
FEDERAL COURT OF AUSTRALIA
AstraZeneca Pty Ltd v GlaxoSmithKline Australia Pty Ltd [2005] FCA 1645
TRADE PRACTICES – Consumer Protection – Misleading or Deceptive Conduct – False Representations – where pharmaceutical company used ‘Total Control’ slogan in asthma drug advertising – where advertisements footnoted or quoted scientific study – where relevant consumer group prescribing General Practitioners – whether contravention of Part V, Trade Practices Act 1974 (Cth)
Taco Co of Australia Inc v Taco Bell Pty Ltd (1982) 42 ALR 177, applied
Campomar Sociedad Limitada v Nike International Ltd (2000) 202 CLR 45, applied
Parkdale Custombuilt Furniture Pty Ltd v Puxu Pty Ltd (1982) 149 CLR 191, applied
Johnson Tiles Pty Ltd v Esso Australia Ltd (2000) 104 FCR 564 , applied
ASTRAZENECA PTY LIMITED v GLAXOSMITHKLINE AUSTRALIA PTY LIMITED
NSD 707 OF 2005
EDMONDS J
16 NOVEMBER 2005
SYDNEY
|
IN THE FEDERAL COURT OF AUSTRALIA |
|
|
NEW SOUTH WALES DISTRICT REGISTRY |
NSD 707 OF 2005 |
|
BETWEEN: |
ASTRAZENECA PTY LIMITED APPLICANT
|
|
AND: |
GLAXOSMITHKLINE AUSTRALIA PTY LIMITED RESPONDENT
|
|
EDMONDS J |
|
|
DATE OF ORDER: |
16 NOVEMBER 2005 |
|
WHERE MADE: |
SYDNEY |
THE COURT ORDERS THAT:
1. The application be dismissed.
2. The applicant pay the respondent’s costs.
Note: Settlement and entry of orders is dealt with in Order 36 of the Federal Court Rules.
|
IN THE FEDERAL COURT OF AUSTRALIA |
|
|
NEW SOUTH WALES DISTRICT REGISTRY |
NSD 707 OF 2005 |
|
BETWEEN: |
APPLICANT
|
|
AND: |
GLAXOSMITHKLINE AUSTRALIA PTY LIMITED RESPONDENT
|
|
JUDGE: |
|
|
DATE: |
16 NOVEMBER 2005 |
|
PLACE: |
SYDNEY |
REASONS FOR JUDGMENT
Edmonds J:
1 The applicant, AstraZeneca Pty Limited (‘AstraZeneca’), is an Australian company and a member of the AstraZeneca Group, a Swedish-English global pharmaceutical company. AstraZeneca manufacturers and markets in Australia a range of therapeutic products including medications for the control of the symptoms of asthma.
2 The respondent, GlaxoSmithKline Australia Pty Limited (‘GSK’), is also an Australian company and a member of the global GlaxoSmithKline Group. GSK also manufactures and markets in Australia a range of therapeutic and other health care products including medications for the control of the symptoms of asthma. Its leading medication is sold under the brand name ‘Seretide’.
THE PROCEEDINGS
3 AstraZeneca has brought proceedings in this Court, in reliance on the jurisdiction conferred by s 86 of the Trade Practices Act 1974 (Cth) (‘the Act’) for injunctive, pecuniary and other relief flowing from representations alleged to have been made in contravention of Part V of the Act.
4 These proceedings arise out of publication by GSK of various representations in certain advertising, marketing and promotional material concerning Seretide. AstraZeneca contends that the publication of this material constitutes misleading or deceptive conduct contrary to s 52(1) of the Act and also constitutes the making of representations that Seretide has benefits it does not have in contravention of s 53(c) of the Act. The advertising, marketing and promotional material said to contain the representations which contravened the provisions of the Act consists of the following items (hereinafter together called ‘the Seretide Advertisements’):
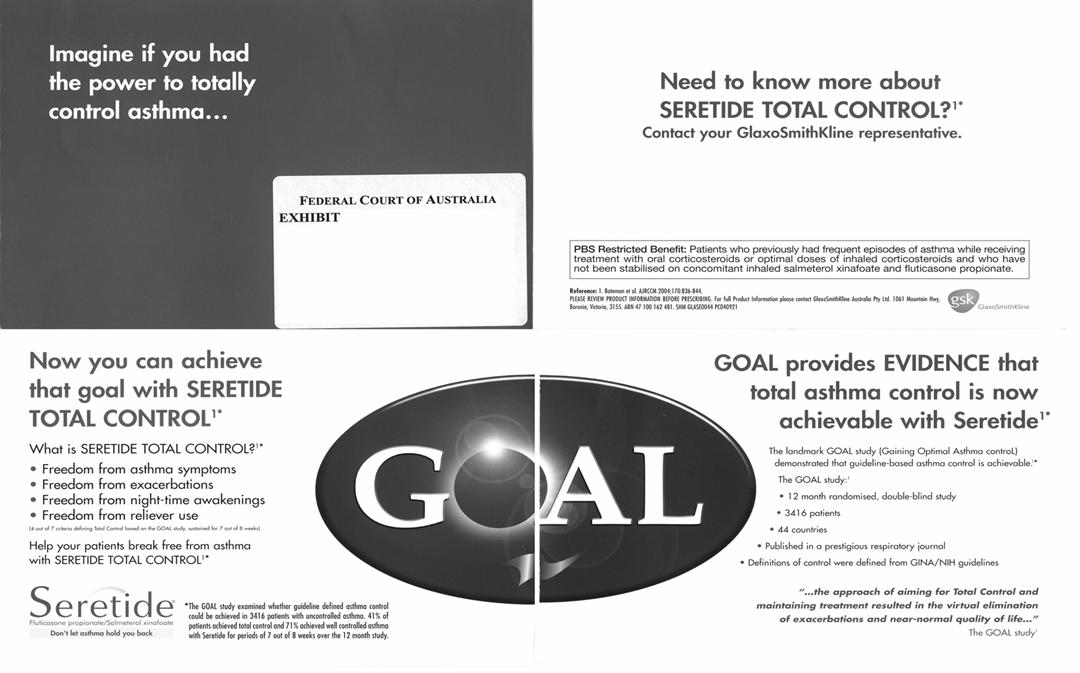
(1) What is referred to in the evidence as the GOAL Mailer, a four page pamphlet, the front page of which reads: ‘Imagine if you had the power to totally control asthma …’ depicted in Fig. 1.
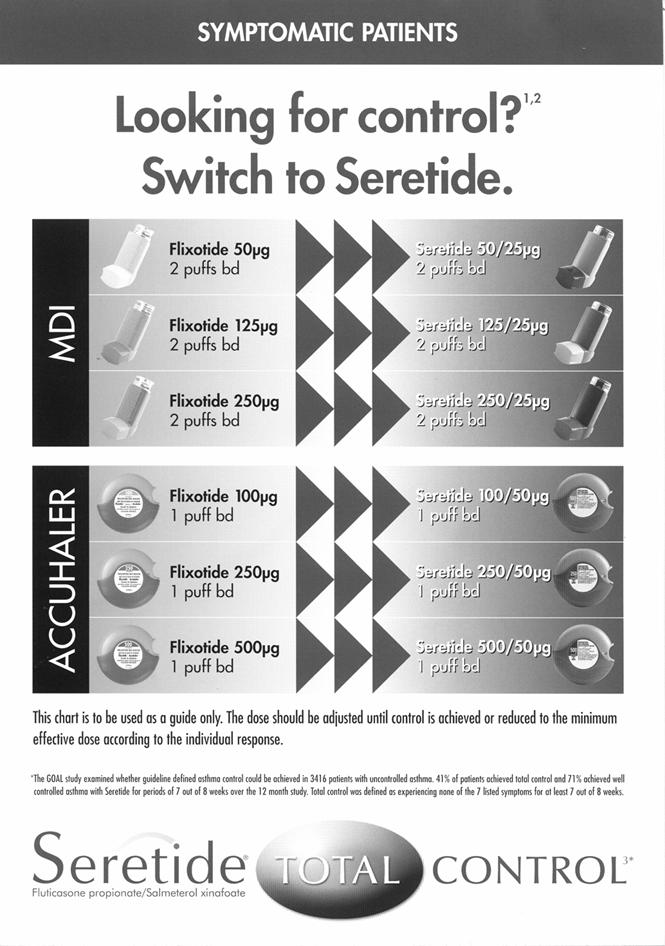
(2) What is referred to in the evidence as the sales aid given by GSK representatives to GPs headed on one side ‘Symptomatic Patients’ – ‘Looking for control?1,2 Switch to Seretide’ depicted in Fig. 2.
(3) What is referred to in the evidence as ‘the sleeping man’ advertisement depicted in Fig. 3.
(4) What is referred to in the evidence as ‘the upgrade’ advertisement depicted in Fig. 4.

5 AstraZeneca seeks an injunction restraining GSK by itself, its directors, its employees or agents at any time in the future from:
(a) Publishing any of the Seretide Advertisements.
(b) In any advertising, marketing or promotional material for the product Seretide:
(i) using the phrase ‘Seretide Total Control’;
(ii) referring to the GOAL Study unless accurate reference is made to the primary end point, the key features of the study design (including the three patient strata) and any reference to cumulative figures is omitted.
It also seeks delivery up on oath to AstraZeneca, or its duly authorised agents for destruction under supervision all advertisements, posters, pamphlets, brochures, materials or other means of communication or documents of any nature in GSK’s possession, power, custody or control which is substantially in the form of the Seretide Advertisements. Finally, it seeks an order that GSK undertake corrective advertising in a manner to be agreed or ordered by the Court.
