
FEDERAL COURT OF AUSTRALIA
Australian Competition and Consumer Commission v Medibank Private Limited [2018] FCAFC 235
ORDERS
AUSTRALIAN COMPETITON AND CONSUMER COMMISSION Appellant | ||
AND: | Respondent | |
DATE OF ORDER: |
THE COURT ORDERS THAT:
1. The appeal be dismissed with costs.
Note: Entry of orders is dealt with in Rule 39.32 of the Federal Court Rules 2011.
PERRAM J:
1 The Australian Competition and Consumer Commission appeals from orders made by a judge of this Court dismissing its proceeding after a 12-day trial: Australian Competition and Consumer Commission v Medibank Private Limited [2017] FCA 1006. Its first case at trial was that the Respondent had misrepresented to its customers that they would not be left with any out-of-pocket expenses for pathology or radiology services provided to them whilst admitted as an in-patient in a hospital. It is convenient to refer to pathology and radiology services together as 'diagnostic services'. Its second case was that it had misrepresented to its customers that it would not reduce their benefits under their policies but in fact did so. It had done so, so it was alleged, by terminating agreements it had with various diagnostic service providers which had, until their termination, meant that a number (but not all) of the Respondent's customers who were in-patients in a hospital did not experience an out-of-pocket expense in respect of those providers' services. After that termination, those customers began to experience out-of-pocket expenses. Its third case was that the Respondent had acted unconscionably in the way it had ended those agreements. The trial judge rejected each case and the Appellant now pursues each on appeal.
2 For the reasons which follow I would reject the Appellant's appeal in relation to the two misrepresentation cases. For the reasons given by Beach J, I would reject its appeal in respect of the unconscionability case. The appeal should, therefore, be dismissed with costs.
3 The Respondent conducts its business under two brands: the Medibank Private brand and the ahm brand. The Appellant's cases in relation to the two brands differed although they were closely related. It is convenient to treat its case on the two brands separately.
Medibank Brand: The Diagnostic Cover Representation
4 The case advanced by the Appellant was that the Respondent had misrepresented to its customers that they would not have to bear any out-of-pocket expense in respect of diagnostic services rendered to them as in-patients in a hospital.
5 The Respondent sold private health insurance policies under the brand Medibank Private through three trade channels: in retail stores and kiosks; over the telephone from call-centres operated by a third party referred to as Salmat; and via a webpage it maintains on the World Wide Web. The Appellant contended that the diagnostic services representation had been conveyed through all three channels. It also alleged that it had been conveyed in a variety of documents it posted to customers after they had entered into a policy with the Respondent. As such, the Appellant's case at trial was complex and voluminous. It had to deal with the documents which had been sent and the condition of the website. It also had to try and distil the gist of the actual encounters which took place between its in-store retail staff and consumers and between consumers and the sales representatives working the telephones in Salmat's call centres.
6 Naturally, this was a significant forensic endeavour which makes it no surprise that the trial lasted 12 days. However, despite the sprawling field of combat the Appellant's case had an important central element which was common to almost all of the significant material tendered at trial. It can be found in the post-sale information provided to customers, on its website and in the literature which was provided to both its in-store employees and to the representatives working for Salmat. It took many different forms but from the Appellant's perspective all those varieties of embodiment revealed a similar message.
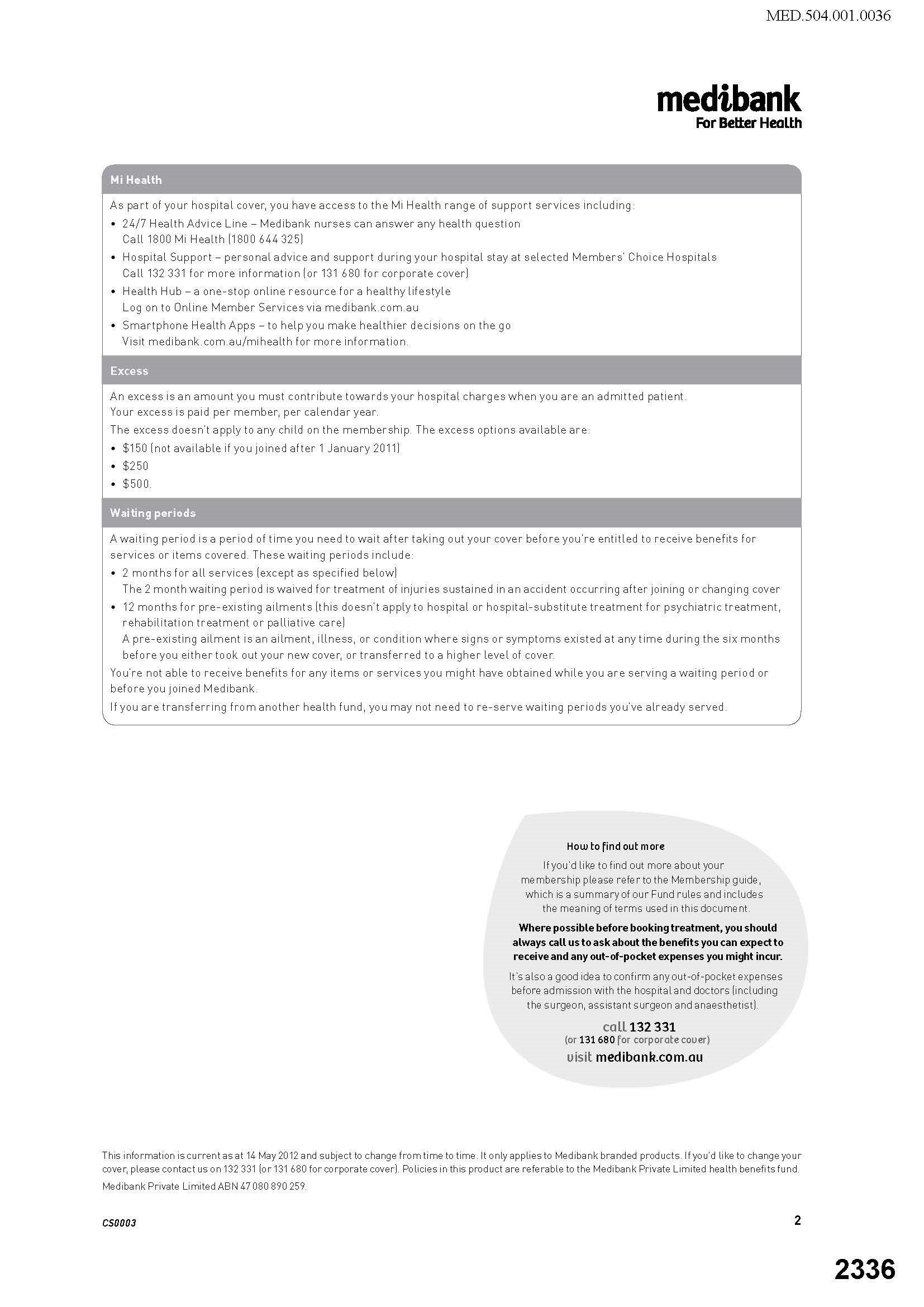
7 In the interests of clarity it is useful to set out one example in full so the point can be understood. The example is a document entitled 'Cover Summary Basic Hospital'. It was two pages in length and was as follows:
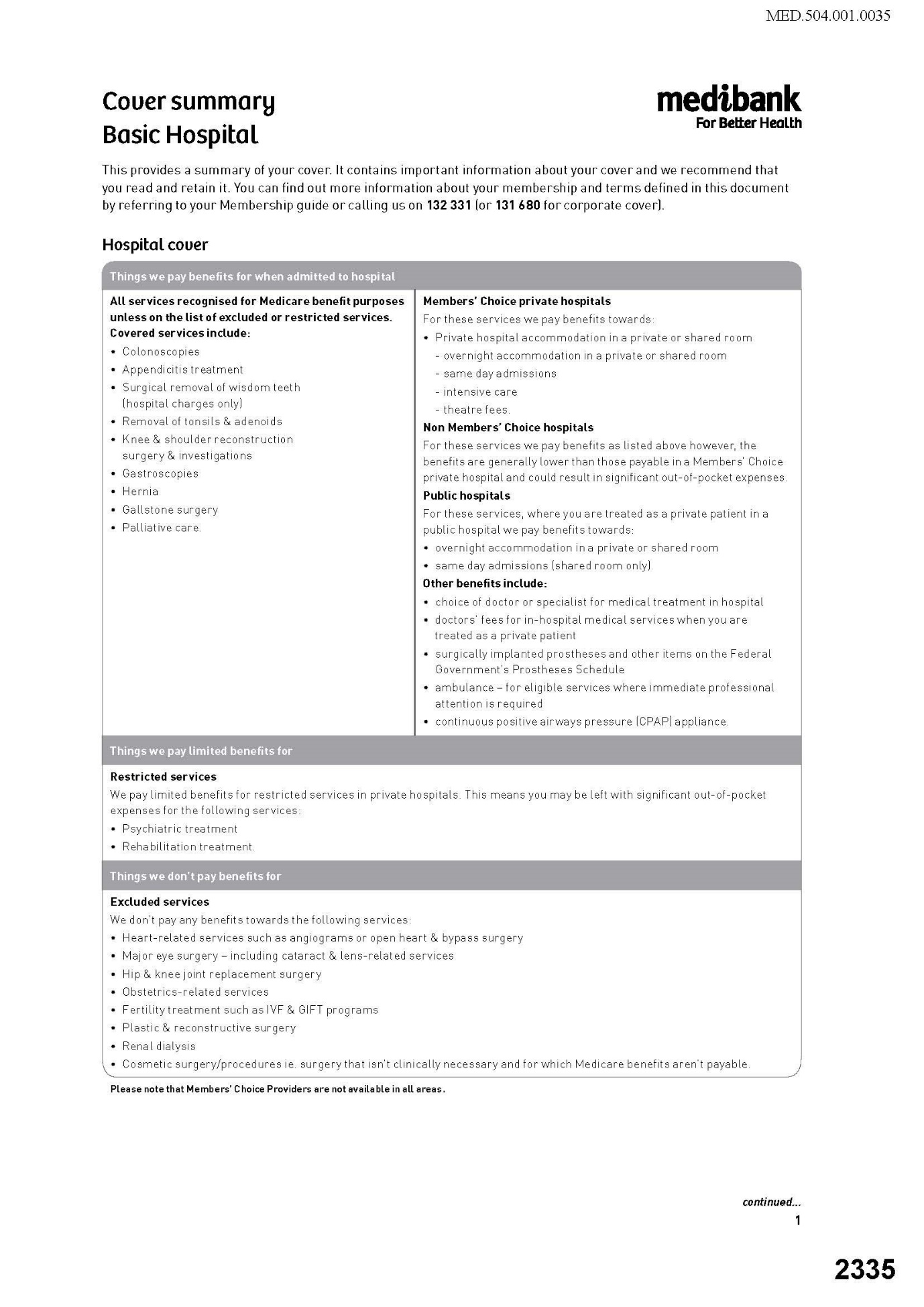
8 Before explaining the Appellant's argument it is necessary to provide some matters of context. First, the Respondent issued many different policies with fluctuating cover levels (top cover, basic cover etc.) to different kinds of customers (singles, couples, families). At the trial, it was accepted on all sides that attention could be limited to the 'basic cover' product since it was suitably representative of the issues which arose in relation to all of the Respondent's policies. Secondly, the cover contemplated was of two kinds. One was cover for services recognised by Medicare. The only such services are those provided by medical practitioners. In the case of services provided by a medical practitioner, the Commonwealth pays Medicare benefits in the amount of 75% of what is referred to as the schedule fee for that service. The schedule fee is fixed by the Commonwealth and prescribed in the Medicare Benefits Schedule. Thus the cover described in the first column of the extract above is cover in respect of the cost of medical services in the schedule.
9 Medical practitioners are not bound to charge only the schedule fee and many charge more. Because Medicare pays 75% of the schedule fee in all such cases, the cover mentioned in the first column is cover for the balance of 25% of the schedule fee which the Respondent is required by law to cover. An insurer may provide cover for more than this 25% and thereby reduce, or even eliminate, any 'gap' between the actual cost of the service and the schedule fee. It is, in part, in their coverage of such gaps that the various private health insurers compete with each other.
10 The second type of cover offered under the policy did not relate to services provided by medical practitioners. It related instead to services provided by hospitals such as accommodation, theatre fees, ambulances and so on. These appear in the second column.
11 Returning to the cover summary itself, it was the Appellant's case that the Respondent conveyed the representation that a customer would not be exposed to any out-of-pocket expenses in respect of diagnostic services provided to them as an in-patient in a hospital. One interesting aspect of the argument which may be noted at the outset is that the cover summary does not refer to diagnostic services at all. As will be seen this is not just a curious feature of the Appellant's case but is ultimately closely related to the reason why the diagnostic representation case cannot succeed.
12 The Appellant's theory for why the diagnostic cover representation could be gleaned from a cover summary which does not mention such services (and every equivalent document or material) had three steps:
(a) under the heading 'Hospital Cover' in the first column it was suggested that 'covered services' included all services recognised for Medicare benefits purposes. But this was subject to the proviso that the services be not 'restricted' or 'excluded services';
(b) in the cover summary's treatment of restricted services it was made clear that customers might well be left with substantial out-of-pocket expenses. There were, however, only two such services: psychiatric services and rehabilitation services. It was also clear that no benefits would be paid for 'excluded services' at all. The list for such services was longer but did not include, relevantly, any diagnostic services; and
(c) reading all three sections together the implication was said to be that out-of-pocket expenses would only be incurred for excluded and restricted services. Since diagnostic services were not amongst those kinds of services it followed that no out-of-pocket expense would be payable when a patient received diagnostic services as an in-patient in a hospital.
13 The Appellant buttressed this point with various additional matters of emphasis. For example, stress was placed on the words in the first column 'covered services' which were said to convey, in an insurance context, that the customer would have no exposure to costs.
14 Of course, as a cursory examination of the cover summary quickly reveals, there were matters tending in the opposite direction, too. One of these is the statement in the second column that the Respondent would 'pay benefits towards' private hospital accommodation which might suggest less than full indemnity. On the other hand, the second column is dealing principally with cover for accommodation rather than medical expenses. Also relevant is the balloon on the second page which asks the customer to call before going to hospital to ask about 'any out-of-pocket expenses you might incur'.
15 The trial judge was not persuaded that statements of the kind contained in the cover summary conveyed the diagnostic cover representation. Before explaining his Honour's reasons for those conclusions it should, I think, be acknowledged that at least as a matter of initial impression it is not difficult to understand the Appellant's argument and, indeed, even to see some force in it. What the trial judge's reasons expose, however, is the Achilles' heel of this apparently plausible case. That heel is the fact that the cover summary does not mention diagnostic services. The forensic manoeuvrings by the Appellant to make statements of the kind referred to in the cover summary apply to diagnostic services lays bare critical architectural defects in its case theory. As the trial judge noted at [171] the logic of the Appellant's argument leads to a result which means that there would be no out-of-pocket expenses for any medical services for which benefits were payable (apart from restricted services), not just diagnostic services. There were, in fact, more than 5,000 such procedures.
16 This mattered because there were many statements in the Respondent's written promotional materials which indicated that there could be out-of-pocket expenses in relation to services provided by doctors. One of these included a product sold by the Respondent called 'Gap Cover' which was designed to eliminate or reduce the size of any out-of-pocket expense relating to a doctor's fees (but which could not be purchased in relation to diagnostic services). The trial judge made this point about that material:
'171 If the applicant's contentions were correct, it would follow, as Medibank contended, that on the applicant's view of things, the documents relied upon by the applicant must also convey a representation to the consumer that Medibank indemnifies members for all costs of all included procedures – which number well over 5000 – not just radiology and pathology. And no one could possibly believe or infer that, because, apart from anything else, it flies in the face of repeated warnings about out-of-pocket expenses in the Cover Summaries, the Member Guide and other product documents.'
(emphasis added)
17 No appeal has been brought from the finding in the last sentence. Indeed, as will be seen shortly, it was a finding consistent with the way the Appellant ran its case. So the statements did not give rise to a representation that there would be no out-of-pocket expenses in the case of doctors because there were repeated warnings about out-of-pocket expenses for doctors in the materials.
18 The Appellant's response to this problem was that those warnings did not apply to diagnostic services. Its argument on this topic had matured throughout the course of the litigation. Initially, when the case was opened by senior counsel for the Appellant, the argument was that diagnostic services were not provided by medical practitioners at all. This exchange occurred between the trial judge and senior counsel for the Appellant:
'His Honour: And do you say that these diagnostic services aren't provided by doctors?
Mr Armstrong: No, your Honour. They're provided by diagnostic service providers, pathologists or radiologists. And Medibank itself draws a distinction between doctors and those other medical service providers because – I'm not sure if it's in this version of the member guide, but certainly a later version makes clear that the gap cover program is only available for doctors' charges and it's not available in respect of diagnostic – sorry – pathology and radiology services.
His Honour: I can't even think – do we call radiologist doctors or not in common – I should know something like that, but I ---
Mr Armstrong: I don't know, your Honour. I don't know.
His Honour: Someone will know.
Mr Armstrong: Yes.'
19 This turned out to be wrong. Although patients rarely meet their pathologists or radiologists there is no doubt that these professionals are doctors even if they often work for significant commercial entities. By the time of the appeal this was no longer in contest. The collapse of that front forced the Appellant to retreat to the proposition that even if the providers of diagnostic services were in fact doctors, they would not be perceived as such by consumers. It was necessary for the Appellant to retreat no further, however, and to hold, if it could, this redoubt. Why? If it abandoned altogether the position that diagnostic service providers were to be understood as standing apart from the position of doctors then the logic of its argument would lead unavoidably to the proposition that there would be no out-of-pocket expenses for all medical services. The trial judge recorded the Appellant's submission about this [165] which strongly suggests that at trial the Appellant accepted that consumers would not have thought there would be no out-of-pocket expenses for services provided by doctors:
'165 The applicant submits that "the impression conveyed by Medibank's communications was that diagnostic service providers were a different category of medical service provider relative to other doctors and specialists" and the "implication was that diagnostic charges were in a category of 'MBS treatments' for which members need not be concerned about out-of-pocket expenses notwithstanding that doctors could charge such expenses". Put another way, it was contended that the relevant documents suggested that a distinction was to be drawn, for the purposes of construing Medibank's descriptions of its insurance products in the marketing and product information, between medical practitioners who are doctors and medical practitioners who are pathologists and radiologists.'
(emphasis added)
20 It does not really matter now whether that was the Appellant's case below or not. The trial judge found at [171] that consumers understood that there might be out-of-pocket expenses in the case of services provided by doctors and no appeal has been brought from that conclusion. What that means is that it is critical for the Appellant to establish that the relevant class of consumers (a concept I return to below) would have understood diagnostic service providers not to be doctors to whom could apply the clear statements (accepted by the trial judge) that there could be out-of-pocket expenses. A concerted effort was mounted at trial to do so. The trial judge recorded this attempt and rejected it at [170].
21 So the position on appeal is this:
it is an unchallenged finding of fact that consumers do not distinguish diagnostic service providers from the services of other medical practitioners; and
it is an unchallenged finding of fact that the Respondent's promotional materials did not convey a representation to consumers that they would not be left with an out-of-pocket expense in the case of services provided by medical practitioners.
22 It is then useful to turn to the Appellant's challenge to the interpretation placed by the trial judge on the words 'cover', 'included', 'excluded', 'restricted' and 'towards' in the promotional materials (such as the cover guide). This was ground 2(b)(i) of the notice of appeal and the contention was that his Honour had given these words a meaning that ordinary and reasonable members of the target audience would not have given them. The relevant portion of the reasons are at [168]-[169]:
'168 The simple fact is that diagnostic services are not restricted or excluded procedures, and nothing in the documentary evidence on which the applicant relies suggests otherwise. As Medibank contended, a reasonable consumer would therefore, correctly, understand radiology and pathology services to be included services. The contrary conclusion urged by the applicant relies on the notions that the word "cover", wherever used, must be read to mean "entirely cover" or "indemnify" and that Medibank's documents would lead consumers to believe (contrary to the fact) that diagnostic service providers are a different species of medical practitioner or specialist, which, in turn, would lead the consumer to believe that "diagnostic charges were in a category of MBS treatments for which members need not be concerned about out-of-pocket expenses".
169 The word "cover" cannot be read to mean "entirely cover" or "indemnify". In my view, no reasonable consumer would understand the word "cover", used in the context of statements describing medical procedures to which the policy responds, to mean "indemnify". As Medibank submits, "[a] reasonable consumer would understand the words as they are clearly intended: to identify the types of medical procedures covered by one policy as opposed to another. There is a clear and obvious distinction between the risks covered by insurance and the benefits payable for those risks".'
(emphasis in original)
23 In its written submissions the Appellant developed the point this way:
'[The trial judge] accepted that diagnostic services were presented as "included" in cover, but he focused on the meaning of "cover" and immediately attributed to all consumers an insurance lawyer's awareness of distinctions between "the risks covered by insurance" and "the benefits payable for those risks". He implied an unstated qualification – that "cover" necessarily means partial cover – and rejected out of hand the possibility that one reasonably-open interpretation for an ordinary person might be that a covered or included service was for one for which they were no longer exposed to a risk of out-of-pocket costs. In each respect his Honour erred.'
(emphasis in original)
24 This submission should be rejected for two reasons. First, the meaning his Honour gave to the words was the same meaning that the Appellant accepted at trial they bore in relation to the services of doctors. His Honour did not give them a special or technical meaning; rather, he just refused to give them a different meaning for diagnostic services. A curious feature of the Appellant's argument – surely indicative that something has gone awry – is that it requires one to give the word 'cover' a different meaning in the consumer's mind depending on whether one is talking about doctors (in which case cover means only that benefits are payable which can result in an out-of-pocket expense) or about pathologists and radiologists (in which case it means full indemnity). This is impossible to accept. Secondly, there is in any event no substance to the suggestion that the trial judge substituted an insurance lawyer's views for those of the ordinary reasonable consumers. If anyone was doing that it was the Appellant by suggesting that 'cover' meant full indemnity. Ground 2(b)(i) should be rejected.
25 Next it was submitted (in Grounds 1 and 2(a)) that the trial judge had failed to have regard to the different characteristics of the persons to whom the statements were directed. It does not appear to have been in dispute that the target audience represented a full cross-section of the Australian adult community who had an interest in purchasing policies from the Respondent or renewing policies already held. The Appellant's written submissions contained the following propositions:
'Medibank's communications were directed to members of the public who might be investigating acquiring or changing their private health insurance. That target audience was so large and varied as virtually to constitute the entire Australian adult population. That audience included "the astute and the gullible, the intelligent and not intelligent, the well-educated and the poorly educated".
The learned judge did not address the range of characteristics of that target audience, either in his core reasoning at [161] to [178] or in obiter at [179] to [216]. Then, he did not examine the range of reasonable interpretations that ordinary members of that wide audience might draw from the Medibank marketing and member communications.'
(citations omitted)
26 The question which the trial judge was required to ask himself was what the effect of the conduct was on a reasonable member of the class of consumers involved: Campomar Sociedad Limitada v Nike International Limited [2000] HCA 12; 202 CLR 45 ('Campomar') at 85 [103]. It would certainly be contrary to that approach to ask whether any particular persons within the target audience were misled. However, as I understood the Appellant's submission it was not that the trial judge should have asked himself that prohibited question but rather that, before asking himself whether a reasonable member of the class would have been misled, he should first have acquainted himself with the various sub-classes and their respective characteristics within the target audience. I think there may be some issues of analysis around how the construct of the reasonable consumer is affected by an initial assay of the various factions within the target audience. However, this Court heard no argument on that issue and it would be inappropriate to take that further. It is convenient to assume, therefore, that the trial judge ought to have addressed himself to the range of characteristics of the target audience before asking what the effect of the conduct would have been on the reasonable member of that target audience and that he erred in not doing so.
27 But to make that assumption would only have the consequence of requiring this Court to come to its own view on the same issue. Taking into account the various aspects of the target audience identified in the Appellant's submissions does not cause me to doubt the correctness of the trial judge's conclusions on this issue. This is because it is not in dispute that the Respondent's materials did not convey to consumers that there would be no out-of-pocket expenses in the case of medical services provided by doctors. It is also not in dispute that consumers do not distinguish diagnostic service providers from doctors. Once one has arrived at that position, it is difficult to see how the trial judge could have arrived at any conclusion other than the one at which he did. A consideration of the range of aptitudes of the target audience cannot be material whilst those findings remain unchallenged. Grounds 1 and 2(a) should be rejected.
28 Of course, the Appellant's case was not just based upon the Respondent's written materials. Interactions between the Respondent and its customers involving purely these written materials were limited to those who purchased online and the post-purchase written documents provided to all customers by post after sale.
29 But the Appellant's case also focused on what had been said to the customers who purchased policies as a result of attending one of the Respondent's stores or retail kiosks or, alternatively, as a result of speaking to one of the sales representatives in a Salmat call-centre by means of a telephone. Forensically, this required the Appellant to prove its case in relation to those interactions. What was that case? It was the case set out at ¶¶9-10 of its concise statement:
'9. Medibank markets its Policies to Australian consumers through different channels, including (primarily) via websites, and via sales representatives operating by telephone, in-store or through web-chat using prepared scripts (the Marketing).
