitted that claim 49 was invalid on the ground that it was a mere collocation.
785 In Wake Forest, the Full Court set aside an injunction restraining S&N from marketing its foam kits on the basis of alleged infringement of claim 49. The Full Court (Finn, Bennett and Middleton JJ) considered that the aseptic package in claim 49 did not interact with the other integers to produce the desired result of applying negative pressure, so that the combination claim was invalid as a mere collocation.
786 Their Honours distinguished between, on the one hand, a mere optional addition to a combination claim which was not an element of the invention and served only to limit the claim (and thus did not affect its validity) and, on the other hand, an integer which was an element of, and said to limit, the invention (which would affect the validity of the claim).
787 Their Honours accepted at 472 that the aseptic package or bag in claim 49 itself did “nothing to cause, limit or affect the functional result of negative wound pressure as desired”, although it was doubtless beneficial. As the aseptic package had no “inter-related working” with any of the other integers “in the sense that any one of the integers is doing something which it could not do without the presence of one or more of the others” (at 472), the claim for the combination was not valid.
788 The Full Court rejected KCI’s submission that the effect of including an additional integer such as the aseptic bag was simply to limit the claim, and had no ramifications for validity, in circumstances where it asserted that the aseptic package was an essential integer of the combination invention pursuant to s 18(1) of the Act. The Full Court rejected the submission that the failure of the aseptic package to interact with all the other integers to produce a new product or result did not render the claim a mere collocation.
789 The Full Court relied, in particular, on Dixon J’s analysis in Palmer v Dunlop Perdriau Rubber Co Ltd (1937) 59 CLR 30 at 73 of the requirements for a patentable combination of known integers. His Honour there held that if the separate elements, although brought together, continued only to perform their known function as before, they would not amount to a patentable invention.
790 The Full Court stated at 473:
Unlike the case of Pugh v Riley Cycle Co Ltd (1914) 31 RPC 266, for instance, the aseptic package is not an optional extra merely assisting in the presentation of the apparatus, or limiting or adding to the claim. Rather, it is claimed to be an essential feature crucial to the claimed invention and therefore must interact with that apparatus. While the integers that form the actual apparatus might be said to be a new combination, when placed with the essential feature of the aseptic package being part of the invention claimed they form a mere collocation of the apparatus on the one hand and the aseptic package on the other.
(citation added)
791 Before me, KCI “formally” asserted the validity of claim 49 in its written submissions, but did not address the issue in oral argument.
792 In written submissions, KCI appeared to assert that the Full Court, should not, consistently with relevant authority, have gone beyond the face of the specification to determine whether the combination claim was a mere collocation, and erred by instead extending its consideration to the evidence.
793 The Full Court stated at 475:
For the above reasons, the primary judge should have concluded on the evidence before him and on the basis of the construction of claim 49 put forward by the respondents, that claim 49 was invalid, and that the respondents in these circumstances failed to demonstrate that there was a serious question to be tried.
We should stress that we have approached the question of the validity of claim 49 by reference to the evidence and submissions made as to the construction of claim 49 put forward by the respondents. We have not determined the validity of claim 49 finally, this being a matter for the primary judge at trial. We have merely arrived at the conclusion that the primary judge should not have granted the injunction in light of the evidence and the construction of claim 49 put forward by the respondents.
794 In my opinion, their Honours’ approach and analysis of authority was persuasive and I am, in any event, bound by their enunciation of principle.
795 Before the Full Court, KCI conceded that the aseptic package did not interact with the other integers of claim 49 to produce a new product and result. Before me, it advanced no new evidence to suggest the contrary and indeed, as S&N submitted, the evidence at trial fortified KCI’s earlier concession. In my opinion, claim 49 was invalid, inter alia, on the ground that it constituted a mere collocation.
Non-compliance with s 40 of the Act
Sufficiency
796 S&N also alleged that the specification failed to describe the invention “fully” and the best method known to the applicant of performing the invention, contrary to s 40(2)(a).