6 AstraZeneca’s application originally claimed damages; however, this was abandoned at the commencement of the hearing.
AstraZeneca’s Statement of Claim and GSK’s Defence
7 In its Statement of Claim, AstraZeneca claims that in each of the Seretide Advertisements, GSK made representations to the following effect:
(1) that all or virtually all asthma patients will achieve 100% control or total control of all asthma symptoms by using Seretide;
(2) alternatively, that a majority (i.e. greater than 50%) of all asthma patients will achieve 100% control or total control of all asthma symptoms by using Seretide;
(3) alternatively, that a sufficiently high proportion of all asthma patients will achieve 100% control or total control of all asthma symptoms by using Seretide to justify the use of the brand slogan ‘Seretide Total Control’;
(4) that 41 % of all patients taking part in the study known as the ‘Gaining Optimal Asthma Control’ study published in the American Journal of Respiratory & Critical Care Medicine in 2004 (GOAL Study) achieved 100% control of all asthma symptoms by using Seretide;
(5) alternatively, that 41 % of all patients taking part in the GOAL Study achieved ‘total control’ (as that term is defined in the Seretide Advertisements) of all asthma symptoms by using Seretide;
(6) that 71 % of all patients taking part in the GOAL Study achieved ‘well controlled asthma’ (as that term is defined in the Seretide Advertisements) of all asthma symptoms by using Seretide; and
(7) that the patient results of the GOAL Study identified in pars (4), (5) and (6) (sic) will be achieved or will be likely to be achieved in clinical practice.
(hereinafter together called ‘the Representations’).
8 In its Defence, GSK denied that it made the Representations. In written submissions, it contended that:
(1) The representations pleaded at pars (1) to (3) of [57] are not made expressly in any of the Seretide Advertisements. If they arise, they can only arise by implication considering each of the Seretide Advertisements as a whole.
(2) The representation pleaded at par (4) is in part true, but as to the latter part is not express and can only arise by implication.
(3) The representations pleaded at pars (5) and (6) are literally true – the case that these representations are misleading or deceptive depends upon what is not said.
(4) The representation pleaded at par (7) is not made expressly in any of the Seretide Advertisements; it depends on implication arising from the whole of each of the Seretide Advertisements. The GOAL Study makes it clear that clinicians might not replicate its conditions; the case that the representation is misleading or deceptive depends upon what is not said.
9 In its Statement of Claim, AstraZeneca claims that the Representations were misleading and deceptive or likely to mislead and deceive, in that:
(1) the majority (ie greater than 50%) of all patients across all strata identified in the GOAL Study did not achieve ‘total control’ (as that term is defined in the GOAL Study) from all asthma symptoms at the conclusion of the testing;
(2) a sufficiently high proportion of patients in the GOAL Study did not achieve 100% control or total control from all asthma symptoms to justify the use of the brand slogan ‘Seretide Total Control’;
(3) the definition of the term ‘total control’ as found in the GOAL Study is not replicated in the Seretide Advertisements;
(4) the definition of the term ‘well controlled asthma’ as found in the GOAL Study is not replicated in the Seretide Advertisements;
(5) the figures employed in the disclaimer to each of the Seretide Advertisements represent cumulative results across all strata identified in the GOAL Study and in the absence of identifying the three different strata of patients with differing levels of asthma and differing responses to treatment as found in the GOAL Study, the Seretide Advertisements do not accurately represent the findings of the GOAL Study for the purposes of prescribing medical practitioners;
(6) one of the three strata (referred to as strata 1) in the GOAL Study, being the strata with the highest rates of totally controlled and well controlled asthma for patients with no use of inhaled corticosteroids in the previous six months, does not fall within the PBS Restricted Benefit as specified in the Seretide Advertisements;
(7) the disclaimers to each of the Seretide Advertisements do not identify that the GOAL Study was undertaken over two distinct phases, with specific patient compliance requirements for each of those phases which is material to the outcome of the testing;
(8) it is unlikely that patients in clinical practice would achieve similar results to patients in the GOAL Study and the Seretide Advertisements do not identify this; and
(9) The GOAL Study trial participants were a selected group who were more likely to be compliant in that they did not include any patients with significant concomitant diseases, or smokers of more than 10 pack-years, or patients under 12 years of age, and the Seretide Advertisements do not identify this.
10 In its Defence, GSK denied each of these matters and answered as follows:
(1) the Representations were not made in the Seretide Advertisements; but
(2) even if any of the Representations were made, no reasonable member of the class of prospective readers of the Seretide Advertisements, being general medical practitioners and respiratory specialists, would have been misled or deceived or likely to have been misled or deceived.
11 Finally, AstraZeneca claimed, further or alternatively, that GSK represented that Seretide had benefits it did not have in contravention of s 53(c) of the Act which GSK, in its Defence, denied.
The Evidence
12 In support of its case, AstraZeneca relied on evidence from Dr Glen Pater and Dr Matthew Peters. Both witnesses were required for cross-examination.
13 In support of its case, GSK relied on evidence from Professor David Barnes, Dr Michael Elliott and Dr Stephen Howe. Professor Barnes was not required for cross-examination but Drs Elliott and Howe were.
14 Chronologically, it is convenient to first deal with the evidence of Dr Elliott, who is the Medical Director of GSK and a Vice-President of the GlaxoSmithKline group of companies.
Dr Elliott
15 GSK has sold Seretide in Australia since July 2000. It was first sold into pharmacies at that time to ensure stock was available at the time the medication obtained Pharmaceutical Benefits Scheme (‘PBS’) listing on 1 August 2000.
16 Seretide is a combination therapy – it contains two active components, the generic names of which are fluticasone propionate and salmeterol xinafoate. It is supplied by GSK in a number of dosages in either a metered dose inhaler (50/25, 125/25 or 250/25) or in a dry powder Accuhaler® (100/50, 250/50 or 500/50).
17 Seretide is only available for use by patients on prescription.
18 There is only one other combination therapy for asthma on the market in Australia and that is AstraZeneca’s product ‘Symbicort’ which came onto the market in Australia in about April 2003.
Asthma and its Treatment
19 Asthma is a condition which has no known cure. All asthma medications are directed toward the management or control of the symptoms and inflammation of asthma.
20 Asthma medications can be placed in the following categories:
(2) Reliever medications – which are used by patients to relieve acute symptoms as they are experienced. These first came on the market in Australia in about 1967. GSK’s reliever medication of this type is called ‘Ventolin’ (salbutamol sulfate). AstraZeneca’s reliever medication of this type is called ‘Bricanyl’ (terbutaline sulfate).
(3) Corticosteroids – which are anti-inflammatory medications which, in contrast to reliever medications are intended to be taken regularly as a means to the prevention of asthma symptoms by treating the underlying inflammation. These first came on the market in Australia in about 1995. GSK’s corticosteroid medication is called ‘Flixotide’ (fluticasone propionate). AstraZeneca’s corticosteroid medication is called ‘Pulmicort’ (budesonide).
(4) Long acting reliever medications (known as LABA’s) – developed subsequent to the reliever medications referred to in (1) above. LABAs operate in the same way as reliever medications but are taken prophylactically like corticosteroids rather than in response to a symptom. LABAs first came on the market in Australia in about 1995. GSK’s LABA medication is called ‘Serevent’ (slameterol xinfoate). AstraZeneca’s LABA medication is called “Oxis’ (eformoterol fumarate dihydrate).
(5) Combination therapies being a combination of a corticosteroid and a LABA. The first of these was GSK’s Seretide which was followed by AstraZeneca’s Symbicort.
Seretide Sales
21 Between 1 July 2000 and the date upon which AstraZeneca began selling Symbicort, in approximately January 2003, Seretide was the only combination therapy drug on the market. During this time, GSK sold approximately 4,279,793 units of Seretide.
22 Between January 2003 when AstraZeneca’s product Symbicort began being sold and July 2004, GSK sold approximately 4,025,774 units of Seretide. During the same period AstraZeneca sold approximately 413,974 units of Symbicort.
23 Between 1 August 2004 and 31 March 2005 GSK sold approximately 1,794,499 units of Seretide. During the same period AstraZeneca sold approximately 322,593 units of Symbicort.
Asthma Control Studies
24 As asthma medications are directed at the control of the underlying inflammation and symptoms of asthma rather than the achievement of a cure, much attention is given by doctors to the management of the ongoing use of various drugs. This is predominantly due to doctors being wary of side effects associated with long term use of medications.
25 Peak asthma advisory bodies around the world use and maintain guidelines concerning the treatment and control of asthma.
26 In recent years studies have been undertaken to determine the actual level of asthma control being achieved by asthma sufferers in comparison to guideline defined asthma control.
27 In 2000, K.F. Rabe published an article in the European Respiratory Journal entitled ‘Clinical management of asthma in 1999: the Asthma Insights and Reality in Europe (AIRE) study’. The AIRE study examined asthma management in 2803 patients across Europe and demonstrated that only 5.3 per cent of patients achieved guideline defined asthma control.
28 In 2001, E. D Bateman published an article in the same journal entitled ‘Is overall asthma control being achieved? A hypothesis generating study’. It reported a study that ‘demonstrated that asthma control, as defined by management guidelines, is achievable ... . This was a hypothesis generating study upon which further prospective studies should be based’(at p 594). The study referred to another study, then underway, designed to assess the proportion of patients able to achieve guideline defined control of asthma.
29 On or about 15 July 2004 the results of the further study referred to in the 2001 article were published (initially online and subsequently in an article in the American Journal of Respiratory and Critical Care Medicine Volume 170) entitled ‘The Gaining Optimal Asthma Control Study’ (‘the GOAL Study’).
30 The GOAL study assessed whether guideline defined asthma control is a realistic target. The study was a one-year randomised, stratified, double-blind, parallel group of 3416 patients with uncontrolled asthma. This design is the most rigorous way of assessing the efficacy and safety of a medicine. The medications used throughout the study were GSK’s medications, Seretide and Flixotide.