10. Since at least early 2012, in the Marketing in respect of each policy, Medibank:
(a) stated that, or to the effect that, the Policy would provide cover for all MBS items, save to the extent that a service was "restricted" or "excluded";
(b) stated that, or to the effect that, where a member received a service that was restricted or excluded, the member might incur an Out-of-pocket Expense; and
(c) did not identify In-hospital Diagnostic Services as restricted or excluded, although other restricted or excluded services were explicitly identified.'
(emboldening in original)
30 This was in fact the same case the Appellant made about the cover summaries which was at paragraph 11:
'11. Further, after selecting and purchasing a policy, members received written summaries of their cover under the policy (Cover Summaries). The Cover Summaries repeated the messages described in paragraph 10.'
(emboldening in original)
31 Mr Brownfield, the Respondent's Divisional General Manager for Customer Channels, gave evidence for the Respondent about the significance of these channels. In the financial year ending 30 June 2012, for example, 47% of the Respondent's customers joined through purchases made through the retail channel and 36% through policies sold via a call-centre (online was 17%). So the retail and call-centre part of the case was a very important aspect of the Appellant's case.
32 The Appellant pursued an orthodox way of proving what had occurred although, as will be seen, it encountered some obstacles in doing so. As a first step, it tendered the written materials which had been provided to the Respondent's retail employees and the sales representatives in the Salmat call-centres. These materials were as follows:
(a) Retail stores and retail kiosks
'Medibank Retail Network – My Best Practice Training Manual' dated 11 June 2013.
A program (or tool) called 'SPOT'. This was an interactive price calculation tool which was used to help retail staff compare the Respondent's products for a customer to identify a suitable cover and to create a personalised quote for the customer. Screenshots from the SPOT tool were put in evidence.
A document entitled 'Tips and Tricks to using SPOT' which described how the SPOT tool might be used.
(b) Salmat call-centre
Salmat staff had access to the SPOT tool.
Salmat itself generated an online based script for its call-centre staff using a system called Mi-Cat. Although these scripts were generated by Salmat it was not suggested that the Respondent was not responsible for their substantive content. Versions of these Mi-Cat documents were in evidence. The Mi-Cat system ceased being used on around 10 July 2013. It is not clear what replaced it.
33 The Appellant's contention in relation to the retail stores was, therefore, that it could be inferred that what appeared in the manual, the SPOT tool and the Tips and Tricks document was likely to have been conveyed to consumers. In the case of the call-centres, the proposition was that it could reasonably be inferred that what was in the Mi-Cat printouts and the SPOT tool was conveyed to consumers.
34 The second step was that these materials contained textual passages that were the same as those appearing in the cover summary (i.e. the reference, inter alia, to out-of-pocket expenses for restricted services). For the same reason that that document conveyed the diagnostic cover representation it could be seen that the same matter must have been represented to customers in-store and via call-centres.
35 It might have been possible to dispose of this argument on the same basis as the cover summary. This would have involved accepting the first step in the Appellant's argument, i.e., that if the representation were made in materials provided to staff and call-centre representatives then it was probably made to the public as well. But the second step would, on this view, be rejected because it would be accepted that customers were aware that there might be out-of-pocket expenses for doctor's fees and that the public would not distinguish doctors from diagnostic service providers.
36 The trial judge did not go down that path because he never got to the second step. This was because the first step was impaired by evidence led by the Respondent. This was the evidence of Mr Brownfield whom I have already mentioned above. He was the person with overall management responsibility for the processes by which new members joined the Respondent and the interactions that customers had with the Respondent during the course of their membership. However, he took up that role only on 17 October 2016. As the Appellant pointed out, that was sometime after 2014 when the events with which this appeal is concerned largely occurred.
37 Mr Brownfield gave evidence about many of the Respondent's promotional materials including evidence about the retail and call-centre channels. He described the current way that retail staff interacted with a customer in-store. He referred to the manual and the SPOT tool to explain what they were. His evidence about how they were used was as follows:
'Medibank does not instruct or require its retail staff to follow a script when speaking with customers. Rather, Medibank trains its retail staff about its insurance policies and makes available to staff various tools and documents to assist staff in dealing with customers. Staff can select from these various resources when speaking with customers and responding to customer queries.'
38 This was evidence about present practices but the case appears to have been approached on the basis that it could be inferred that the practices in 2014 were the same as they were in 2017 when Mr Brownfield gave evidence. The Appellant did not submit that such an inference ought not to be drawn but it did seek to downplay the significance of Mr Brownfield's evidence on the basis that insofar as it related to events in 2014 Mr Brownfield's knowledge was surely derivative since he did not commence in his position until 2016. There are three problems with that submission. First, Mr Brownfield's evidence was about the Respondent's present practices so the premise of the submission is incorrect. A more fruitful argument might have been that it should not be inferred that the practices in place since 2016 were the same as those prior to 2014. Such a contention might have encountered, however, the rhetorical question: why not? The difficulties in answering that question would have been exacerbated by the fact that the Appellant elected not to cross-examine Mr Brownfield. In any event, one need not linger on this issue.
39 Secondly, although the Appellant characterised Mr Brownfield's evidence as hearsay during the course of this appeal, it took no such objection at trial. Its submission is, therefore, an invitation to downplay the weight that is to be given to Mr Brownfield's evidence. This raises essentially an issue about its reliability. To gauge its reliability (on the erroneous hypothesis that it actually was hearsay) it would have been necessary to ascertain from Mr Brownfield the reasons he was willing to act on the correctness of what those who reported to him had informed him about events prior to 2014, i.e., why it was not reliable. That would have required Mr Brownfield to be cross-examined.
40 Thirdly, in that situation the Appellant's argument reduces to the bald proposition that all hearsay which has been admitted should be given little weight simply because it is hearsay. Such a proposition would render the hearsay rule unnecessary – why object to evidence if it can be given no weight? In any event, it is contrary to authority: Federal Commissioner of Taxation v SNF (Australia) Pty Ltd [2011] FCAFC 74; 193 FCR 149 at 158 [25] applying what was said by Evatt J in Walker v Walker [1937] HCA 44; 57 CLR 630 at 638 ('I deny the proposition that, merely because it was "hearsay" and therefore inadmissible, it is necessarily deprived of probative value').
41 Consequently, the Appellant remains saddled, as it was at trial, with Mr Brownfield's uncontested evidence that the manual and the materials provided to retail staff were not used as scripts. The trial judge acted on this evidence to conclude that the first step in the Appellant's argument (the drawing of an inference of likely retail employee behaviour from the contents of the material) should not be taken. This his Honour did at [187]-[188] where he recorded the Respondent's argument about this before himself accepting that argument:
'187 Senior counsel [for the Respondent] also submitted that:
(1) Mr Brownfield "gave unchallenged evidence that Medibank makes available to staff various tools and documents to assist staff in dealing with customers".
(2) To the extent that the applicant contends that those documents were the only documents used by Medibank staff, "there is simply no evidence to support that submission, and it's contrary to the evidence".
(3) The applicant asks the Court to "infer or assume that the only thing that's communicated from a Medibank retail store staff person to the consumer is word-for-word, some words that appear in the training manual …" and that submission is "frankly absurd … because a training manual is a training manual. And one's common experience is you don't walk into a retail store and the retail staff member has a training manual in front of them and is reading from the training manual as they speak to you". He continued: "… They can't go any further than that. Now, it is a simple question of evidence. The evidence they bring to the Court to prove that these representations were made to consumers at the point of sale is simply this training manual". He submitted that what he described as "the high point" of the applicant's case "fails immediately" and that the Court should not be satisfied "that this is what members were told and, with some precision of the sort of words, a representation of this kind was conveyed to members".
188 In my view, for the reasons advanced by Medibank, the Court is unable to conclude on the balance of probabilities that the diagnostic cover representation was at any relevant time made to members, or potential members, of Medibank in a retail store. It is not possible to make such a finding on the speculative basis contended for by the applicant in the absence of any actual evidence about interactions between Medibank staff with its customers in retail stores. Further, it is inherently unlikely that the training materials could ever have been used as a rigid script for such interactions and, indeed, Mr Brownfield swore that they were not. It is also inherently unlikely that the interactions took place without due regard to the brochures and other documents available to consumers at the retail stores. In the event, whether or not it is inherently unlikely, the applicant has failed to discharge its burden of proof in relation to this element of its case.'
42 By Grounds 2(b)(ii) and (iii) the Appellant submitted that the trial judge erred in thinking it relevant that it did not call any member of the target audience and by not accepting the relevance of the Respondent's failure to call any witness as to its training or practices.
43 However, neither of these arguments, even if correct, goes anywhere. Taken at their highest the best that could be said for the Appellant is that the statements appearing in the retail materials were conveyed to the customers in-store. But this is not enough for the Appellant to succeed. Nothing in the retail materials rises any higher than the statements appearing in the documents entitled 'Cover Summary Basic Hospital' set out above at [7]. For the reasons I have already given, it does not convey to the target audience the diagnostic cover representation. For that reason, even assuming the Appellant were right about the use by the retail staff of these materials, the case would still fail. Grounds 2(b)(ii) and (iii) should be rejected with respect to retail channels.
44 It is then necessary to turn to the call-centre evidence.
45 The evidence concerning what occurred in the Salmat call-centres was incomplete. Mr Brownfield explained the existence of Salmat's Mi-Cat materials but not how they were used. He also explained that they ceased being used in July 2013. He did not give evidence in relation to the Mi-Cat materials that they were not used as a script. To look at the Mi-Cat materials is to see immediately why Mr Brownfield gave no such evidence. It is clear that the Mi-Cat materials were a computer generated script designed specifically to guide a call-centre sales representative through a call with a customer and telling them precisely what to say at each juncture of the call.
46 It is difficult to know what to make of Mr Brownfield's evidence that the Mi-Cat system had ceased being used by Salmat in July 2013. It is difficult to imagine, however, that it ceased using instruction sets of that kind (nor does Mr Brownfield suggest that to be so). In this Court neither party made anything about the expiry of the Mi-Cat system. The trial judge, as will be seen, did not regard the matter as material either. In that circumstance, I propose to proceed on the basis that materials like the Mi-Cat materials were in place at the relevant time.
47 The point which the Appellant sought to extract from the Mi-Cat materials was a passage which, in substance, had exactly the same content as the cover summary set out above. It submitted, in relation to that material, that 'there is nothing [in the Mi-Cat material] to suggest that there is a major category of routine services – namely in-hospital diagnostic services – that is likely to be medically necessary, is covered by Medicare, is not identified as a restricted or excluded service, but nevertheless is not subject to the costs-protection that was the reason for the customer seeking [private health] insurance in the first place'.
48 The Respondent's response to this at trial was to submit that the passages relied upon by the Appellant did not constitute the entire universe of information conveyed by the Respondent which, significantly, included the Welcome Packs. It also advanced very similar arguments to those which it had advanced against the cover summary document.
49 The trial judge dealt with this at [195]:
'195 I shall return below to consider in more detail the submissions that arise out of some of the language used in the Salmat documents, including the use of the word "towards", the definition of "Restricted Services", and the information that is provided to new customers in the Welcome Pack. As to the Salmat documents specifically, it is not possible for the Court to draw the inferences sought to be drawn by the applicant with respect to the use of those documents. In particular, the Court cannot be satisfied, on the balance of probabilities, that the documents in evidence constitute the only information with which new customers must necessarily be provided. As to the submission that the Salmat materials constitute the only evidence of the instructions given to call centre operators and that it should be inferred that it "reflects the tone … of the information provided by the operators", I am not satisfied that the evidence allows me to draw that inference. In any event, the Court is unable to conclude, on the balance of probabilities, that the diagnostic cover representation was at any relevant time made to members, or potential members, of Medibank via call centre operators. It is not possible to make such a finding on the speculative basis contended for by the applicant in the absence of any actual evidence about interactions between Medibank staff and customers.'
50 This is largely the same way that his Honour dealt with the retail store material. However, this reasoning appears to overlook the fact that the Salmat materials plainly were scripts (e.g. instructions to the user saying 'MUST READ IN FULL') and that Mr Brownfield's evidence did not suggest otherwise. For that reason, I would accept the Appellant's argument that his Honour erred in dismissing as speculative any attempt to prove the diagnostic representation 'in the absence of any actual evidence about interactions between Medibank staff and customers'. It was not speculative at all. The Mi-Cat materials were plainly scripts; it was an inevitable inference that what was in the scripts was said to consumers. Additional evidence of interactions between staff and consumers was not necessary. If it was to be shown that something other than what was in the Mi-Cat scripts had happened that would be different. For example, if the Respondent wanted to show that the apparent effect of something appearing in the scripts was otherwise than it appeared, then it might want to call some evidence about this. I would therefore uphold ground 2(b)(ii) and (iii) to the extent that they concern his Honour's view that the Mi-Cat materials were not sufficient on their own.
51 However, I do not think this ultimately assist the Appellant. The representation case disclosed by the Mi-Cat material is the same in form as that disclosed in the cover summary document. It therefore has to confront the fact that it does not refer to diagnostic services. This brings it face to face with the trial judge's finding at [171] that consumers understood that there would be out-of-pocket expenses for doctors and his finding at [170] that they did not distinguish diagnostic service providers from doctors.
52 Once one arrives at that point it is impossible to see how anything in the Mi-Cat materials could do better than the cover summary. An ordinary reasonable consumer who spoke with a call-centre representative would have understood that there could be out-of-pocket expenses in the case of the services of doctors and they would not have distinguished diagnostic service providers from doctors. It seems to me therefore that the Appellant's case fails on this point. Grounds 2(b)(ii) and (iii) should be rejected.
53 It is not entirely clear whether the Appellant pursued an argument that the trial judge had erred in fact in concluding that the diagnostic cover representation had not been made although this did appear to be the contention in ground 1. Nevertheless the Appellant's written submissions tended to suggest that the error lay not so much in the finding that the representation had not been made but rather in the legal errors addressed above.
54 On the assumption that such an argument was pursued I would not be disposed to accept it. Such an argument would need to bring itself within the principles in Warren v Coombes [1979] HCA 9; 142 CLR 531. It would need to be demonstrated that the refusal of the trial judge to draw the inference that the diagnostic cover representation had been made had involved error. I do not see how it is possible to arrive at a different conclusion to the one the trial judge arrived at whilst it remains accepted that consumers did not understand from the Respondent's activities that they would not have out-of-pocket expenses for doctor's charges but also did not distinguish the position of doctors from that of diagnostic service providers. To the extent that Ground 1 made this contention it should be rejected.
55 The Appellant's next argument was that the diagnostic cover representation was the dominant message of the Respondent's marketing. If that were correct it followed that it could not necessarily be diluted by subsequent disclaimers. This was ground 2(b)(iv). The Appellant placed particular reliance upon what was said by the High Court in Australian Competition and Consumer Commission v TPG Internet Pty Ltd [2013] HCA 54; 250 CLR 640 ('TPG'). That case reminds one that the misleading nature of a dominant message may not be successfully neutralised by the provision of later accurate information for by then the harm may already have been done in that the customer has been enticed to treat with this merchant rather than some other merchant. On this view of affairs, customers would be enticed to deal with the Respondent because of statements made by in-store staff or call-centre staff along the lines of the cover summary.
56 It is useful to ask, however, what this dominant message could have been at this point in the transaction. It cannot have been the diagnostic cover representation because the marketing materials do not mention diagnostic services at all. It can only have been a representation that there would be no out-of-pocket expenses for all medical services. It is only the later statements in the Welcome Pack that can have left consumers with the impression that there could be out-of-pocket expenses for doctors. But the Appellant does not contend for such a representation.
57 The difficulty for the Appellant is well-illustrated by assuming in its favour that its submission based on TPG is correct. What follows is that the subsequent statements in which it is plainly indicated that there may be out-of-pocket expenses for doctors is insufficient to dispel the dominant message. But what is the dominant message? It is not the diagnostic cover representation. It is instead a representation that there will be no out-of-pocket expenses in the case of any medical service. What follows from an application of TPG to that factual constellation is the conclusion that that representation was made (rather than the diagnostic cover representation). But this is a case which the Appellant has never advanced. Indeed, at trial it accepted that that representation was not conveyed.
58 The difficulty is that the primary judge found the representation never to have been made. TPG is a case concerned with whether a misleading dominant message may be not misleading by later qualification. The question in this case, however, is not about whether the conduct is misleading. It is whether the representation was ever made at all. This suggests that TPG has little to do with a case like this: see especially 654-655 [47]-[49] where the Court explained the different position of consumers in Parkdale Custom Built Furniture Pty Ltd v Puxu Pty Ltd [1982] HCA 44; 149 CLR 191 and TPG.
59 The Appellant's last contention in relation to the diagnostic cover representation was that contained in ground 2(b)(v). To understand this ground one needs to know that the Respondent had a number of customers who at the date of termination of the MPPAs (defined below at [73]-[74]), were, in fact, receiving in-hospital diagnostic services from diagnostic service providers with such MPPAs. Such customers went from the position that they had no out-of-pocket expense in relation to the provision of diagnostic services to a position where, after the termination of the MPPAs, they found themselves having to pay such an expense. These persons have been referred to in the litigation as the recipient members.
60 At trial the Appellant tendered statements of benefits for some of these customers which showed that they had not had an out-of-pocket expense prior to 1 September 2014. The Appellant submitted to the trial judge that the recipient members would have noticed that they handed over their Medibank card to the provider and then paid no out-of-pocket expenses. The trial judge dealt with this submission at [219]:
'219 In my view, there is, with respect, nothing in this submission. First, it is not immediately clear how a member would be able to identify diagnostic services on the face of the statement. Secondly, and in any event, whatever a reasonable ordinary Medibank member would have made of the statements of benefits, nothing in them could be read or construed as relevantly contradicting the information provided to members in the Welcome Pack and other documents, including brochures, and the information available online, about the possibility of incurring out-of-pocket expenses.'
61 On appeal the Appellant contended that the trial judge had failed to address its principal contention, namely, that the Respondent provided a 'no gap' experience to these recipient members. According to the Appellant '[b]y doing so it represented to them that their policies did protect them from out-of-pocket costs for these services'.
62 There are a number of difficulties with this. First, as the Respondent correctly points out, not receiving an out-of-pocket expense in respect of a diagnostic service could be equally caused by either of:
the diagnostic service provider only charging 100% or less of the schedule fee; or
the diagnostic service provider charging more than 100% of the schedule fee and the Respondent doing something to ameliorate the gap.
63 The Appellant's case assumes that a person who received no gap would infer the second rather than the first of these. But no ready explanation is advanced as to why that would be so. Secondly, the statement of benefits identifies the services rendered by their MBS item number. For a consumer to understand what was being said they would either need to know what the MBS item numbers were for diagnostic services or to look them up. Thirdly, it is quite possible that there might be item numbers where there was no out-of-pocket expenses (because the provider only charged the MBS fee) and others for which an out-of-pocket expense was payable. It is very difficult to extract anything clearly from such a document.
64 The trial judge was therefore quite correct to reject the case based on the statement of benefits. Nor, leaving aside the statement of benefits, do I think the fact that the recipient members were spared out-of-pocket expenses for diagnostic services, helps to advance the case on the diagnostic representation case. If an ordinary reasonable consumer did not believe, as a result of the Respondent's promotional activities, that they would not be left with out-of-pocket expenses for doctor's services and that diagnostic service providers were not distinguishable relevantly from doctors, how does it assist to know that the recipient members had out-of-pocket expenses for diagnostic services? It is difficult to see that that fact could have any effect on the other two. Not having to pay an out-of-pocket expense for a diagnostic service could not logically impact on one's views as to whether one would have expenses of that kind in relation to doctors generally; nor is it possible to see why it would have any impact on one's ability to distinguish diagnostic services from those of doctors.
65 I would reject ground 2(b)(v).
Medibank Brand: The Notice Representation
66 The Appellant alleged that the Respondent had also represented to consumers that it would give prior notice to its members of any detrimental change to the level of benefits it would pay under its policies. Such a change had occurred, so the Appellant alleged, but the Respondent had not given notice. Consequently, it had engaged in misleading and deceptive conduct. The Respondent denied that it had made the representation alleged.
67 It is useful to start with the representation itself. The Appellant relied upon the Medibank Member's Guide which was in effect from 16 January 2012. Relevantly, it said this:
'Changes to the terms and conditions of your membership
Please note that all members of Medibank Private are subject to the Fund Rules, which set out the terms and conditions of their cover, as well as the services we pay benefits for. The Fund Rules can be changed from time to time with the approval of the Minister …. If any changes will have detrimental effect on your entitlement to benefits we will provide you with reasonable notice in writing before they are due to come into effect.'
68 This refers to the 'Fund Rules'. The trial judge dealt with these at [77]-[80] in terms which were not suggested to be controversial. The Private Health Insurance Act 2007 (Cth) assumes, but does not appear to require, that a private health fund will have rules. In the Dictionary in Schedule 1 this is said:
'rules, of a private health insurer, means the body of rules established by the insurer that relate to the day-to-day operation of the insurer's *health insurance business and (if any) *health-related business.'
69 Section 93-20(2)(c) relevantly provides:
'93-20 Keeping insured people up to date
…
(2) A private health insurer must ensure that, if a proposed change to the insurer's *rules:
…
(c) is informed about the proposed change a reasonable time before the change takes effect; and
…'
70 A person who acquires a private health insurance policy from Medibank becomes a member of Medibank's Health Benefits Fund. Membership of that fund is governed by the Fund Rules which consist of 'Main Rules' and 'Schedules'. The Main Rules were available in-store and on the Respondent's website. They were also summarised in the Member Guides. The Schedules defined the benefits which were payable in relation to the different products which the Respondent sold. These were not provided to members but were summarised in the Member Guide. The Fund Rules also specified the relevant premiums.
71 The Fund Rules defined the benefits payable to members in respect of hospital treatments, which included benefits for medical procedures, in accordance with the requirements of the Private Health Insurance Act 2007 (Cth). The Fund Rules also defined additional benefits that became payable to a member if Medibank had an arrangement or agreement in place with a private hospital or medical practitioner and the member received hospital treatment from that hospital or practitioner.
72 The implications of that statement are not immediately obvious and require some further explanation. By way of example, the Respondent might have agreed with a particular provider of diagnostic services that the Respondent would pay 10% on top of the schedule fee for its members. The Fund Rules would then provide for that additional 10% to be a benefit. The net effect would not, however, be the receipt of the additional 10% by the member, but rather the amount would pass to the diagnostic service provider.
73 There were three main categories of agreement or arrangement which the Respondent could enter into and which, if in place, provided for additional benefits to be paid to members in that sense. These were Hospital Purchaser Provider Agreements ('HPPAs'), Medical Purchaser Provider Agreements ('MPPA's) and GapCover Arrangements.
74 An HPPA is an agreement between Medibank and a private hospital pursuant to which the hospital accepts payment in satisfaction of amounts that would otherwise be owed by a member to a hospital. An MPPA is an agreement between the Respondent and a medical practitioner pursuant to which the medical practitioner accepts payment by the Respondent in satisfaction of amounts that would otherwise be owed by a member to the medical practitioner.
75 The Respondent had MPPAs with a number of Diagnostic Service Providers. When a medical practitioner had provided an in-hospital diagnostic service to a member, these provided for the Respondent to pay the diagnostic service provider the difference between the relevant schedule fee and the diagnostic service provider's fee. The diagnostic service provider agreed in return not to charge more than a specified fee. MPPAs also commonly provided that either party could terminate the agreement on the giving of 60 days' notice, on most occasions following an initial period of 12 months.
76 On 1 September 2014 the Respondent abolished most of its MPPAs. The effect of this was that in many cases patients who received in-hospital diagnostic services began to receive accounts from the diagnostic service providers. This charge was the difference between the fee charged by the diagnostic service provider and the schedule fee for the service; that is to say, the members became exposed to a gap payment which had previously not been present.
77 At trial, the Appellant submitted that the Member Guide equated the Fund Rules with an entitlement to benefits. Consequently, although couched in language about changes to the Fund Rules, the ordinary reasonable consumer would have understood the statement as being concerned with benefits more generally. Further, the Appellant sought to obtain some benefit from Part E of the Industry Code which, under the heading 'Changes to Hospital Contracting Arrangements', said this:
'We recognise that while not constituting a change to hospital benefits for the purpose of Section 2 above, changes to hospital contracting arrangements between a fund and a hospital can affect a consumer. We understand that requirements for notification of consumers of such changes and transition arrangements are included in the relevant agreements …'
(emphasis added)
78 The trial judge rejected this submission on the basis that the termination of the MPPAs did not effect any change to the Fund Rules. He noted that the benefit payable to a member remained the same both before and after the termination. His Honour illustrated this with an extract from the Fund Rules:
Charge | Benefit |
… | … |
Exceeds the MBS fee and the Professional Attention is provided under a Contract with the Medical Practitioner. | 25% of the MBS fee, plus an amount up to the difference between the MBS fee and the charge, in accordance with the Contract with the Medical Practitioner. |
79 It is true that no change was made to this rule although in each case where an MPPA had been terminated this would appear to mean this rule was no longer relevant since the service would not have been provided under a 'contract with the medical practitioner'. However, neither party made anything of that and it does not appear to have any impact on the logic of his Honour's reasoning.