797 The details of the allegation were set out in its submissions as follows:
|
PLEADING/ |
CLAIMS |
RESPONDENT'S EVIDENCE |
APPLICANTS' |
|
The Specification does not describe the meaning of “an area sufficient to promote migration of epithelial or subcutaneous tissue toward the wound” and how to determine such area or how to ensure the negative pressure is applied to a wound over "an area sufficient to promote migration of epithelial and subcutaneous tissue toward the wound |
1 and dependent claims |
Penington (2) paras 49-52 CB 4/36/0468. Stacey (1) paras 97-98, 148-149 CB 4/42/0568,0578. |
Marshall (1) paras 51, 52, 103 CB 3/26/0255,0267. Marshall (2) paras 15, 36 CB 3/27/0292,0296. Pohl paras 157, 159, 192 CB 3/33/ 0390,0391,0399 |
|
The Specification does not describe the meaning of “time sufficient to facilitate closure of the wound” and how to determine such time |
1 and |
Penington (2) paras 53-55 CB 4/36/0469. Stacey (1) paras 99-100, 150-151 CB 4/42/0568,0579. |
Marshall (1) paras 53, 68, 71, 104, 115 CB 3/26/0256,0259,0268,0270 . Marshall (2) para 37 CB 3/27/0296. Pohl paras 165, 192 CB 3/33/0392,0399. |
|
The Specification does not describe the meaning of “time sufficient to permit the formation of granulation tissue in the wound” and how to determine such time |
2 |
Stacey (1) para 101 CB 4/42/0569. |
Marshall (1) paras 76, 106, 193 CB 3/26/0260,0268,0284. |
|
The Specification does not describe the meaning of |
121 |
Stacey (1) para 119 CB 4/42/0572. Penington (3) paras 11(b), 17(d) CB 4/37/0500,0508. |
Marshall (1) – no evidence on “selected stage of healing” Pohl paras 213, 218(l), 222(i) CB 3/33/0403,0406,0408. |
798 S&N alleged that on the evidence, the skilled addressee (who is competent, has ordinary skill and is conversant with the common general knowledge) was not taught how to make or use something within the claims; nor can he or she determine whether he or she has made or used something within the claims. They were therefore bad for insufficiency.
799 In Kimberly-Clark at 16-17, the High Court referred to the provision in the Patents and Designs Act 1907 (UK) from which s 40(2)(a) of the Act derived, of which Romer LJ, in No-Fume Ltd v Frank Pitchford & Co Ltd (1935) 52 RPC 231, stated at 243:
“[I]n other words, [it is essential] that the patentee should disclose his invention sufficiently to enable those who are skilled in the relevant art to utilise the invention after the patentee's monopoly has come to an end. Such disclosure is, indeed, the consideration that the patentee gives for the grant to him of a monopoly during the period that the patent would run.
…
It is not necessary that he should describe in his specification the manner in which the invention is to be performed, with that wealth of detail with which the specification of the manufacturer of something is usually put before the workman who is engaged to manufacture it.”
800 The High Court stated at 17:
The question is, will the disclosure enable the addressee of the specification to produce something within each claim without new inventions or additions or prolonged study of matters presenting initial difficulty?
801 A description will suffice if it contains enough information to enable the addressee to produce one embodiment that falls within each claim, even if there are other embodiments that are claimed but for which “new inventions or additions or prolonged study of matters presenting initial difficulty” are required.
802 In Lockwood Security Products Pty Ltd v Doric Products Pty Ltd (2004) 217 CLR 274, the High Court said at 297, citing its earlier decision in Kimberly-Clark:
For the purposes of s 40(2)(a), it is not necessary for the inventor to disclose all the alternative means; it is enough that there is disclosure in the sense of enabling the addressee of the specification to produce something within each claim without new inventions or additions or prolonged study of matters presenting additional difficulty.
803 In Eli Lilly, after reciting the test from Kimberly-Clark, Heerey J went on to say:
As Cotton LJ said in Edison and Swan Electric Light Co v Holland (1889) 6 RPC 243 at 277, it is not necessary that the addressee:
… should be able to do the work without any trial or experiment which, when it is new or especially delicate, may frequently be necessary, however clear the description may be.
804 Professors Penington, Stacey and Kimble gave evidence that they did not know, and would not have known in November 1991, what dressing to select with the rigidity to achieve the acquired result. The integer was meaningless to Professor Penington who would not have been able to select the dressing. Professor Stacey would have found the integer difficult to understand and would have been at a loss in selecting a dressing. Professor Kimble would not have known what dressing to select and indeed, did not believe that such a dressing exists.
805 In my opinion, due to the meaningless nature of the “screen rigidity integer” and the associated failure to provide the skilled reader with sufficient guidance on how to select or construct a screen which would achieve the promised result, the invention was not sufficiently described as required by s 40(2)(a) of the Act. Save for that integer, in my opinion the preferred embodiment set out in the specification would have fallen within the scope of the claims, and the specification would have disclosed an embodiment of the invention within their scope.