31 The italicized terms in [30] are defined as follows:
(a) One-year - patients were involved in the study for a 52 week period. Asthma studies conducted prior to the GOAL study generally involved a 12 to 24 week study period.
(b) Randomised - a method whereby the investigators randomly allocate patients who are eligible to enter the study (that is, after the run-in period) into groups to receive one or more of the study medications. In the GOAL study, patients were randomised to receive either Seretide or Flixotide for the 52 week study period.
(c) Stratified - a method whereby patients are allocated to different groups. In the GOAL study, patients who were recruited were allocated to three groups/strata according to their medication during the six months prior to entering the study. Using a stratified system allowed patients to be allocated a starting dose of Seretide or Flixotide appropriate to their current asthma status. Stratification occurred during the run-in period.
(d) Run-in period - the period before the trial is commenced and patients are not given any study medication. In the GOAL study, patients remained on their usual medication and were assessed to determine whether they had uncontrolled asthma. Only patients who had uncontrolled asthma were deemed eligible to enter the 52 week study.
(e) Double blind - neither the investigator nor the patient are aware of the study medication given to the patient. In the GOAL study, patients were given two dry powder Accuhalers; one containing an active ingredient, the other containing placebo. The purpose of double blinding is to prevent performance bias.
(f) Parallel group - atrial that compares two groups of people, often one group receives the study drug and the other (the control group) receives a placebo or, as with the GOAL Study, both groups receive a study medication i.e. Flixotide or Seretide. Neither group received a placebo during the GOAL Study.
32 The GOAL study was the first of its kind as it was conducted over a much longer period of time than previous studies and a significantly greater number of asthma sufferers participated.
33 The GOAL study utilised two guideline based measures of asthma control referred to as ‘total control’ and ‘well controlled’ asthma. Both these definitions were based on the Global Initiative for Asthma (‘GINA’) and the National Institutes of Health (‘NIH’) guidelines.
34 The criteria for being defined as having ‘total control’ or ‘well controlled’ asthma in the GOAL Study were as follows:
|
|
Total Control |
Well Controlled |
|
|
(All of the following 7 criteria) |
(2 or more of the following 3 criteria) |
|
1. |
No daily symptoms |
Minimal symptoms of <_ 2 days per week |
|
2. |
No salbutamol use |
Minimal salbutamol use on , 2 days per week and < _4 occasions per week |
|
3. |
Daily a.m. PEF of >_80% predicted |
Daily a.m. PEF of >_ 80% predicted |
|
|
|
(All of the following 4 criteria) |
|
4. |
No night-time awakenings |
No asthma night-time awakenings |
|
5. |
No exacerbations |
No exacerbations |
|
6. |
No emergency visits |
No emergency visits |
|
7. |
No treatment-related adverse events enforcing change in therapy |
No treatment-related adverse events enforcing change in therapy |
35 The GOAL Study showed that out of the study group of 3,421 patients, as divided into three stratum (based on asthma severity), total control was achieved using Seretide as follows:
|
|
Phase 1 |
Phase 2 |
|
Stratum 1 |
42% |
50% |
|
Stratum 2 |
32% |
44% |
|
Stratum 3 |
19% |
29% |
Accordingly, by the end of the year long study, 41% of participants in the study had achieved GOAL defined total control.
GSK’s Advertising
36 GSK began advertising the product Seretide in approximately August 2000 upon its listing on the PBS.
37 The marketing of Seretide, although continuous, can be broken into 3 phases being:
(1) from PBS listing to the publication of the GOAL Study;
(2) from publication of the GOAL Study to November 2004; and then
(3) from November 2004 to date.
Phase (1)
38 The initial advertising for Seretide during phase (1) included the following advertisements:
(a) ‘The right combination’;
(b) ‘Give asthma both barrels’;
(c) ‘Choose your weapon, choose your strength’;
(d) ‘Control asthma night and day’;
(e) ‘Give your asthma patients around the clock control’;
(f) ‘Don't let asthma hold you back’;
(g) ‘Control asthma through the night’;
(h) ‘Control a little asthma with a little Seretide’;
(i) ‘Make a little steroid go a long way’;
(j) ‘Control asthma like never before’;
(k) ‘With Seretide, your asthma patients can get up and go’;
(l) ‘3 strengths, 2 devices, 1 combination’.
39 The target audience for these advertisements and others during this period, and with all later Seretide advertising, were General Practitioners (‘GPs’).
40 Preparation for the launch of the GOAL Study began in or about February 2004 including GSK organising events such as the Landmark Symposium for GPs on 22 February 2004 in Melbourne to introduce them to the GOAL Study and share with them the available results of the Study at that time. 180 Respiratory and General Physicians attended the Landmark Symposium.
41 Other presentations were also given between February 2004 and the release of the GOAL Study in July 2004 as part of the preparation for the launch of the study. These included 300 GPs attending GSK’s Satellite Symposium entitled ‘Asthma Control – Moving the Goalposts’ which was part of the International Primary Care Respiratory Group (‘IPCRG’) 2nd World Conference in Melbourne from 19 – 22 February 2004.
42 Between 24 and 26 February 2004, GSK also organised a further seven meetings occurring in Sydney, Adelaide, Brisbane, Perth and Melbourne to assist in the launch of the GOAL Study.
Phase (2)
43 After the publication of the results of the GOAL Study on the internet, GSK commenced phase (2) of its Seretide marketing campaign on or about 1 August 2004.
44 GSK’s advertising campaigns at that time included the dissemination of information and printed material through the company’s sales representatives (assisted by printed sales aids) as well as printed advertisements in medical journals and tabloid medical magazines and further, through hosting educational workshops and meetings. Copies of the advertisements used during what I have referred to as phase (2) are referred to in the paragraphs below and include GSK’s ‘Asthma? What asthma?’ campaign.
45 In Australia, GPs must complete a total of 60 group 1 ‘continuing education’ points every three years in order to maintain their registration. As part of its promotion of the GOAL Study, GSK organised a number of education sessions referred to as ‘AIM’ workshops which were designed to provide GPs with an appreciation of the impact of poorly controlled asthma in Australia and guidance on best practice detection and management of asthma in primary care. Attendance at these sessions gave practitioners 30 out of the 60 required education points.
46 The AIM workshops were lead by independent respiratory specialists between August 2004 and December 2004. A total of 1,258 GPs were educated in the AIM workshops about the GOAL Study and the meaning of total control during that time.
47 The educational materials used in the AIM workshops were prepared by Adrenalin Strategics Pty Ltd, a medical education development company in conjunction with GSK. These educational materials must be reviewed and approved by the Royal Australian College of General Practitioners (‘RACGP’) who allocate and manage the continuing educational points. These materials included among other things, the Study Guide, the Participant’s Workbook and the Facilitator’s Guide for the AIM workshops. Each refer to ‘Total Asthma Control’ and the GOAL Study.
48 Further AIM workshops have been held in February, March and April 2005, and to date 1600 more GPs have been trained in the workshops.
49 In addition to the above, from September 2004 to December 2004, an AIM Survey was undertaken and used to assist practitioners identify patients who were not achieving optimal levels of control and help them to aim for total control. A total of 512 GPs were enrolled in the survey. Those GPs who participated in the survey were different to those GPs who participated in the AIM workshops.
50 GSK’s ‘Asthma? What asthma?’ advertising campaign began in August 2004. In September 2004 GSK’s ‘Asthma? What asthma?’ campaign was amended to incorporate the results of the GOAL Study.
51 The ‘Asthma? What asthma?’ campaign was run by GSK in medical tabloids and journals from September 2004 including Australian Doctor magazine, Medical Observer magazine, Rural Doctor magazine with a circulation of 5,100 and MIMs bi-monthly publication with a circulation of 25,000. The Australian Doctor magazine is a weekly publication with a circulation of 23,738 while the Medical Observer magazine is also a weekly publication and has a circulation of 24,823. Each publication is circulated to GPs, specialists and other miscellaneous subscribers.
52 The target audience for the ‘Asthma? What asthma?’ advertising campaign was, as with earlier advertising, GPs.
Phase (3)
53 On or about November 2004 GSK commenced its ‘Total Control’ campaign.
54 As part of the ‘Total Control’ campaign, on 26 November 2004 GSK undertook a mail out to 14,000 GPs (approximately 70.7 per cent of the doctor population in Australia) informing them of the GOAL study and total control. This mail out was referred to by GSK as the GOAL Mailer. The GOAL Mailer is one of the four publications in respect of which AstraZeneca seeks injunctive and other relief: see [4(1)], supra, Fig. 1.
55 Also on 26 November 2004 GSK undertook a further mail out to a further 4,200 GPs with higher volumes of asthma patients. This mail out was referred to by GSK as the Glaxo Mailer.
56 All GPs received either the Glaxo Mailer or the GOAL Mailer.
57 On 26 November 2004 GSK also ran a competition (for GPs to win a stethoscope) to further enhance GPs’ understanding of GOAL and total control referred to as the Beecham Competition. For this competition, 6,200 entry forms were printed and delivered to GPs by GSK’s sales representatives. Nationally, 747 GPs entered into this competition.
58 On or about 1 January 2005, GSK added a further aspect to its ‘Total Control’ campaign to include the logo ‘Seretide Total Control’ with the word ‘Total’ appearing within an ellipse in a similar format as that previously used by GSK to advertise GOAL. In every execution of this logo, GSK has referenced the logo to the GOAL study and the qualifier set out below:
‘The GOAL study examined whether guideline defined asthma control could be achieved in 3416 patients with uncontrolled asthma. 41% of patients achieved total control and 71% achieved well controlled asthma with Seretide for periods of 7 out of 8 weeks over the 12 month study. Total control was defined as experiencing none of the 7 listed symptoms for at least 7 out of 8 weeks.’