80 The Appellant also submitted at trial that its case was assisted by notices which the Respondent had sent to its members which notified them of changes to the Fund Rules. These were of two kinds: changes to the amount of the premium and changes to the benefits payable. Here the point was that this reinforced the representation relied upon by the Appellant.
81 The trial judge concluded that there had been no change to the Fund Rules (which was an agreed fact). His Honour therefore concluded that the Respondent had not acted contrary to the assurance in the Member Guide that if there were any changes to the Fund Rules which would have a detrimental effect on a members' entitlement to benefits it would provide them with reasonable notice in writing before the changes were due to come into effect. In relation to the Industry Code his Honour did not think that it helped the Appellant. Indeed, the Industry Code appeared to recognise that changes to the agreement of the kind under discussion were not changes to benefits. His Honour rejected the argument based on the change notices. The fact that change notices had been sent in the circumstances contemplated by the Fund Rules and the Private Health Insurance Act 2007 (Cth) could not assist in making good a case that a notice needed to be sent when neither the Fund Rules nor the Act required it.
82 On appeal the Appellant submitted that the trial judge had applied a lawyer's construction to the words of the Member Guide. The Member Guide did not suggest that there was a distinction between changes to benefits resulting from changes to the Fund Rules 'compared to changes to benefits resulting from other causes'. Further, the trial judge had failed to examine the range of reasonable interpretations that an ordinary member of the target audience might draw. Instead, he had imputed to all consumers an understanding of a highly technical distinction found 'only within the machinery clauses of the Fund Rules'. The Appellant submitted this was contrary to TPG at [53] and Australian Competition and Consumer Commission v Coles Supermarkets Australia Pty Ltd [2014] FCA 634; 317 ALR 73 ('Coles') at 100 [160]. The Appellant also submitted that his Honour had erred in his treatment of the change notices. It was said that the notices did not correct anything in the Member Guide and that if the latter was relevantly misleading then so were the change notices. His Honour had erred in attributing to members a sophisticated understanding of the Member Guide.
83 The Respondent took issue with this submitting that the difficulty for the Appellant was that the terms of representation were clear and that the Member Guide simply did not say what the Appellant sought to extract from it. As to the suggestion that the distinctions drawn by the trial judge were technical, the Respondent denied there was anything technical about them at all. The concept of changes to the Fund Rules was not a technical one. Likewise, his Honour had not failed to take account of the varying aptitudes of the target audience. In relation to the change notices, the trial judge was correct in his conclusion that they did not convey the representation alleged. There was no avoiding the agreed fact that the change notices involved a change to the Fund Rules and hence they could not assist the Appellant's argument.
84 Viewed from a certain perspective there is apparent force in the Appellant's submission. The statement that members would be notified of any changes to Fund Rules which would have a detrimental effect on a member's entitlement to benefits could, in some contexts, be seen as incomplete. It is literally correct but if it formed part of a strategy on the Respondent's part to entice persons into dealing with the Respondent then it would probably be misleading unless qualified. For example, if the statement appeared as the headline component of a marketing campaign like this:

then it would probably have been misleading not to tell potential customers that they would not be notified of the termination of MPPAs which would have the effect of potentially creating a gap payment when there was none before. It would not be to the point, were this a case of headline advertising, that the headline statement was literally correct. Further, that correcting or fuller information is available elsewhere would not dispel the misleading and deceptive nature of the headline advertisement. So in TPG it was misleading to market an ADSL2+ plan at $29.99 per month without also pointing out with at least equal prominence that it had to be bundled with a telephone service costing $30 per month. And in Coles, it was misleading to advertise bread as freshly baked bread which had been par-baked in advance and whose baking was merely completed in store. In that case 'freshly baked' and similar statements were identified as the dominant message.
85 However, the Appellant's case on the notice representation is far from a headline advertising case. To explain why it is necessary to say something of the document containing the alleged representation, the Member Guide. The trial judge dealt with it at [133]-[134]. It was a post-sale document which was sent as part of a Welcome Pack to new members. It was sent by email and within 48 hours of the member signing up. The Member Guide was not the only item in the Welcome Pack. It also contained a cover summary, a brochure entitled 'Quick Tour of Your Cover' and a statutorily required document known as a standard information statement. The Member Guide was also made available on the Respondent's website and at its retail stores.
86 Turning to the Member Guide effective 16 January 2012 itself, the first thing to note is that it is 52 pages long. At page 3 there is a table of contents including an entry for 'Changes to the terms and conditions of your membership' which is said to start at p 9. On the first page the document describes itself this way:
'This guide is a summary of the main Fund Rules and policies of Medibank Private affecting members who are Australian residents.'
87 The passage the Appellant relies on is at the foot of p 9. What is apparent from this is that the Member Guide is not promotional material in the sense that it is not seeking to advertise the Respondent's services. By definition, those who receive the Member Guide have already signed up. This is not to deny its capacity to be misleading per se but only to underscore that it does not involve a headline advertising statement such as those in TPG ('ADSL2+ for $29.99 per month') or Coles ('freshly baked bread'). There is no sense in which the Member Guide can be seen as enticing a consumer into a transaction: see TPG at 654-655 [48].
88 From that flows a second matter. The Member Guide provides information about the Fund Rules in what may fairly be interpreted as an attempt to speak in plain English. As such it is to be seen as an information source. In that context, the statement about changes to the Fund Rules it contains is literally correct. But because it is not part of a stratagem to draw people in the fact that it might be seen as incomplete in itself is of much less moment. This because an analysis of its capacity to mislead needs to be understood in a context which includes the fact that the Member Guide also gave an accurate description of the effect of contractual arrangements with medical practitioners providing in-hospital services (p 24-25). That discussion was not a surreptitious footnote to the section dealing with changes to the Fund Rules. Rather, both were part of a non-marketing document serving as a source of information. In my view, any consumer who decided to embark on a reading of the Member Guide would not be reading it in the fleeting way inherent in the Appellant's submission.
89 In those circumstances, the trial judge was correct to reject this case. I would reject grounds 2(c)(i)-(iv).
The ahm Brand: Diagnostic Cover and Notice Representations
90 As already mentioned, the Respondent offered private health insurance under two brands, the Medibank brand (considered above) and also the ahm brand. The Medibank business was much larger than the ahm business with the latter contributing only 5% of the Respondent's revenues. The principal difference between ahm and Medibank was that ahm was strictly an online business and did not maintain retail stores.
91 The Appellant began its submission by observing that its case in relation to ahm was comparable in volume and complexity to the language used in the case relating to the Medibank brand. Yet despite that the trial judge had despatched its entire case in a single sentence. That is not, however, a correct statement. His Honour dealt with the matter this way:
'221 The diagnostic cover representation is also pleaded in respect of ahm branded products. As outlined earlier, ahm is an online and telephone sales business. Its private health insurance products differ from those branded as Medibank products to some extent, so the relevant documents and the material available on the ahm website differs from the Medibank material.
222 Although the applicant referred to a number of specific ahm documents in an annexure to its written closing submissions, in the end it did not contend that any documents in evidence relating to ahm were relevantly or materially different to the evidence adduced in respect of Medibank or that any different question of construction or principle arises in respect of that evidence for the purposes of the diagnostic cover representation case.
223 Because the diagnostic cover representation case was conducted on that basis, it follows, for the reasons given above in respect of the evidence adduced concerning Medibank branded products, that the applicant has also not established that the diagnostic cover representation was made in respect of the ahm branded products.'
92 That was in relation to the diagnostic services representation. In relation to the notice representation his Honour set out the relevant portion of the ahm Member Guide at [227]-[228]. He then dealt with that at [242]-[243]:
'227 It was not suggested that this version of the Member Guide is not an adequate exemplar. The ahm Member Guide (effective 11 June 2013) is similarly worded:
Fund Rules and policies
When you join ahm Health Insurance, you agree to be bound by our Fund Rules. These are available online at ahm.com.au or you can call us on 134 246 to request a copy. Our Fund Rules, policies and benefits are subject to change from time to time with the agreement of the Minister … If we make changes that affect your cover in a detrimental way we will let you know in writing prior to the change taking place.
228 The reference to "policies and benefits" in the 11 June 2013 ahm Member Guide was deleted from ahm Member Guides on and after April 2014.
…
242 As for the ahm Member Guide effective between June 2013 and April 2014, the applicant says that its case with respect to the notice representation is "particularly strong" because it amounts to a representation that ahm would notify members of any detrimental change to "policies and benefits". I also do not accept that submission. For these purposes, there is no relevant distinction between the expressions "fund rules", "policies" and "benefits" – the benefits payable for each policy are defined by the Fund Rules. As Medibank submitted:
[a]ny changes to benefits payable under a policy must involve a change to the Fund Rules. The Fund Rules prescribe that benefits must only be paid in accordance with the Fund Rules. So too, any change to a "policy" must involve a change to the terms of the schedule to the Fund Rules that define the benefits payable in respect of the policy.
243 Further, the ministerial approval to any relevant change, which is referred to in both the Medibank and ahm Member Guides, is something that is only required for changes to the Fund Rules. The termination of the MPPAs required no such approval.'
93 The Appellant's first submission is that the trial judge failed to give adequate reasons. The Appellant does not cavil, however, with the trial judge's statement at [222] that the Appellant 'did not contend that any document in evidence relating to ahm was relevantly or materially different to the evidence adduced in respect of Medibank'. In that circumstance, it is difficult to see any deficiency in the trial judge's reasons.
94 In fact, the only matter which the Appellant pointed to in its submissions in this Court as to the difference between the ahm materials and the Medibank materials related to the use of words 'partially covered' in the ahm Quick Guide and 'partial cover' on its website. This was, as it happens, also its only substantive ground of appeal relating to the ahm brand.
95 The Quick Guide corresponded to the cover summary used in the Medibank business. Under the heading 'What's partially covered' there was a discussion of restricted services (discussed above). The equivalent statement in the Medibank cover summary was 'Things we pay limited benefits for'. The Appellant submitted that the ahm language was even more reassuring than the Medibank language. Even assuming this difference was pointed out to the trial judge, the point is without merit. The ahm wording is different to the Medibank wording but not in a way which is material.
96 The Appellant also submitted that the Quick Guides were not adequate disclaimers to correct the diagnostic cover representation. But for the same reasons as in the case of the Medibank brand, the diagnostic cover representation was simply not made. The disclaiming effect of the Quick Guides is irrelevant.
97 In relation to the notice representation, the Appellant acknowledged that the trial judge had given some reasons but it submitted that these were inconsistent. The inconsistency arose this way. At [235] and [239] the trial judge had rejected the Appellant's contention in relation to the Medibank brand that the Member guide equated Fund Rules with an entitlement to benefits. The purpose of that argument was to allow the statement in the Member Guide that any changes to the Fund Rules which would have a detrimental effect on the members' entitlement to benefit to serve as a representation about members' benefits. The effect of the submission, if accepted, was that the statement would have required notification of benefit reductions even if they did not result from changes to the Fund Rules (i.e. arising from a termination of an MPPA instead).
98 But, submitted the Appellant, at [242] the trial judge had taken the opposite position:
'242. As for the ahm Member Guide effective between June 2013 and April 2014, the applicant says that its case with respect to the notice representation is "particularly strong" because it amounts to a representation that ahm would notify members of any detrimental change to "policies and benefits". I also do not accept that submission. For these purposes, there is no relevant distinction between the expressions "fund rules", "policies" and "benefits" – the benefits payable for each policy are defined by the Fund Rules. As Medibank submitted:
[a]ny changes to benefits payable under a policy must involve a change to the Fund Rules. The Fund Rules prescribe that benefits must only be paid in accordance with the Fund Rules. So too, any change to a "policy" must involve a change to the terms of the schedule to the Fund Rules that define the benefits payable in respect of the policy.'
99 So the submission is that in dismissing the Appellant's argument at [242] his Honour had done so by equating benefits with the Fund Rules but at [235] and especially [239] he had rejected an argument that the Member Guides equated the two.
100 There is an inconsistency in the trial judge's approach but it does not materially impact the correctness of his Honour's reasoning. At a formal level, it is correct to say, as the trial judge did at [242], that because the benefits are specified in the Fund Rules there is a close relationship between the benefits stated in the Fund Rules and the Fund Rules themselves. I would accept that there is a certain inconsistency with what the trial judge said at [239]:
'239 Further, I reject the submission that the Medibank Member Guide "equates" the Fund Rules with "the entitlement to benefits". It does no such thing.'
101 However, it is clear that the basic point his Honour was making was that the termination of an MPPA does not affect the benefits which are payable under the Fund Rules. Neither the Fund Rules nor the benefits they provide for are altered by the termination of an MPPA. What does happen is that the termination of an MPPA may make a different benefit rule applicable to the member. That, however, does not involve any change in the benefits for which the policy provides and in that regard his Honour's analysis is correct regardless of the suggested inconsistency. The basic problem is that the termination of an MPPA does not effect a change in the Fund Rules or the benefits. I would reject Grounds 3-5 insofar as they apply to ahm.
102 For all those reasons, I would dismiss the appeal insofar as it relates to misrepresentations. For the reasons given by Beach J I would dismiss the unconscionability case. The Appellant must pay the Respondent's costs.
I certify that the preceding one hundred and two (102) numbered paragraphs are a true copy of the Reasons for Judgment herein of the Honourable Justice Perram |
Associate:
REASONS FOR JUDGMENT
MURPHY J:
103 I have had the benefit of reading the separate reasons of Perram J and Beach J in draft form. I agree with the orders they propose and generally agree with their reasons.
I certify that the preceding one (1) numbered paragraph is a true copy of the Reasons for Judgment herein of the Honourable Justice Murphy. |
Associate:
Dated: 20 December 2018
REASONS FOR JUDGMENT
BEACH J:
104 I have had the considerable advantage of reading in draft form Perram J's reasons concerning appeal grounds 1 to 5. I agree with those reasons and have nothing to add on those topics. Accordingly, it is only necessary to address appeal grounds 6 and 7 concerning statutory unconscionability.
105 Before addressing these grounds directly it is necessary to deal with some introductory and background matters.
106 The ACCC's case at trial concerning s 21 of the Australian Consumer Law (ACL) relevant to appeal grounds 6 and 7 related to the conduct of Medibank in terminating most of its Medical Purchaser Provider Agreements (MPPAs) with in-hospital pathology and radiology providers concerning pathology and radiology services (diagnostic services) without giving notice of doing so to all of its members.
107 The ACCC's case at trial was that Medibank prior to termination of the MPPAs perceived that if members were told of the change there was a significant risk that they would lapse; the reference to "lapse" refers to members ceasing to insure with Medibank. It was also perceived, so the ACCC said, that publicity about the change would impact Medibank's brand and reputation, and have a negative impact on the lead-up to Medibank's initial public offering.
108 It was said that Medibank knew that consumers including its members:
(a) were unlikely to enquire about and would have difficulty enquiring about the relevant change;
(b) were likely to find out about the change when they were at their most vulnerable;
(c) were likely to be distressed by the change; and
(d) were likely to incur costs for which they did not budget.
109 The ACCC's case at trial was that Medibank's decision not to notify members of the relevant change, or as it described it implementing the non-disclosure strategy, was unconscionable because:
(a) Medibank knowingly exploited what was said to be a lack of understanding by its members of private health insurance (PHI);
(b) Medibank knew that its decision not to notify members would cause them harm; and
(c) not notifying members was unethical because it breached industry norms, which were said to be enshrined in the Private Health Insurance Act 2007 (Cth) (PHIA) and the Private Health Insurance Code of Conduct (Industry Code), to provide consumers with current information about their entitlement to benefits.
110 The ACCC says that the evidence before the primary judge established that Medibank, despite knowledge of members' expectations about cover, despite knowledge that members relied on Medibank for information about changes affecting benefits, despite having ready means of giving notice, despite anticipating surprise for affected members if it did not give notice, and despite foreseeing the distress that some affected members would experience, instead preferred to pass the risk of that surprise and distress to affected members rather than openly alerting all members and bearing the commercial consequences of doing so. In all the circumstances, the ACCC says that such conduct involved a sufficient departure from right practice as to justify its characterisation as unconscionable.
111 Now the primary judge rejected such a case. But the ACCC contends that he was in error in doing so for the reasons summarised in appeal grounds 6 and 7. Before discussing these grounds it is useful to further expand on the ACCC's case thesis before the primary judge and before us. Essentially, it was put to us that his Honour only properly addressed one of two stages in Medibank's internal processes relevant to the ACCC's unconscionable conduct case, and then the wrong stage when dealing with the non-disclosure strategy.
ACCC's case thesis
112 The ACCC's unconscionable conduct case delineated two separate stages in Medibank's internal processes. First, there was the process leading to the decision to terminate most of the MPPAs; I will refer to this decision as the "diagnostics funding decision". The ACCC says that this process and decision were the responsibility of Medibank's "Provider Networks and Integrated Care" (PNIC) division, and centred around the "Medical Funding Review" (MFR) undertaken from late 2013 until April 2014, the first stage of which became the diagnostic funding review. Medibank's witness Dr Andrew Wilson was involved in the PNIC process and was the head of the PNIC. From my review of the contemporaneous documents, which I will discuss later, that is an accurate description of the first stage. Second, there was a process leading to what has been described as the non-disclosure strategy in respect of the diagnostics funding decision. According to the ACCC, this was the responsibility of Medibank's "Customer Centred Healthcare" (CCH) division, and was formulated via a separate process from May 2014. The ACCC submitted that Dr Wilson had no relevant involvement in the CCH process.
113 In terms of Medibank's structure at the relevant time, generally speaking the PNIC comprised one half of Medibank's health insurance business. Its remit was to review and oversee Medibank's healthcare purchasing. Contrastingly, the CCH division was responsible for acquisition, retention and relations with members.
114 The ACCC says that information first recorded in the PNIC process was cited by CCH personnel at important points in their deliberations. And it is contended that the question of what they knew or should have expected had to be shaped by the information they were shown to have had. In submissions to us on appeal, the ACCC stressed that it was necessary for us to consider the PNIC process in detail in order to appreciate the significance of critical steps in the CCH process. I have looked at the relevant contemporaneous documents on this aspect that were drawn to our attention on the appeal and will discuss these in more detail later. For the moment, let me return to how the case was put to us by the ACCC on this appeal.
115 Early in the MFR, Medibank collated various survey-based reports regarding consumer/member understanding of medical costs and insurance cover. These included the "Ipsos Report", a "TH?NK" report summarised in the "Sibbick memo", and the "Atchison Report". I will identify and discuss these documents later. According to the ACCC, these reports identified low levels of consumer understanding and wide expectations that members would not pay anything but their excess. It is said that they reported that members became particularly dissatisfied when they were surprised about gaps, and that members were more likely to be surprised by diagnostic gaps than any other medical gap. According to the ACCC, one noteworthy observation in the Sibbick memo was that "Seven out of ten members had no discussions about Medical OOPs [out-of-pocket costs] prior to their admission [to hospital]".
116 According to the ACCC, Medibank was aware at the relevant time of the limited effectiveness of past initiatives promoting "informed financial consent" (IFC). Importantly, so the ACCC said, all the principal recommendations in the Sibbick memo were to the effect that Medibank should be proactive in alerting members to potential out-of-pocket costs (OOPs), to avoid "surprise" for them.
117 Further, the ACCC says that the Ipsos and TH?NK reports were cited in a November 2013 presentation to the PNIC "Leadership Team" (PNIC LT) concerning the MFR. It is said that the presentation treated the reports as reliable. It reviewed various risks associated with the possible benefit change for diagnostic services. It also touched on the issue of member communications. So too did a later 2013 "Key Risks" document.
118 Before proceeding further, I would make one point concerning the use of the expression "benefit change". The termination of most of the MPPAs i.e. the diagnostics funding decision had a financial consequence to many members in potentially increasing their exposure to OOPs, but it was not strictly a direct benefit change as such. Nevertheless, I will for the moment use the phrase "benefit change" as understood in that more informal sense.
119 According to the ACCC, in January 2014 an Implementation Risk Report was presented to the PNIC LT. Again it referenced the Ipsos, TH?NK and Atchison reports, without criticism. It is said that it set out observations broadly reflecting those reports, including that members would "tolerate" reasonable gap charges, but that surprise at unexpected OOPs did cause "dissatisfaction" and that the surprise element of gaps should be removed wherever possible.
120 The ACCC then says that discussions progressed to the Medibank Executive Committee (ExCo) in mid-February 2014. Dr Wilson was a member of ExCo. The PNIC division's presentation on the MFR again cited the Ipsos and other reports without criticism and repeated elements of the Implementation Risk Report. Importantly, so the ACCC says, the February presentation to ExCo introduced reference to a "Ramsay analysis", as "indicat[ing] that lapse of claiming members will result in a positive net financial outcome for Medibank".
121 Now the Ramsay analysis was not itself in evidence before the primary judge. But according to the ACCC it was apparent from other evidence that it was to the effect that where the cost of claims from high-claim members outweighs the revenue earned from their premiums, moderate lapse within that high-claim subgroup can produce a net financial gain for Medibank, which Medibank could reinvest in marketing to recruit new lower-cost members.
122 Now in evidence before the primary judge, Dr Wilson had no independent recollection of how the Ramsay analysis was addressed in ExCo. He confirmed that it was the only model prepared by Medibank as to lapse resulting from the benefit change. But at trial he described it as "flawed". However, according to the ACCC, the only flaws he identified related to a line item irrelevant to the impact on affected members, and to his view that it overestimated likely lapse effects.
123 The ACCC then says that a working group meeting overseeing the MFR was held in April 2014. It set task-lists for, inter alia, "draft[ing] member comms", "develop[ing] complaints handling", and "ensur[ing] staff levels [were] adequate to manage additional caseload". It also foreshadowed a proposal for ex gratia payments to some affected members.
124 The ACCC then points out that the PNIC LT met on 10 April 2014 and considered an "Implementation Proposal". Importantly, according to the ACCC, this proposal not only referenced the Ramsay analysis, but it modified it specifically for the diagnostics funding decision, re-calculating the financial consequences for Medibank upon certain assumptions such as 114,000 "impacted" members (the "Ramsay/114" analysis). Now Dr Wilson thought that the analysis overstated potential lapse by about 50%. Nevertheless, so the ACCC says, he agreed that to the extent that there was a risk of lapse, it was a risk that Medibank was prepared to take, and it would be at the expense of the affected members.
125 The April PNIC LT meeting then approved the decision to terminate most of the MPPAs i.e. it made the diagnostics funding decision. That decision was then ratified by ExCo.
126 The ACCC then emphasised the second stage. It says that the earliest CCH division documents regarding the "Member Communications approach" cited the Ramsay/114 analysis. Such documents also highlighted a medium risk that if there was a general requirement to communicate the reduction in benefit to members, that communication might cause members to lapse. According to the ACCC, at about the same time Medibank's Corporate Affairs team responsible for media relations expressed reservations about the diagnostics funding decision, believing that it represented a reputational risk for Medibank and that it may be portrayed as Medibank removing benefits from its members. In a May communications report Corporate Affairs recommended a "reactive communications strategy … the aim is to keep communications contained".
127 The ACCC then says that the CCH Communications Manager circulated among the proposed members of the CCH division's implementation steering committee (Steering Group) a recommendation that "Medibank and ahm not … communicate this change to members. Rather we take an 'educational' approach around Informed Financial Consent…". The proposed members were also sent the PNIC division's April 2014 Implementation Proposal, including its Ramsay/114 analysis.
128 According to the ACCC, the sequence of internal CCH presentations and correspondence that followed showed that the Steering Group participants expected that providers would continue to charge diagnostic gaps and that some members would be surprised by new OOPs, assumed that most members would tolerate reasonable OOPs, and recorded that initiatives to remove the surprise aspect of gaps should be investigated. The ACCC says that the CCH staff cited, without criticism, Sibbick memo findings like "seven in ten members had no discussions about medical out of pocket costs".
129 The ACCC says that despite this background information about the limited effectiveness of IFC procedures, and members' likely surprise and dissatisfaction if Medibank were not proactive about informing them of the benefit change, the CCH personnel proposed merely a "comms strategy to be centred around helping members understand OOPs, their rights to IFC and how to minimise OOPs … messaging will support the proposition of 'call us before you go to hospital'". The "comms strategy" was to be "passive" and "avoid comms not targeted to members who are identified as going to hospital". In short, so the ACCC says, the communications strategy adopted was that more information about IFC generally would be included in member literature, but specific information about the diagnostics funding decision would be provided only where members contacted Medibank. And this strategy was adopted. Medibank amended various brochures and guides to reflect it. But the revisions were in general terms, encouraging members to make enquiries about costs generally. The amendments did not squarely disclose the diagnostics funding decision.
130 Now the ACCC says that by at least June 2014 Medibank had notified diagnostic providers about the diagnostics funding decision. Medibank also notified other stakeholders, including the Private Health Insurance Ombudsman (PHIO). It also prepared its frontline staff for an anticipated surge in member complaints, preparing "Fact sheets" that blamed providers for OOPs. It anticipated that staff would confront some challenging member situations and so planned a limited program of ex gratia payments to members who complained enough. The ACCC says that this evidences an actual expectation on the part of Medibank of surprise and distress for some members. But according to the ACCC, Medibank still did not initiate a proactive notice to members, either in general or to targeted cohorts.