Failure to define invention
806 S&N alleged that the Patent was invalid for failure to comply with the requirement in s 40(2)(b) of the Act that the specification end with claims which define it.
807 S&N set out the following table of terms which allegedly failed properly to define the monopoly claimed, but it did not otherwise amplify the allegation:
|
PHRASE |
CLAIMS |
RESPONDENT'S EVIDENCE |
APPLICANTS' EVIDENCE |
|
“sufficiently rigid to prevent wound overgrowth” |
1, 49, 50, |
Gordon (1) paras 51-53 CB4/46/0670. Kimble (1) paras 50, 65, 96-97 CB 4/44/0636,0639,0647. Penington (2) paras 47-48, 73, 83 CB 4/36/0467,0474, 0477. Stacey (1) paras 95-96, 145, 147, 242 CB 4/42/0567,0578,0602 |
Marshall (1) paras 78, 101 CB 3/26/0261,0267. Pohl paras 175-176, 191, 290 CB 3/33/0395,0399,0435. |
|
“an area sufficient to promote migration of epithelial or subcutaneous tissue toward the wound” |
1 and |
Penington (2) paras 49-52 CB 4/36/0468. Stacey (1) paras 97-98, 148, 149 CB 4/42/0568,0578,0579. |
Marshall (1) paras 51, 52, 103 CB 3/26/0255,0267. Marshall (2) paras 15, 36 CB 3/27/0292,0296. Pohl paras 157, 159, 192 CB 3/33/0390,0391,0399. |
|
“time sufficient to facilitate closure of thewound” |
1 and |
Penington (2) paras 53-55 CB 4/36/0469. Stacey (1) paras 99-100, 150, 151 CB 4/42/0568,0579. |
Marshall (1) paras 52, 68, 71, 104, 115 CB 3/26/0255,0259,0268,0270. Marshall (2) para 37 CB 3/27/0296. Pohl paras 165, 192 CB 3/33/0392,0399. |
|
“time sufficient to permit the formation of granulation tissue in the wound” |
2 |
Stacey (1) para 101 CB 4/42/0569. |
Marshall (1) paras 76, 106, 193 CB 3/26/0260,0268,0284. |
|
“maintaining said reduced pressure until the wound has progressed toward a selected stage of healing” |
121 |
Stacey (1) para 119 CB 4/42/0572. Penington (3) paras 11(b), 17(d) CB 4/37/0500,0508. |
Marshall (1) – no evidence on “selected stage of healing” Pohl paras 213, 218(l), 222(i) CB 3/33/0403,0406,0408. |
808 In General Tire, the Court of Appeal stated at 167 that:
... the issue of definition is to be considered as a practical matter and little weight is to be given to puzzles set out at the edge of the claim which would not as a practical matter cause difficulty to a manufacturer wishing to satisfy [itself] that [it] is not infringing the patent.
809 In General Tire, the Court of Appeal further observed that the court is not required to strain to uphold the patent, but allowances should be made for any difficulties of the case, so an alleged issue of want of definition should always be considered in relation to the particular facts.
810 The Court of Appeal also approved the statement of Shaw LJ in British Thomson-Houston Company Ltd v Corona Lamp Works Ltd (1922) 39 RPC 49 at 89 that:
It is easy, whenever language of generality and relativity applicable to size, measure, weight or the like have been employed, to put puzzles which might indicate that, at certain points, you are at that thin strip of mechanical territory in which, on the one side, there might be failure, and, on the other, success. But the reply to such criticism is that that is not how practical men work. They work to achieve success, and if, adopting the broad lines laid down in a specification, they do not find any real difficulty in achieving success, this may not conclude the matter, but it goes far to show that the vagueness of the specification has not mislead them – practical people who were not seeking for failure but for success – has not caused the invention to fail to reach their mind, but has, on the contrary, for all practical purposes, guided them, and that without difficulty, towards the success which prior to that no experiment nor invention had achieved.
811 I have already considered in detail many of the terms and integers challenged by S&N under this heading in other contexts. The screen rigidity integer, in my view, lacked inherent meaning, and as it was common to all claims, they did not define the specification. Save for the screen rigidity integer, as a “practical matter”, with “due allowance for the difficulties of the case”, in my opinion, the impugned terms were not so vague or wanting in particularity as to fail to comply with 40(2)(b) of the Act.
Lack of clarity
812 S&N also alleged that the Patent did not comply with s 40(3), as a number of the claims lacked clarity due to the inclusion of purported limitations.