59 The first appearance of the ‘Seretide Total Control’ logo occurred in the sales aid used by GSK’s sales representatives from February 2005. The sales aid is one of the four publications in respect of which AstraZeneca seeks injunctive and other relief: see [4(2)], supra, Fig. 2.
60 GSK’s first use in any magazine of the logo ‘Seretide Total Control’ occurred in the upgrade advertisement in the 20 March 2005 issue of Australian Doctor magazine. This advertisement is one of the four publications in respect of which AstraZeneca seeks injunctive and other relief: see [4(4)], supra, Fig. 4.
61 Subsequent appearances of this advertisement were made in Australian Doctor magazine and the Medical Observer magazine issues dated 1 April 2005 and thenagain in the Medicine Today publication for April 2005.
62 GSK’s advertisement entitled ‘Seretide Total Control’ depicting the sleeping man was also first used in the 20 March 2005 issue of Australian Doctor magazine. This advertisement is one of the four publications in respect of which AstraZeneca seeks injunctive and other relief: see [4(3)], supra, Fig. 3.
63 Dr Elliott was cross-examined but apart from admitting that within GSK it was he who bore ultimate responsibility for the consent of advertisements and that the GOAL Mailer would be part of the education and information base of a GP, his cross-examination did little to shed light on the critical issues in this case.
Dr Pater
64 Dr Pater has been the Director of Medical and Regulatory Affairs at AstraZeneca since 2001. He swore two affidavits which were read, but they contain nothing of relevance which was not in evidence through others.
65 However, his cross-examination elicited the following:
(1) One of the major ways in which pharmaceutical companies promote their products to general practitioners and other healthcare professionals is through the use of representatives who visit the practitioners.
(2) The industry codes of practice require that whenever a representative visits a general practitioner or other health care professional and provides any information about a drug, they are required to provide the product information documents in addition to any other materials they might leave although he was not sure if such product information documents were routinely left behind at each visit.
(3) That:
(i) The MIMS booklet constituted a source of information about drugs that is available to general practitioners.
(ii) Another source of information about drugs available to practitioners is the information they receive from pharmaceutical company representatives on their visits to them; and
(iii) The asthma management handbook that is published by the National Asthma Council is another source of information utilised by practitioners concerned with the treatment of asthma.
(4) From time to time AstraZeneca publishes full page display advertisements, of the type of which the sleeping man advertisement is an example, in publications such as Australian Doctor and Medical Observer.
(5) Such publications are generally part of a larger marketing campaign.
(6) He was not sure whether advertisements of that type are intended to be a self-contained source of information for GPs who might have come across them; at times they may.
(7) It may be true that one would not expect a GP seeing an advertisement of that kind to regard it as the complete and self-contained source of information on the basis of which he or she could or would make a decision to prescribe the drug Seretide for a patient but there may be other people who do see it as a self-contained advertisement. By way of clarification, he said there are 20,000 GPs in Australia encompassing a broad range of practitioners, some part-time, some full-time with varying degrees of education and experience and he did not know that all of them are called upon by representatives of pharmaceutical companies. Nor did he know what journals they read. He was not sure what impact advertising had on all of them.
(8) The words ‘before prescribing please review product information’ are included on advertisements of this type published by AstraZeneka in promoting its products. When asked whether it was always there he said: ‘I think it is usually there – “always” is a strong claim’.
(9) AstraZeneca expects GPs should have regard to the product information when making prescription decisions in the course of their practice.
(10) Doctors regard patients with asthma as patients who require ongoing management and as patients to be seen periodically for review of their condition and their treatment. It was generally true that GPs regard any treatment they might prescribe or continue to prescribe to any particular patient is dependent upon their assessment of that patient’s condition and ongoing needs and is also dependent upon the success of any treatment that they might have been on at an earlier point in time.
(11) It may be that when seeing any particular asthma patient a GP will have regard to the particular susceptibility of that patient to any side effect from a drug that he might consider prescribing. When pressed that it would be routine for a doctor to give consideration to such a matter, he said “I don’t know that I can answer that’. I find this response disingenuous.
(12) A journal such as that in which the GOAL Study is published is not a journal to which GPs would normally have recourse.
Dr Peters
66 Dr Peters is a thoracic physician in full-time hospital practice. He has been involved in clinical trials with Seretide for nine years and this continues at the present time. He has been on an Advisory Board for AstraZeneca and what was, in effect, an Advisory Board for GSK in relation to the GOAL Study. The AstraZeneca Advisory Board was for Symbicort.
67 He has read the published report of the GOAL Study many times and has read other published comment about the Study. He has participated in numerous professional discussions with colleagues about the GOAL Study, including detailed discussions with representatives of GSK, some of which were in connection with his Advisory Board participation for GSK.
68 The GOAL Study, which is complex in concept, was designed to test a hypothesis – that, if you have near-zero tolerance for asthma symptoms and increase asthma treatments at a very low symptom threshold, asthma could improve over time to the point that, for all practical purposes, the patient would not know that he/she has asthma (apart from taking treatment). These dose increases would occur with very occasional symptoms – such as using a Ventolin puffer twice within eight weeks. There was a further aim – to compare the performance of Seretide and Flixotide in achieving this very high standard of control – Seretide being a medication composed of Flixotide with an added long-acting bronchodilator. The definition of ‘total control’ used in the GOAL Study is not a definition that was used in clinical practice nor is it one that has been advocated as a standard in any national or international guidelines before or since.
69 The GOAL Study does prove what it set out to prove – namely that it is possible to achieve total control, as defined, in some asthma patients. However, whether using Seretide or Flixotide, the GOAL Study shows that you cannot achieve total control, defined at the very high standard as described in the Study, in most people.
70 That there was superiority for Seretide (over Flixotide) is clear from the data in the Study. These findings are not unique.
71 In his opinion there are real concerns about the GOAL/total control approach. Nearly all patients completed the study using the higher strength of inhaled corticosteroids – whether allocated to Flixotide or Seretide. The ‘cost’ of seeking ‘total control’ of asthma symptoms is the potential for adverse, long-term health consequences associated with sustained high doses of corticosteroids. These include cataracts, thinning of the skin and perhaps osteoporosis. Also, the principles applied in the GOAL Study may not be relevant to patients of doctors in the real world of managing asthma symptoms. For example, he said he may treat a patient who is on an intermediate dose of treatment (whether Seretide or Flixotide does not matter). A review of the patient’s asthma may show that everything is going well with the management of the asthma and the medication regime is familiar and being complied with. The patient complains of no symptoms at all except two episodes of slight wheeze, six weeks apart, on cold nights at rugby training. He had to take his Ventolin puffer but he was able to carry on. This is not total control against the definition in the GOAL Study and following the GOAL protocol would mandate a treatment increase. If Dr Peters, as his physician, prescribed increasing his dose, the patient would probably object regarding his asthma as being under very satisfactory control.
72 Against the background of these observations, when he looks at the GSK advertisements for Seretide he makes the observation that in the GOAL Study Seretide achieved total control in a minority of patients.
73 In clinical practice, it would be unfortunate, in his opinion, if prescribers formed the view that Seretide can ensure a patient would achieve elimination of asthma symptoms since the GOAL Study does not show this. In his view, the very tight linkage implicit in ‘Seretide Total Control’ as one phase cannot be validly drawn from the GOAL Study. It is also worthy of note that the Study population does not exactly correspond with the representative patient population seen by doctors around Australia. As one important example, smokers were excluded. Asthmatic patients who smoke had less effective responses to usual asthma treatments. It should also be borne in mind that asthma does improve generally when patients go into clinical trials. This is probably because they are more consistently adherent to treatment protocols than they might be outside a trial. They may also have the natural human desire to please in a situation where the patient is receiving considerable atttention from doctors and, even more importantly, the nurses who are the study coordinators.
74 He also notes the reference in the advertisements to the requirement for PBS reimbursement of Seretide. The effect of that restriction is that reimbursement is available for patients commencing Seretide therapy after previously having frequent episodes of asthma when being treated only with oral corticosteroids or optimal doses of inhaled corticosteroids. In this regard, patients in Stratum 1 in the GOAL Study who were naive to steroid use (one-third) could not be eligible for Seretide on the PBS. Likewise, many of the remaining patients may not have been eligible for Seretide on the PBS depending on the clinician’s view of what ‘frequent’ means.
75 He knows and acknowledges that because of his extensive knowledge of the GOAL Study, he is not in the same position as most GPs treating asthma patients, viewing promotional material or even trying to understand the Study more deeply. His experience of GP education systems around the GOAL Study tells him that the scientific detail is not easy for GPs to begin to understand and that few GPs would be comfortable following the dose escalation strategy in patients who are really very well but do not quite meet the criteria for total control. Finally he is not a GP and does not read the medical magazines regularly.
76 In summary, Seretide and Flixotide are excellent drugs for the treatment of asthma. The GOAL Study is an important study and yielded results that are of great interest to him as a respiratory physician. However, the achievement of total control in the GOAL Study was in a minority of patients only.
77 In cross-examination, Dr Peters said:
(1) The publication in which the GOAL Study report was published and in which the editorial comment of Dr Barnes was published is probably the pre-eminent global publication in respiratory medicine. It is the sort of journal that is of interest to researchers and specialists in the field.
(2) He was familiar with the publication MIMS; that it is a small paperback size publication which incudes commonly used medications with abbreviated product information. He generally refers to it for information on pharmaceutical products outside his general field.
(3) GPs rely on a variety of sources of information in their day to day practice and that MIMS may be one of them for information about the products they may or may not choose to use.
(4) While he had not read through the full product information for Seretide or Flixotide at any time he knew that companies go to great lengths to make sure that the information that they provide to the relevant authorities is accurate and of high quality and he did not doubt that that applied to those products.