131 The diagnostics funding decision took effect from 1 September 2014. According to the ACCC, members did encounter unexpected OOPs. By mid-November its implementation manager reported that "while savings are flowing according to budget, the member experience has been characterised by high out of pockets by some providers, no [IFC], and a letter accompanying the account that blames [Medibank]". Indeed, member complaints were such that the ex gratia payment program was extended at least twice into January 2015.
132 Let me now turn to the appeal grounds and the ACCC's assertions of error. I will return to the evidence before the primary judge later.
Appeal Grounds 6 and 7 and the ACCC's contentions
133 Ground 6 asserts that the primary judge erred in holding that Medibank did not engage in unconscionable conduct in contravention of s 21 of the ACL. It is said that the primary judge ought to have found that Medibank engaged in unconscionable conduct having regard to some or all of the following facts and circumstances:
(a) Medibank knew that many members with Medibank hospital insurance or ahm hospital insurance were of the erroneous belief that they would not incur any OOPs during a hospital admission;
(b) Medibank made the relevant representations, which were false, misleading or deceptive; I would note here that his Honour found that no such representations were made, and Perram J has disposed of the appeal grounds on that question;
(c) Medibank knew that a significant proportion of its members made no enquiries about OOPs prior to admission to hospital;
(d) prior to the diagnostics funding decision many members did not incur OOPs for in-hospital diagnostic services because the provider's charges were borne by Medibank;
(e) Medibank knew or had reason to suspect that if, upon making the diagnostics funding decision, it informed its members that they might be required to pay OOPs for in-hospital diagnostic services, a not insignificant number of them would have ceased to be members of Medibank's hospital fund thereby reducing its financial benefit from the diagnostics funding decision;
(f) Medibank expected that the average OOPs for members, following implementation of the diagnostics funding decision, would be $151 for each pathology service and $83 for each radiology service;
(g) Medibank knew or had reason to suspect that the expense in sub-paragraph (f) would be a distressing burden to meet for many members, particularly for members suffering from chronic diseases and particularly where they were surprised by the expense;
(h) Medibank knew that if members were made aware of the possibility that as an in-patient they might incur OOPs for in-hospital diagnostic services, a not insignificant number of them would have sought to make arrangements to avoid or reduce that expense;
(i) the Industry Code required, or reflected a norm of conduct requiring, Medibank to give prior notice of a change to benefits like the diagnostics funding decision;
(j) Medibank was easily able to notify its members about any changes to their benefits;
(k) despite the matters in sub-paragraphs (a) to (j), Medibank adopted and implemented the non-disclosure strategy; and
(l) Medibank adhered to the non-disclosure strategy even after:
(i) it had received a higher volume of complaints than it had expected at the time the diagnostics funding decision was made;
(ii) it knew from at least mid-October 2014 that some of its members had not been told by diagnostic providers about the OOPs that they might incur for in-hospital diagnostic services before they received those services; and
(iii) it knew from at least November 2014 that some diagnostic providers had increased their charges for in-hospital diagnostic services after 1 September 2014.
134 Ground 7 asserts that the primary judge, in considering whether Medibank had in all the circumstances engaged in unconscionable conduct, erred in:
(a) holding that the ACCC's claim that Medibank had engaged in unconscionable conduct contrary to s 21 of the ACL, was dependent upon it being established that Medibank had contravened ss 18, 29(1)(g), 29(1)(m) or 34 of the ACL;
(b) finding that the evidence of Dr Wilson was relevant to Medibank's state of mind when it adopted and implemented the non-disclosure strategy, despite Dr Wilson having no involvement in the formulation and implementation of that strategy; and
(c) failing adequately to consider the evidence as to the formulation and implementation of the non-disclosure strategy.
135 Re-ordering the grounds for convenience and by reference to grounds 7(a) and (b) first, the ACCC in summary contended the following.
136 First, it is said that the primary judge erred in holding that the unconscionable conduct claim could not succeed unless the ACCC also proved misleading and deceptive conduct. It contended that this was not the case articulated in its concise statement, the trial was not conducted on that basis, and it was not correct in law.
137 Second, it is said that his Honour erred in finding that the unconscionable conduct case could not survive in the face of Dr Wilson's unchallenged testimony.
138 As to this, the ACCC says that the subjective state of mind of an individual officer of a corporation is only one factor and is not dispositive in assessing whether the conduct of the corporation ought to be regarded as contrary to right practice.
139 Further, it is said that Dr Wilson's state of mind was irrelevant because he had no role in or responsibility for the communications strategy. He was a complete stranger to the relevant CCH decision-making process. This meant, in turn, that there was no relevant cross-examination that could be directed to Dr Wilson in lieu of the absent Mr Goldman. Generally, Dr Wilson's personal views could not be attributed to Medibank for the purposes of the communications strategy decision.
140 Moreover, so the ACCC submitted, so far as the primary judge had regard to Dr Wilson's criticisms of the Ramsay/114 analysis, Dr Wilson conceded that he could not recall any discussion of it at the April 2014 ExCo meeting. And in any event according to the ACCC, the flaws Dr Wilson identified were peripheral to the present issues. Moreover, there was no evidence as to how the relevant CCH personnel regarded the analysis, save that they cited it repeatedly across several formal presentations without any recorded criticism.
141 As to grounds 6 and 7(c), the ACCC in summary contended the following.
142 The ACCC pointed out that although the primary judge held that the unconscionable conduct case must fail for want of misleading conduct, nevertheless he did proceed to consider some aspects of the ACCC's case. But according to the ACCC his reasons focused almost entirely on the PNIC's justification for the diagnostics funding decision (see at [259] to [273]). As the ACCC described it, his Honour "despatched in three short paragraphs" the whole of the evidence regarding the relevant decision, being the CCH decisions as to the communications strategy ([279] to [281]). And he rejected, by reference to Dr Wilson's views, the ACCC's contention that the knowledge or reasonable expectations of Medibank's decision-makers must be taken to have been defined by the information available to them (at [292]). And finally he rejected, by reference to Dr Wilson's views, any relevance of the Ramsay/114 analysis (at [298]).
143 But the ACCC says that once it is accepted that Dr Wilson's views were irrelevant, it is necessary for the documentary record of the CCH process to be examined with care, which it is said that his Honour failed to do; I will address this further in the next section of my reasons. Now Medibank denied that the Ipsos or Sibbick conclusions were adopted by the CCH decision-makers. Alternatively, it characterised their internal exchanges as "drafts". But the ACCC points out that Medibank did not call the relevant decision-makers to give evidence. Accordingly, so the ACCC says, the only evidence of what the relevant decision-makers expected or could reasonably have expected was to be ascertained from the documentary record.
144 According to the ACCC, what the documents that we were taken to on appeal demonstrate is that the CCH decision-makers knew or had reason to expect that:
(a) many members under either brand were of the erroneous belief that they would not incur any OOPs during a hospital admission;
(b) a significant proportion of members made no enquiries about OOPs prior to admission to hospital;
(c) members who paid OOPs that were not expected or were higher than expected were more likely to lapse than members who paid OOPs but had been accurately informed; moreover, as a percentage, members were more likely to be surprised by greater than expected diagnostic gaps than any other medical gap;
(d) prior to the diagnostics funding decision many members did not pay the diagnostic gap, because the gap was paid by Medibank;
(e) if Medibank had informed its whole membership base that they might be required to pay diagnostic gaps, it risked a significant number of them ceasing to be members, thereby reducing its financial benefit from the diagnostics funding decision;
(f) the average diagnostic gap for members following implementation of the diagnostics funding decision was expected to be $151 for each pathology service and $83 for each radiology service; and such additional expense would be a distressing burden to meet for many members, particularly for members suffering from chronic diseases and particularly where they were surprised by the expense;
(g) if members were made aware of the possibility that as an in-patient they may incur diagnostic gaps, a significant number of them would have sought to make arrangements to avoid or reduce that expense;
(h) there was a norm of conduct set by or aligned with the Industry Code that insurers would notify members of detrimental changes such as those flowing from the diagnostics funding decision; and
(i) Medibank was readily able to notify its members about any changes to their benefits.
145 According to the ACCC, the contemporaneous documents also show that Medibank adhered to the non-disclosure strategy even after it had received a higher volume of complaints than it had expected, it knew from at least mid-October 2014 that many members had not been advised by their diagnostic service provider about the OOPs they could incur for in-hospital diagnostic services, and it knew from at least November 2014 that some diagnostic service providers had increased their charges for in-hospital diagnostic services after 1 September 2014.
146 Further, according to the ACCC, Medibank sought to excuse its decision not to give proactive notice to members on the grounds that it had not itself caused any misapprehensions on their part as to cover, and that it was sufficient to encourage them to contact it before treatment or to require providers to inform them about the diagnostic gap. But according to the ACCC, Medibank was on notice of the poor understanding among members, that they tended not to enquire about OOPs before treatment, and that IFC protocols were unreliable. The ACCC said that these considerations and the thrust of the Industry Code showed that members were likely to rely on Medibank to give notice about changes such as those flowing from the diagnostics funding decision. Further, according to the ACCC, Medibank had ready means of giving notice. And it actually foresaw sufficient surprise and distress among members to plan the ex gratia payment program for members who complained enough. But according to the ACCC, Medibank preferred to take those risks of surprise and of lapse among affected members, rather than openly alerting all members, squarely confronting the reputational risk it had created, and perhaps upsetting the assumptions modelled in its Ramsay/114 analysis.
147 According to the ACCC, Medibank knew or should have expected that its communications strategy risked surprise and distress for members who would encounter personal costs that otherwise they could have planned for or avoided. And it is said that Medibank did so to its commercial advantage, principally to reduce reputational risk and to confine membership lapse risks to its higher-cost members.
148 According to the ACCC, Medibank's conduct was, in all the circumstances, unconscionable. And it is said that the primary judge was in error in not so finding.
The evidence before the primary judge
149 Given that one of the ACCC's principal complaints is that the primary judge focused on Dr Wilson's evidence, which it says was not probative of the decision-making process concerning the communications strategy, to the exclusion of or at least at the expense of fully considering the contemporaneous record, I have perused the principal contemporaneous documents for myself. They disclose, in summary, the following chronological sequence.
150 On 30 July 2013, a presentation was made to the PNIC, on which Dr Wilson was cross-examined, titled "Ramsay Group Out-of-Contract: Membership & Financial Impact". This presentation and consideration, which was to be subject to a Deloitte's review, dealt with the implications of Medibank going out of contract with a significant national provider. It was not commissioned in or for the context of the process leading to the diagnostics funding decision. One of the implications of going out of contract was expressed in the following form:
Favourable Shift in Member Profile
– During an out-of-contract Medibank is likely to lose members with high utilisation and claiming profiles
– Medibank will have the opportunity to reinvest a significant proportion of short term financial gains into aggressive marketing and member acquisition targeted at members that have low claim and low churn profiles
151 It is to be noted that Dr Wilson gave evidence before the primary judge that the Ramsay analysis was flawed, including for the reason that although there might be a short term gain from the lapsing of a high claim member, there was likely to be a net negative position because of the life-time loss of premiums for that member; they could have been sick for a year but otherwise healthy for a life-time.
152 Further, in July 2013 scoping for an MFR was undertaken with the scope said to be:
The Medical Funding Review (MFR) will examine Medibank's benefit outlay expenditure on medical services for admitted patients and develop options for funding medical providers that reduce the cost burden on Medibank and/or members.
The objective of the MFR is to develop options for funding medical providers that:
– Reduce expenditure per service by Medibank and/or members; and
– Reduce expenditure per hospital episode by Medibank and/or members
The MFR will be split into four phases:
– Phase 1 – Market Context and Current State;
– Phase 2 – Medical Benefits Data Analysis;
– Phase 3 – Medical Funding Model Options; and
– Phase 4 – Implementation Considerations.
153 In terms of the project team, Dr Wilson was described as the "Project Sponsor". The diagram for the team structure showed Dr Wilson at the head with Mr Peter Derbyshire (project director) reporting to Dr Wilson. Reports to Mr Derbyshire included Jessica Chia (project manager), Rory Atchison (economic analysis), Deepa Kandasamy (data analysis) and Ann O'Gorman-Skarratts (medical services manager).
154 On 14 November 2013, Ms Chia made a presentation to the PNIC LT concerning the MFR. Various propositions were presented including the following:
(a) It was stated that "The project team recommends the 'Fund Gap' option for both pathology and radiology services". And that a recommended option is "All diagnostic providers to be paid the mandatory minimum benefits – 25% of the MBS [Medical Benefit Schedule] fee. Medicare would pay the other 75%".
(b) It was also stated that "The assumption has been members lapse if they pay diagnostic OOPs, but our analysis shows members accept reasonable OOPs especially if they are advised beforehand". So it was appreciated at this time that giving prior notice had potential advantages to all concerned. Various graphs were presented under this comment. On the graph titled "Paying a medical OOP does not result in membership lapse" was stamped "To be updated with Diagnostics (Pathology & Radiology) - Rory"; although the front page refers to 14 November 2013, other references appear to indicate that this is a later version as at 11 December 2013. So too, the graph titled "Likelihood of lapse increases when medical OOP exceeds $5000" was similarly stamped. Clearly, there was to be an update. Another version of the relevant slides in evidence which is more contemporaneous with 14 November 2013 does not have the graphs stamped.
(c) The 14 November 2013 version contained the following statement:
Half of PHI hospital members expect to pay a medical OOP
Think Global Medical Gaps Survey 2013 n = 500+ (In progress)
Preliminary Findings
1. Paying Medical OOP costs does not increase the member lapse rates
2. Medical OOP expenses are unlikely to be high on consideration list when joining Medibank
3. The lack of "No Gap" providers is unlikely to be the main cause of member lapse rates
4. The type of OOP expense did not impact NPS.
(d) The sources for the 14 November 2013 version were said to be:
(iv) Ipsos Member Hospital Experience Survey data for waves 3, 4 and 5;
(v) Ipsos Health Care and Insurance Syndicated Survey 2011 and 2013;
(vi) Think Global Medical Gaps Survey 2013; this was the report summarised in the Sibbick memo of 17 December 2013 that I will come to shortly;
(vii) Medibank EDW at 18/10/13; and
(viii) Project analysis.
(e) The 11 December 2013 version, which as I have said showed graphs to be updated, referred to references (d)(i), (iii), (iv) and (v) only. It also contained the following statement which indicated that paying an OOP may not affect the retention rate:
Member research in progress supports our previous findings
Think Global Medical Gaps Survey 2013 n = 1,508
Key findings
1. Paying a medical OOP does not impact intention to remain at Medibank
2. Paying a medical OOP does not impact likelihood to recommend Medibank
3. Paying a medical OOP does not impact members' perception of value
4. Significant difference in member satisfaction only when medical gap is $1000+
155 On 28 November 2013, Mr Rory Atchison of the PNIC and Mr Stephen Bunker, consultant, made a presentation titled "Impact of Medical Gaps on Membership Lapse" (Atchison Report) which presented as a summary finding from an analysis of Medibank hospital experience survey results that:
Finally, diagnostic gaps initially only adds to the impact on likelihood to lapse for diagnostic gaps > $500 but, as with doctor gaps, adds nothing once gap expectations are included in models.
156 Further, I would note that in evidence before the primary judge was a report dated 14 December 2012 which set out survey results from Medibank's members from October 2008 to September 2011, being described as "Wave 5" by the Ipsos-Eureka Social Research Institute (Ipsos Report). We were taken to various parts of this report during the hearing of the appeal, section 4.10 being the most relevant including Tables 48, 49 and 50. For the moment, it is only necessary to reproduce an extract from the "Executive Summary" as follows:
Gaps and formal consent
There were a number of significant differences in ratings of Gap and Formal Consent measures in Wave 5. While the proportion of patients paying excesses has remained stable in Wave 5, the proportion indicating they paid additional fees has increased in Wave 5. Further, in Wave 5, there was a significant decrease in the proportion who said they paid a co-payment or paid a gap.
Informed Financial Consent was calculated for each patient; a patient was considered to be informed if they had paid a gap and were advised of each gap before their hospital stay, regardless of whether the gap amount advised was accurate. In Wave 5, for the first time in the history of the survey, over half of patients (52.9%) were considered informed; this represents a significant increase from Wave 4 (49.9%).
All patients who paid a gap were asked whether the gap was greater than expected, less than expected, or as expected. For a treating specialist, four in five said the gap was as or less than expected, for anaesthetists, seven in ten said the gap was as or less than expected, for any other doctor, two thirds said the gap was as or less than expected – all results stable compared to Wave 4. For x-ray, tests and pathology however, the majority said the gap was as or less than expected – a significantly greater result compared to Wave 4 (53.8%).
Among those who paid a gap, the average gap paid was $1,324 in Wave 5, an increase of $96, since Wave 4 ($1,228). When asked who was responsible for informing patients of this expense, three in five patients mentioned the doctor / specialist treating them. Approximately two in five mentioned the hospital while over one third mentioned Medibank Private. Significantly fewer patients in Wave 5 said that whoever causes the Gap should inform them compared to Wave 4.
When asked whether they had negative feelings toward any person or organisation as a result of the gap, the largest mention was Medibank Private (30.8%).
157 Further, in an internal presentation dated 17 December 2013, although apparently presented in January 2014, Mr Joseph Sibbick of the GTM Team presented a document titled "Medibank Gaps Report" (the Sibbick memo). Apparently, Dr Wilson had not seen the Sibbick memo at the time and was unclear who Mr Sibbick was. In the section headed "Background and Objectives" the following was said:
It is a commonly held misconception amongst PHI holders that once you enter a hospital all costs are covered, therefore the reality can create displeasure amongst Members.
TH?NK has conducted qualitative and quantitative research to understand Members' awareness, knowledge and reaction to out-of-pocket expenses associated with 'medical' treatments, to gain insights on:
1. Potential impact on the brand, perceptions of value, likelihood to switch, and impact on joining a new fund as a result of an out-of-pocket experience
2. Focus on Medical OOP when selecting a PHI policy, compared to other factors
3. Opportunities to minimise the adverse impact of related out-of-pocket experiences, in order to improve Medibank's position with Members
4. Members' current expectations in terms of: who is responsible for OOP decisions / Understanding of how their medical cover works / Willingness to query OOP costs with their doctors / Expectation of OOP depending on the type of treatment / Expense claiming process – expectations and how Medibank can further assist
158 Other parts thereof referred to the ease of comprehension concerning the explanation of gaps and OOP. Reference was also made to the intentions of people to switch funds after experiencing OOPs, with one metric suggesting that 30% would consider switching. It was also reported that "There are large portions of the member base who do not have a good understanding of PHI in general, particularly those who have not claimed on their hospital cover".
159 It was also reported that:
One third of Medibank members who experienced a medical out of pocket were surprised by it (because it was more than they were expecting to pay).
– Being informed (or not) prior to a hospital admission played a role in this surprise.
– Pregnancy patients were most likely to be surprised by the Medical OOP, while Chronic condition patients were most likely to be surprised by the Medical OOP being more than they thought.
– Seven in ten members had no discussions about Medical OOPS prior to their admission.
Large proportions of members expected that they would not be paying anything but their excess.
– Expectations for Medical OOPs were largely unmet for Claimers, particularly at the more expensive end of the scale ($1,000+)
– For Non-Claimers, the majority did not expect to pay Medical OOPs at all.
160 It would seem that this was acknowledging that a significant percentage of members did not well appreciate OOPs and that being informed beforehand removed the element of "surprise".
161 In relation to expectations and future intentions, the following was reported:
Having been educated about the opportunity to discuss costs prior to a hospital admission, 80% would take up that option.
However, eight in ten of those members would come to Medibank, while 66% would go to their specialist (Medibank advice would be to speak to the doctor/specialist).
Members were mixed in their intentions to switch doctors/specialists to avoid Medical OOPs, indicating that there are other factors in the decision beside cost.
– For those seeking treatment for chronic conditions, almost half would not change doctors to reduce Medical OOPs – possibly due to valuing continuity of care.
In terms of Medical OOP expectations, Claimers expected to pay more than Non-Claimers (for the appendix operation scenario), indicating that experiences can impact on expectations and again highlighting the knowledge gaps among Non-Claimers.
162 In terms of "surprise factor", the following was also reported:
Surprise factor had a greater negative impact than price
While the amount of paid expenses influenced the likelihood to consider switching providers, the "surprise" element of incurring unexpected OOP costs left a greater negative impression for members.
Non-claimers in particular were more likely to hold a "naïve" view that PHI would cover all medical expenses.
Members who paid medical OOP as well as excess were even more surprised, possibly because they already had a set excess $ amount in their mind.
163 Finally, under the heading "Be the most 'proactive' PHI provider", it was said that:
Being proactive is about thinking ahead, therefore start the conversation with your members regarding medical OOP expenses, before the need arises.
164 This seems to be suggesting the advantages of prior notice.
165 In January 2014, in a presentation titled "Diagnostic Funding Review" (in reality the MFR albeit with its focus at this time on diagnostic services) dealing with "Understanding the implementation risks of the '100% of MBS' recommendation for diagnostic services", it was stated under "Implementation Risk Assessment" the following:
The initial risk assessment found that most risks are able to be mitigated to acceptable levels, however the risk of diagnostic providers reacting in a 'worst case' manner and adversely impacting member experience and causing reputation damage needed further analysis.
The 'worst case' reactions considered in the following pages are:
1. Adverse member impact:
1.1 Refusing service to members
1.2 Upfront charging for MPL members
1.3 Unreasonable out of pockets
2. Brand and reputation damage due to:
2.1 Public media campaign
2.1 Communications to doctors / specialists
3. Damage to IPN / Sonic relationship
166 In terms of risk 1.3, the following was said:
– Member research and data analysis of claims has found that out of pockets for medical costs at reasonable levels does not significantly change members' likelihood to lapse
– This is probably partly due to the fact that these members are claiming and are therefore experiencing value in their PHI
– Member lapse tends to be associated with lower levels of product, poor recent interaction with MPL, age, tenure etc,
– If members were surprised by medical gaps then that did cause dissatisfaction, but the gaps themselves (up to approx $5,000) did not impact on intention to lapse or downgrade cover. Initiatives to remove the 'surprise' aspect of gaps should be investigated
– These findings have been consistent across 3 levels of analysis (see following page)
– MPL member claims data – 2012
– Think customer research – Nov 2013
– Member hospital experience survey – 2010/2012
– It should be noted that these findings do not directly test the situation that may arise with this initiative, ie widespread OOPs for diagnostics, negative public campaign, and competitive product advantage. However for this be a material risk it would require hospitals and specialists to advocate on behalf of diagnosticians that members switch PHI's to avoid diagnostic gaps – we consider this unlikely
It appears that members will tolerate 'reasonable' medical gaps, however the surprise element of gaps should be removed wherever possible
167 Again, that last part is reinforcing similar themes to those described above.
168 Under the summary of member impact and brand risk the following was said:
– Providers are unlikely to refuse service or require upfront payments
– Out of pockets will probably be charged by the diagnostic providers but are unlikely to drive significant member lapse, unless they are unreasonable
– Specialists may drive members to switch funds on the basis of competitive differential, but diagnostic providers relationships with members are not as strong and are unlikely to drive switching behaviour
– Public campaign could impact sales but competitors are unlikely to pursue claiming members
– IPO considerations and shareholder involvement are the remaining material risks
(Original emphasis.)
169 And in terms of the conclusion on risk assessment the following was said:
– Risk Assessment
– Risk of membership loss is low
– Risk of negative public campaign having a significant impact on brand or sales is low
– BUT, risk of public campaign impacting on IPO is high, and
– Risk for Sonic / IPN relationship is high if unilateral implementation occurs
170 What is significant to note was that these comments concerned a risk assessment as opposed to what was known or expected. But it was appreciated that there might be a potential risk concerning the IPO with the relevant decision and potentially prior notice.
171 In an ExCo presentation in February 2014 titled "Update on PNIC Strategy", there was a presentation on the MFR, albeit again described as the "Diagnostic Funding Review" with its focus on diagnostic services.
172 Under the heading "Consider option to pay all diagnostic benefits at a maximum of 100% of MBS and allow providers to charge out of pockets", the following was said:
– MPPAs would have to be terminated on expiry
– Diagnostic providers to be paid the mandatory minimum benefits only ie 25% of the MBS fee (Medicare pays the other 75%)
– Diagnostic providers would be allowed to charge members an out-of-pocket, (member research shows members would tolerate reasonable gaps)
– Size of annually recurring benefit opportunity is estimated at $24.6m ($17.5m pathology, $7.1m radiology). Impact of risk equalisation reduces benefit outlay savings to $16.1m – 34% reduction ($11.8m pathology, $4.3 radiology)
– Providers would be permitted to use our electronic claims submission processes as long as they charge members an OOP of less than $500 out of pocket per claim – the 'Gap Cover Scheme' would be used to control this
While the estimated recurrent benefit outlay saving is $25m the proposal carries the risk of dispute with diagnostic providers including Sonic
(Original emphasis.)
173 In a table headed "Risk of negative media and damage to IPN relationship remain high", the following was identified:
Ref | Risk | Impact | Initial Risk Level | Mitigation Action/s | Residual Risk Level |
1 | Providers charge out-of-pockets to members | Member dissatisfaction causing Increased lapse and reduced sales | L | ? Research indicates low risk of member lapse ? Campaign to promote informed consent and avoid member surprises | M |
2 | Requirement to communicate reduction in benefit to members | Communication may cause members to lapse | M | ||
3 | Providers require MPL members to pay up front in full | Member dissatisfaction causing Increased lapse and reduced sales | L | Considered unlikely as diagnostic provider have to get specialist or hospital to enforce as diagnostic provider not present at admission or when tests are ordered | l |
4 | Providers run negative media campaign | ? Interference with IPO ? Member lapse / lost sales | H | ? Run alternate campaign but this will just contribute to greater noise in IPO year ? Avoid conflict with providers by negotiating outcome or delaying implementation until after IPO | H L |
5 | Providers run negative campaign with specialists and hospitals | Member switch / lapse | L | Unlikely to get much traction as diagnosticians would struggle to get specialists and hospitals to champion their battle | M |
6 | Sonic cancels IPN alliance | Withdraw member benefit and lost opportunity to partner with IPN | H | Negotiate outcome with Sonic, offering delayed implementation and support to transition to OOP relationship with member | H |
7 | Increased calls from members and complaints to PHIO | Longer call wait times, PHIO involvement | L | Implementation planning and readiness | L |
8 | Competitor / aggregators promote benefit differential to main | Member lapse / lost sales | L | As per Ramsay experience competitors unlikely to promote to claiming members | L |
174 Again, this was setting out a risk assessment to the effect that inter-alia one medium risk was that communications with members about the termination of the MPPAs might cause some members to lapse. Further, there was a high risk in terms of potential effect on the IPO.
175 Further, it was concluded:
Analysis suggests that reasonable gaps do not drive lapse, especially if members are advised beforehand
– Member research and data analysis of claims has found that out of pockets for medical costs at reasonable levels does not significantly change members' likelihood to lapse
– This is probably partly due to the fact that these members are claiming and are therefore experiencing value in their PHI
– Member lapse tends to be associated with lower levels of product, poor recent interaction with MPL, age, tenure etc,
– If members were surprised by medical gaps then that did cause dissatisfaction, but the gaps themselves (up to approx $5,000) did not impact on intention to lapse or downgrade cover. Initiatives to remove the 'surprise' aspect of gaps should be investigated
– These findings have been consistent across 3 levels of analysis and member research (see appendix)
– Even if low levels of lapse do materialise, the Ramsay analysis indicated that lapse of claiming members will result in a positive net financial outcome for Medibank
It appears that members will tolerate 'reasonable' medical gaps, however the surprise element of gaps should be removed wherever possible
176 It was undoubtedly appreciated that to give members prior notice of the relevant change was advantageous. Further, the Ramsay analysis was referred to without demur, namely, that the lapse of claiming members caused by the relevant decision will result in a positive net financial outcome for Medibank.
177 It would seem apparent to me that Medibank perceived that an effect of terminating the MPPAs could be that it would achieve a potential benefit of chronic sufferers who were members lapsing. But it was also perceived that any financial benefit could be re-invested to the benefit of other members. There is nothing in the contemporaneous documents at this time that indicated any disagreement with either conclusion.
178 On 10 April 2014, an "Implementation Proposal for the Diagnostics Funding Review" was put to the PNIC LT. This has been described by the ACCC as the Ramsay/114 analysis. The minutes of meeting of the PNIC LT record that on that day the meeting was chaired by Dr Wilson with the minutes recording:
Recommendation to proceed with implementation plan as per presentation was approved. Confirm that changes will not require 'detrimental change' notification to members.
179 It would appear that the confirmation sought was to be based on an assessment of the legal requirements.
180 The proposal identified the following main risks:
The 3 main risks in implementing the 100% of MBS recommendation are:
1. Managing Sonic and the risk to the primary care strategy
2. Understanding the practical responses by diagnosticians, specialists and hospitals to the change that may create unintended consequences
3. Managing the timing of this initiative regarding internal readiness and other disruptive changes such as hospital out of contracts
181 In terms of competitive forces the following was said:
Competitive forces and practical issues may make OOPs difficult for pathology and basic radiology
– Diagnostic providers will either charge OOPs or absorb the reduction in revenue.
– The challenges to OOPs are:
1. Diagnostic billing systems are mainly legacy and do not handle OOPs easily.
2. Bills are made up of many small items resulting in many small OOPs.
3. IFC will be very difficult in pathology and may rely on hospital and specialist assistance.
4. Competitive forces are strong in pathology and specialists can switch supply.
– OOPs in radiology are easier especially for CT and MRI.
– Providers are likely to absorb the fee reduction given margins are currently healthy and they need to preserve their volumes given pathology is a scale game.
(Original emphasis.)
182 In terms of the lapsing of members the following was said:
Analysis suggests that reasonable gaps do not drive lapse, especially if members are advised beforehand
– Member research and data analysis of claims has found that out of pockets for medical costs at reasonable levels does not significantly change members' likelihood to lapse
– If members were surprised by medical gaps then that did cause dissatisfaction, but the gaps themselves (up to approx $5,000) did not impact on intention to lapse or downgrade cover. Initiatives to remove the 'surprise' aspect of gaps should be investigated
– Not all overnight seps have path (69%) and rad (28%) services, furthermore not all services are contracted at >100%, so only 39% of seps will have Path and 10% will have a Rad experience that may attract out of pockets
– Even if low levels of lapse do materialise, the Ramsay analysis indicated that lapse of claiming members will result in a positive net financial outcome for Medibank
183 Again, there seems to have been reliance upon the Ramsay analysis without demur. Moreover, the advantages of removing any "surprise" do seem to have been appreciated.
184 Moreover, in terms of member impact the following was said:
– OOPs for overnight treatment is estimated to average $151 (Path), and $83 (Rad), OOPs for same day are even lower
– Even if the OOPs for overnight stays did drive a small amount of lapse, the lapse of claiming members is likely to be cash positive overall
– 114k members (170k separations) are assumed likely to be impacted by OOPs
– Average claims per member when diagnostics are involved are $7,692 ($4,963 per sep)
– If 10% of those members lapsed then 11k members would be lost
– This would result in $16.5M in lost revenue (ave premium $1500), and $85M in claims avoided
– The impact on sales and general lapse should also be considered
– If average GM2 is assumed to be $140 per member per annum, then 485,000 members would have to be lost before the benefit of net reduction in claims is wiped out – this is considered highly unlikely
– The conclusion therefore is that membership loss is not a significant financial risk in the evaluation of this initiative
185 This is significant in that it indicates the perception that membership loss was not a significant financial risk flowing from the initiative.
186 Further, in terms of project approach, it was made clear that the "Diagnostics Funding Review" (or what I have defined as the MFR, albeit at the time focused on diagnostic services) implementation, being the decision to terminate most MPPAs, would be run via the "Out of Contract" working group structure (OOC Working Group), headed by Anthony Goldman. This was to be done within the CCH division, not the PNIC.
187 In terms of the implementation time-table, the start date was 1 September 2014. The time-table only provided for written prior notice to diagnostic providers (other than Sonic) 60 days out. Sonic was to be "ring fenced" from the decision for 2 years. The Project Director was to be Jenny Patton.
188 As part of the OOC Working Group there were a number of work streams including "Member Comms & Marketing" and "Corporate Affairs and Internal Comms". In terms of activities and responsibilities, it was proposed that "Member Comms & Marketing", headed by Lauren Johnson, would:
– Develop member communications strategy
– Member of Communications Sub-committee to align comms and key messages
– Draft member comms
– Manage mailouts
– Manage social media channels and digital
– Support Corp Affairs on media strategy
189 Corporate Affairs was also to be involved. Indeed, it was suggested that a "Comms Working Group" would be part of Corporate Affairs.
190 Now a number of themes may be drawn together at this point that arise from the contemporaneous documents that I have discussed.
191 First, any communications strategy concerning the diagnostics funding decision had not been settled on. More particularly, there had been no decision made to engage in a non-communication strategy with members.
192 Second, it was appreciated that there may have been a net positive financial impact to Medibank flowing from the initiative. But it also seems to have been appreciated that such a financial benefit could be utilised to the advantage of its members.
193 Third, it was appreciated that there was a potential consequence following from the initiative of some members lapsing, particularly chronic sufferers.
194 Fourth, it was appreciated that there was a potential risk to the IPO flowing from the initiative and, potentially, any prior publicity.
195 Fifth, it was appreciated that a significant percentage of members had a poor understanding of OOPs with a consequent element of "surprise" when they were so informed thereof. It would seem that the advantages of prior notice to avoid such surprise were well appreciated.
196 Sixth, there was an inquiry being undertaken as to whether any "detrimental change to benefits" notification needed to be made to members.
197 Seventh, it would seem that the relevant member communications strategy was to be developed by the OOC Working Group in consultation with Corporate Affairs and the Steering Group, which was set up as I will discuss in a moment. This was to be done within the CCH division. This did not involve Dr Wilson. Let me return to the chronology.
198 In evidence before his Honour was a May 2014 presentation titled "Diagnostics – Member Communications approach". But there was no evidence as to its author or who it was sent to. It contained a "Project Risks" Table similar to the ExCo presentation in February 2014 with an additional risk 9 added.
199 It also contained a statement as follows:
High level quantification of potential member impact
– OOPs for overnight treatment is estimated to average $151 (pathology), and $83 (radiology), OOPs for same day are even lower
– Increased Lapse – Even if the OOPs for overnight stays did drive a small amount of lapse, the lapse of claiming members is likely to be cash positive overall
– 114k members (170k separations) are likely to be impacted by OOPs as a result of this change
– Average claims per member when diagnostics are involved are $7,692 ($4,963 per seperations) (sic)
– If 10% of those members lapsed then 11k members would be lost
– This would result in $16.5M in lost revenue (average premium $1500), and $85M in claims avoided
– Reduced Sales – if 3% (same figure as assumed in the Ramsay model) of the annual sales target was lost due to perceived diminution in the competitive product position then 5,500 memberships would be lost at a lifetime value of approximately $1,855 – total value $10M
– The conclusion therefore is that approx 16,500 memberships may be lost with a financial gain of $60M
200 Again, this seemed to rely on the Ramsay analysis and to confirm that any risk of lapsing could produce a net financial benefit.
201 Further, in evidence before his Honour was another presentation dated May 2014 expressly addressed to the CCH Leadership Team (CCH LT) titled "Diagnostics Funding Review – Implementation Proposal". This presentation contained similar slides to the April 2014 Implementation Proposal. It also contained a "High Level quantification" slide as set out in the preceding paragraph.
202 Let me at this stage deal with some internal considerations by Medibank in May 2014 concerning a communications strategy.
203 On or around 14 May 2014, Corporate Affairs put together a communications overview document which Ms Victoria Hanlon (Media Relations Manager, Corporate Affairs) circulated to Mr Goldman and Ms Patton via email. Apparently Corporate Affairs had some reservations about the project, how it would be received externally, and the risk this could present to Medibank's reputation. It set out the following:
Diagnostics funding review
Communications overview and recommendations
Reputation and timing risks
Corporate Affairs believes that the diagnostic funding review represents a reputation risk to Medibank.
It will be challenging to convey why we are conducting a review, in a way that confirms a clear rationale and value proposition for members and may be portrayed externally as Medibank removing benefits from our members. This is particularly concerning considering current increased scrutiny on Medibank.
Additionally, mid-year is our highest sales, call volume and customer interaction period and we have concerns about business capacity to deliver this project (in a way that is experienced positively by customers) during this period.
Recommendations before proceeding
1. Delay project timing – it is our recommendation that the timing of this project is delayed until mid-July to notify providers. This would reduce frontline demand during a peak period.
2. Analytics to define messaging – analytics work to help developing external positioning and key messaging. For example:
– Is it possible to demonstrate a growth in diagnostics costs combined with a growth in diagnostic usage? If so, this would strongly support our case for doing this, with regards to moderating escalating costs.
– Are there any differences in managing this for MPL and ahm?
– What is the external messaging and rationale for the change as per our strategy pillars of health cost leadership and customer centred healthcare?
3. Establishment of a steering group – to ensure due diligence and governance.
4. Obligations to communicate with members – clarification from Legal on what we will be required to communicate to members and timing of this.
Communications approach
At this stage Corporate Affairs would recommend a reactive communications approach initially, where only key internal and external stakeholders will be notified (see table on following page).
Communications and messaging will be prepared for other audiences in case the change receives publicity only.
The aim is to keep communications contained.
Corporate Affairs activities and deliverables
Corporate Affairs will develop the following:
– Integrated communications plan, incorporating:
1. Key messages (to be developed once detailed provider approach and discussion plan is provided by PNIC negotiations team)
2. Stakeholder engagement plan and briefing materials
3. Media approach, release and materials
4. Internal and frontline communications approach and materials
Stakeholder engagement
Stakeholders | Approach/activities | Who? | When? |
Board | ? TBC | ||
ExCo | ? Regular updates on activity, provider reaction, positioning and reputation risk | Steering Group | |
Large providers ? Sonic ? Epworth ? Primary Health Care ? Cabrini ? Healthscope ? St Vincent's ? St John of God ? The Sisters of Mary ? Imed Network (Tas) | ? Direct engagement through face to face meetings. ? Provide feedback of reaction and meeting outcomes to OOC working group to help tailor approach and messaging for other stakeholders. | PNIC | |
Dept of Finance Dept of Health | ? TBC – phone call and email heads up. | James Connors | Post provider engagement |
Associations, collages (sic), independents: ? Pathology Australia ? AMA ? Australian Institute of Radiology | ? TBC | ||
Smaller providers (nbr??) | ? Letter to terminate contract and outlining Medibank position | PNIC | |
Medibank customers Ahm customers | ? TBC | ||
Frontline employees – MPL and ahm | ? TBC – training might be required? ? Frontline comms and scripting | ||
Senior Executive team | ? TBC | ||
All employees | ? TBC | ||
Media | ? TBC – likely reactive approach only, but dependent on customer and provider comms and response. |
Key messages
– If we continue to pay benefits in line with the current trend, we believe it would impact premiums in the future and, as a result, the affordability of private health insurance.
– Medibank pathology benefits and radiology benefits paid in excess of MBS increased by 18.5% and 16.8% respectively in 2012 (to be supported with data on potential increase in service usage).
– The diagnostic review has been conducted as part of due diligence by Medibank, to moderate the growth curve of increasing diagnostic costs.
– We encourage members to discuss their options with their doctors, including establishing informed financial consent and using providers who participate in a gap cover scheme.
Considerations and questions
– When is PNIC meeting with Sonic?
– Is it possible to demonstrate a growth in diagnostics costs combined with a growth in diagnostic usage? If so, this would strongly support our case for doing this, with regards to moderating escalating costs.
– Are there any differences in managing this for MPL and ahm?
– What is the external messaging and rationale for the change as per our strategy pillars of health cost leadership and customer centred healthcare?
(Original emphasis.)
204 Now a number of points. First, the initial strategy recommended was a reactive strategy. Second, the stakeholder engagement table did not include members. Third, the strategy proposed was to keep communications contained. Fourth, it would seem that the question of communications to members was to be considered through the lens of Medibank's legal obligations to notify.
205 On 15 May 2014, Ms Lauren Johnson, communications manager sent an email to Mr Doug Osborn and Mr Chris Carroll stating:
The OOC working group are currently addressing the implementation of the removal of MPPA's for Diagnostics – pathology & radiology.
The short of it is our MPPAs are driving MPL's diagnostic benefits to increase dis-proportionately to Medicare and the rest of the PHI industry. Medibank currently pays $24.6m in benefits above the legislated minimum ($17.5m in pathology and $7.1m in radiology. Therefore a decision has been made to eliminate MPPAs and only pay diagnostic benefits at a maximum of 100% of the MBS.
What does this mean for our members? If they require pathology and/or radiology services during their hospital admission then they may have an out-of-pocket. This is not definite though because it's at the discretion of the specialist as to whether or not they will pass on the cost. If they do and based on modelling it's estimated the average cost would be approx $151 for pathology and $83 for radiology.
Based on this information and more that's included in the attached pack, I'm recommending the following member communications approach.
Medibank and ahm not to communicate this change to members. Rather we take an 'educational' approach around Informed Financial Consent, understanding your rights. This approach would see the engagement of the following channels; some type of collateral item, Retail, CCL and potential press, Social, Digital.
This recommendation still needs be tested with the Ombudsman and Legal and we'll also need advice on if we have any obligation to communicate this change to pre-booked members. In the meantime though I would appreciate it if you could please confirm you're happy with my recommended approach.
206 On or around 16 May 2014 it would seem that it was proposed by Mr Goldman that a steering committee be set up for the diagnostics initiative implementation currently being run by the OOC Working Group. I have previously defined this as the Steering Group. Mr Goldman wrote to Mr Cooke and others in the following terms:
We would like to invite you to be a member of the steering committee for the Diagnostics initiative implementation currently being run by the OOC Working Group.
The steering group would be chaired by Ross Cooke as the initiative sponsor, and would be responsible for approving major issues such as, key messages, media strategy, member comms approach, member support strategies, frontline capacity, legal risks and ultimately will sign off on business readiness.
The Steering Group will need to meet fortnightly, at least initially, and meetings would be no longer than 1 hour. The Steering Group for this initiative would probably continue until end September, but there is the possibility that this group becomes the fixed Steering Group for Out Of Contract readiness.
As the initiative is specifically concerned with implementation and readiness, the membership of the Steering Group is proposed to be as follows:
– Ross Cooke (Chair)
– Dan O'Brien
– Mei Ramsay
– Jason Gowie
– Chris Carroll
– David Rankin
– Jenny Patton (Project Director)
– Anthony Goldman (Project Manager)
207 Of this group, five had been involved with the PNIC (Mr Cooke, Mr O'Brien, Mr Rankin, Ms Patton and Mr Goldman) and two with CCH (Mr Gowie and Mr Carroll); Mei Ramsay apparently was not a part of either PNIC or CCH.
208 On 22 May 2014, Ms Johnson sent an email to Deepa Kandasamy seeking data that "we'll need to help with the approach for member communications", including chronic member data. Diagnostic data for the OOC Working Group was provided on 27 May 2014.
209 On 28 May 2014, Ms Johnson sent an email to Mr Osborn and Mr Carroll in the following terms:
A few members of the working group met yesterday and we're in agreement that there are potentially 2 groups of members:
1. General – no direct communication based on data and legal advice.
2. Special – we're still working on this cohort, but an example of the categories is below. The approach for this group is still to be decided. We are waiting for more data.
– Chronic
– ICU
– OOP threshold above
In addition, I will commence to update our Going to Hospital brochure and from this will be able to extract some content to create a DL flyer specific to OOP and diagnostics to make available to Frontline staff.
210 It would appear that by this time legal advice had been received suggesting that no direct communication with members was necessary, at least generally speaking. But it would appear that the need for communication with special groups (i.e. chronic) was still under consideration.
211 Let me turn to some of the contemporaneous documents for June 2014.
212 In the provider engagement brief prepared in June 2014 for the implementation of the diagnostics funding decision it was stated:
Our research found that seven in ten members had no discussions about medical out of pocket costs prior to their admission; and 35% of members were surprised at their medical out of pocket expenses. Of those who were surprised, just over half (53%) were informed by their medical specialist or surgeon of the possibility of experiencing an out of pocket expense.
213 On 4 June 2014, Mr Goldman sent an email to Mikala Hehir and Victoria Hanlon in the following terms:
Hi Guys, here is the full pack on the research done by think Global into the impact of medical gaps,
Also attached is a 1 pager from Rory [Atchison], which summarises these findings and the result of his analysis
214 The one page attachment from Mr Atchison was in the following terms:
Findings from 3 sources (2 member surveys, 1 Medibank claims data) suggests that, after taking into account a range of demographic, product and insurance related factors, medical OOPs are not a key driver of lapse or lapse intentions
– Member hospital experience survey 2010-12 data (n=52,056) showed likelihood of lapse only increased for members with medical OOPs > $5,000 and no impact of diagnostic OOPs.
– Lapse likelihood impacted by greater than expected medical OOPs, Hospital excess, Age
– A sample of Medibank 2012 claims data (n=77,842) showed no significant difference in lapse between memberships with no medical gaps and gaps of $2,000-$3,000.
– Tenure, product, age, product type, hospital excess and previous claims were better indicators of lapse propensity
– Recent analysis on small dataset from Think Global research showed satisfaction (n=) and positive intentions (n=) were not associated with medical OOPs or members being informed or surprised about gaps.
– Instead, satisfaction with the claims experience was the principal driver above any demographic or product related factors:
– Neutral or negative claims experience reduced satisfaction by 87% and 94% respectively and reduced positive intentions by 77% and 88% respectively.
– These are consistent with previous lapse analysis by PHI Customer Analytics on lapse propensity that highlighted drivers as residential location, product/cover, PHI most recent interaction, tenure, pre-paid payments, age, OMS registration and last contribution method without mentioning medical OOPs.
(Original emphasis.)
215 On 5 June 2014, a presentation was made to the Steering Group concerning the "Diagnostics Funding Review" (i.e. the MFR with its then focus on diagnostic services). It contained the following statement:
Member Communication Strategy to focus on supporting members with OOPs
– REDACTED
– Comms strategy to be centred around helping members understand OOPs, their rights to IFC and how to minimise OOPs
– Investigation under way into high users of diagnostics to try and identify group for direct communications ie chronic conditions
– Messaging will support the proposition of 'call us before you go to hospital'
– Marketing materials and support for frontline will include:
– Scripts/training for frontline – OOPs generally and diagnostics for members going to hospital
– Changes to the 'going to hospital guide'
– Stand-alone flyer on OOPs
– Website information
– PHIO engagement will occur during June / July
(My emphasis.)
216 The passages that I have emphasised set out the communications strategy that was contemplated. The only direct communication contemplated was with high users of diagnostics, such as chronic sufferers.
217 On 19 June 2014, there was a further presentation to a Steering Group meeting. The presentation set out a "Provider Engagement log". It also contained a risk register identifying risks with the proposal. Risks 16 and 17 were expressed in the following terms:
16. Negative impact on MPL reputation due to perception of reducing benefits
17. Negative impact on high sales period if notification and potential media occurs during June- July period
218 And in terms of communications strategy, the following summary was given:
Communications Strategy Summary
– Member –
– Focus on members who contact us prior to going to hospital
– Advise members on OOPs in general with specific mention of diagnostics
– Main message is explaining likelihood of OOPs, informing member about rights to Informed Fiancial (sic) Consent and advising they speak to Dr about options to avoid or minimise OOPs
– Have not found group of members to communicate directly with eg chronics with risk of high OOPs
– Web / Going to hospital guide and seperate (sic) OOP flyer will be produced
– Provider –
– Call or meeting with all impacted diagnostic providers
– Letter of notice to all impacted diagnostic providers
– Contract managers to discuss with Member's Choice hospitals – letter to support if required
– Proposed letter to specialists – refered (sic) 100+ services to diagnosic (sic) provider with MPPA above 100% – approx 3,000 to 4,000 letters
(My emphasis.)
219 It appears that by this time there had not been an identification of a particular cohort for direct communication. Clearly, Medibank considered the various options for notification, but decided against a direct communications approach to members generally or a cohort thereof.
220 Further, on 20 June 2014, Mr Osborn sent an email to Mr Goldman in the following terms:
The member communications strategy is now a passive one – ie that we'll await members who feel concerned/aggrieved to contact us – rather than requiring a proactive mail out. This falls into the realm of Change Management/Frontline. Do you need anything further from Marketing\Member Communications?
221 On 4 July 2014, there was a third meeting of the Steering Group. On 18 July 2014 there was a fourth meeting of the Steering Group. The presentation detailed a member engagement strategy in the following terms:
Member Engagement Strategy
– Meeting held on 17 July with Craig Harris, Michael Ehrentraut, Bec lee, AG
– Agreed the following:
– Avoid comms not targeted to members who are identified as going to hospital
– Promote members contacting us before hospital with POS in retail, Qtalk in CCL and Web
– Trawl recent interactions for key words ie hospital name to further identify members to contact
– Investigate ability of eligibility check to further identify members to contact
– Ensure frontline is well prepared to manage the 'going to hospital' discussion and to introduce out of pockets in a positive way
– Leverage retail org structure to ensure training and compliance
– Web based training
– Role play guides including scripting suggestions
– CCL and retail would create specialists to handle difficult interactions
– Update to the 'Going to Hospital' guide that is available on the website and is sent directly to any member advising us that they are going to hospital
– Specific flyer regarding out of pockets for display in retail stores and available on web
– A full audit and update of web and printed material
– General press advertising in mainstream publications to establish Medibank's change agenda and our focus on the delivery of quality, affordable healthcare
222 On 29 July 2014, Ms Johnson wrote to Mr Goldman and Ms Patton in the following terms:
Thanks for your feedback. I felt there really wasn't much on IFC in the Going to Hospital brochure to poach and from conversations around this piece took it that it was to focus on IFC. But in saying that I do believe the copy is addressing
– What you can do to understand and minimise gaps:
– Call MPL as soon as you think you may have to go to hospital
– Ask your providers what they will charge
– Ask your providers if there are no or lower gap alternatives
– What to do if you are charged a gap you weren't expecting
In regards to the other points these are covered off in my overall comments and have asked Kate to include a section on what kind of Out-of-pocket expenses member can expect. This can cover
– How are fees set (doctors free to set their own)
– MBS fees 75% / 25% (scheduled fees)
– Item numbers must be recognised by Medicare
But I can expand on this to include where are gaps likely to come from – list most common chargers of gaps (allows us to introduce diagnostic gaps).
Also I don't see how we can address Diagnostics any other way than in a roundabout way.
Jenny – are you OK with the direction of the copy I provided? Want to make sure we're all on the same page.
223 As at 30 August 2014, the communications strategy adopted appears to have been embodied in a document prepared earlier which recorded in part the following:
Diagnostics funding review – Communications strategy
Communications approach
To ensure appropriate stakeholders are briefed regarding the implications of Medibank's diagnostic funding review and that Medibank and ahm members are aware of options they can choose from to minimise out of pocket costs.
Communications with the larger diagnostics providers under an MPPA with Medibank have already commenced, with formal termination letters to be issued 27 June. Termination of the current MPPAs will take effect from 1 September 2014.
The approach to media will be reactive only, although we do expect media coverage to follow the mailing of specialist letters.
Background
In order to protect our members from unknown out-of-pocket costs, Medibank has in the past contracted with several large pathology and radiology companies to provide set fees and charges.
Unfortunately we did not foresee that these contracts have led to inflationary pricing.
Medibank has conducted a review of diagnostic services we pay for on behalf of our members, to help moderate increasing diagnostic costs and to keep healthcare affordable.
As a result, Medibank is no longer contracting with diagnostic service providers (termination of MPPAs) and will only be paying for diagnostic services on behalf of members at MBS scheduled fees.
Medibank currently has MPPAs with 44 diagnostics service providers and will commence termination on 1 July 2014 (providing 60 days notice), with MPPAs scheduled to be terminated 1 September 2014.
Stakeholder engagement activities
Stakeholders | Approach/activities | Who? | When? |
Board | ? Regular updates on activity, provider reaction, positioning and reputation risk. | George Savvides | TBC (prior to media activity) |
ExCo | ? Regular updates on activity, provider reaction, positioning and reputation risk | Steering Group | On-going |
Sonic | ? Direct engagement through face to face meeting. | PNIC | 15 May & 10 June |
Department of Finance and Department of Health | ? Phone call and email heads up outlining approach and risk mitigation | Dan O'Brien | w/c 10 June (post Sonic meeting) |
PHIO | ? Direct engagement through face to face meeting. | Jenny Patton | Post DoF feedback |
Key Govt stakeholders: ? Office of Minister for Health | ? Phone call and email heads up. | Dan O'Brien & James Connors | w/c 23 June |
Associations, colleges, independents: ? Pathology Australia ? Australian Institute of Radiology | ? Letter (sent via email as a PDF) outlining Medibank's position | James Connors | 16 June |
CAT team | ? Frontline comms and scripting – explaining the changes, why they are occurring and timeline | Mirjana Misfud | 16 June |
Large providers ? Mater Brisbane ? St John of God ? St Vincent's ? Uniting Health Care ? North Shore Private ? Epworth ? Cabrini Health Ltd ? Health Care Australia ? Healthscope ? Melbourne Health ? Primary Health Care ? IMED Network | ? Direct engagement through face to face meetings. ? Provide feedback of reaction and meeting outcomes to OOC working group to help tailor approach and messaging for other stakeholders. | PNIC | 16 – 27 June Allow time for follow up meetings depending on provider responses |
Smaller providers (27) | ? Phone communication | PNIC | 16 – 27 June |
AMA | ? Direct engagement through face to face meeting. | James Connors | w/c 23 June |
Frontline employees – MPL and ahm | ? TBC – training might be required? Potential for team huddles ? Frontline comms and scripting | TBC Victoria Hanlon | 21 July |
All employees | ? Message in George Savvides email to all employees. ? Intranet feature with link to white paper and media release | Melissa Barnes | 21 July |
Letters to all providers (43) (except Sonic) | ? Letter to all providers (except Sonic) following meetings/phone calls, reiterating our intention and the reasoning behind it. | PNIC | Letters to be issued 27 June, to be with providers by 1 July. |
Media | ? Reactive approach only – media statement prepared. | Victoria Hanlon | TBC |
Senior Executive team | ? Corporate Affairs Breaking News outlining media approach | Victoria Hanlon & Mikala Hehir | TBC |
Medibank customers ahm customers | ? Update to "Going to hospital brochure" ? Update to web content related to diagnostics and going to hospital | Lauren Johnson | TBC |
(My emphasis.)
224 It would also appear, consistently with this reactive strategy concerning members, that front line staff were being readied to deal with queries from members concerning OOPs and any change.
225 It would also appear that it was contemplated that some providers, for example, Cabrini Health, would contact Medibank's members directly concerning the change. Indeed they may have done so before 1 September 2014. Others did so after 1 September 2014; see for example the pro forma letter dated 2 September 2014 sent by Queensland Diagnostic Imaging to patients.
226 In terms of Medibank's experience of the initiative after 1 September 2014, Mr Goldman sent an email to Ms Johnson and others on 17 November 2014 in the following terms:
The Diagnostics initiative has been live since 1 Sep and while savings are flowing according to budget, the member experience has been characterised by high out of pockets by some providers, no Informed Financial Consent, and a letter accompanying the account that blames MPL.
We have been paying selective ex gratias up to now to manage member experience.
The objective of this meeting is to discuss how to improve the member experience and to assess the future of the ex gratia policy.
227 This was in part to deal with the response of providers.
228 On 20 July 2015 and in terms of member complaints after the event, Medibank responded to a query from the ACCC which sought information on complaints (the requested information is in italics):
Between 1 September 2014 and the date of this letter, details of all complaints, as well as copies of any written complaints, received by Medibank from members about changes to the coverage of diagnostic services, including:
(i) the name and contact details of the member;
(ii) the specific nature of the complaint; and
(iii) any steps taken to address those complaints.
Medibank is aware of receiving a total of 779 complaints related to out of pocket diagnostic expenses in the period from 1 September 2014 to 23 June 2015.
Not all of these complaints were necessarily specific to the changes to the coverage of diagnostic services under the MPPAs. As can be seen from the high level breakdown of complaint type below, some complaints appear to be general expressions of dissatisfaction with respect to diagnostic out-of-pocket expenses or that private health insurance does not cover all costs, including out-of-pocket expenses. In many cases, no specific reason for the complaint was captured, beyond the fact that it related to an out-of-pocket expense. Accordingly, Medibank cannot be certain in these cases that they were in fact complaints about the 'changes' to MPPA coverage, or if members were simply unhappy they had to incur out-of-pocket expenses.
Medibank is also aware that some diagnostic organisations and providers encouraged members to complain to Medibank about the coverage of diagnostic services, where the diagnostic organisations or providers elected to charge above the relevant MBS fee and therefore create an out-of-pocket expense for their patients under the new model. Medibank is unable to determine the proportion of total complaints that were attributable to that factor, however Medibank expects that it gave rise to a reasonable number of the complaints that specifically referenced the MPPA change.
Accordingly, Medibank has erred on the side of caution and provided complaints data which refers to any issue related to diagnostic out-of-pocket expenses, noting that this does not mean that all complaints related to the change in MPPA arrangements.
DIAGNOSTIC SERVICES OUT-OF-POCKET EXPENSES COMPLAINTS | |
Reason for complaint | Number |
No specific reason provided | 523 |
Member unhappy about MPPA changes | 170 |
Member unhappy about out-of-pocket expenses/wants gap paid | 32 |
Member not advised of change to out-of-pocket expenses/need to pay out-of-pocket expenses | 38 |
Member was told they were covered or there would be no out-of-pocket expenses | 5 |
Member previously had not incurred out-of-pocket expenses | 8 |
Member not happy with changed position to out-of-pocket expenses | 3 |
Total | 779 |
SOLUTION | |
Action | Number |
Ex gratia payment provided | 697 |
Other steps taken to resolve (including further attempts to contact member) | 46 |
Outcome unknown | 33 |
No resolution required | 3 |
Total | 779 |
As can be seen from the above table, the vast majority of member concerns were resolved by Medibank providing a one-off ex gratia payment, which effectively covered the cost of the out-of-pocket expense the subject of the complaint. In some cases, complaints were resolved through the provision of further information and confirmation of the position with respect to out-at-pocket expenses for diagnostic services. There were also a small number of instances in which a particular complaint required further investigation, or further information was needed from the member (e.g. the amount of the out-of-pocket expense) but Medibank was subsequently unable to contact the member, despite attempts to do so.
SOME LEGAL PRINCIPLES
229 At this point it is convenient to set out the salient legal principles including some workable propositions that I have distilled from the case law.
230 Section 21 of the ACL is in the following terms:
(1) A person must not, in trade or commerce, in connection with:
(a) the supply or possible supply of goods or services to a person; or
(b) the acquisition or possible acquisition of goods or services from a person;
engage in conduct that is, in all the circumstances, unconscionable.
…
(3) For the purpose of determining whether a person has contravened subsection (1):
(a) the court must not have regard to any circumstances that were not reasonably foreseeable at the time of the alleged contravention; and
…
(4) It is the intention of the Parliament that:
(a) this section is not limited by the unwritten law relating to unconscionable conduct; and
(b) this section is capable of applying to a system of conduct or pattern of behaviour, whether or not a particular individual is identified as having been disadvantaged by the conduct or behaviour; and
(c) in considering whether conduct to which a contract relates is unconscionable, a court's consideration of the contract may include consideration of:
(i) the terms of the contract; and
(ii) the manner in which and the extent to which the contract is carried out;
and is not limited to consideration of the circumstances relating to formation of the contract.
231 Section 22(1) relevantly provides:
(1) Without limiting the matters to which the court may have regard for the purpose of determining whether a person (the supplier) has contravened section 21 in connection with the supply or possible supply of goods or services to a person (the customer), the court may have regard to:
(a) the relative strengths of the bargaining positions of the supplier and the customer; and
(b) whether, as a result of conduct engaged in by the supplier, the customer was required to comply with conditions that were not reasonably necessary for the protection of the legitimate interests of the supplier; and
(c) whether the customer was able to understand any documents relating to the supply or possible supply of the goods or services; and
(d) whether any undue influence or pressure was exerted on, or any unfair tactics were used against, the customer or a person acting on behalf of the customer by the supplier or a person acting on behalf of the supplier in relation to the supply or possible supply of the goods or services; and
(e) the amount for which, and the circumstances under which, the customer could have acquired identical or equivalent goods or services from a person other than the supplier; and
(f) the extent to which the supplier's conduct towards the customer was consistent with the supplier's conduct in similar transactions between the supplier and other like customers; and
(g) the requirements of any applicable industry code; and
(h) the requirements of any other industry code, if the customer acted on the reasonable belief that the supplier would comply with that code; and
(i) the extent to which the supplier unreasonably failed to disclose to the customer:
(i) any intended conduct of the supplier that might affect the interests of the customer; and
(ii) any risks to the customer arising from the supplier's intended conduct (being risks that the supplier should have foreseen would not be apparent to the customer); and
(j) if there is a contract between the supplier and the customer for the supply of the goods or services:
(i) the extent to which the supplier was willing to negotiate the terms and conditions of the contract with the customer; and
(ii) the terms and conditions of the contract; and
(iii) the conduct of the supplier and the customer in complying with the terms and conditions of the contract; and
(iv) any conduct that the supplier or the customer engaged in, in connection with their commercial relationship, after they entered into the contract; and
(k) without limiting paragraph (j), whether the supplier has a contractual right to vary unilaterally a term or condition of a contract between the supplier and the customer for the supply of the goods or services; and
(l) the extent to which the supplier and the customer acted in good faith.
232 It is appropriate to make some observations concerning ss 21 and 22(1).
233 First, one is referring to a statutory standard rather than an equitable standard. The context of s 21 makes this clear; s 20 deals with unconscionable conduct within the meaning of the unwritten law. Further, both the lens "in all the circumstances" (s 21(1)) and the non-exhaustive list of matters to which the Court may have regard (s 22(1) in this case) indicate that neither the boundaries nor content of the equitable doctrine are defining or limiting features. Nevertheless, the statutory construct may include aspects of the equitable construct.
234 Second, the evaluation of the conduct in all the circumstances requires "close consideration of the facts" (Thorne v Kennedy (2017) 350 ALR 1 at [41], citing Kakavas v Crown Melbourne Ltd (2013) 250 CLR 392 at [14]). Now such an observation was made when applying the equitable doctrine, and is particularly apposite in that context when considering the parties' relationship, one party's relative special disadvantage vis-à-vis another, whether situational or constitutional, and the conduct said to constitute the unconscientious taking advantage thereof. Necessarily such matters are fact specific. But equally, if not more so, such close consideration of the facts is necessary in the context of s 21. And s 22 elaborates on the factual matters and circumstances that are to be considered. Clearly, forensic analysis rather than platitudinous philosophy is required to identify the boundaries and content of the relevant conduct in context, before one considers the secondary characterisation of unconscionability.
235 Further, to say that unconscionability is to be assessed in all the circumstances is to deny the legitimacy of an atomistic approach which takes each of the factors in s 22(1) or each of the factors identified by the ACCC in appeal ground 6 and considers them only separately. Now although for convenience I have initially looked at some factors of either type separately, nevertheless I have considered the whole episode so to speak. I will address this later.
236 Further, assessing whether conduct in all the circumstances is to be characterised as unconscionable involves an evaluative judgment. And the primary judge enjoyed some advantage over us in making such a judgment given that he was taken by the parties through the voluminous contemporary documents in more painstaking detail and over a considerably longer trial time. But on the question that I am dealing with concerning Medibank's communications strategy, his Honour had little additional advantage in terms of hearing the oral evidence and assessing witnesses' reliability, the key oral evidence in this case being that of Dr Wilson. I say that because Dr Wilson was not significantly cross-examined on the issues that I am currently addressing in relation to the communications strategy, the failure to communicate with members and the reasons for such a course. Indeed, he had little relevant first-hand knowledge or input into the decision-making process concerning the communications strategy. Moreover, in terms of a detailed analysis of the contemporaneous documents, his Honour did not descend into great detail in his reasons although he no doubt considered them in detail. For these reasons, I am not at any significant disadvantage relative to his Honour in undertaking a similar evaluative exercise including drawing proper inferences from the documents tendered. But error must be demonstrated before his Honour's evaluative judgment can be set aside, that is, error which entails a different evaluative judgment to be made. I would note that I am not here dealing with alleged error that is said to vitiate a discretionary judgment. Let me return to the substantive law.
237 Third, one cannot simply align the statutory concept of unconscionable with something not done in good conscience in the sense in which equity has so treated the matter. As I have said, it is clear from s 21 and the factors that may be taken into account under s 22(1) that one is dealing with a broader notion. But reference to intellectual ideas of customary morality and societal values are at too high a level of abstraction to be practically useful or the objective touchstone. Further, such general themes distract attention from the values that need to be considered, namely the values explicitly or implicitly enshrined in the text, context and purpose of the ACL and the statutory regime applying to health insurance. But in identifying and applying those values, and indeed in considering the relevant matters under s 22(1) applicable to the particular case, societal or community values may also be implicitly satisfied. For example, in considering conduct affecting a particular sub-group of the community, the application of each relevant matter under s 22(1) should take into account and may need to be tailored to the characteristics of that sub-group and the alleged contravener's interaction therewith, consistent implicitly with community standards. But if unconscionable conduct is found, it will not be because of some amorphous characterisation of it as being against community values. Rather, it will be so characterised as being against the statutory construct informed by the values that I have identified and which I will expand upon later.
238 Fourth, it has been said that "unconscionable" means something not done in good conscience; I need not linger on whether "unconscientious" is a more apt description. But let me say something on the question of "conscience". In the context of equity, Kakavas explained the matter by reference to the appellant's submissions in that case in the following terms (at [15] and [16]):
In advancing a claim based on the principle expounded by Mason J in Amadio, the appellant relies upon the standards of personal conduct compendiously described as the conscience of equity. According to Pomeroy's Treatise on Equity Jurisprudence:
"the 'conscience' which is an element of the equitable jurisdiction came to be regarded, and has so continued to the present day, as a metaphorical term, designating the common standard of civil right and expediency combined, based upon general principles and limited by established doctrines, to which the court appeals, and by which it tests the conduct and rights of suitors, – a juridical and not a personal conscience."
The conscience spoken of here is a construct of values and standards against which the conduct of "suitors" – not only defendants – is to be judged.
(My emphasis, citations omitted.)
239 That encapsulation of "conscience" closely correlates with the description given by the deliverer of the 2009 W.A. Lee Lecture in Equity. But in the present context dealing with the element of "conscience" in statutory unconscionability, the "construct of values and standards" is extended beyond the boundaries and content of what equity would normally embrace. The metaphorical term of "conscience" in the present context has an enhanced dimension. Moreover, it is not just a juridical conscience to use Pomeroy's description. It is a statutorily created or recognised conscience with its construct of values and standards informed by the explicit and implicit values enshrined in the text, context and purpose of the ACL and the statutory regulation of the health insurance industry. Further, once that is appreciated, the qualifying epithet "good" in the phrase "good conscience" is otiose. The relevant conduct is either against the statutory construct of conscience or it is not; the qualifier of "good" in opposition to "bad" may have made sense when dealing with a moralistic version of conscience that had that implicit duality, but the statutory construct does not so require. Now I accept that any description of values even within the statutory construct of conscience will have attendant imprecision in terms of their boundaries and content. But it would be an exaggeration to say that they are so indeterminate as to be little more than a pretext to facilitate condemning conduct that is disapproved of simply on moral grounds.
240 Fifth, in terms of any requirement to demonstrate "moral obloquy" or "a high level of moral obloquy", the use of such labels is a gloss on the statutory text. I adopt that part of Allsop CJ's analysis in Paciocco v Australia and New Zealand Banking Group Ltd (2015) 236 FCR 199 (Paciocco (FFC)) at [259] to [306] where he explained that the statutory language should not simply be restated by substituting words or a phrase that Parliament did not choose, that the choice of synonyms should be eschewed and that danger lurked in using non-statutory phraseology to capture the meaning of the statutory language. As he said at [262]:
The task involved is not the choice of synonyms; rather, it is to identify and apply the values and norms that Parliament must be taken to have considered relevant to the assessment of unconscionability: being the values and norms from the text and structure of the Act, and from the context of the provision. Parliament has given some guidance to its proper application (and to its meaning) by identifying in s 12CC certain non-exhaustive factors that may be taken into account by a court in deciding whether conduct was unconscionable. Given the value-laden character of the word, it is necessary to ascertain and organise the relevant values and norms by reference to which the meaning of the word is to be ascertained, and by reference to which the application of the section is to be undertaken (the two tasks being distinct). It must, however, be emphasised at the outset that the values and norms that are relevant are those that Parliament has considered, or must be taken to have considered, as relevant. The following discussion should be understood as dealing with those matters, and not with any values or norms disembodied from, or unconnected with, the choice made by Parliament.
241 What his Honour described as the nature of the task is precisely the point, albeit modified in the present context to the values or norms enshrined or implicit in the ACL and the statutory regulation of the health insurance industry. At most, the statutory concept of unconscionable may accommodate a flavour of moral obloquy, but it is to divert the relevant normative inquiry to specifically seek to identify its existence or to clothe the relevant conduct with such a conclusory label (see also at [304] and [305]). If the task as suggested by his Honour is undertaken, then such a label is unnecessary both to the process of evaluation of the relevant conduct and to its normative characterisation.
242 I also endorse Leeming JA's observations in Ipstar Australia Pty Ltd v APS Satellite Pty Ltd (2018) 356 ALR 440 at [275] to [278]:
Finally, Ipstar's written submissions (although not those made orally) maintained that "unconscionability requires a high level of moral obloquy". I have not found any assistance in asking whether Ipstar's conduct involved a "high level of moral obloquy", and I respectfully do not accept the submission, notwithstanding the use of that term by Spigelman CJ in Attorney-General (NSW) v World Best Holdings Ltd (2005) 63 NSWLR 557; 223 ALR 346; [2005] NSWCA261 (World Best) at [121]…
The passage in World Best in its context is as follows:
"Even if the concept of unconscionability in s 62B of the Retail Leases Act is not confined by equitable doctrine, as the decisions under s 51AC of the Trade Practices Act suggest, restraint in decision-making remains appropriate. Unconscionability is a concept which requires a high level of moral obloquy. If it were to be applied as if it were equivalent to what was 'fair' or 'just', it could transform commercial relationships in a manner which the Minister expressly stated was not the intention of the legislation. The principle of 'unconscionability' would not be a doctrine of occasional application, when the circumstances are highly unethical, it would be transformed into the first and easiest port of call when any dispute about a retail lease arises."
I do not think that Spigelman CJ was purporting to gloss the statute when his Honour referred to a "high level of moral obloquy". Rather he was concerned to emphasise that to find that conduct was not "fair" or "just" was insufficient, and that the doctrine was one of "occasional application, when the circumstances are highly unethical". The essence of each of the four sentences in the passage reproduced above is that the doctrine is unlikely to be available in ordinary cases. It is important not to read the second sentence reproduced above in isolation, or as if it were a statute.
…
Sackville AJA, with whose reasons McColl JA and I agreed, regarded invocation of the phrase "high level of moral obloquy" as unhelpful in PT Ltd v Spuds Surf Chatswood Ltd [2013] NSWCA 446 at [101]–[102]… "Moral" is a notoriously imprecise adjective: "someone under a moral obligation" was the example of conceptual uncertainty chosen in Re Baden's Deed Trusts (No 2) [1973] Ch 9 at 20. When combined with "obloquy", which is scarcely a word in common parlance, the imprecision is heightened. To insist on the presence of a "high level" of such an imprecise quality does not, in my respectful opinion, assist in the task of giving legal meaning to unconscionable in s 22 of the Australian Consumer Law. But even if the epithet were less imprecise, there would be no warrant to construe s 22 as being subject to some threshold requirement. Instead the statutory language falls to be applied in terms.
(My emphasis.)
243 Such observations are also in sympathy with Basten JA's disquietude in Canon Australia Pty Ltd v Patton (2007) 244 ALR 759 at [1] and [4]. Moreover, if I accept Leeming JA's perspective on Spigelman CJ's use of "high level of moral obloquy", it is open to me to also conclude that that is how Gageler J also appreciated Spigelman CJ's use and therefore how Gageler J himself was deploying the phrase in Paciocco v Australia and New Zealand Banking Group Ltd (2016) 258 CLR 52 (Paciocco (HC)) at [188]; Gageler J did not purport to use Spigelman CJ's phrase in a manner different to how Gageler J understood Spigelman CJ to be using it.
244 Sixth, as Allsop CJ explained in relation to cognate provisions of the Australian Securities and Investments Commission Act 2001 (Cth) (ASIC Act) (at [285] to [296]):
(a) fairness and equality are values and conceptions underpinning s 22(1)(a), (b), (d) to (f) and (i) to (k); more particularly, s 22(1)(a), (j)(i) and (k) recognise asymmetry of power;
(b) a lack of understanding or ignorance of a party is the conception underpinning s 22(1)(c);
(c) the risk and worth of the bargain are the conceptions underpinning s 22(1)(e) and (i); a broader and related although not explicit concept is the question of asymmetry of information; and
(d) good faith and fair dealing are values and conceptions underpinning s 22(1)(l).
245 And as to the concept of good faith, which resonates with honesty and fair dealing, it is convenient to set out parts of Allsop CJ's exposition at [288] to [290]:
The usual content of the obligation of good faith that can be extracted from cases … is an obligation to act honestly and with a fidelity to the bargain; an obligation not to act dishonestly and not to act to undermine the bargain entered or the substance of the contractual benefit bargained for; and an obligation to act reasonably and with fair dealing having regard to the interests of the parties (which will, inevitably, at times conflict) and to the provisions, aims and purposes of the contract, objectively ascertained.
None of these obligations requires the interests of a contracting party to be subordinated to those of the other. It is good faith or fair dealing between the parties by reference to the bargain and its terms that is called for, be they both commercial parties or business dealing with consumers. As Posner J said in Market Street Associates Ltd Partnership v Frey 941 F (2d) 588 (1991) the contractual notion of good faith varies in what is required for its satisfaction by reference to the nature of the contract. But the notion is rooted in the bargain and requires behaviour to support it, not undermine it, and not to take advantage of oversight, slips and the like in it….
The standard of fair dealing or reasonableness that is to be expected in any given case must recognise the nature of the contract or relationship, the different interests of the parties and the lack of necessity for parties to subordinate their own interests to those of the counterparty. That a normative standard is introduced by good faith is clear. It will, however, not call for the same acts from all contracting parties in all cases. The legal norm should not be confused with the factual question of its satisfaction. The contractual and factual context (including the nature of the contract or contextual relationship) is vital to understand what, in any case, is required to be done or not done to satisfy the normative standard.
246 Seventh and more generally, although honesty and fairness in dealing with consumers is relevant including acting without deception, it would be wrong to say that unfair conduct in and of itself amounts to unconscionable conduct. But establishing unfair conduct may be a step along the way to showing unconscionable conduct. It would also be wrong to say that because hardship is or may be caused to a consumer by conduct, such an actual or likely consequence in and of itself establishes that the conduct was unconscionable. But again, establishing actual or likely hardship may be a step along the way to showing unconscionable conduct, although it is not necessarily required.