813 In Kimberly-Clark Australia Pty Ltd v Arico Trading International Pty Ltd & Ors (1998) 42 IPR 111, Burchett J observed that there was no requirement that “only exact expressions” be employed (at 119). His Honour concluded (at 120):
A patentee does not, as Dixon CJ made clear in Martin v Scribal Pty Ltd (1954) 92 CLR 17 at 60, have to express his claim with a precision that “must be but an arbitrary restriction on the inherent variability of [a] feature” which is part of the invention.
814 In Minnesota Mining, Aickin J stated at 274 that:
Lack of precise definition in claims is not fatal to their validity so long as they provide a workable standard suitable to the intended use.
815 In Nesbit Evans Group Australia Pty Ltd v Impro Ltd (1997) 39 IPR 56, Lindgren J (with whom Hill J agreed) stated at 95 that claims which provide a workable standard suitable to their intended use do not lack clarity merely because they may require an exercise of judgment by the person skilled in the art. His Honour stated:
[I]t is not unusual for a claim to define an invention partly by the use of a relative expression which necessitates exercise of judgment… and so long as the claims provide a workable standard suitable to the intended use, they will be valid… The expressions in question must be understood in a practical, common sense manner.
816 In DÉcor, Lockhart J described lack of clarity in the context of s 40 at 395 as “vagueness of description, want of particularity and evident indistinctness of thought may be the source of so much uncertainty as to the scope of the monopoly that the claim fails to fulfil the requirement of stating with definiteness to what the patentee is exclusively entitled” (Kauzal v Lee (1936) 58 CLR 670 at 685)).
817 Lockhart J acknowledged (at 395) that the expression “open mouthed container” in DÉcor was general and that many containers would answer the description, but the term was not ambiguous. He reiterated Aickin J’s statement in Minnesota Mining at 274 that “[l]ack of precise definition in claims is not fatal to their validity so long as they provide a workable standard suitable to the intended use”.
818 S&N conceded that unclear claim terms may be defined or clarified by reference to the body of the specification and that a “purposive”, common sense approach to what the words used convey in the context of the published knowledge as at the priority date was required.
819 S&N also acknowledged that an invention may be described in a way that involves matters of degree. The consideration is whether, on any reasonable view, the claim has meaning. Where a claim includes a vague word or phrase which not defined in the body of the specification, it is a question of fact, to be determined on the evidence, whether it renders the claim invalid for ambiguity. Blanco White, Patents for Inventions (5th ed, Stevens & Sons, 1983) at 4-701 states that:
…a claim is bad if no reasonably certain construction can be given to it, or it is fairly and equally open to diverse meanings. But the rule goes further than this. A court is not bound to find a meaning for a claim, nor to approach a claim with the "conviction that its language is capable of a reasonable construction when carefully examined" that is the due of an Act of Parliament. Thus a claim may be bad for uncertainty although the court could find its true meaning (and would do so if the words concerned appeared in a commercial contract) if it is so obscure that "its proper construction must always remain a matter of doubt"…
(emphasis added)
820 S&N also conceded that courts typically approach the standard of clarity required with leniency, but submitted that the present case was akin to Flexible Steel Lacing Company v Beltreco Ltd & Anor (2000) 49 IPR 331, where Hely J held that method and product claims for pulley lagging used in conveyor systems were invalid for lack of clarity. Hely J stated at 355 and 359-360:
Given the equivocations in the drawings, they do not resolve the puzzle created by the uncertainties and inconsistencies in the text. The method claim is fairly open to more than one meaning not because of grammatical problems but because, even to a skilled reader, it would not be clear which of two methods [it] describes. That problem cannot be overcome by the expectation on the part of a skilled worker, to which I earlier referred…
…
[T]he product claim is obscure; it is fairly and equally open to diverse meanings… Another possibility is that the claim embraces both. Sometimes, ambiguity or insufficiency in description can be resolved by a skilled addressee through the application of commonsense and common knowledge… I do not think that this is such a case.
(emphasis added)
821 S&N also relied on High Tech Auto Tools Pty Ltd v Ferocem Pty Ltd (1994) 29 IPR 337, where JM Sellars (Delegate of the Commissioner of Patents) held that the use of certain expressions in the claims rendered them unclear or uncertain in scope, and Abbott Laboratories & Anor v Corbridge Group Pty Ltd & Anor (2002) 57 IPR 432 at 449, where the Full Court (Lee, Emmett and Hely JJ) held that an inter-claim referencing error led to a nonsensical result and a lack of clarity.