(5) In drawing a distinction between himself as a specialist and a GP, he had access to information to which GPs would not have access.
(6) He would not be surprised if a minority of GPs would have read the extent of the product information literature as registered for the products they commonly use in the treatment of asthma including Seretide. Such GPs would have alternative information sources such as the GP-oriented medical magazines, forms of advertisement which come with computer-generated prescription systems and indeed visits from representatives of products. They have a variety of information sources which are slightly different from his own.
Dr Howe
78 Dr Howe is a general practitioner from Hurstville, a suburb of Sydney. He joined the Hurstville Railway Medical Centre in 1990 and has practised there as a GP since that time. He swore two affidavits in these proceedings.
79 Dr Howe’s first affidavit dealt with a number of relevant matters going to his knowledge and experience as a GP in prescribing medications for treatment of the symptoms of asthma, his exposure to and his experience with Seretide and Symbicort in prescribing them for his asthma patients, his exposure to and knowledge of the GOAL Study, his exposure to and experience in dealing with advertising by drug companies of their products and the Seretide Advertisements in particular.
80 Relevantly, Dr Howe’s evidence was to the effect that:
(1) He saw asthma patients on a regular basis – one or two patients on average per day.
Asthma Treatment
(2) Asthma is a condition that must be managed rather than cured.
(3) Over his years of practice, he has observed a shift in the treatment of asthma from treating of acute symptoms as they arise to long term management of asthma symptoms.
(4) For over 20 years, asthma patients have been treated with ‘reliever’ medications such as Ventolin (salbutamol). Theses medications are bronchodilators and are predominantly used by patients to immediately resolve asthma symptoms and avoid crisis.
(5) A shift occurred in the treatment of asthma patients in the mid 1990’s and the focus in treatment turned to prophylaxis and ‘preventer’ medications. These medications are called corticosteroids and act as anti-inflammatory drugs.
(6) Corticosteroids became the predominant medication used in the treatment of asthma patients in the 1990’s. The use of corticosteroids has been found to have, among other things, the following side effects:
(a) Growth retardation in children;
(b) Oral thrush;
(c) Mood variations; and
(d) Weight gain.
The above side effects led doctors to reduce the amount of corticosteroids being used by patients where possible.
(7) The objective with corticosteroids was to avoid over prescription and once effective control of asthma was achieved through a higher dose of corticosteroid, the normal treatment was to ‘down titrate’ patients to lesser dosages of corticosteroid.
(8) Reliever medications also improved during the 1990s and included the release for clinical use of long acting beta-agonists (LABAs) which are also referred to as long acting reliever medications. They have the effect of dilating the airways, like Ventolin, but are effective for longer periods of time.
(9) In the late 1990’s a further change occurred in the treatment of asthma patients when it was found that better results were obtained by combining the use of reliever medications (specifically LABAs) with corticosteroids. Asthma patients were prescribed separately (but to use together) both a reliever medication and a corticosteroid. This allowed asthma patients to reduce the dose of corticosteroid being used.
(10) In or about 2000, a reliever medication and corticosteroid became available in one combined medication. This was Seretide.
Asthma Symptoms and Expectations
(11) It is his expectation (and aim) for his asthma patients that they should be as symptom free as possible, however, he expects that most if not all of his asthma patients will show some symptoms from time to time.
(12) Depending on the severity of the patient’s condition his aim is to reduce the number of exacerbations an asthma patient may suffer during a year to two or three.
(13) Major indicators of the severity of a patient’s asthma include symptoms such as night time awakenings, the use of reliever medications, hospital visits, exacerbations and days off work.
(14) Night time awakening is a particularly important indicator as it is evidence of more severe asthma. If a patient is being woken in the middle of the night because of difficulty in breathing then this is of particular concern when considering treatment.
(15) Most of his patients are symptom free in terms of night time awakenings. He would estimate that approximately 15 per cent of his asthma patients are more acute asthma sufferers who would suffer from this symptom and depending on the patient and the season may experience one or two night time awakenings per week on average. This increases in colder whether. He would regard 75 per cent to 80 per cent of his asthma patients as having controlled asthma, however, they still accept that they will experience some symptoms from time to time.
Seretide Prior to the GOAL Study
(16) He first became aware of Seretide at or about the time it became available for clinical use in 2000. He also began prescribing Seretide for his patients at about that time. At about this time, his doctor prescribed Seretide for him and he continues to use it.
(17) As with most other new medications that come on the market, he became aware of the benefit of combination therapy and Seretide through journal articles published at the time of its release as well as through pharmaceutical company representatives, seminars and discussions he has had with other GPs.
(18) From the time Seretide came on the market he began prescribing it for his patients. One of the major factors in doing so, other than its clinical benefits, was the fact that it consisted of two medications that he had previously been prescribing that had been combined into one. This had immediate benefit for his patients as it was a more convenient method of asthma management and had the financial benefit of requiring his patients to purchase only one drug.
(19) As he obtained good results through the use of Seretide, he continued to prescribe it for his patients. On Seretide his patients had significantly fewer symptoms including fewer night time awakenings and less reliever medication use.
(20) At the time of its release on the market it was the only combination therapy available and he considered it a significant improvement in the treatment of asthma patients for the reasons expressed in pars (18) and (19) above.
Symbicort
(21) Symbicort is a combination LABA/corticosteroid medication produced by AstraZeneca which became available for clinical use by GPs some time after Seretide and, up until approximately six months ago, was only available in one dose. Seretide was available in three different dosages from the point it became available for clinical use.
(22) In his practice he also prescribes Symbicort, although to a lesser extent than Seretide.
(23) It has been his experience that Symbicort and Seretide are equally effective in the treatment of asthma patients and he does not consider one to be clinically superior to the other.
(24) His tendency to prescribe Seretide more often than Symbicort is generally due to the fact that most of his asthma patients, who are taking combination therapy for their asthma, were already using Seretide at the time Symbicort became available.
(25) As there is, in his view, no clinical reason to change the medication of his asthma patients currently using Seretide to an alternate combination therapy, he has and will continue to prescribe the same medication.
(26) It is most often the case, in his experience, that an asthma patient will already be comfortable with a form of delivery for their asthma medication and accordingly, he will prescribe the asthma medication that provides the delivery method which the particular patient is already using.
(27) The different delivery methods include:
(a) Inhaler – used by first breathing out, then placing the mouthpiece in the mouth, tilting the head back and breathing in while pressing the button at the top to release the medication;
(b) Accuhaler – used by placing the mouth over mouthpiece and pulling a trigger mechanism that releases medication into the mouth and breathing in;
(c) Turbuhaler – used similarly to an inhaler however instead of pressing down a person twists the release mechanism;
(d) Nebuliser – used through a mask and pump.
(28) In circumstances where he is changing a patient’s medication from using a corticosteroid alone to a combination therapy, he will prescribe the combination therapy medication that provides a delivery method the patient is comfortable with. Accordingly, if a patient is already using a GSK product such as Flixotide and using the delivery method of an Accuhaler then he will prescribe Seretide Accuhaler. If a patient is using an AstraZeneca medication such as Pulmicort and is comfortable using the AstraZeneca’s delivery method of a Turbuhaler, he will prescribe Symbicort.
(29) In his practice he finds that most of his patients are more comfortable using an Accuhaler than a Turbuhaler. He has found that some of his elderly patients and young patients find the Turbuhaler more difficult to use than the Accuhaler. The Turbuhaler requires more manipulation by the patient to deliver the medication than the Accuhaler.
GOAL Study
(30) He first became aware of the GOAL Study in 2004 at about the time the results of the study were published.
(31) He did not change his prescription practices as a result of the GOAL Study. It had been his practice to change his patients’ medication from single corticosteroid to combined corticosteroid/reliever for some years prior to the release of the GOAL Study. Most of his asthma patients were already using the combination medication at the time the GOAL Study was released.
Advertisements
(32) He subscribes to a number of medical publications including, Family Physician, Australian Medical Journal, Australian Doctor, Medical Observer and Current Therapeutics.
(33) These publications contain numerous advertisements for medications for a variety of pharmaceutical companies.
(34) He often sees the same picture or advertisement in these publications and unless there is something compelling in the advertisement that is different to what he has previously seen then he will not stop to consider the subject of the advertisement.
(35) When a new advertisement appears and a claim is made about a particular medication, he will look at the advertisement and consider the claim. Whenever a claim is made in an advertisement he will always consider the claim bearing in mind my own clinical experience of the medical condition the subject of the claim and the particular medication being advertised.
(36) He is generally sceptical about claims made in advertisements in medical journals. He believes this is the case with most GPs. He will look at the claim made and then at any underlying support. If the medication is a new medication he will consider what makes it different from the medication he is already prescribing for his patients.
(37) When considering advertisements or advertorials that are contained in these publications he also takes into account what he sees as a ‘sponsored’ review of the medication as compared to a more objective review that may be contained in a journal article about a medication or condition.
(38) He also sees a number of pharmaceutical company representatives who come to the Medical Centre to talk about their medications. During these meetings these representatives often show him advertising material relating to their products. As with advertisements in magazines and medical publications, he considers the information being provided to him during these meetings bearing in mind his own understanding of the medication and/or condition that is being treated.
Total Control Advertisements
(39) He has seen advertisements for Seretide using the phrase ‘Seretide Total Control’ since about March 2005.
(40) He has also seen advertisements for Seretide using the phrase, Seretide Total Control, in advertising provided to him by GSK’s representatives when they have come to his medical practice in or about March 2005.
(41) The Seretide Advertisements have not affected his prescription practices for Seretide or the circumstances in which he would prescribe it or other medication. In particular the matters set out in paragraphs (22) to (28) remain valid and are the matters that affect his prescribing practices in relation to asthma.
81 In his second affidavit, Dr Howe commented on Dr Peters’ affidavit:
(1) He agreed with Dr Peters’ that there is a potential for adverse health consequences associated with sustained high doses of corticosteroid use. It is common knowledge amongst clinicians that sustained use of corticosteroids may result in adverse side effects occurring. Dr Howe considers this when choosing dosages for his patients on Seretide as well as he prescribes any other corticosteroid for his patients.
(2) The potential for the side effects referred to by Dr Peters in his Affidavit occurring in clinical practice are, in Dr Howe’s view, slight. He monitors any of his patients who are on higher doses of corticosteroids for any side effects and reduces the dosage of corticosteroid if non-trivial side effects occur.
(3) There is no universal treatment of asthma patients. The treatment of patients with asthma (as with other diseases) is up to the treating GP in consultation with the individual patient.
(4) Dr Howe’s aim for his asthma patients, including those for whom he prescribes Seretide, is to be as symptom free as possible.
(5) In clinical practice Dr Howe strives to achieve the maximum amount of lung function for patients with the least amount of side effects from medication. Ideally, he tries to achieve a level of control of his patient’s asthma symptoms that approximates the GOAL defined level of total control. However, total control, as set out in the GOAL Study, is a very high level of control. It is often a matter of balancing an increase in the amount of corticosteroid used in treatment with any possible side effects. Once a level of control is reached that is the optimum level of control for that particular patient’s needs then he would generally try and down titrate the level of corticosteroid while at the same time keeping control of the patient’s asthma symptoms.
(6) This is a practice Dr Howe has have followed since well before seeing the Total Control advertisements and he did not change his practice as a result of seeing the advertisements in medical magazines or other promotional material.
(7) The balance between increasing a patient’s dose of corticosteroids in treating asthma symptoms and considerations of potential side effects is not a new issue. It has been a consideration of Dr Howe’s since combination therapy was introduced in clinical practice and even before. The ultimate decision concerning treatment is made by him in consultation with the individual patient. He will consider what the patient tells him they would like to achieve with their asthma management and he will aim to achieve this result with their treatment.
(8) In Dr Howe’s opinion, it is basic medical practice to discuss the available medications and any potential side effects with patients in order to allow the patient to make an informed decision concerning their treatment.
(9) Consistently with this, Dr Howe notes that the authors of the report on the GOAL Study state, at page 842:
‘In clinical practice, the decision on whether to aim for total control in patients who have reached a lesser level of control when this involves doubling the dose of controller treatment will need to be made on an individual basis in consultation with the patient.’
(10) This statement from the GOAL Study, in Dr Howe’s view, reaffirms that the treatment of a patient’s asthma symptoms is up to the treating GP in consultation with the individual patient. Some GPs may increase the dose of corticosteroid having consulted with the patient and others may not. There is nothing in the total control advertising material which suggests to him a different approach should be adopted. Further, the GOAL study itself recognises that the conditions of that study may not always be replicated in clinical practice. It is his experience that the conditions of a clinical trial or study are necessarily artificial and will often be varied. He certainly does not feel constrained to impose GOAL study dosages on his asthma patients for whom he prescribes Seretide and he does not regard the Seretide total control material to encourage him to do so.
(11) Neither the GOAL Study nor the Seretide total control advertisements prompted Dr Howe to escalate the dosages he was giving to his patients in order to achieve the GOAL defined level of total control.
(12) Dr Howe agreed that GPs are not often exposed to scientific data regarding clinical studies. However, he did not consider the GOAL Study to be overly hard to comprehend and he is able to understand the basic concepts. He first became aware of the GOAL study in 2004 through his reading of medical magazines and journals, discussions with GSK’s representatives and at an education session.
82 In cross-examination, Dr Howe was asked:
‘And ultimately, in terms of working out what level of control to aim for with a particular patient, you have to consult with the individual patient, consider what the patient tells you they would like to achieve with their asthma management, and you tell them what costs in terms of health effects and financial costs there are going to be? – Yes I do.’
83 A little later he was asked:
‘It would be wrong, wouldn’t it, to say that in your practice you always try to assist your asthma patients [to] achieve the level of total control of asthma symptoms which the GOAL Study outlined? – It would be very difficult to obtain that.’
84 He subsequently conceded that what he had said in par 72 of his first affidavit: ‘In my practice I always try to assist my asthma patients achieve this level of control of their asthma symptoms’, may be misconstrued. He qualified what he said there by saying that it was an ultimate aim to which he aspired.
85 He was then asked:
‘Do you honestly say that given the need to consult with the individual patient, to consider what the patient tells you they would like to achieve with their asthma management and that you would aim to achieve this result with their treatment. No, what you said in your affidavit yesterday was right; wasn’t it? – Yes.
It is an individual matter for individual patients in consultation with you? – Yes.’
86 He indicated that he was familiar with the GOAL Study and that in that respect he may be one of the better informed GPs. He agreed that he had attended AIM workshops, read about the GOAL Study in journals and magazines, that he was an asthmatic himself and that he had a close interest in the topic of asthma.
87 He was then asked some questions about the sleeping man advertisement including whether he was able to say from that advertisement what proportion of patients in the GOAL Study achieved the level of total control. His response was that the advertisement did not specify how many patients. When asked whether he had read the advertisement many times, he said: ‘I have seen it’ and when asked whether he was familiar with the advertisement, he said: ‘Yes, I’ve seen it’. He was then asked to take a moment to read it again and said: ‘I’ve seen it several times in a variety of magazines so I am familiar with it’. It was again suggested that he should read it again and tell the Court if it conveyed to him what proportion of patients in the GOAL Study achieved a level of total control. His response was that it did not actually specify what proportion.
88 He was then asked the same question in relation to the upgrade advertisement and again he answered that the advertisement did not convey to him the proportion of patients in the GOAL Study who achieved a level of total control.
89 He was then asked the same question with respect to the sales aid and again answered in the negative to the question whether it conveyed to him the proportion of patients in the GOAL Study who achieved a level of total control.
90 He was then asked the same question in relation to the GOAL Mailer. He said that there was a small insert down the bottom which discussed the proportion of patients that achieved total control and well controlled asthma.
91 Finally, Dr Howe said that it was possible that he had not given any reason for the conclusion or opinion to which he came in par 65 of his affidavit.
92 In re-examination Dr Howe was asked to explain to the Court the extent of the attention he had paid to the sleeping man advertisement at the time of its publication in Australian Doctor, Medical Observer and other journals. He answered:
‘Any sort of advertisement you often see in medical journals and it is often part of a program put in by the various drug companies so it would be part of the whole campaign. I would only have given it short attention because I realised it was part of GSK’s Seretide advertising campaign so it would have been brief because I am aware of it.’
The Submissions
AstraZeneca’s Submissions
93 AstraZeneca, in its submissions, identifies the salient features of the Seretide Advertisements as:
(1) Conveying the dominant impression that a sufficiently high proportion of all asthma patients will achieve total control of all asthma symptoms by using Seretide to justify the use of the brand slogan ‘total control’. That description is not justified in circumstances where even on the most favourable view of the GOAL Study only a minority of patients achieved total control.
(2) The lack of prominence given to the qualifying footnotes that appeared in each of the Seretide Advertisements relative to the prominence given to the brand slogan ‘Seretide Total Control’ and the fact that what is disclosed in the footnotes is to the contrary effect of what is conveyed by the dominant message; the dominant message being achievement of total control generally in patients, the footnote being to the effect that only happens in a minority of patients, and if you want to see what happens to most patients, they get to well controlled but not totally controlled.
94 Senior Counsel for AstraZeneca contended that this second submission was made good by the answers which Dr Howe gave in cross-examination to a series of questions put to him as to whether the Seretide Advertisements told him what proportion of patients in the GOAL Study achieved the level of total control. This evidence is referred to at [87] – [90] supra. In the case of the sleeping man advertisement, the upgrade advertisement and the sales aid, although not the GOAL Mailer, Dr Howe said that none of them told him what proportion of patients in the GOAL Study achieved the level of total control. In the case of the sleeping man advertisement he was asked a number of questions going to how many times he had read it and he answered that he had seen it several times in several magazines. And he was also given the opportunity to read it again in the witness box after which the question was put to him again, but he still maintained it did not tell him the relevant information.
95 In my view, the only conclusions that can be drawn from this evidence are:
(1) That Dr Howe did not fully read the sleeping man advertisement in the witness box because had he done so it would have been readily apparent that it did disclose the number of patients in the GOAL Study who achieved the level of total control;
(2) That he had never fully read the sleeping man advertisement, the upgrade advertisement or the sales aid or if he had, because of his familiarity with GSK’s advertising campaign – he had seen the sleeping man advertisement a number of times – he had not paid attention to the detail of that advertisement, the upgrade advertisement or the sales aid. He was not asked why he was familiar with the detail of the GOAL Mailer; and
(3) That he was, despite being called by GSK, a witness who, not only in his answers to this series of questions, but also to other questions put to him in cross-examination and his evidence in chief, totally forthright and observant of the Court’s Guidelines for Expert Witnesses, in particular, that his primary duty is to assist the Court.
96 For the first two reasons, I do not think the answers given by Dr Howe to this series of questions advance AstraZeneca’s case on this second submission – the lack of prominence given to the qualifying footnotes relative to the prominence given to the brand slogan ‘Seretide Total Control’.
97 In addition to the features identified in [93], AstraZeneca points to the following aspects as giving the Seretide Advertisements a misleading nature:
(1) The omission of words from a quotation from the GOAL Study in the GOAL Mailer [4](1), supra, Fig. 1 or, more correctly, the failure to continue the quotation to the end of the sentence from which the quoted words were taken. The relevant quote in the GOAL Mailer appeared as:
‘… the approach of aiming for total control and maintaining treatment resulted in the virtual elimination of exacerbations and near-normal quality of life ….’
Whereas the sentence in the GOAL Study from which it was taken read:
‘In addition, the approach of aiming for total control and maintaining treatment resulted in the virtual elimination of exacerbations and near-normal quality of life in the majority of patients and brought substantial benefit even to those who failed to achieve this high level of control.’ (Emphasis)
AstraZeneca submits that the reference to the majority of patients indicates that this was a conclusion with respect to well-controlled asthma (with an overall 71 per cent success rate) not totally-controlled asthma (with an overall 41 per cent success rate). It is simply wrong to say that the GOAL Study concluded that the use of Seretide resulted in the virtual elimination of exacerbations and near normal quality of life so as to justify the slogan ‘Total Control’.
(2) The GOAL Study does not purport to replicate what would happen statistically in the real world of clinical practice. The GOAL Study was designed to test a hypothesis (that treatment can be increased to a point where asthma symptoms are felt only very occasionally), and the definition of ‘total control’ used in that Study is not used as a standard in clinical practice. Prescribing doctors must also take into account the potential for adverse long-term health consequences associated with sustained high doses of corticosteroids. The Seretide Advertisements, in using the GOAL Study as the basis for making recommendations to GPs concerning which medication to prescribe in clinical practice, without disclosing these limitations, is misleading.
98 A particular manifestation of that deficiency concerns the use of the overall cumulative figures in the GOAL Study, including Stratum 1, being patients with no use of inhaled corticosteroids in the previous six months. As would be expected, this group performed the best in terms of totally controlled (50 per cent) and well-controlled asthma (78 per cent). However, as Dr Peters points out in his affidavit, patients in Stratum 1 (and many of the remaining patients) would not be eligible for Seretide on the PBS, the criterion for which is stated in the advertisements themselves. Accordingly, it is highly unlikely that GPs would prescribe Seretide to those patients.
GSK’s Submissions
The Sleeping Patient Advertisement [4](3); Fig. 3
99 That the expression ‘Seretide Total Control’ is qualified or explained is immediately apparent from the footnote references following ‘Control’. The note at the asterisk beneath the PBS restricted benefit notice is clear: 41 per cent of patients achieved total control in the GOAL Study. The reader is immediately aware that the word ‘total’ is not used in an absolute or unqualified sense, contrary to AstraZeneca’s submission. The disconformity between the general meaning of the word ‘total’ when used as an adjective and the qualification makes clear what is otherwise apparent from the design of the advertisement, namely that ‘Seretide Total Control’ is a branding slogan not a statement imparting information to prescribing doctors.
100 AstraZeneca submits that the qualifier is not prominent in the advertisements. Although it is in small type, the advertisements are short documents, there is relatively little written on them, and they are there to be read. Only someone with very poor eyesight would find them illegible. AstraZeneca also asserts that many would not read the note. This assertion is made without any evidentiary support. However, even if it is right, it is immaterial as the subject advertisements do not cause GPs to change their view of the efficacy of Seretide.
The Upgrade Advertisement [4](4); Fig. 4
101 This advertisement is similarly clear in its use of the term ‘total control’. In this instance ‘total’ is further distinguished as a mere brand by the manner of its presentation. In addition to the qualifier referred to above, the text to the left of the puffer reads ‘more asthma patients were able to achieve totally or well-controlled asthma using … Seretide’. Clearly not all patients using Seretide obtained totally or even well-controlled asthma.
The Sales Aid [4](2); Fig. 2:
102 This was distributed by GSK’s sales representatives. Its emphasis is that doctors should consider switching their patients from Flixotide to Seretide. Dr Howe’s evidence is that he did not recall considering the phrase ‘total control’ on this chart until asked to do so for the purpose of this proceeding. Rather, he finds the chart a useful tool in his practice for assessing dosages. This advertisement is even less likely to cause the confusion than the first as the qualifier appears above the phrase ‘Seretide Total Control’.
The GOAL Mailer [4](1); Fig. 1:
103 This confirms that the total control campaign addresses the proposition that it is possible to achieve the GOAL defined notion of ‘total control’ with Seretide rather than representing that it will be achieved in any given number of patients. Every time the expression ‘total control’ is used in conjunction with ‘Seretide’ on the brochure there is an asterisk referring the reader to the qualifier demonstrating that only 41 per cent of patients on the GOAL study achieved this high level of control. The use of ‘achieve’ and ‘achievable’ emphasises GSK’s submission in this respect. Contrary to AstraZeneca’s submission, this brochure does not ‘misquote’ the GOAL study. Rather, it says that the ‘approach’ of aiming for total control brings benefits. As the fuller quote cited by AstraZeneca reveals, such benefits accrued to the majority of patients who did not achieve total control. Accordingly, it is right to say that the GOAL Study concluded that, in attempting to achieve total control, the use of Seretide in a majority of patients resulted in the virtual elimination of symptoms and near-normal quality of life. As both Dr Howe and Dr Peters indicate, patients can have very satisfactory levels of asthma control without attaining the GOAL Study defined level of total control.
Reasoning
104 The question whether particular conduct of which complaint is made is misleading or deceptive or likely to mislead or deceive is, in the ordinary case, a question of fact to be answered in the context of the evidence as to the alleged conduct and as to relevant surrounding facts and circumstances: Taco Co of Australia Inc v Taco Bell Pty Ltd (1982) 42 ALR 177 at 199 per Deane and Fitzgerald JJ.
105 AstraZeneca did not adduce any evidence going to the underlying knowledge and experience of GPs in dealing with the symptoms of asthma in their patients. That may have been because it accepted the evidence relied on by GSK through Dr Howe. Whether that is so or not, it cannot be doubted that such evidence forms part of the ‘relevant surrounding facts and circumstances’ referred to in Taco by reference to which the question of whether the conduct complained of is misleading or deceptive is to be determined. I shall return to the relevance of this evidence when considering the content of each of the Seretide Advertisements below. Before doing so, it is necessary to deal with a threshold difficulty with AstraZeneca’s case.
106 It is common ground that the class of persons to whom the Seretide Advertisements are directed, including such representations, express or implied, as they contain, are medical practitioners, in particular GPs, rather than the general public. Whether or not any such representations are misleading falls to be considered having regard to that audience.
107 In the case of a section of the public who are members of a class of prospective purchasers or consumers, which may be expected to include a wide range of persons, it has been said that it is necessary to isolate by some criterion a representative member of the class: Campomar Sociedad Limitada v Nike International Ltd (2000) 202 CLR 45 at [103]. And in Parkdale Custombuilt Furniture Pty Ltd v Puxu Pty Ltd (1982) 149 CLR 191 at 199, Gibbs CJ said that s 52 of the Act must, in his opinion, be ‘regarded as contemplating the effect of the conduct on reasonable members of the class’.
108 Whether it is necessary to undertake this further process of isolation or selection in the case of a class of persons all of whom are GPs may be doubted, but for present purposes I propose to approach the question of whether the conduct complained of is misleading or deceptive from the point of view of the effect of that conduct on a reasonable GP.
109 A threshold difficulty with AstraZeneca’s case is its failure to identify the error or ‘erroneous assumption’, as it has been called, having a causal connection with the conduct complained of, namely, the representations alleged to have been conveyed by the Seretide Advertisements. Nowhere is it said, in express terms, either in the pleadings or in the submissions, that, for example, the Seretide Advertisements are misleading or deceptive or likely to mislead or deceive because they may lead GPs into error, namely, prescribing Seretide for their asthma patients on the erroneous assumption that it will provide them with total control of the symptoms of asthma. That may well underlie AstraZeneca’s case, but it was never identified as such in either the statement of claim or in the written and oral submissions made to the Court. Absent identification of the error, there can be no causal connection with the representations alleged to have been conveyed by the Seretide Advertisements.
110 That it is a difficulty with AstraZeneca’s case is exemplified in what the High Court said in Campomar at [104]:
‘It is here that there arises a critical question on the case put for the appellants. It concerns the so-called “doctrine” of “erroneous assumption” said to be derived from, in particular, decisions of the Full Court of the Federal Court in McWilliam’s Wines Pty Ltd v McDonald’s System of Australia Pty Ltd (1980) 49 FLR 455, Taco Co of Australia Inc v Taco Bell Pty Ltd and Lego Australia Pty Ltd v Paul’s (Merchants) Pty Ltd (1982) 60 FLR 465. In their joint judgment in Taco Bell (at 200), Deane and Fitzgerald JJ emphasised that “no conduct can mislead or deceive unless the representee labours under some erroneous assumption” …
Their Honours added that, in determining the question whether conduct properly should be categorised as misleading or deceptive or as likely to mislead or deceive, the nature of the erroneous assumption which must be made before conduct could have that character “will be a relevant, and sometimes decisive, factor” (at 200).’
111 To the same effect, albeit in different terms, was what was said by the Full Court of this Court in Johnson Tiles Pty Ltd v Esso Australia Ltd (2000) 104 FCR 564 at [63]:
‘The touchstone of liability is the conduct by act or omission of Esso and its characterisation as misleading or deceptive. The analysis of the statement of claim must begin by identifying the conduct and the facts relied upon to give it that character. The principles governing characterisation are well established. Conduct is misleading or deceptive if it induces or is capable of inducing error – Keehn v Medical Benefits Fund of Australia Ltd (1977) 14 ALR 77; Weitmann v Katies Ltd (1977) 29 FLR 336; Parkdale Custom Built Furniture Pty Ltd v Puxu Pty Ltd (1982) 149 CLR 191 at 198 (Gibbs J); Rhone-Poulenc Agrochimie SA v UMI Chemical Services Pty Ltd (1986) 12 FCR 477. The so called “doctrine” of “erroneous assumption” referred to by the High Court in Campomar Sociedad Limitada v Nike International Ltd (2000) 169 ALR 677 at 704, is merely another way of expressing that general proposition albeit it seems to have arisen in the context of cases involving similar product names. The statement in the joint judgment of Deane and Fitzgerald JJ in Taco Co of Australia Inc v Taco Bell Pty Ltd (1982) 42 ALR 177 at 200 that “no conduct can mislead or deceive unless the representee labours under some erroneous assumption”, cited in Campomar, is another way of saying that the representee must be led into error.’
112 Even if an error or erroneous assumption may be inferred in terms of that suggested in [109], a further difficulty for AstraZeneca’s case is that it led no evidence to suggest that GPs rely on the information/representations made in advertisements of the kind comprising the Seretide Advertisements and appearing in publications of the kind in which some of those advertisements appear to prescribe medication for those of their patients suffering from the symptoms of asthma. Indeed, such evidence as was led or elicited in cross-examination would indicate that GPs place no reliance on such advertisements in prescribing medications for their patients with symptoms of asthma; that they merely regard such advertisements as part and parcel of wider marketing campaigns undertaken by drug companies to promote their products, and not as a source of information by reference to which they prescribe medications for their patients. This is borne out by the prescribing practises of Dr Howe described at [80](22) – (29) supra and his evidence at [80](31) and (41) supra. Even some of the questions that were put to him in cross-examination were predicated on the basis that prescribing was an individual matter for individual patients in consultation with their doctor, effectively denying any reliance on any representation conveyed by the Seretide Advertisements: See [82] and [85] supra. It is also borne out by the evidence of Dr Pater in cross-examination at [65](1) – (10) supra. He said it may be true that one would not expect a GP seeing an advertisement of that kind to regard it as the complete and self-contained source of information on the basis of which a GP could or would make a decision to prescribe the drug Seretide for a patient but there were 20,000 GPs and maybe some would see it that way. That is as high as the evidence got that GPs rely on such advertisements to prescribe medication for their patients.
113 But evidence of the ‘relevant surrounding facts and circumstances’ referred to in Taco, or context as it is compendiously called, also indicates that GPs relied on sources of information, including their own familiarity and experience in the form of patient acceptance and results achieved in prescribing Seretide since it first came on the market, other than any representations conveyed by the Seretide Advertisements, as a basis for prescribing medication to their patients suffering from the symptoms of asthma. Seretide was first available in Australia from August 2000 and had been extensively prescribed prior to the publication of the Seretide Advertisements. Indeed, even after Astrazeneca’s product Symbicort became available, Seretide had an overwhelming dominant position in the market – see [21] – [23] supra, no doubt due in part to the prescribing practises adopted by Dr Howe and other GPs described at [80](22) – (29) supra.
114 In the absence of any evidence that any representations conveyed by the Seretide Advertisements would be relied upon by GPs in prescribing medication for their patients suffering from the symptoms of asthma, it is impossible to find any causal connection between the conduct complained of and any inferential error or erroneous assumption of the kind suggested in [109]. That would be sufficient to dispose of AstraZeneca’s case, but there are other reasons why it must fail.
115 Even if one could infer an error or erroneous assumption under which GPs laboured and a logical causal connection between the Seretide Advertisements (and any representations they conveyed) and the hypothesised error, it does not necessarily follow that that will result in the conduct being regarded as misleading or deceptive for the purpose of s 52 of the Act. As was said by the Full Court in Johnson Tiles at [64]:
‘Conduct may be misleading or deceptive because it involves an express representation which is false. In the statement of claim in such a case the representation will be pleaded as a fact as will the falsifying facts. The conduct may involve an implied representation conveyed by words or conduct or some combination thereof. Such a representation will be falsified in the same way as an express representation. But the identification of a representational element is not necessary, albeit it will be involved in most cases. Conduct is to be characterised by reference to its actual or possible consequences – Hornsby Building Information Centre Pty Ltd v Sydney Building Information Centre Ltd (1978) 140 CLR 216 at 228 (Stephen J). This does not require demonstration that anyone has actually been misled – Annand & Thompson Pty Ltd v Trade Practices Commission (1979) 25 ALR 91 at 102 (Franki J) and 111 (Northrop J); Brock v Terrace Times Pty Ltd (1982) 56 FLR 464; Taco Co of Australia Inc v Taco Bell Pty Ltd at 202 (Deane and Fitzgerald JJ). It does require a capacity to mislead or deceive attributable to the conduct in question. There must be a logical causal connection between the conduct and some hypothesised error. But not every case involving a logical connection between conduct and alleged error will result in the conduct being regarded as misleading or deceptive for the purposes of s 52. There is an evaluative judgment involved. As the Full Court said in SAP Australia Pty Ltd v Sapient Australia Pty Ltd (1999) 169 ALR 1 at 14:
“The characterisation of conduct as “misleading or deceptive or likely to mislead or deceive” involves a judgment of a notional cause and effect relationship between the conduct and the putative consumer’s state of mind. Implicit in that judgment is a selection process which can reject some causal connections, which, although theoretically open, are too tenuous or impose responsibility otherwise than in accordance with the policy of the legislation.”’ (Emphasis)
116 Three of the Seretide Advertisements, namely the sales aid (Fig. 2), the sleeping man advertisement (Fig. 3) and the upgrade advertisement (Fig. 4) contain:
(1) No representation, express or implied, of the kind pleaded in [5](a) – (c) of its Statement of Claim: See [7](1) – (3), supra. At most they contain what is common ground – a free-standing brand slogan – ‘Seretide Total Control’ – and even that is referenced to a footnote qualification to the GOAL Study.
(2) No express representation of the kind pleaded in [5](d) of its Statement of Claim: See [7](4), supra. If it arises by implication, its logical causal connection with any inferred alleged error is too tenuous to be regarded as misleading or deceptive for the purposes of s 52. This conclusion flows from the fact that the implied representation is, in substance, true (total = 100 per cent) and the fact of the audience to which it is directed.
117 In the case of these advertisements, the representations pleaded in [5](e) and (f) of AstraZeneca’s Statement of Claim: See [7](5) and (6), supra – are true. Any case that they are misleading or deceptive is predicated on a premise of what is not said; again any logical causal connection between what is not said and any inferred alleged error is too tenuous to be regarded as misleading or deceptive for the purposes of s 52. This conclusion stems in large part, if not in whole, from the truth of what is said and the fact of the audience to which it is directed.
118 And, no express representation of the kind pleaded in [5](g) of AstraZeneca’s Statement of Claim: See [7](7), supra, is made in these advertisements. If it arises by implication, it is because of what is not said; any logical causal connection between what is not said and any inferred alleged error is too remote to be regarded as misleading or deceptive for the purposes of s 52. This conclusion stems from the reference to the GOAL Study in the advertisements, the fact that the GOAL Study makes it clear that clinicians might not replicate its conditions and the fact of the audience to which it is directed.
119 The GOAL Mailer also contained the brand slogan ‘Seretide Total Control’, not always free-standing as in the other advertisements, but in association with word messages which arguably give rise to implied, if not express, representations of the kind complained of. The message on the front page –
‘Imagine if you had the power to totally control asthma ….’
followed by the message on the second page –
‘Now you can achieve that goal with SERETIDE TOTAL CONTROL1*’
is the case in point.
120 That, however, is counter-balanced by the message, equally prominent, on the third page:
‘GOAL provides EVIDENCE that total asthma control is now achievable with Seretide1*’
121 In both cases the references are to the qualifying footnote:
‘* The GOAL study examined whether guideline defined asthma control could be achieved in 3416 patients with uncontrolled asthma. 41% of patients achieved total control and 71% achieved well controlled asthma with Seretide for periods of 7 out of 8 weeks over the 12 month study.’
122 Complaint is also made of the quotation from the GOAL Study at the foot of the third page: viz.,
‘… the approach of aiming for Total Control and maintaining treatment resulted in the virtual elimination of exacerbations and near-normal quality of life …’
Not because of any inaccuracy, but because it does not go far enough – it does not go to the end of the sentence from which the words are extracted so as to include the words:
‘… in the majority of patients and brought substantial benefit even to those who failed to achieve this high level of control.’
In other words, it is misleading or deceptive by omission.
123 Even assuming that one or more of the representations complained of can be made out as being conveyed by the GOAL Mailer, the logical causal connection between the representations and the inferred error is so tenuous that it is not possible to arrive at any finding that the representation is false and misleading. This conclusion is supported by the following matters:
(1) The balance of the advertisement, viewed as a whole, as referred to in [120].
(2) The qualifying footnotes at all levels referred to in [121].
(3) The truth of the extract from the GOAL Study, with or without the omitted words, in [122].
(4) The audience to which the advertisements was directed, [106] supra.
(5) The prescribing practises of GPs as set out at [80](22) – (29), supra.
(6) The experience of GPs in dealing with asthma symptoms and their familiarity and experience in dealing with Seretide and Symbicort as adduced in the evidence of Dr Howe [80](1) – (30), supra.
124 Even if there was an identified error or erroneous assumption which one could rely on to find a logical connection between any such implied representation and the identified error, I would not be prepared to find, for the reasons given, that any such representation was misleading or deceptive in terms of s 52 of the Act.
125 The application must be dismissed with costs.
|
I certify that the preceding one hundred and twenty-five (125) numbered paragraphs are a true copy of the Reasons for Judgment herein of the Honourable Justice Edmonds. |
Associate:
Dated: 16 November 2005
|
Counsel for the Applicant: |
Mr I M Jackman SC |
|
|
|
|
Solicitor for the Applicant: |
Minter Ellison |
|
|
|
|
Counsel for the Respondent: |
Mr R Webb SC with Mr N R Murray |
|
|
|
|
Solicitor for the Respondent: |
Deacons |
|
|
|
|
Date of Hearing: |
26 July 2005 |
|
|
|
|
Date of Judgment: |
16 November 2005 |