247 Eighth, statutory unconscionability does not require only focusing on Medibank's or its officers' or employees' state of mind, whether actual intention or knowledge or what it ought to have known. It is a broader concept requiring an "objective value judgment on behaviour" (cf Yeoman's Row Management Ltd v Cobbe [2008] 4 All ER 713 at [92] per Lord Walker of Gestingthorpe). But the subjective state of mind of the alleged contravener whether actual or constructive is relevant to the broader sense. Although I am concerned with a normative notion of conscience, the boundaries and content of which are informed by the explicit and implicit values previously identified, Medibank's state of mind is relevant.
248 Ninth, industry practice is a relevant consideration. To the extent that this is formalised in an industry or other code, express recognition is given thereto in s 22(1)(g) and (h). But acting consistently or otherwise with industry practice has broader relevance to the unconscionability question as Keane J explained in Paciocco (HC) at [290]:
The appellants seek to stigmatise as unconscionable or unfair or unjust an activity in the marketplace in which nothing materially distinguishes the situation and conduct of either Mr Paciocco or ANZ from any of the other participants in that activity. It may be said that ANZ and its competitors have dealt "unconscionably" or "unfairly" or "unjustly" with all of their customers in that, in a careless or partisan use of language, all banks may be said to do so as a matter of course. But to argue that conduct by one participant in a market, which is an unremarkable example of conduct engaged in by all participants in that market, is unconscionable, or unjust or unfair, in breach of the statutory norms, without any suggestion that the market itself is unlawfully skewed, is something of a stretch…
249 Of course that was a different context, but it demonstrates that the standards, norms and practices of the relevant industry sector, in the present context the health insurance industry, are relevant to the assessment of statutory unconscionability albeit not confined thereby. But I should also stress that conduct consistent therewith does not necessarily entail that such conduct is not unconscionable.
250 Tenth, the boundaries and content of the relevant statutory regime applying to the health insurance industry is also important context within which to assess statutory unconscionability. I will elaborate on this in much more detail later.
251 Eleventh, it is not necessary to show that a person is under a disadvantage or that any particular person has been disadvantaged by conduct (s 21(4)(b)). But in any event, a person is not treated as being in a position of substantial disadvantage merely because there is an inequality of bargaining power. And in any event as Keane J said at [293] on the ultimate question:
While a disparity in bargaining power may be necessary to attract the operation of the provision, the mere existence of the disparity is not sufficient to do so. The existence of a disparity in bargaining power, which is an all-pervading feature of a capitalist economy, does not establish that the party which enjoys the superior power acts unconscionably by exercising it.
252 Twelfth, in terms of the technical operation of s 22(1), it is necessary to consider each of the non-exhaustive list of matters set out in s 22(1) if relevant. The word "may" in s 22(1) is conditional rather than permissive. If any matter in the list is potentially relevant to the conduct under consideration, it must be considered. As Gageler J expressed it in relation to cognate provisions of the ASIC Act (at [189]):
The word "may" in s 12CB(2) of the ASIC Act was not permissive, but conditional. The import of s 12CB(2) was to spell out that circumstances relevant to the determination of whether conduct was objectively to be characterised as "unconscionable" according to the ordinary meaning of that term might or might not include, in respect of particular conduct, all or any of the particular matters referred to in s 12CB(2). The provision made clear that, where any one or more of those matters existed in respect of particular conduct, each of those extant matters was to form part of the totality of the circumstances mandatorily to be taken into account for the purpose of determining the statutory question posed by s 12CB(1). The provision did not leave it open to a consumer who alleged that conduct of a supplier was in breach of s 12CB(1) to pick and choose. The customers could not choose to rely on matters referred to in s 12CB(2)(a) and (b), yet to ignore matters referred to in s 12CB(2)(c), (d) and (e).
253 Further, it is inappropriate to focus on one or more of the applicable matters listed in s 22(1) to the exclusion or unjustifiable expense of others.
254 Thirteenth and more generally, it is important to note that the conduct which attracts the operation of the statutory provision is assumed to be of sufficient seriousness such as to potentially warrant the imposition of a pecuniary penalty. That perspective is not irrelevant to the construction and application of ss 21 and 22(1).
255 Finally, I have considered the observations made in various Full Court authorities of this Court including Australian Competition and Consumer Commission v Lux Distributors Pty Ltd [2013] FCAFC 90 at [23], Paciocco (FFC) at [259] to [306], [371] and [398], Commonwealth Bank of Australia v Kojic (2016) 249 FCR 421 at [54] to [59], [69] and [85], Colin R Price & Associates Pty Ltd and Another v Four Oaks Pty Ltd (2017) 251 FCR 404 at [50] to [58], Kobelt v Australian Securities and Investments Commission (2018) 352 ALR 689 at [187] to [193] and [381] and Unique International College Pty Ltd v Australian Competition and Consumer Commission [2018] FCAFC 155 at [103] et seq. But none of them are inconsistent with what I have said. I have just separated out some structural elements from the meta-themes that permeate this space.
ANALYSIS OF APPEAL GROUNDs
256 Let me now deal with each appeal ground in detail. It is convenient to first discuss appeal grounds 7(a) and (b).
(a) Ground 7(a)
257 Paragraph 7(a) asserts that the primary judge erred in holding that the unconscionable conduct claim could not succeed unless the ACCC also proved misleading or deceptive conduct or at least the relevant representations. Now his Honour found that the failure of the ACCC's case on misleading conduct or at least the making of the relevant representations was fatal to its case on unconscionable conduct (at [253] and [254]). But nevertheless his Honour independently went on to consider the other circumstances relied on by the ACCC, and concluded that they did not lead to a finding that Medibank's non-disclosure strategy was unconscionable in all the circumstances (at [255] et seq.).
258 Let me linger for a moment on how the ACCC framed its case. It seems clear from the ACCC's concise statement, there being no formal pleadings, that a necessary foundation of its unconscionable conduct case was the making of the representations, which as is apparent have not been established either before the primary judge or before us. Indeed, the concise statement at [31] asserted:
Further, in the circumstances where Medibank:
(a) made the Diagnostic Cover Representations and the Notice Representations as described in paragraphs 15 and 16 respectively;
(b) was and is a signatory to the Industry Code;
(c) knew or expected the matters described in paragraph 18;
(d) knew or expected consumers were disadvantaged or vulnerable as described in paragraphs 23 and 24 respectively;
(e) had made the calculations as described in paragraph 20 and 21; and
(f) by November 2014 knew the matters described in paragraph 27,
by implementing the Benefit Change and the Non-disclosure Strategy, Medibank engaged in conduct that was in all the circumstances unconscionable, in contravention of s.21 of the ACL.
(My emphasis.)
259 Not only was the first circumstance mentioned in the ACCC's list the making of the representations, but [31] was formulated as a conjunction of circumstances (a) to (f). Now it is understandable why the ACCC relied upon the making of the representations as a foundation for the implementation of the non-disclosure strategy and its characterisation as unconscionable conduct, the implementation of the diagnostics funding decision itself not being pressed as unconscionable conduct. Unconscionable conduct concerning non-disclosure was much easier to establish if the context involved the prior representations having been made. But if the cover representation and the notice representation were not made, as concluded by the primary judge who has not been shown to be in error on this aspect, characterising the non-disclosure in all the circumstances, but without the representations, as unconscionable conduct becomes more problematic.
260 In my view this ground lacks substance. First, his Honour did not dispose of the matter on a pleading point as if the unconscionability case relied for its success on the establishment of the representations or indeed misleading or deceptive conduct, notwithstanding the form of the concise statement that had the former as a foundation. Second, his Honour dealt with the alternative scenario as a matter of substance. He addressed unconscionability on the alternative foundation that the representations had not been made or misleading or deceptive conduct had not occurred, but held that such an alternative case failed in any event.
(b) Ground 7(b)
261 Paragraph 7(b) asserts that his Honour erred in finding that the evidence of Dr Wilson was relevant to Medibank's state of mind when it adopted and implemented the communications strategy including its decision not to directly communicate to members the diagnostics funding decision. It is said that Dr Wilson had no involvement in the formulation and implementation of that strategy. A Jones v Dunkel related point has also been made by the ACCC which it is convenient to deal with under this ground of appeal.
262 Now Medibank contends that Dr Wilson was competent to express the opinions reproduced at [301] of his Honour's reasons given his senior position in Medibank and responsibility for the MFR. Dr Wilson led the PNIC division of Medibank responsible for the MFR in 2013 to 2014, which resulted in the termination of various MPPAs. It is said by Medibank that Dr Wilson had ultimate executive responsibility for the MFR as head of that division. Further, it is said that throughout his time at Medibank, Dr Wilson reported directly to the CEO and was a member of ExCo. Further, Medibank says that the facts referred to by Dr Wilson were established on the evidence, were not challenged on appeal and are dispositive of the ACCC's case. I will return to this aspect later when I discuss appeal grounds 6 and 7(c).
263 Now it would seem that the primary judge largely ruled against the ACCC's unconscionability case concerning the non-disclosure strategy based upon Dr Wilson's unchallenged evidence. So much seems apparent from his reasons at [301] and [302] where he said:
The principal – and, in my view, insuperable – difficulty with the applicant's case on unconscionability, is that it cannot survive in the face of Dr Wilson's unchallenged testimony about Medibank's approach to communications with its members about out-of-pocket expenses for diagnostic services following the decision to terminate the MPPAs, and its decision not to send a letter or communication of the type the applicant contends it ought to have sent. Dr Wilson's evidence in that respect was as follows:
… [t]he approach was to reinforce communications to members about OOPs in general with specific mention of diagnostics. I considered that that approach was consistent with information Medibank generally provided to members about the potential for OOPs in connection with hospital visits, through its Member Guide and other brochures. I considered that that approach to member communications was appropriate for a number of reasons.
First, Medibank's MPPAs with the providers of diagnostic service[s] … has never covered the whole market. Medibank has never had an MPPA with every single pathology and radiology provider. As a consequence, it was my understanding at the time that Medibank's policies did not promise members that they would not receive OOPs for those services, and many members would have received OOPs for those services.
Second, I believed that the expected additional OOPs arising from the diagnostic funding change were not likely to be material in relative terms to the OOPs that members already typically paid for hospital visits, where surgeons' fees, and anaesthetists' fees and various hospital charges are typically in the several hundreds, if not, thousands, of dollars.
Third, after it was decided not to terminate the Sonic and Epworth MPPAs (especially since Sonic was and remains one of the largest pathology providers), there was no universal "across-the-board" change being implemented by Medibank (i.e. we did not end up ending all our MPPA arrangements, and members could still access them if treated by a Sonic or Epworth site).
Ultimately, that evidence, which I unhesitatingly accept, demonstrates that the decision not to communicate with members (about which the applicant complains) was a decision made in the context of the exercise by the relevant committee of its business judgment. Some may agree with it, some may disagree with it, but, in my view, there was nothing remotely unconscionable about it.
264 I am inclined to agree with the ACCC that his Honour placed too much emphasis on Dr Wilson's evidence on this aspect, particularly in light of the answers he gave under cross-examination (T655 to 657 and 662). Despite the contents of his witness statement, under cross-examination Dr Wilson conceded that although he was a member of the PNIC division (indeed its head, and as well a member of ExCo) and had overall project responsibility for the implementation of the diagnostics funding decision, the communications strategy with members was a matter for the CCH division of which he was not a member. He had no direct role in the communications strategy decision, as the contemporaneous documentary record that I have laid out earlier demonstrates. Moreover, it would appear that the personnel responsible for the communications strategy did not report to him, and he in any event had no authority to overrule them. Moreover, it would appear that he expressed no view to them about member communications.
265 Now Medibank said that Dr Wilson could properly give evidence on the communications strategy. It pointed out that not only was Dr Wilson head of the PNIC and a member of ExCo, but five out of eight members of the Steering Group were also members of the PNIC. But I do not think that this detracts from the ACCC's point. He was not directly involved in the communications strategy or the reasons underlying it. He was not a member of the Steering Group. In my view, his assertions at best only had limited value and should have been given little weight. Indeed, his evidence as to his knowledge concerning the communications strategy was vague to say the least. For example, his written evidence was replete with statements such as "As I understood it", "I was not usually involved in those discussions", and "I was informed of the general communication approach".
266 I agree with the ACCC that Dr Wilson's personal views on the basis for the communications strategy had little if any probative value, and that his state of mind was not the relevant state of mind to attribute to Medibank, eschewing for the moment descriptions such as "directing mind and will" for the reasons I gave in Australian Securities and Investments Commission v Westpac Banking Corporation (No 2) (2018) 127 ACSR 110; [2018] FCA 751 at [1660]. If there was a mind or minds to be relevantly aggregated for the purposes of attribution, it was the person(s) identified earlier who were part of the Steering Group and involved in the communications strategy. Indeed, upon the concessions being made by Dr Wilson under cross-examination, the admissibility of some aspects of his evidence ought to have been revisited, although this was not done by the ACCC and therefore hardly the fault of his Honour. But on any view, his personal views should have counted for little against the documentary record and his lack of direct involvement in the communications strategy.
267 But to give diminished weight to Dr Wilson's personal opinions concerning the reasons for the communications strategy and to give greater weight to the contemporaneous record does not alter or demonstrate error in his Honour's conclusion (at [302]) that "the decision not to communicate with members (about which the applicant complains) was a decision made in the context of the exercise by the relevant committee of its business judgment". That conclusion is supported by the contemporaneous documents. Of course, it is a separate question as to whether that conclusion forecloses a finding of unconscionability. In my view, the fact that conduct is engaged in on the basis of a "business judgment" does not entail that it cannot be unconscionable conduct. To focus only on the perspective of the alleged contravener and to classify its conduct as based upon a "business judgement", as it may well have been, is too narrow a focus for the purposes of ss 21 and 22.
268 There is another point to be made. Relatedly to the question of the diminished significance of Dr Wilson's evidence concerning the reasons for the communications strategy, I agree with the ACCC that a Jones v Dunkel inference ought to have been drawn against Medibank in relation to its failure to call the relevant personnel still within the employ of Medibank at the time of trial who were involved in the decision making process concerning the communications strategy.
269 The ACCC's case was that the Ipsos and TH?NK research results were adopted by and formed part of the information taken into account in Medibank's deliberations, including as to the non-disclosure decision. Medibank disputed this.
270 Dr Wilson in his evidence sought to downplay the significance of those reports. But the various meeting presentations, some of which I have referred to earlier, demonstrate that such reports were considered and that there was no suggestion that they ought to have been sidelined.
271 Further, and as I say, Dr Wilson was not able to give evidence about the deliberations of the CCH-based team who handled the actual member communications strategy. In those circumstances, Medibank's unexplained failure to call any of the persons who had been involved in that implementation work should have enabled the primary judge more readily to draw the inferences suggested by the documentary record that:
(a) the Ipsos, TH?NK and like research reports did form part of the information taken into consideration by Medibank when it was making its decision as to member communications;
(b) Medibank drew relevant conclusions reported in the TH?NK report or the Sibbick memo;
(c) Medibank recognised the limited reliability of IFC and that mere reliance on IFC procedures was likely to result in a proportion of members encountering "surprise" at a hospital or when they received bills after a hospital treatment; and
(d) the "Ramsay/114" type cost-benefit calculation was part of the background as to why Medibank determined not to initiate general notice to members, by letters and by up-front statements in its main telephone and website marketing.
272 But where I think the ACCC's analysis is too ambitious is that it cannot reasonably be inferred from the contemporaneous documents that the Steering Group adopted in a wholesale way each and every statement in the Ipsos and TH?NK surveys and that the "Ramsay" type analysis was a principal motivating reason why the Steering Group decided not to issue a general notice to members.
273 In my view, no compelling inference arises from the documentary evidence that those matters principally influenced any decision of the Steering Group.
274 But even if such inferences were open, I am not satisfied that unconscionable conduct would in an event have been established. Harsh the conduct may have been. Unfair the conduct may have been. But that is not sufficient to establish statutory unconscionability. I will elaborate on this in a moment when I discuss grounds 6 and 7(c). In summary, I am satisfied that ground 7(b) has been made out. But for reasons that I will explain, that does not justify a different conclusion on the ultimate question, which was that statutory unconscionability had not been made out.
(c) Grounds 6 and 7(c)
275 It is convenient to deal with these grounds together as the parties have done before us.
276 By ground 6, the ACCC contends that the primary judge erred in failing to find that Medibank engaged in unconscionable conduct having regard to the matters stated in paragraphs 6(a) to (l) of this ground. As I will explain, this ground has not been made out.
277 By ground 7(c), the ACCC contends that the primary judge erred in failing to adequately consider the evidence as to the formulation and implementation of the non-disclosure strategy, or what I have described as the communications strategy. The ACCC principally makes this point by reference to the succinctness of his Honour's reasons concerning the communications strategy, including at [301] and [302] which I have just discussed. But even if I agreed with the ACCC that the primary judge may not have fully considered the evidence on the communications strategy, this does not avail the ACCC. A consideration of the material to which our attention was drawn and which I have analysed earlier does not lead to a different conclusion to that reached by the primary judge.
Contextual matters
278 Before proceeding further, it is appropriate to set out various matters, which are supported by findings of the primary judge that have not been challenged before us, relating to context relevant to a consideration of the unconscionable conduct claim.
279 First, the benefits payable to Medibank's members were defined by its Fund Rules, which provided for the benefits required by the PHIA and the Private Health Insurance (Benefits Requirements) Rules 2011 (Cth). The Fund Rules also defined additional benefits that became payable to a member if Medibank had an arrangement or agreement in place with a private hospital or medical practitioner and the member received hospital treatment from that hospital or practitioner. Now under the Fund Rules there were three main categories of agreements or arrangements which Medibank could enter into which provided for additional benefits to be paid to members above the amounts prescribed by the PHIA and under the said subordinate instrument: the MPPAs, Hospital Purchaser Provider Agreements (HPPAs) and GapCover arrangements.
280 Second, prior to the diagnostics funding decision, Medibank was not a party to an MPPA with every provider of in-hospital diagnostic services. Only about 25% of radiology services and 60% of pathology services for which Medibank paid benefits to members were paid under an MPPA. And even after the diagnostics funding decision was made, Medibank remained a party to a number of MPPAs. And at the time of trial, Medibank still had in place MPPAs with two major providers, being Sonic and Epworth. Prior to the diagnostics funding decision, such MPPAs represented approximately 45% of the additional benefits that Medibank paid for pathology services, that is, benefits above 25% of the MBS fee.
281 Third, consumers including Medibank members were generally unaware of the existence or terms of the MPPAs.
282 Fourth, Medibank informed prospective and current members through its printed and website product information that:
(a) the benefit payable by Medibank for medical services was an amount up to 25% of the MBS fee for the service;
(b) doctors may charge an amount above the MBS fee, however, Medibank only provided benefits above the MBS fee if Medibank had an arrangement with the relevant doctor to pay an additional amount or the doctor participated in GapCover;
(c) GapCover did not apply to diagnostic services; and
(d) after Medibank paid benefits, the member was responsible for paying any amounts remaining on the hospital and medical accounts.
283 Fifth, and importantly, whilst Medibank's decision in the MFR relating to diagnostic services was to terminate or let lapse various MPPAs, that did not alter Medibank's member benefits in terms of entitlements such as his Honour found. Additional benefits for diagnostic services flowing from any MPPA were only ever conditional on Medibank entering into an MPPA with a provider. It had no obligation to do so. And it had no obligation to maintain or rollover any MPPA once entered into. Moreover, Medibank never publicised the existence or extent of MPPAs to members. And Medibank members had no legitimate expectation as to the entry into, maintenance of, or rollover of any MPPA.
284 Sixth, any cost savings to Medibank from the diagnostics funding decision did not in substance over the medium to long-term augment Medibank's profit to its own personal account due to the regulation of PHI premiums, but only allowed Medibank to fund other benefits for members or reduce premium increases. Dr Wilson explained this in the following terms:
The benefits Medibank provides to its members are funded through the premiums paid by members. Like all health insurers, any changes to Medibank's premiums have to be approved by the Federal Minister for Health under the Private Health Insurance Act 2007. To obtain approval, Medibank has to provide detailed financial information, together with cost and benefits projections that justify the proposed changes (this is usually done as part of an annual "rate rise" process). I understand that these submissions are closely scrutinised by the Department of Health and the Australian Prudential Regulation Authority. To obtain approval for a premium increase, Medibank must demonstrate that the increase is needed for Medibank to be able to continue to pay benefits to our members under their policies while sustaining a strong financial risk profile (requiring an appropriate profit margin and sufficient financial reserves for capital adequacy purposes). While the rate rise approval process assumes that Medibank will make a profit margin (within an acceptable range) in order to remain financially viable, margin growth is constrained through the rate rise process. Accordingly, any cost savings that Medibank makes in one area (unless they are spent on other initiatives) would effectively reduce the allowable premium increases due to health cost inflation, rather than being permanently retained by Medibank.
(My emphasis.)
285 Seventh, as his Honour also found, the vast majority of diagnostic services were provided on an outpatient basis, which were not within the ambit of PHI.
286 None of these matters have been significantly challenged before us. And to these matters may be added the following.
287 Eighth, Medibank's diagnostics funding decision was necessarily public, and was not intended to be kept nor was kept secret. Medibank had to inform diagnostic service providers and Medibank anticipated that they would publicly criticise Medibank. Such providers publicly did so. Medibank also informed numerous stakeholders including the Department of Health, the relevant specialist colleges for pathology and radiology and the PHIO.
288 Ninth, Medibank modelled the additional OOPs that may be incurred by members flowing from the decision and concluded that the additional amounts were modest and well within the range of medical OOPs which members regarded as reasonable, which his Honour so found (at [273] and [276]). No error has been demonstrated in such a finding. And as Medibank has pointed out before us, Dr Wilson gave evidence that he also considered that the additional OOPs that might be experienced by members were not material relative to OOPs that members already paid as a consequence of hospital visits, where surgeons' and anaesthetists' fees and various hospital charges were typically in the hundreds, if not thousands, of dollars.
289 Tenth, it is apparent from the contemporaneous documents that I have reviewed earlier that Medibank concluded that a general notice to all members was not warranted. But Medibank also analysed whether there were particular cohorts of members who might be unusually affected by the diagnostics funding decision such as members with chronic conditions. But as his Honour found, Medibank decided that with the benefit of detailed modelling, there was not such a cohort. Moreover, even for claiming members with chronic conditions, Medibank's modelling suggested that the average increase in OOPs would be modest, and in the order of $100; this encompassed an average increase of $40 for radiology, being the difference between $33 and $73 shown in tables produced in evidence, and $60 for pathology, being the difference between $13 and $73 shown in those tables.
290 Eleventh, Medibank enhanced its member communications for members with a forthcoming hospital admission, as his Honour found. Medibank also reinforced its member communications about IFC and patients' understanding of it, including updating its "Going to Hospital" brochure, completing a new IFC brochure, and insisting on IFC as a condition of allowing diagnostic providers to continue to use its billing channel.
Survey responses
291 Now the ACCC relied on various Medibank documents recording survey responses about, inter-alia, member understanding and acceptance of medical OOPs which it says were adopted by Medibank. The ACCC focused on the Ipsos Report, the Atchison Report and the Sibbick memo. I have referred to these survey responses in an earlier part of my reasons.
292 Medibank says that the ACCC's contentions that certain survey results recorded in the documents were adopted by Medibank is not supported by the evidence and was correctly rejected by the primary judge (at [289] to [295]). Now I am not convinced by his Honour's analysis on this aspect. It seems to me that aspects of these survey responses were considered by CCH personnel concerned with the communications strategy.
293 But I would say that even if these survey results were in some sense adopted by Medibank, at least in part, I do not think that this avails the ACCC. The following propositions may be accepted.
294 First, it was appreciated that there may have been a net positive financial impact to Medibank flowing from the initiative. But it also seems to have been appreciated that such a financial benefit could be utilised and ultimately had to be used to the advantage of its members.
295 Second, it was appreciated that there was a potential consequence following from the initiative of some members lapsing, particularly chronic sufferers.
296 Third, it was appreciated that there was a potential risk to the IPO flowing from the initiative and, potentially, any prior publicity.
297 Fourth, it was appreciated that a significant percentage of members had a poor understanding of OOPs with a consequent element of "surprise" when they were so informed thereof. It would seem that the advantages of prior notice to avoid such surprise were well appreciated.
298 Fifth, there was an inquiry being undertaken as to whether any "detrimental change to benefits" notification needed to be made to members in terms of Medibank's legal obligations.
299 But all of this does not assist to demonstrate unconscionable conduct as I will discuss later.
Ramsay analysis
300 Medibank also says that the ACCC's reliance at trial on the so-called Ramsay analysis was rightly rejected by the primary judge (at [296] to [300]). The analysis was referred to in the course of Medibank's assessment whether to proceed with the diagnostics funding decision. But it is said that it formed no part of Medibank's decision concerning member notification. It is said that the Ramsay analysis was undertaken in anticipation of the possibility that the Ramsay hospital group would not renew its HPPA with Medibank. The Ramsay analysis expressed a conclusion that Medibank might gain financially from such an event. Medibank says the analysis was a subsidiary point to the primary conclusion reached by Medibank that members accepted reasonable medical OOPs.
301 Further, Medibank points to the fact that Dr Wilson was questioned about the analysis and gave evidence that it did not feature in the decision making about diagnostic funding and that he believed the analysis to be flawed because it did not take into account the lifetime value of premiums paid by the member.
302 But even accepting the ACCC's position concerning the Ramsay analysis including the Ramsay/114 analysis in the sense that I can infer that it was taken into account in part by the relevant decision-makers responsible for the communications strategy, I do not think that this ultimately makes out the ACCC's case concerning statutory unconscionability in all the circumstances as I will explain later.
The elements of ground 6
303 I agree with Medibank that the ACCC's formulation of appeal ground 6 ignores relevant circumstances bearing on the question of unconscionability, which I have summarised above. But for the moment let me deal with each of the ACCC's elements specified in ground 6 in turn.
304 First, paragraph 6(a) asserts that Medibank knew that many members with Medibank hospital insurance or ahm hospital insurance were of the erroneous belief that they would not incur any OOPs during a hospital admission. Now it seems clear that Medibank was aware that some members did not have a good understanding about their potential exposure to OOPs. But that was not peculiar to diagnostic services. Moreover, given the extent of Medibank's general communications about its products, notification of the diagnostics funding decision was no answer to that concern.
305 Second, paragraph 6(b) asserts that Medibank made the representations, which were false, misleading or deceptive. But the primary judge found that Medibank did not make the alleged representations, and this finding has not been successfully challenged on appeal.
306 Third, paragraph 6(c) asserts that Medibank knew that a significant proportion of its members made no enquiries about OOPs prior to admission to hospital. Now Dr Wilson gave evidence before the primary judge that there is commonly a discrepancy between a patient's recollection of financial information provided and what treating doctors say about the provision of financial information to patients. Moreover, Dr Wilson did not agree that ordinary patients tend not to be very good at making enquiries about OOPs prior to admission. Nevertheless, I am prepared to accept the ACCC's assertion for present purposes. But in all the circumstances this does not take the ACCC that far in establishing unconscionable conduct.
307 Fourth, paragraph 6(d) asserts that prior to the diagnostics funding decision many members did not incur OOPs for in-hospital diagnostic services. Now this too may be accepted as far as it goes. But it is also to be noted that prior to the change, members did not incur an OOP for diagnostic services if either Medibank did not have an MPPA with the provider and the provider charged less than the MBS fee or Medibank had an MPPA with the provider. Generally, members were unaware of the existence of the MPPAs. Further, prior to the change many members in fact incurred OOPs for diagnostic services. In 2013, 42.9% of members receiving an in-hospital radiology service (45,085 out of 104,984) incurred an OOP and 7.6% of members receiving an in-hospital pathology service (20,289 out of 265,442) incurred an OOP.
308 Fifth, paragraphs 6(e), (f), (g) and (h) assert various matters. It is said that Medibank knew or had reason to suspect that if upon making the diagnostics funding decision it informed its members that they might be required to pay OOPs for in-hospital diagnostic services, a not insignificant number of them would have ceased to be members of Medibank's hospital fund thereby reducing its financial benefit from the diagnostics funding decision (paragraph 6(e)). But this overstates the evidence. Further, it is said that Medibank expected that the average OOP to members following implementation of the diagnostics funding decision would be $151 for each pathology service and $83 for each radiology service (paragraph 6(f)). But this overstates the evidence. Further, it is said that Medibank knew or had reason to suspect that such expenses would be a distressing burden to meet for many members, particularly for members suffering from chronic diseases and particularly where they were surprised by the expense (paragraph 6(g)). But this also overstates the evidence. Further, it is said that Medibank knew that if members were made aware of the possibility that as an in-patient they may incur OOPs for in-hospital diagnostic services, a not insignificant number of them would have sought to make arrangements to avoid or reduce that expense (paragraph 6(h)). But again this overstates the evidence. Let me make a few observations relating to these points.
309 Medibank considered the likely reaction of diagnostic providers to the termination of MPPAs and formed the view that they might not charge OOPs. But it considered that if they did so charge, the amounts were unlikely to exceed $151 for pathology and $83 for radiology. Further, on the data available, Medibank concluded that members were unlikely to be unduly concerned about OOPs at the levels being contemplated. Dr Wilson gave evidence to this effect. Dr Wilson also gave evidence that he believed that following the change, many diagnostic providers might not charge OOPs. His view was based on the foundation, which has not been successfully impugned by the ACCC, that many uncontracted diagnostic providers did not charge OOPs to Medibank members and many diagnostic providers bulk-billed in an out-patient setting. Further, on the evidence before his Honour, members with chronic illnesses were not in a materially different position from other members. Data on members with chronic conditions indicated that members suffering from chronic conditions could experience a modest increase in OOPs; on average there would be an expected increase of $40 per annum for radiology OOPs and $60 per annum for pathology OOPs, the calculation of which I have explained earlier.
310 Now the ACCC contends, which I also accept, that Medibank expected some surprise and pushback from its membership. For example, in evidence was an email dated 22 August 2014 from Mr Goldman to Mirjana Panova and others stating:
As discussed in yesterday's meeting diagnostic providers are going to do their best to get OOPs going, and will attempt to direct members to call us etc. Anchal's note is another timely reminder.
At the moment our member / frontline support is focussed on training to ensure that our staff can explain the reasons why we have made the change and to suggest the member talk to their doctor about ways to avoid or minimise gaps.
In addition to this we will have the flyer in retail and available to CCL on gaps and IFC, the going to hospital guide will also have the message regarding how to understand and minimise gaps.
Also as discussed yesterday we will consider how to handle claims of misinformation and possibly more liberal ex gratia rules in the early days.
My question to you is – what else could we / should we do to support our frontline??
– Should we set up a war room / hotline for staff to call and get help with challenging member situations
– What happens if a member calls from the hospital when they are confronted with the OOP
– Do you think we have adequately prepared our staff in terms of the training or is there more we could do
Craig you will need to make the final call on could we / should we do more, but I am looking to all of you to send around your ideas and thoughts.
311 So, it was anticipated that frontline staff might need a "war room / hotline" for dealing with challenging member situations. But I am not sure where this takes the ACCC. Members' surprise does not carry the day.
312 The ACCC also contends that Medibank avoided disclosure to protect its reputation. And I must say that there is some support for this in the relevant documentation. But it is not as if the decision to terminate the MPPAs was kept or could be kept secret. I do not think that this reputational argument carries the ACCC far.
313 Further, the ACCC submitted, which can be accepted, that the decision to terminate the MPPAs impacted on a significant proportion of claiming members. Whereas before the decision a large percentage of claiming members with diagnostic services (or pathology services) encountered nil OOPs, after the decision only a small percentage of such claiming members encountered nil OOPs. But, of course, that does not say anything about the absolute levels (or the average thereof) of the additional OOPs that claiming members would have to pay after the decision that they were not paying previously. I have dealt with that question elsewhere.
314 Further, the ACCC strongly emphasised the fact that chronic sufferers were a more vulnerable class of members. Now I accept that there was such a sub-class. The difference in average medical OOPs per claiming member was likely to have had a bigger impact on chronic sufferers; indeed for a sub-sub-class such as chronic sufferers of kidney disease there may have been even bigger impacts. Further, many chronic sufferers may have been pensioners. Further, the chronic sufferers may have experienced more surprise or distress by the impacts of the relevant decision. I will return to this question later.
315 Sixth, paragraph 6(i) asserts that the Industry Code required or reflected a norm of conduct requiring Medibank to give prior notice of a change to benefits such as the diagnostics funding decision. But the Industry Code did not establish a norm of conduct requiring notification of the termination of the MPPAs. Now in terms of the Industry Code relevant to the present exercise and to which Medibank was a signatory, I am here dealing with the Private Health Insurance Code of Conduct (version 5, July 2014). The Voluntary Code of Practice for Hospital Purchaser / Provider Negotiations between Private Hospitals and Private Health Insurers appears to have lapsed in December 2002 according to a bulletin circulated to members of the Australian Private Hospitals Association on 2 September 2009; I would note that clause 16.1 was not otherwise unhelpful to the ACCC's case in one sense, albeit that it concerned HPPAs. In terms of the Industry Code, the following provisions may be noted.
316 Clause 2 provided:
2. OUR COMMITMENT UNDER THE CODE
As a signatory under the Code, as a private health insurer, we will:
(a) continuously work towards improving the standards of practice and service in the private health insurance industry;
(b) provide information to consumers in plain language;
(c) promote better informed decisions about our private health insurance products and services:
(i) by ensuring that our Policy documentation is full and complete;
(ii) when asked by a consumer, by providing an effective verbal explanation of the contents of the Policy documentation;
(iii) by ensuring that our staff and other persons providing information on our behalf are appropriately trained;
(d) provide information to consumers on their rights and obligations under their relationship with their Private Health Insurer, including information on this Code;
(e) provide consumers with easy access to our internal dispute resolution procedures, which will be undertaken in a fair and reasonable manner; and
(f) where internal dispute resolution procedures do not reach a satisfactory outcome for the consumer, or if a consumer wishes to deal directly with an external body, advise the consumer of the right to take the issue to an external body, such as the PHIO;
but apart from the provisions for enforcement and sanctions in the Private Health Insurance Codes of Practice, a breach of the Code shall not give rise to any legal right or liability.
317 Clause 3 provided:
3. PRIVATE HEALTH INSURANCE ENVIRONMENT
In meeting our commitments, we will have regard to:
(a) the provisions of the Private Health Insurance Act 2007 which govern private health insurance policies and arrangements between consumers, Private Health Insurers and government, including the requirement to meet prudential standards;
(b) our requirement to comply with the provisions of the Competition and Consumer Act 2010;
(c) the need for effective competition and cost efficiency being promoted in the private health insurance industry, and the need for ensuring flexibility in the development and enhancement of products and services for consumers.
318 Part E of the Industry Code dealt with policy documentation. Clause 1(g) of Part E said that Medibank would "provide in a timely manner to consumers information on any changes to their policy, being made in plain language and in a format aimed to assist comprehension by consumers".
319 Clauses 2.1 and 2.2 of Part E provided as follows:
2. DETRIMENTAL CHANGES TO POLICIES
2.1 DETRIMENTAL CHANGES TO HOSPITAL POLICY BENEFITS
A significant detrimental change to hospital policy benefits includes:
(a) removal of material benefits or restriction to default benefits for any identified condition;
(b) addition of material excesses/co-payments; or
(c) increases in excesses/co-payments greater than 50%.
Where there is a detrimental change to hospital benefits we will:
(a) for significant detrimental changes provide the affected consumer with details of the change giving at least 60 days' written notice;
(b) for all other detrimental changes provide the affected consumer with details of the change giving at least 30 days' written notice; and
(c) not apply the changes to pre-booked admissions; and
(d) put in place transitional measures for patients in a course of treatment for a reasonable time period, for example, up to six months.
2.2 SIGNIFICANT DETRIMENTAL CHANGES TO ANCILLARY BENEFITS
A significant detrimental change to ancillary policy benefits includes:
(a) introduction of a new limit or sub-limit; or
(b) a greater than 50% reduction in any limit.
For significant detrimental changes to ancillary benefits we will:
(a) provide the affected consumer with at least 30 days' written notice; and
(b) put in place transitional measures for rollover type benefits accumulated in a previous year.
320 Now it was accepted before us that a termination of an MPPA was not, strictly, such a detrimental change to hospital policy benefits. Indeed, this is in some respects confirmed by clause 3 which stated:
3. CHANGES TO HOSPITAL CONTRACTING ARRANGEMENTS
We recognise that while not constituting a change to hospital benefits for the purpose of Section 2 above, changes to hospital contracting arrangements between a fund and a hospital can affect a consumer. We understand that requirements for notification of consumers of such changes and transition arrangements are included in the relevant agreements and the Code of Conduct for Health Fund and Hospital Negotiations. We acknowledge that additional guidance can be found in DoHA circulars and in PHIO's Transition and Communication Protocols.
(My emphasis.)
321 Moreover, clause 3 was only dealing with HPPAs and not MPPAs in any event; further, query the obsolete reference therein to the other code.
322 Generally speaking, what is apparent is that there was nothing in the Industry Code that explicitly required prior disclosure of the termination of the MPPAs. Now clause 2.1 of Part E established industry agreed timeframes to the statutory obligations, which I will come to in a moment, to give "reasonable notice". But each of the matters referred to in clause 2.1 involved a change to the Fund Rules, which is not what occurred in the present case.
323 In addition to the Industry Code, it is necessary that I say something at this point about the membership guides, the Fund Rules and also the relevant legislation.
324 The Medibank membership guide and the ahm membership guide, albeit differently expressed, referred to members being subject to the relevant Fund Rules. And each guide stated that if Fund Rules were changed from time to time in a way that had a detrimental effect on members' entitlements to benefits, then prior reasonable written notice would be given. But, of course, the termination of MPPAs did not constitute any change to Fund Rules. Now the ahm guide language was broader in including changes to "policies and benefits". But this does not assist the ACCC's case because the termination of MPPAs were not properly so described. And as for the Fund Rules, using Medibank's to exemplify the point, these were never modified by the termination of the MPPAs as I have said. Moreover, to the extent that clause E2.11 encompassed any MPPAs as distinct from HPPAs, it only provided that any amendment thereto during the period of the agreement could not increase any OOPs payable by members. It was silent on termination or the effect thereof. I should set out clauses E2.1 and E2.11 to make good these points.
325 Clause E2.1 provided:
E2.1 Hospital Benefits Payable According to the Schedules
The Benefits payable in respect of Hospital Treatment and the conditions relevant to those Benefits are set out in the Fund Rules and associated Schedules.
(Original emphasis.)
326 But there was no change to the "Benefits" as defined.
327 Further, clause E2.11 was in the following terms:
E2.11 Agreements with Doctors and Hospitals
(1) Subject to these Fund Rules, the Fund may enter into an Agreement with a Medical Practitioner or a group of Medical Practitioners, or a Hospital or a group of Hospitals, specifying the total charge for any Treatment and the Benefits payable by the Fund.
(2) Any amendments to the Agreement that take effect during the period of the Agreement may not increase any out-of-pocket expenses payable by Members.
(3) …
(Original emphasis.)
328 Further, there is nothing in the PHIA or the Private Health Insurance (Complying Product) Rules 2010 (No 2) (the Rules) made thereunder which assists the ACCC's unconscionability case in terms of suggesting that notification of the termination of the MPPAs was either necessary or desirable. Indeed the prescriptive provisions more point against the suggestion that Medibank acted unconscionably by not giving notice of such termination. Chapter 3 of the PHIA regulates complying health insurance products. Section 63-1 provides that a private health insurer must ensure that the only kind of insurance that it makes available as part of its health insurance business is insurance in the form of complying health insurance products (ss 63-5 and 63-10). It must inter-alia meet community rating requirements (Division 66), coverage requirements (Division 69), benefit requirements for policies that cover hospital treatment (Division 72) and requirements under the Rules. There is no issue that Medibank met these prescriptive requirements.
329 Division 93 of the PHIA sets out very detailed provisions concerning giving information to consumers. Section 93-1 required the insurer to maintain at all times an up to date standard information statement for each product subgroup of each complying health insurance product. It had to contain the information, and be in the form, set out in the Rules. Section 93-15 regulated the giving of information to newly insured people. Section 93-20 regulated keeping insured people up to date. Section 93-25 required the giving of advance notice of detrimental changes to the insurer's rules. Further, s 93-30 provided that it was an offence for an insurer not to do the thing required under s 93-30.
330 Relevantly, it is worth setting out ss 93-20(1) – (3):
93-20 Keeping insured people up to date
(1) A private health insurer must ensure that an adult insured under a complying health insurance policy issued by the insurer is given the standard information statement for the product subgroup that the policy belongs to, at least once every 12 months.
(2) A private health insurer must ensure that, if a proposed change to the insurer's rules:
(a) is or might be detrimental to the interests of an insured person; and
(b) will require an update to the standard information statements for a complying health insurance product of the insurer;
an adult insured under each complying health insurance policy in the product:
(c) is informed about the proposed change a reasonable time before the change takes effect; and
(d) is given the updated standard information statement for the product subgroup that the policy belongs to as soon as practicable after the statement is updated.
(3) A private health insurer must ensure that, if an adult who is insured under a complying health insurance policy of the insurer asks an officer, employee or agent of the insurer for information about what the policy covers or the benefits the policy provides, the adult is given the information as soon as practicable.
331 Further, s 93-25(1) provided:
93-25 Giving advance notice of detrimental changes to rules
(1) A private health insurer must ensure an adult insured under a complying health insurance policy issued by the insurer is informed about any proposed change to the insurer's rules (other than a change to which subsection 93-20(2) applies), a reasonable time before the change takes effect, if the proposed change is or might be detrimental to the interests of an insured person.
332 In terms of the form and content of the standard information statement, this was prescribed by, inter-alia, rules 13 to 16 of Part 3 of the Rules, and relevant to the present context Schedules 1 and 4. Rule 13 should be set out:
13. Information and form
(1) For subsection 93-5 (1) of the Act, this Part and Schedules 1, 2, 3 and 4 set out the form of, and the permitted content to be contained in, a statement about a product subgroup of a complying product.
(2) The form of the statements in Schedules 1, 2 and 3, and the permitted content for those forms, must not be added to, deleted, rearranged or modified in any way except:
(a) as specified in the relevant Schedules;
(b) to omit, when inapplicable, the grey text, or to omit text for which the grey text is the appropriate alternative;
(c) to place a barcode or product code in the margin; and
(d) until 1 April 2008 - to omit the 'Medicare Levy Surcharge' field.
(3) A statement must not exceed one A4 page, except as permitted by rule 16.
333 The statutory regulation was highly prescriptive as to the permitted content. Moreover, generally speaking, the standard information statement was not to exceed one A4 page. And it was this statement that had to be updated from time to time.
334 Now the substance of the ACCC's case is that in essence Medibank had an obligation to give prior notice of the termination of MPPAs in the sense that not to do so amounted to unconscionable conduct and constituted a contravention of s 21. But no part of the prescriptive statutory and regulatory regime went anywhere close to requiring such disclosure. Now this does not necessarily foreclose such non-disclosure as constituting unconscionable conduct. Nevertheless, such an assessment must be made in that context; and no one has suggested that Medibank has not complied with the PHIA and the Rules. Further, as is apparent, s 93-20 only required prior notice of a "proposed change to the insurer's rules" that is or might be detrimental to the interests of an injured person. Relevantly here, the termination of the MPPAs did not involve any change to Medibank's rules.
335 Finally on this aspect, there is nothing in the Health Insurance Act 1973 (Cth) itself that touches or concerns the issue I am addressing.
336 Seventh, paragraph 6(j) asserts that Medibank was easily able to notify its members about any changes to their benefits. But I agree with Medibank that the ease or difficulty of issuing a notice to 3.8 million members is not the central point. The relevant question is whether not notifying all members was unconscionable in all the circumstances.
337 Eighth, paragraph 6(k) asserts that despite the matters in sub-paragraphs (a) to (j), Medibank adopted and implemented the non-disclosure strategy. Now I am not sure that the decision not to directly notify is properly identified in terms as a "non-disclosure strategy". Nevertheless, in substance a decision was taken not to directly notify.
338 Ninth, paragraph 6(l) asserts that Medibank adhered to the non-disclosure strategy even after:
(a) it received a higher volume of complaints than it had expected at the time the diagnostics funding decision was made;
(b) it knew from at least mid-October 2014 that some of its members had not been told by diagnostic providers about the OOPs that they might incur for in-hospital diagnostic services before they received those services; and
(c) it knew from at least November 2014 that some diagnostic providers had increased their charges for in-hospital diagnostic services after 1 September 2014.
339 But I agree with Medibank that the fact that complaints were received after the diagnostics funding decision does not entail that ex ante the decision Medibank's failure to notify was unconscionable or that such failure after the decision was unconscionable. Moreover, given the scale of Medibank's business (3.8 million members), the number of complaints was relatively very modest.
340 In summary, I would reject ground 6. The factors set out in ground 6 are either not established or do not together or separately and in the context of the matters earlier discussed establish that his Honour was in error in finding no unconscionable conduct. Further, even if ground 7(c) has some substance to it, I do not consider that upon a review of all relevant material any different overall conclusion is warranted. And in any event there are even broader themes that support his Honour's overall conclusion.
Broader secondary analysis and conclusions
341 Let me at this stage move away from the factors identified by the ACCC and make the following more general points.
342 First, Allsop CJ said in Paciocco (FFC) at [297]:
The variety of considerations that may affect the assessment of unconscionability only reflects the variety and richness of commercial life. It should be emphasised, however, that faithfulness or fidelity to a bargain freely and fairly made should be seen as a central aspect of legal policy and commercial law. It binds commerce; it engenders trust; it is a core element of decency in commerce; and it gives life and content to the other considerations that attend the qualifications to it that focus on whether the bargain was free or fair in its making or enforcement.
343 Now there is little doubt that Medibank has shown faithfulness and fidelity to the bargain struck with its members. What is inherent in the ACCC's case is necessarily the proposition that Medibank should have gone further than the bargain with members enshrined in the contractual and legislative regime. But that is a less secure platform to rest its unconscionable case on.
344 Second, by the way the ACCC has put its case by asserting that non-notification amounted to unconscionable conduct, it has sought to create in substance a construct of imposing an obligation to notify in all the circumstances which is not to be found in the very detailed and prescriptive contractual and legislative regime. That is hardly an attractive foundation.
345 Third, Medibank did not act in a manner inconsistent with industry practice in terms of communications with members.
346 Fourth, as I have explained, Medibank in seeking to implement the diagnostics funding decision was not seeking to ultimately profit to its own account. Any gain in essence had to ultimately be used for the benefit of members including reducing increases in premiums as I have previously explained.
347 Fifth, the diagnostics funding decision was not secret and could not be kept secret; for example, providers were notified who were then likely in turn to notify members directly. Further, in any event members had no prior notice of MPPAs from Medibank; in those circumstances, not to notify of any termination of something of which they were not aware is hardly a strong foundation for unconscionable conduct.
348 Sixth, the financial consequences of the diagnostics funding decision should not be overstated. Many were paying OOPs in any event. Further, there was no complete coverage with MPPAs before the decision. And this is all in the context where Medibank made no promises concerning the MPPAs, which the members were not aware of anyway, and where the ACCC has failed on its representations case.
349 Seventh, I accept that the diagnostics funding decision and the failure to notify may have had a greater effect on claiming members who were chronic sufferers. But the quantum of the effects of this should not be over-stated for the reasons that I have previously explained. In any event, the fact that conduct may be said to have had harsh consequences on a class of members does not in and of itself establish that it was unconscionable. To repeat, neither unfair conduct nor harsh conduct nor both are sufficient to establish unconscionable conduct.
350 Eighth, the ACCC's "surprise" thesis may be accepted. The diagnostics funding decision and its consequences may have surprised a member when it was drawn to his or her attention. But as I say, when all the circumstances are considered even with this surprise, unconscionable conduct is not made out.
351 Ninth, I have considered whether there ought to be a separate treatment of the unconscionability question depending upon whether one was considering a failure to notify before the diagnostics funding decision or a failure to notify after that decision. But on balance, even if there is a slightly different analysis to be made, the answer is still the same: there was no unconscionable conduct.
352 Tenth, there was no suggestion established by evidence that Medibank did not act in good faith.
353 Eleventh, I accept that if members had been notified of the diagnostics funding decision before or after 1 September 2014, that in addition to the response of some members lapsing their membership, other members, instead of lapsing, may have tried to plan for or avoid the OOPs, for example, by changing their provider. And I accept that some members, who did not lapse, may have been distressed by the unexpected costs. Certainly, Medibank acted harshly. And I am also prepared to conclude that it acted unfairly. But this is not enough to establish statutory unconscionability.
(d) Conclusion
354 In summary, I have considered all the circumstances that were emphasised by the parties before us. I have also, of course, considered ss 21(4)(b) and (c)(i) and (ii), and the applicable factors in s 22(1) particularly ss 22(1)(a), (c), (g), (i), (j) and (l). But at the end of the day, if Medibank's conduct is assessed against the statutory conscience being the construct of values and standards that I have discussed earlier, its conduct was not unconscionable.
355 The essence of the ACCC's case was to argue that:
The critical norm in the present case is the basic proposition that in any industry, consumers should be given accurate information to enable them to make informed decisions between competing products in the market, both at the time of purchase and later, via updating notices, if features of the product are changed by the offeror. This is especially so given that the market here is complex and not well understood by consumers, there is information asymmetry between the insurer and consumers, and information about the scope of insurance protection is important to help consumers plan for and make informed decisions about medical treatment. Aspects of these norms are reflected in the PHI Act and the Industry Code, but most centrally and most generally in the ACL itself.
356 But for the reasons that I have endeavoured to explain, this is a gloss on the relevant product, its characteristics, the relevant regulatory regime, the nature of the diagnostics funding decision and its consequences.
357 Grounds 6 and 7(a) have not been made out, and even if grounds 7(b) and (c) have been made out they do not change the ultimate result. I otherwise agree with the reasons and orders proposed by Perram J.
I certify that the preceding two hundred and fifty-four (254) numbered paragraphs are a true copy of the Reasons for Judgment herein of the Honourable Justice Beach. |
Dated: 20 December 2018