822 Lord Loreburn LC in Natural Color Kinematograph Co v Bioschemes Ltd (1915) 32 RPC 256 (“Bioschemes”) at 266 stated:
It is the duty of a patentee to state clearly and distinctly, either in direct words or by clear and distinct reference, the nature and limits of what he claims. If he uses language which, when fairly read, is avoidably obscure or ambiguous, the patent is invalid, whether the defect be due to design, or to carelessness, or to want of skill.
823 In Martin v Scribal Pty Ltd (1954) 92 CLR 17 at 59, Dixon CJ adopted the following description of the duty of the court and the test of ambiguity from the judgment of Lord Parker in Bioschemes:
Further, though it may be true that in construing an instrument inter partes the court is bound to make up its mind as to the true meaning, this is far from being the case with a Specification. It is open to the court to conclude that the terms of a Specification are so ambiguous that its proper construction must always remain a matter of doubt, and in such a case, even if the Specification had been prepared in perfect good faith, the duty of the court would be to declare the Patent void…
824 Although I was not persuaded that most of the above impugned terminology presented any irresolvable ambiguity, abiding uncertainty or doubt (particularly when the specification was read as a whole), as discussed in detail above, the screen rigidity integer lacked inherent meaning even to a skilled reader, who would not have known what dressing to select. Its obscurity and uncertainty could not be rectified by reference to the specification, where the same deficiencies characterised the discussion of the integer. As the screen rigidity integer was common to all claims in suit, its obscurity, uncertainty and lack of cogent meaning rendered them all relevantly unclear. Therefore, in my opinion, the claims were invalid on the ground that they lacked clarity as required by s 40(3) of the Act.
Fair basis
825 S&N alleged that the claims in suit were not fairly based on the matter described in the specification, as required by s 40(3) of the Act.
826 S&N alleged that a number of claims were purportedly limited by integers that were not described in the specification as part of the invention. In terms of Lockwood No 2, they purported to define the invention by mere stray phrases in the specification and lacked a real and reasonably clear disclosure. The integers were:
(a) claims 9 and 121: cyclical application of pressure;
(b) claim 8: continuous application of pressure;
(c) claims 1, 2, 6, 7 and 121: period of pressure application;
(d) claim 3: type of wound; and
(e) claims 10, 11 and 12: ratio of cyclical pressure application.
827 S&N submitted that the inclusion in claims 50 and 52 of a “singular tubular member having a first end inserted beneath at least a portion of the foam section” was not disclosed by the specification, which described a tube or hose being inserted “into” the foam but not the tube or hose being inserted “beneath” the foam. Alternatively, the claims travelled beyond the matter described in the specification, contrary to the principles expressed in Lockwood No 2.
828 S&N submitted that the claims regarding a “fluid-impermeable seal/cover” in claims 49 and 50 were not disclosed in the specification, which did not refer to the use of a seal or cover which was fluid-impermeable. Alternatively, the relevant claims travelled beyond the matter described in the specification, in which the description of the “seal” did not include the words “fluid-impermeable”.
829 S&N submitted that the specification did not include a real and reasonably clear description or disclosure of the ratios in claims 10, 11 and 12, which referred to “at least” a specified ratio. Alternatively, the claims travelled beyond the matter described in the specification, as the specification specified “as low as 1:10 or as high as 10:1”, while the claims used “at least 10:1”, thus including a ratio higher than 10:1 (eg 20:1 or indeed 100:1, and so on).
830 In CCOM Pty Ltd v Jiejing Pty Ltd (1994) 51 FCR 260, the Full Federal Court stated at 436 that it is not appropriate to adopt “an over meticulous verbal analysis”. The Full Court stated at 437:
... it is wrong to proceed as if testing for infringement and to seek to isolate in the body of the complete specification, or in the provisional specification, "essential integers" or "essential features" of an invention disclosed therein and to ask whether they correspond with the essential integers in the claim in question... Nor would it be applying the statute to ask whether the earlier specifications fairly described the essential features of the invention disclosed in the later specification...
831 On that basis, I was not persuaded that the above impugned integers were not fairly based on matter described in the specification.
conclusion
832 In my opinion, the application should be dismissed and the cross-claim should be allowed. I shall invite submissions on the form of orders and costs.
|
I certify that the preceding eight hundred and thirty-two (832) numbered paragraphs are a true copy of the Reasons for Judgment herein of the Honourable Justice Dodds-Streeton. |
Associate:

